Introduction
Ceruloplasmin is a serum ferroxidase responsible for 95% copper transport in the blood. It is well known for its role in the pathogenesis of Wilson disease and regulating iron metabolism.[1] Also, ceruloplasmin is a positive acute-phase reactant, meaning its levels increase in inflammatory conditions or cell injury.[2] Copper is a trace element that acts as a cofactor for multiple enzymes in critical cellular reactions, such as cytochromes, which participate in the electron transport chain and redox catalysis.[3] Recent studies have shown that alterations of ceruloplasmin protein and copper homeostasis are associated with Alzheimer disease.[4][5]
Fundamentals
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Fundamentals
Ceruloplasmin production occurs in the liver and is a ferroxidase enzyme encoded by the CP gene in humans.[6] Liver hepatocytes predominantly synthesize ceruloplasmin. In the liver, P-type ATPase (ATPase 7B) enzymes are necessary to incorporate copper into apo-ceruloplasmin.[7] Ceruloplasmin is then released into the bloodstream to transport properly to distal sites and to complete its functions in other metabolic processes, namely iron homeostasis and metabolism. A solution of ceruloplasmin is blue, and excess serum levels may give the serum a greenish hue. Each ceruloplasmin molecule can bind to 6 to 8 copper atoms; usually, 50% are in cupric (+2) and 50% are in cuprous (+1) states.[8]
Issues of Concern
As an acute phase reactant, ceruloplasmin may elevate in multiple conditions such as trauma, tissue damage, infection, or inflammation. It bears mention that ceruloplasmin may increase in states of high estrogen and progesterone; for instance, pregnant women, patients receiving estrogen therapy, and women on oral contraceptives may have high levels of ceruloplasmin.[2] In addition, many medications, notably anti-seizure drugs (eg, valproic acid), are known to increase ceruloplasmin levels.[9] Measurements of the ceruloplasmin level are not common in standard laboratory testing, but certain symptoms may raise clinical suspicion and prompt the ordering of ceruloplasmin levels.[10] These include the following:
- Anemia
- Ataxia
- Nausea and abdominal pain
- Neuropathy
- Jaundice
- Fatigue
- Behavioral changes
- Tremors
- Difficulty walking or swallowing
- Dystonia
- Sleep disorders
Cellular Level
Ceruloplasmin is an enzyme from the multi-copper oxidase family. It is synthesized primarily in the liver parenchymal cells, with small amounts produced from immune cells, including macrophages and lymphocytes.[11] The peptide chain is synthesized, and copper atoms are added from an intracellular ATPase.[12] Although copper availability is not necessary for ceruloplasmin translation, copper binding is essential for the adequate folding of ceruloplasmin protein and the normal attachment of side-chain oligosaccharides. The apo-ceruloplasmin, which does not contain copper or the ATPase, is less structurally stable, and most undergo intracellular degradation. However, a small portion of apo-enzyme reaches circulation but has a short half-life of 5 to 6 hours compared to the holoenzyme (ceruloplasmin plus copper), which has a longer half-life of a few days.[13]
Molecular Level
Ceruloplasmin has a molecular weight of 132kDa, and its crystal structure was identified in 1997. It is a polypeptide chain of 1046 amino acids with three asparagine-linked oligosaccharide side chains, and it contains a total carbohydrate content of 7 to 8%.[14] The size and charge of the molecule depend on the glycosylation of the molecule, the number of copper atoms, peptide chain variations, and polymerization.[15] Ceruloplasmin is highly prone to proteolysis; recent studies have utilized electron paramagnetic resonance spectroscopy techniques to evaluate its structure and concentration.[16]
Function
The ceruloplasmin molecule is a catalyst for redox reactions in plasma. It can oxidize iron from ferrous (2+) to ferric iron (3+), which assists in iron binding to transferrin. Neurological disorders in hereditary ceruloplasmin deficiency may be caused by disordered iron transport in the brain. It is also thought to be involved in controlling membrane lipid oxidation. In the presence of superoxide, ceruloplasmin promotes LDL oxidation in vitro and is colocalized with oxidized LDL in atherosclerotic lesions.[17] The liver is the crucial organ in copper homeostasis, and more than 90% of the copper exported from the liver to the plasma is in the form of ceruloplasmin. However, ceruloplasmin's role in copper transport from the peripheral tissues is limited. Albumin is the main protein responsible for ionic copper transport from the tissues (such as absorbed copper in the digestive tract). The copper-albumin complex is directed to the liver via the portal system in circulation. Albumin and transcuprein appear to be the other major copper transport proteins, especially immediately post-gastrointestinal absorption.[18]
Testing
Standard Ceruloplasmin measurement is via a blood test, often by analyzing a serum sample with immunoassays, immunoturbidimetry, or immunonephelometry. The sample must be spun and separated as soon as the laboratory receives it and assays it promptly. The samples may be stored at 4 degrees Celsius for up to three days or longer at -70 degrees Celsius. The serum test is often part of the workup when there is suspicion of Wilson disease and is commonly ordered along with urine copper levels. Several factors, including diet, hormone levels, and other genetic disorders, may influence the resulting ceruloplasmin levels in the urine and serum.[19][20]
Deficiency States
Low ceruloplasmin levels may indicate the following pathological conditions: Wilson disease, Menke disease, copper deficiency, aceruloplasminemia, or in states of low protein energy intake (eg, malnutrition.)[21][22]
Excess
High ceruloplasmin levels may suggest or be present in physiological and pathological circumstances, including pregnancy, oral contraceptive use, copper toxicity/zinc deficiency, lymphoma, lung cancer, acute and chronic inflammation, rheumatoid arthritis, angina, Alzheimer disease, schizophrenia, obsessive-compulsive disorder.[23][24][25]
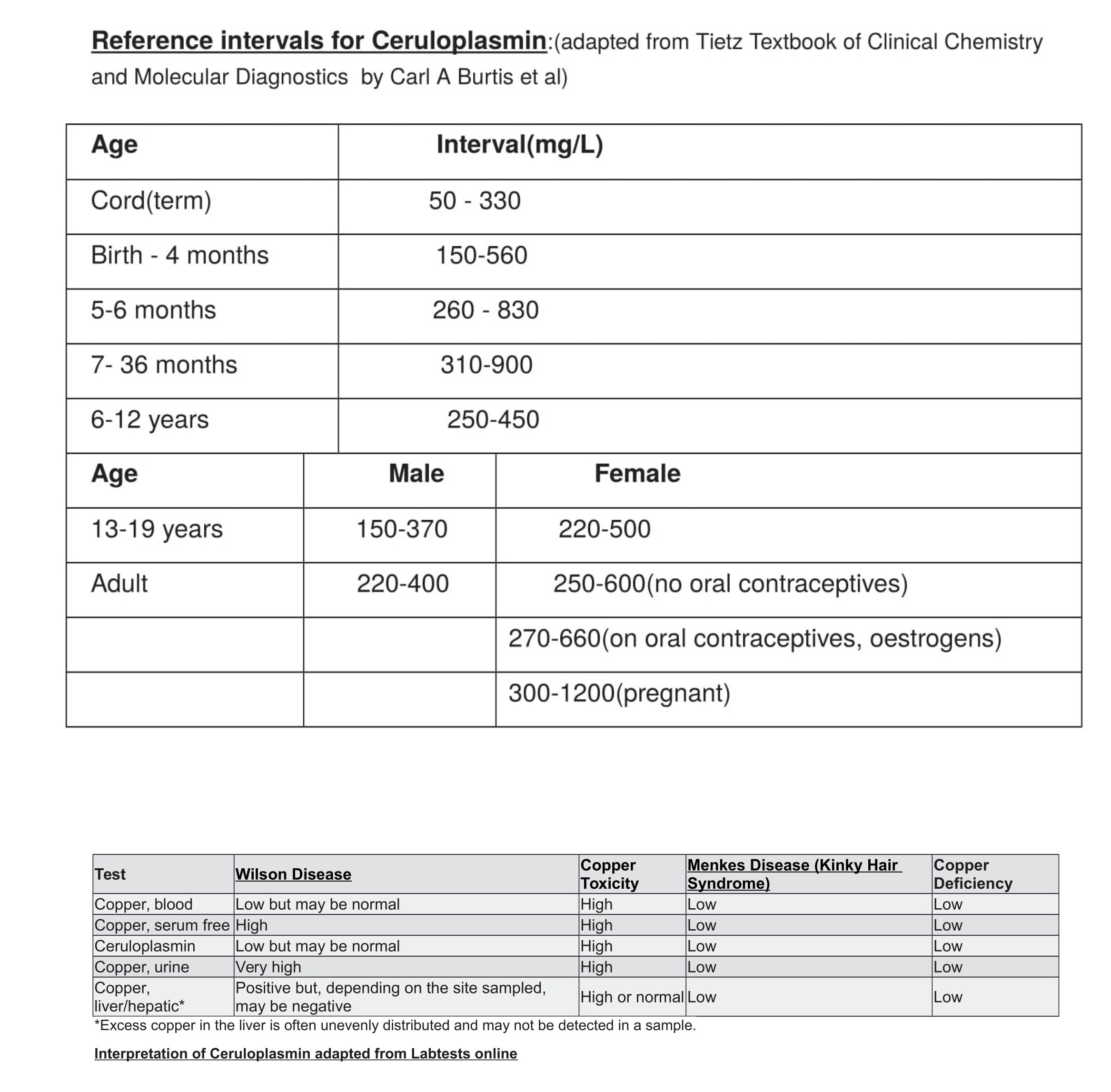
Reference intervals (adapted from Tietz Textbook of Clinical Chemistry and Molecular Diagnostics by Carl A Burtis et al):
Age/Interval(mg/L)
- Cord (term): 50 to 330
- Birth to 4 months: 150 to 560
- 5 to 6 months: 260 to 830
- 7 to 36 months: 310 to 900
- 6 to 12 years: 250 to 450
Age/Male/Female
- 13 to 19 years: 150 to 370/220 to 500
- Adult: 220 to 400/250 to 600 (no oral contraceptives)
- Adult: 270 to 660 (on oral contraceptives, estrogens)
- Adult: 300 to 1200 (pregnant) See Image. Intervals and Interpretation of Ceruloplasmin.
Wilson disease is diagnosed based on clinical presentation, biochemical tests, and ATP7B mutation analysis. Regarding serum ceruloplasmin testing, only those with low serum ceruloplasmin, low serum copper, and high urine copper meet the criteria for Wilson disease. However, some patients diagnosed with Wilson disease exhibit normal ceruloplasmin levels. When urine and serum concentrations of copper and ceruloplasmin are low, the patient suffers from a copper deficiency. Factors interfering with the body's ability to metabolize copper, such as chelator medications, diet, and iron restriction, may also affect serum ceruloplasmin levels.[26][27] See Image. Ceruloplasmin Interpretation.
Pathophysiology
Ceruloplasmin is undetectable before 20 weeks of gestation. Concentrations gradually rise to 25 to 40% of average adult concentrations and, by six months, are close to adult concentrations.[28]
Special Situations
- There have been reports of inherited aceruloplasminemia in several families, and it is a genetic cause of ceruloplasmin deficiency; these patients have neurodegeneration and iron deposition in the brain.[29] Concerning aceruloplasminemia, a diagnosis of aceruloplasminemia could be suspected based upon a biochemical profile showing very low to absent ceruloplasmin in serum, high ferritin, low copper, low iron, microcytic anemia refractory to iron supplementation, and characteristic imaging features. Homozygous cases have distinctive imaging features with marked hypointensity of the liver, basal ganglia nuclei, thalami, dentate nuclei, and cerebral/cerebellar cortices on T2 MRI. MRI of heterozygous cases may reveal cerebellar atrophy without hypointensity of the basal ganglia.[30]
- Menkes disease is an X-linked recessive disorder caused by a mutation in the ATP7A protein. With this mutation, copper cannot be transported out of the GI tract; therefore, copper is unavailable to the liver, which causes low ceruloplasmin levels. The patients present in infancy have sparse, brittle, and kinky hair, growth retardation and neurologic degradation, and death if untreated in the first few years of life.[31]
- Wilson disease results from an autosomal recessive mutation in the ATP7B protein. Mutations in ATP7B (located on chromosome 13) lead to Wilson disease. ATP7B is an efflux transporter in the liver, but it is also essential in the Trans-Golgi Network for transferring copper for the metalation of ceruloplasmin and biliary copper excretion.[32] The point mutation H1069Q is the most common ATP7B mutation in patients from Central, Eastern, and Northern Europe, and 50 to 80% of Wilson disease patients from these countries carry at least one H1069Q allele.[33] Mutations resulting in completely absent or non-functional ATP7B protein activity are associated with early-onset, typically hepatic, severe Wilson disease; these mutations are comparatively rare.[34] It is characterized by hepatolenticular degeneration due to copper deposition in organs, including the basal ganglia, cornea, and liver. In Wilson's disease, ceruloplasmin levels are usually low, but urinary excretion of copper is high. Liver biopsy results show high copper content. Clinically, a dark ring around the iris suggests a diagnosis of Wilson disease. This sign is known as a Kayser-Fleischer ring.[35]
Clinical Significance
Treatment for Aceruloplasmin and Wilson Disease
Treatment for aceruloplasminemia mainly involves chelation therapy and increasing serum ceruloplasmin. Fresh-frozen plasma, which contains ceruloplasmin combined with IV desferrioxamine, effectively decreases iron content in the liver. Repetitive fresh-frozen plasma treatment can improve neurologic signs/symptoms. Treatment options for Wilson disease include chelation therapy (D-penicillamine, trientine, and tetrathiomolybdate) or zinc salts. Medical therapy is continued lifelong as copper accumulation is not manageable with dietary restriction alone. It is important to note that there may be an associated paradoxical worsening of neurological status after initiation of chelation therapy. While this is not fully understood, studies suggest that increased mobilization of free copper by chelator therapy may lead to acute worsening upon initiation of treatment.[34]
Complications
Diabetes mellitus, ataxia, dystonia, Parkinsonism, psychiatric problems (mostly mood disorders), cardiac disease, thyroid dyscrasia, anemia, and liver damage are common complications shared by both Wilson disease and aceruloplasminemia. Amenorrhea and frequent abortions may be complications of copper toxicity that may affect fertility. Antipsychotic drugs are applied in severe mania and to treat psychotic symptoms. In Wilson disease, antipsychotics increase the risk of neurological deterioration and hepatic injury. As such, antipsychotics with low EPS risk, such as clozapine or quetiapine, should be used.[36]
Enhancing Healthcare Team Outcomes
Surveillance should include yearly glucose tolerance tests starting at the age of 15 or the age of diagnosis if, after 15 years old, to monitor for the inception of diabetes mellitus. Regular eye exams should also be a consideration, as retinopathy is a prominent feature in aceruloplasminemia and Wilson disease. An annual echocardiogram, thyroid and liver function evaluation, and a complete blood count (CBC) starting at the diagnosis should be performed to monitor for other potential complications. Blood transfusions should be approached cautiously as the increased iron load may be challenging for patients with these disorders. In patients with Wilson disease, it is strongly recommended that familial screening is performed. The American Association for Study of Liver Diseases and the European Association for the Study of Liver both separately recommend screening first-degree relatives of the affected individuals, suggesting siblings or offspring only.[37] While most patients with Wilson disease who become pregnant have successful pregnancies, a discussion is necessary about the potential side effects of anti-copper therapy, as all available anti-copper drugs can pass into the breast.
Ceruloplasmin Interpretation Adapted from Labtestsonline [See exhibit 2]
Wilson disease
Wilson disease presents between ages 5 to 35.[38]
The clinical presentation may include the following symptoms:
- Hepatolenticular degeneration
- Kayser-Fleischer rings
- Parkinsonism
- Ataxia
- Personality changes
- Depression
- Psychosis
- Acute liver failure
- Chronic liver failure
- Cirrhosis
- Renal issues (renal tubular acidosis with aminoaciduria)
- Secondary Hemolysis is less common
- Most patients with Wilson disease have low ceruloplasmin levels
Treatment may include:
- Penicillamine
- Trientine
- Zinc
Media
(Click Image to Enlarge)
Intervals and Interpretation of Ceruloplasmin
Contributed by R Sirkar, MD
(Click Image to Enlarge)

Ceruloplasmin Interpretation
Contributed by M Lopez, BS
References
Walshe JM. Cause of death in Wilson disease. Movement disorders : official journal of the Movement Disorder Society. 2007 Nov 15:22(15):2216-20 [PubMed PMID: 17712859]
Vasilyev VB. Interactions of caeruloplasmin with other proteins participating in inflammation. Biochemical Society transactions. 2010 Aug:38(4):947-51. doi: 10.1042/BST0380947. Epub [PubMed PMID: 20658982]
Level 3 (low-level) evidenceTwomey PJ, Viljoen A, House IM, Reynolds TM, Wierzbicki AS. Relationship between serum copper, ceruloplasmin, and non-ceruloplasmin-bound copper in routine clinical practice. Clinical chemistry. 2005 Aug:51(8):1558-9 [PubMed PMID: 16040861]
Level 2 (mid-level) evidenceSquitti R, Quattrocchi CC, Forno GD, Antuono P, Wekstein DR, Capo CR, Salustri C, Rossini PM. Ceruloplasmin (2-D PAGE) Pattern and Copper Content in Serum and Brain of Alzheimer Disease Patients. Biomarker insights. 2007 Feb 7:1():205-13 [PubMed PMID: 19690651]
Squitti R, Quattrocchi CC, Salustri C, Rossini PM. Ceruloplasmin fragmentation is implicated in 'free' copper deregulation of Alzheimer's disease. Prion. 2008 Jan-Mar:2(1):23-7 [PubMed PMID: 19164917]
Sharp P. The molecular basis of copper and iron interactions. The Proceedings of the Nutrition Society. 2004 Nov:63(4):563-9 [PubMed PMID: 15831128]
Level 3 (low-level) evidenceMaio N, Polticelli F, De Francesco G, Rizzo G, Bonaccorsi di Patti MC, Musci G. Role of external loops of human ceruloplasmin in copper loading by ATP7B and Ccc2p. The Journal of biological chemistry. 2010 Jul 2:285(27):20507-13. doi: 10.1074/jbc.M109.090027. Epub 2010 Apr 29 [PubMed PMID: 20430895]
Level 3 (low-level) evidenceSharonov BP, Govorova NIu. [Oxidation of ceruloplasmin by hypochlorite. The loss of blue color and preservation of oxidase activity]. Biokhimiia (Moscow, Russia). 1990 Jun:55(6):1145-8 [PubMed PMID: 2169906]
Hurd RW, Van Rinsvelt HA, Wilder BJ, Karas B, Maenhaut W, De Reu L. Selenium, zinc, and copper changes with valproic acid: possible relation to drug side effects. Neurology. 1984 Oct:34(10):1393-5 [PubMed PMID: 6435012]
Level 3 (low-level) evidenceAggarwal A, Bhatt M. Wilson disease. Current opinion in neurology. 2020 Aug:33(4):534-542. doi: 10.1097/WCO.0000000000000837. Epub [PubMed PMID: 32657896]
Level 3 (low-level) evidenceVlasova II, Sokolov AV, Kostevich VA, Mikhalchik EV, Vasilyev VB. Myeloperoxidase-Induced Oxidation of Albumin and Ceruloplasmin: Role of Tyrosines. Biochemistry. Biokhimiia. 2019 Jun:84(6):652-662. doi: 10.1134/S0006297919060087. Epub [PubMed PMID: 31238865]
Das S, Sahoo PK. Ceruloplasmin, a moonlighting protein in fish. Fish & shellfish immunology. 2018 Nov:82():460-468. doi: 10.1016/j.fsi.2018.08.043. Epub 2018 Aug 23 [PubMed PMID: 30144565]
Linder MC. Apoceruloplasmin: Abundance, Detection, Formation, and Metabolism. Biomedicines. 2021 Feb 25:9(3):. doi: 10.3390/biomedicines9030233. Epub 2021 Feb 25 [PubMed PMID: 33669134]
Bento I, Peixoto C, Zaitsev VN, Lindley PF. Ceruloplasmin revisited: structural and functional roles of various metal cation-binding sites. Acta crystallographica. Section D, Biological crystallography. 2007 Feb:63(Pt 2):240-8 [PubMed PMID: 17242517]
Harazono A, Kawasaki N, Itoh S, Hashii N, Ishii-Watabe A, Kawanishi T, Hayakawa T. Site-specific N-glycosylation analysis of human plasma ceruloplasmin using liquid chromatography with electrospray ionization tandem mass spectrometry. Analytical biochemistry. 2006 Jan 15:348(2):259-68 [PubMed PMID: 16321355]
Ibragimova MI, Chushnikov AI, Moiseev VN, Petukhov VIu, Zheglov EP, Pogorel'tsev VI, Khardina NB. [Electron paramagnetic resonance determination of ceruloplasmin concentration in the blood of patients for the diagnosis of urological cancer diseases]. Klinicheskaia laboratornaia diagnostika. 2010 Apr:(4):17-20 [PubMed PMID: 20524342]
Levitan I, Volkov S, Subbaiah PV. Oxidized LDL: diversity, patterns of recognition, and pathophysiology. Antioxidants & redox signaling. 2010 Jul 1:13(1):39-75. doi: 10.1089/ars.2009.2733. Epub [PubMed PMID: 19888833]
Level 3 (low-level) evidenceMoriya M, Ho YH, Grana A, Nguyen L, Alvarez A, Jamil R, Ackland ML, Michalczyk A, Hamer P, Ramos D, Kim S, Mercer JF, Linder MC. Copper is taken up efficiently from albumin and alpha2-macroglobulin by cultured human cells by more than one mechanism. American journal of physiology. Cell physiology. 2008 Sep:295(3):C708-21. doi: 10.1152/ajpcell.00029.2008. Epub 2008 Jun 25 [PubMed PMID: 18579803]
González-Jiménez E, Schmidt-Riovalle J, Sinausía L, Carmen Valenza M, Perona JS. Predictive value of ceruloplasmin for metabolic syndrome in adolescents. BioFactors (Oxford, England). 2016 Mar-Apr:42(2):163-70. doi: 10.1002/biof.1258. Epub 2016 Jan 27 [PubMed PMID: 27083758]
Yada T, Nagae M, Moriyama S, Azuma T. Effects of prolactin and growth hormone on plasma immunoglobulin M levels of hypophysectomized rainbow trout, Oncorhynchus mykiss. General and comparative endocrinology. 1999 Jul:115(1):46-52 [PubMed PMID: 10375463]
Level 3 (low-level) evidenceHermann W. Classification and differential diagnosis of Wilson's disease. Annals of translational medicine. 2019 Apr:7(Suppl 2):S63. doi: 10.21037/atm.2019.02.07. Epub [PubMed PMID: 31179300]
Gautam B, Deb K, Banerjee M, Ali MS, Akhter S, Shahidullah SM, Hoque MR. Serum zinc and copper level in children with protein energy malnutrition. Mymensingh medical journal : MMJ. 2008 Jul:17(2 Suppl):S12-5 [PubMed PMID: 18946444]
Level 2 (mid-level) evidenceKalra R, Kalra VB, Sareen PM, Khandelwal R. Serum copper and ceruloplasmin in pregnancy with anaemia. Indian journal of pathology & microbiology. 1989 Jan:32(1):28-32 [PubMed PMID: 2592032]
Esme H, Cemek M, Sezer M, Saglam H, Demir A, Melek H, Unlu M. High levels of oxidative stress in patients with advanced lung cancer. Respirology (Carlton, Vic.). 2008 Jan:13(1):112-6. doi: 10.1111/j.1440-1843.2007.01212.x. Epub [PubMed PMID: 18197920]
Level 2 (mid-level) evidenceWolf TL, Kotun J, Meador-Woodruff JH. Plasma copper, iron, ceruloplasmin and ferroxidase activity in schizophrenia. Schizophrenia research. 2006 Sep:86(1-3):167-71 [PubMed PMID: 16842975]
Manolaki N, Nikolopoulou G, Daikos GL, Panagiotakaki E, Tzetis M, Roma E, Kanavakis E, Syriopoulou VP. Wilson disease in children: analysis of 57 cases. Journal of pediatric gastroenterology and nutrition. 2009 Jan:48(1):72-7. doi: 10.1097/MPG.0b013e31817d80b8. Epub [PubMed PMID: 19172127]
Level 3 (low-level) evidenceWeiss KH, Merle U, Schaefer M, Ferenci P, Fullekrug J, Stremmel W. Copper toxicosis gene MURR1 is not changed in Wilson disease patients with normal blood ceruloplasmin levels. World journal of gastroenterology. 2006 Apr 14:12(14):2239-42 [PubMed PMID: 16610028]
Kroll CA, Ferber MJ, Dawson BD, Jacobson RM, Mensink KA, Lorey F, Sherwin J, Cunningham G, Rinaldo P, Matern D, Hahn SH. Retrospective determination of ceruloplasmin in newborn screening blood spots of patients with Wilson disease. Molecular genetics and metabolism. 2006 Sep-Oct:89(1-2):134-8 [PubMed PMID: 16644258]
Level 2 (mid-level) evidenceAdam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, Miyajima H, Hosoi Y. Aceruloplasminemia. GeneReviews(®). 1993:(): [PubMed PMID: 20301666]
McNeill A, Pandolfo M, Kuhn J, Shang H, Miyajima H. The neurological presentation of ceruloplasmin gene mutations. European neurology. 2008:60(4):200-5. doi: 10.1159/000148691. Epub 2008 Jul 30 [PubMed PMID: 18667828]
Jafri SK, Kumar R, Lashari SK, Chand P. Menkes disease: A rare disorder. JPMA. The Journal of the Pakistan Medical Association. 2017 Oct:67(10):1609-1611 [PubMed PMID: 28955085]
Prohaska JR. Role of copper transporters in copper homeostasis. The American journal of clinical nutrition. 2008 Sep:88(3):826S-9S [PubMed PMID: 18779302]
Ferenci P. Regional distribution of mutations of the ATP7B gene in patients with Wilson disease: impact on genetic testing. Human genetics. 2006 Sep:120(2):151-9 [PubMed PMID: 16791614]
Bandmann O, Weiss KH, Kaler SG. Wilson's disease and other neurological copper disorders. The Lancet. Neurology. 2015 Jan:14(1):103-13. doi: 10.1016/S1474-4422(14)70190-5. Epub [PubMed PMID: 25496901]
Low QJ, Siaw C, Lee RA, Cheo SW. Kayser-Fleischer rings and Wilson's disease. QJM : monthly journal of the Association of Physicians. 2020 Sep 1:113(9):693-694. doi: 10.1093/qjmed/hcaa005. Epub [PubMed PMID: 31917404]
Członkowska A, Litwin T, Dusek P, Ferenci P, Lutsenko S, Medici V, Rybakowski JK, Weiss KH, Schilsky ML. Wilson disease. Nature reviews. Disease primers. 2018 Sep 6:4(1):21. doi: 10.1038/s41572-018-0018-3. Epub 2018 Sep 6 [PubMed PMID: 30190489]
Li H, Liu L, Li Y, He S, Liu Y, Li J, Tao R, Li W, Shang S. Familial screening of children with Wilson disease: Necessity of screening in previous generation and screening methods. Medicine. 2018 Jul:97(27):e11405. doi: 10.1097/MD.0000000000011405. Epub [PubMed PMID: 29979436]
Mareček Z, Brůha R. [Wilsons disease]. Vnitrni lekarstvi. 2013 Jul:59(7):578-83 [PubMed PMID: 23909262]