Introduction
Cerebellar hemorrhage or hematoma is a type of intracranial hemorrhage (ICH) where the bleeding is located in the posterior fossa or cerebellum and accounts for 9% to 10% of all ICH.[1] The posterior fossa is a small space in the skull containing the brainstem and cerebellum. If a mass such as a hemorrhage grows in this region, particularly the brainstem and 4th ventricle, it can block the normal flow of cerebral spinal fluid leading to hydrocephalus, increased intracranial pressure, and symptoms onset. Cerebellar hemorrhage can be spontaneous, a result of a stroke or secondary to trauma, and occurs most frequently in middle-aged and older adults. Patients typically have underlying risk factors leading to hemorrhages such as hypertension or small vessel disease. The clinical presentation is dependent upon the size and location of the hematoma as well as the location and amount of edema of associated structures in the posterior fossa. The initial imaging modality is typically a non-contrast computed tomography (CT) scan. Management spans the spectrum from close observation to acute surgical intervention with optimal timing of surgery.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The most common non-traumatic etiology for cerebellar hemorrhage as for all intracranial hemorrhages is hypertensive vasculopathy causing microaneurysms and resultant rupture. Cerebellar hemorrhage from hypertension most commonly occurs in the middle-aged or older population, often in the dentate nucleus with extension to other areas from the rupture of microaneurysms along the penetrating small vessels. Other causes of cerebellar hemorrhage include trauma, coagulopathy (cirrhosis, disseminated intravascular coagulation or thrombocytopenia) or bleeding disorders (primary and drug-induced (anticoagulation, antiplatelet or thrombolytic medications)), ischemic stroke with hemorrhagic transformation, cerebral amyloid angiopathy,[2] vascular malformations such as arteriovenous malformation (AVM), dural arteriovenous fistula in the tentorium,[3] brain tumors (primary or metastatic),[4][5] septic embolism, central nervous system infection (encephalitis, moyamoya disease, vasculitis (lupus)), sympathomimetic drugs such as cocaine and amphetamines,[6] aneurysm (posterior circulation) or remote hemorrhage following supratentorial neurosurgical procedure.[7]
The most common primary central nervous system (CNS) tumors to undergo hemorrhagic transformation are glioblastomas. The metastatic CNS tumors that are more prone to hemorrhage include lesions from the lung, breast, kidney, and melanomas. Cerebellar hemorrhage in younger patients may be due to substance abuse, trauma, or CNS aneurysms, or AVMs.
Epidemiology
Nontraumatic intracranial hemorrhage varies by race and age, but overall it is the cause of 9% to 27% of strokes globally with an annual incidence of 12 to 31 per 100000 people.[8][9] Cerebellar hemorrhage occurs in approximately 10% of all ICH with a low annual incidence of 1% to 2% in all strokes. The incidence of ICH increases with age, doubling every 10 years after age 35.[10][11] The rate is highest in the Asian populations, lowest in Whites, with Blacks having an intermediate occurrence rate.[12]
Pathophysiology
The cerebellar location is not unique as far as the causes of intracranial hemorrhage. The prevailing belief is that patients with long-standing hypertension have degenerative changes in the penetrating small blood vessel walls leading to the subsequent formation of microaneurysms that rupture and hemorrhage.[13] Tumors, blood disorders, amyloid, arteriovenous malformation, trauma, and stimulant drug abuse may also lead to cerebellar hemorrhage. Remote cerebellar hemorrhage after craniotomies is thought to be a result of a loss of cerebral spinal fluid (CSF), causing a "sag" in the cerebellum with resultant venous bleeding often tracking along the superior cerebellum with most cases having a benign course.[14]
History and Physical
Symptom onset is typically abrupt, with a significant variation of symptom presentation dependent on the location and size of the hemorrhage. Some patients with smaller cerebellar hemorrhage remain awake and may complain of headache, nausea, vomiting, vertigo, or ataxia. If the hemorrhage is large, patients may present with an altered level of consciousness or even unresponsiveness. Symptoms may change suddenly, correlating with hematoma expansion. Symptoms may also occur during stressful situations or strenuous activity. A detailed history is critical, noting any of the following: a history of hypertension, coagulopathy including chemically induced, head trauma, known history of an intracranial aneurysm, or arteriovenous malformation (AVM), history of malignancy, and use of sympathomimetic drugs (cocaine and amphetamines). Symptom presentation in descending order of frequency include the following:
- Abrupt onset headache
- Nausea and vomiting
- Difficulty with ambulation (truncal ataxia)
- Vertigo and dizziness
- Dysarthria
- Neck pain or nuchal rigidity
- Loss of consciousness or altered mental status
Physical examination is also variable and dependent on hemorrhage location, with some patients awake and others unresponsive. Cerebellar signs may include any combination of the following:
- Limb ataxia
- Dysarthria
- Nystagmus
- Abnormal gaze or facial weakness (cranial nerve palsy ipsilateral to the hematoma)
- Abnormal gait
Evaluation
Noncontrast head computerized tomography (CT) imaging is quick and widely available so it is typically the first and most efficient method of evaluation for those patients who present with signs and symptoms of possible cerebellar hemorrhage. Most hemorrhages are readily identified as hyperdense lesions in the cerebellum. On occasion, dense calcification of the dentate nucleus can be confused with hemorrhage, but the absence of a mass effect, sharp margins, and bilateral presence should point more towards calcification over a hemorrhage. Contrast extravasation following an endovascular procedure will also appear dense like a cerebellar hemorrhage, but dual-energy CT can differentiate the two.[15] Further imaging modalities that may help in the further delineation of the lesion may be CT angiogram, magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), or angiography.
Treatment / Management
Treatment of cerebellar hemorrhage is dependent on the size of the hemorrhage in addition to the clinical presentation. Airway protection with endotracheal intubation may be necessary for patients who present with severely altered and depressed level of consciousness or altered mental status (GCS less than 8). Neurosurgical consultation should be obtained urgently after diagnosis to assist with optimal management and treatment. Small hemorrhages without significant mass effect can often be managed conservatively with admission to a critical care unit capable of frequent neurologic assessments. Large hemorrhages, typically greater than 3 to 4 cm, may require surgical intervention and evacuation, particularly if associated with edema, intraventricular extension, brainstem displacement, or hydrocephalus. If patients are intubated, normocarbia should be maintained. There is no need for prophylactic hyperventilation except in the extreme cases of impending brainstem herniation, and it should only be for a short period.[16] Corticosteroids have not demonstrated any benefit in the treatment of cerebellar hemorrhage.
Patients with cerebellar hemorrhage often have an acute blood pressure elevation, as in any other case of intracranial hemorrhage. It is often a fine balance to aim to minimize hemorrhage growth and increased intracranial pressure while maintaining cerebral perfusion. A recent consensus recommendation believes it is safe to lower the blood pressure to less than 140 mm Hg systolic.[17][18] The 2010 American Heart Association guidelines on the management of blood pressure in intracerebral hemorrhage suggest values less than 160/90 mm Hg or a mean arterial pressure (MAP) less than 110 mm Hg.[19] Body temperature should be maintained within the normal range, and if the patient does develop an elevated body temperature, pharmacotherapy or cooling measures should be instituted to maintain a core body temperature of lower than 37.5 C as the fever has been shown to worsen outcomes in the injured brain.[20] Current evidence does not support hypothermia for cerebellar hemorrhage. Maintaining normal glucose levels is necessary as hyperglycemia has correlations with poorer outcomes in patients with cerebellar hemorrhage.[21][22] Hypoglycemia should also be avoided, and current practice suggests a reasonable glucose range of 100 to 180 mg/dL.[23] In the intensive care setting, insulin therapy over oral agents is preferred. Intensive compared to conventional glucose control did not demonstrate any significant difference in clinical outcomes.[24][25] Normovolemia should be maintained with isotonic fluids with appropriate correction of serum electrolytes such as sodium, potassium, and magnesium. Mild hypertonic fluid such as 1.5% hypertonic saline may be used to correct hyponatremia. Cardiac arrhythmias may occur with an injured brain, and it is important to keep the potassium level above 4.0 mmol/L and magnesium above 2.0 mg/dL so as not to aggravate arrhythmias. (A1)
Anticoagulation and/or antiplatelet medications should be immediately discontinued in cases of cerebellar hemorrhage. The reversal of the coagulopathy should take place with an appropriate reversal agent. Patients on warfarin should receive vitamin K (10 mg) and factor replacement in the form of fresh frozen plasma (FFP) or prothrombin complex concentrate (PCC), both of which are effective.[26] Factor replacement with PCC or 4-factor-PCC should be attempted in patients on novel oral anticoagulants, but supporting evidence is limited.[27][28] Platelet replacement therapy in patients on antiplatelet medications or those with thrombocytopenia and platelet counts less than 50000 is often performed with severe bleeding and before surgical intervention, but the benefit is unknown.(B2)
Differential Diagnosis
The differential diagnosis for patients presenting with any combination of sudden onset of symptoms such as headache, nausea, vomiting, dizziness, or vertigo includes both central and peripheral disease processes.
Central causes:
- Acute demyelinating disorder such as multiple sclerosis (MS) or encephalitis
- Alcohol use disorder
- Cerebellar hemorrhage
- Cerebellar infarction
- Cerebellar neoplasm
- Cerebellitis
- Illicit drug use
- Medication toxicity (phenytoin or carbamazepine)
Peripheral causes:
- Benign paroxysmal positional vertigo (BPPV)
- Labyrinthitis
- Meniere disease
- Vestibular neuronitis
Prognosis
The mortality associated with cerebellar hemorrhage can range from 25% to 57%.[29][30] Outcomes following surgery are strongly correlated with the patient's clinical status before surgery but are favorable in over half of the cases.[29][31] Recommendations are, therefore, that in the absence of multiple comorbidities, surgical intervention should be pursued even in patients with poor preoperative neurologic status.
Complications
Significant cerebellar hemorrhage may have peri-hemorrhagic edema and mass effect, which, unfortunately, can cause multiple complications, including brainstem compression, cerebellar herniation, compression of the fourth ventricle with resultant obstructive hydrocephalus, an extension of hemorrhage into the ventricular system, and recurrent hemorrhage typically within the first 24 hours. There are two options for managing the mass effect from the cerebellar hemorrhage: (1) hyperosmolar agents or (2) decompressive surgery.
Osmolar therapy is used to reduce the space-occupying effects of hemorrhage and edema by increasing serum osmolality and facilitating an osmotic movement of water into the vasculature with resultant reactive vasoconstriction. The goal is an overall reduction in intracranial pressure and tissue shrinkage. There is no superiority of hypertonic saline over mannitol or vice versa for the treatment of intracranial hemorrhage. Hypertonic saline concentrations typically utilized for treatment are 3% (250 mL bolus), 10% (75 to 150 mL bolus), and 23.4% (30 mL bolus). Boluses and continuous infusions have the goal of sodium levels of 145 to 155 mmol/L and osmolality of 310 to 320 mOsm/kg.[32] Complications may occur with infusions such as hypotension, pulmonary edema, heart failure, coagulopathy, hypokalemia, intravascular hemolysis, and encephalopathy, but these are rare.[33] Mannitol is a sugar alcohol that acts as a diuretic and is usually administered as a 1 to 2 g/kg bolus (20% concentration) with additional doses of 0.5 g/kg every 4 to 6 hours.[34][35] It is imperative to maintain euvolemia during its administration, and caution is advised in patients with renal failure as the mannitol may lead to fluid overload, necessitating dialysis shortly after administration. Serum osmolality should remain at less than 320 mOsm/kg to prevent renal toxicity.
Decompressive surgery of choice is a suboccipital craniectomy with hematoma evacuation.[36][37] The surgical option is necessary when the patient's neurologic status continues to decline due to brainstem compression or obstructive hydrocephalus, and it appears secondary to the mass effect of the hemorrhage and peri-hemorrhagic edema. An external ventricular drain (EVD) may be used to treat the obstructive hydrocephalus as an alternative to surgery or in addition to surgery. Criteria used to select patients for surgery and/or EVD placement have their basis on both clinical presentation and radiographic features such as the size of the hematoma, ventricular extension, hydrocephalus, brainstem compression, and cisternal effacement.[38][39] Hemorrhages less than 3 cm in diameter without evidence of brainstem compression or hydrocephalus may be treated with close observation in an intensive care setting without surgery. A stereotactic burr-hole aspiration is an option for patients with smaller hemorrhages.[40]
Deterrence and Patient Education
Most cerebellar hemorrhages are hypertensive in origin. Patients suffering from hypertension should receive an education so that they are aware of all the potential risks and complications associated with poor control of their disease process. These patients should be encouraged to seek medical attention urgently if they develop worrisome symptoms.
Enhancing Healthcare Team Outcomes
The diagnosis and management of a cerebellar hemorrhage are with an interprofessional team that includes a combination of the following: emergency clinician, neurosurgeon, neurologist, primary care provider, intensivist, and acute practice provider. The nurses who usually monitor these patients have specialty training in neuroscience and know what signs and symptoms to watch for the progression of the disorder. They must discuss abnormal findings with the clinicians as quickly as possible. The interprofessional team also includes providers and pharmacists, which is considered the best approach to the management of these cases for optimal care and outcomes. The presentation of cerebellar hemorrhage may be subtle to a patient in extremis and is often not easy, requiring intensive management and treatment. The majority of patients are managed in a critical care setting with frequent neurologic assessments, blood pressure control, electrolyte, and intravenous fluid management, and supportive care. Management requires treatment with multiple pharmacologic agents. The pharmacist should manage medication reconciliation and consider potential drug interactions reporting to the team concerning drug interactions. [Level 5]
The outcome depends on the severity of the bleeding, the presence of neurological deficit, the age of the patient, and other associated co-morbidity. An interprofessional team approach to the evaluation and education of the patient and family will lead to the best outcomes.
Media
(Click Image to Enlarge)
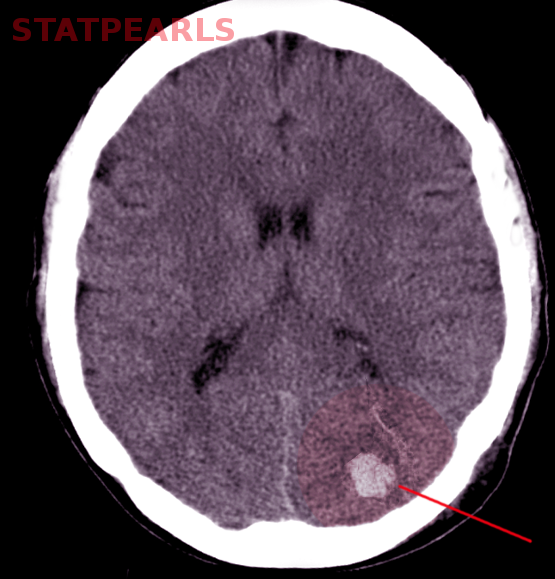
Cerebellar hemorrhage Image courtesy S Bhimji MD
(Click Image to Enlarge)

Cerebellar hematoma Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)
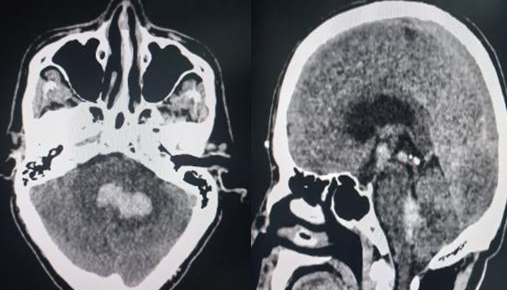
Cerebellar hematoma Contributed by Sunil Munakomi, MD
References
Datar S, Rabinstein AA. Cerebellar hemorrhage. Neurologic clinics. 2014 Nov:32(4):993-1007. doi: 10.1016/j.ncl.2014.07.006. Epub 2014 Sep 11 [PubMed PMID: 25439293]
Itoh Y, Yamada M, Hayakawa M, Otomo E, Miyatake T. Cerebral amyloid angiopathy: a significant cause of cerebellar as well as lobar cerebral hemorrhage in the elderly. Journal of the neurological sciences. 1993 Jun:116(2):135-41 [PubMed PMID: 8336159]
Satoh K, Satomi J, Nakajima N, Matsubara S, Nagahiro S. Cerebellar hemorrhage caused by dural arteriovenous fistula: a review of five cases. Journal of neurosurgery. 2001 Mar:94(3):422-6 [PubMed PMID: 11235946]
Level 3 (low-level) evidenceKim MS, Kim SW, Chang CH, Kim OL. Cerebellar pilocytic astrocytomas with spontaneous intratumoral hemorrhage in adult. Journal of Korean Neurosurgical Society. 2011 Jun:49(6):363-6. doi: 10.3340/jkns.2011.49.6.363. Epub 2011 Jun 30 [PubMed PMID: 21887396]
Level 3 (low-level) evidenceMesiwala AH, Avellino AM, Roberts TS, Ellenbogen RG. Spontaneous cerebellar hemorrhage due to a juvenile pilocytic astrocytoma: case report and review of the literature. Pediatric neurosurgery. 2001 May:34(5):235-8 [PubMed PMID: 11423772]
Level 3 (low-level) evidenceCordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet (London, England). 2018 Oct 6:392(10154):1257-1268. doi: 10.1016/S0140-6736(18)31878-6. Epub [PubMed PMID: 30319113]
Friedman JA, Piepgras DG. Remote cerebellar hemorrhage. Journal of neurosurgery. 2002 Aug:97(2):498-9; author reply 499 [PubMed PMID: 12186489]
Level 3 (low-level) evidenceFeigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. The Lancet. Neurology. 2009 Apr:8(4):355-69. doi: 10.1016/S1474-4422(09)70025-0. Epub 2009 Feb 21 [PubMed PMID: 19233729]
Level 1 (high-level) evidenceSteiner T, Al-Shahi Salman R, Ntaios G. The European Stroke Organisation (ESO) guidelines. International journal of stroke : official journal of the International Stroke Society. 2014 Oct:9(7):838-9. doi: 10.1111/ijs.12369. Epub [PubMed PMID: 25231578]
Broderick JP, Brott T, Tomsick T, Miller R, Huster G. Intracerebral hemorrhage more than twice as common as subarachnoid hemorrhage. Journal of neurosurgery. 1993 Feb:78(2):188-91 [PubMed PMID: 8421201]
Stein M, Misselwitz B, Hamann GF, Scharbrodt W, Schummer DI, Oertel MF. Intracerebral hemorrhage in the very old: future demographic trends of an aging population. Stroke. 2012 Apr:43(4):1126-8. doi: 10.1161/STROKEAHA.111.644716. Epub 2012 Jan 26 [PubMed PMID: 22282880]
Flaherty ML, Woo D, Haverbusch M, Sekar P, Khoury J, Sauerbeck L, Moomaw CJ, Schneider A, Kissela B, Kleindorfer D, Broderick JP. Racial variations in location and risk of intracerebral hemorrhage. Stroke. 2005 May:36(5):934-7 [PubMed PMID: 15790947]
Garcia JH, Ho KL. Pathology of hypertensive arteriopathy. Neurosurgery clinics of North America. 1992 Jul:3(3):497-507 [PubMed PMID: 1633473]
Friedman JA, Piepgras DG, Duke DA, McClelland RL, Bechtle PS, Maher CO, Morita A, Perkins WJ, Parisi JE, Brown RD Jr. Remote cerebellar hemorrhage after supratentorial surgery. Neurosurgery. 2001 Dec:49(6):1327-40 [PubMed PMID: 11846932]
Level 2 (mid-level) evidenceGupta R, Phan CM, Leidecker C, Brady TJ, Hirsch JA, Nogueira RG, Yoo AJ. Evaluation of dual-energy CT for differentiating intracerebral hemorrhage from iodinated contrast material staining. Radiology. 2010 Oct:257(1):205-11. doi: 10.1148/radiol.10091806. Epub 2010 Aug 2 [PubMed PMID: 20679449]
Level 2 (mid-level) evidenceWijdicks EF, Sheth KN, Carter BS, Greer DM, Kasner SE, Kimberly WT, Schwab S, Smith EE, Tamargo RJ, Wintermark M, American Heart Association Stroke Council. Recommendations for the management of cerebral and cerebellar infarction with swelling: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014 Apr:45(4):1222-38. doi: 10.1161/01.str.0000441965.15164.d6. Epub 2014 Jan 30 [PubMed PMID: 24481970]
Anderson CS, Heeley E, Huang Y, Wang J, Stapf C, Delcourt C, Lindley R, Robinson T, Lavados P, Neal B, Hata J, Arima H, Parsons M, Li Y, Wang J, Heritier S, Li Q, Woodward M, Simes RJ, Davis SM, Chalmers J, INTERACT2 Investigators. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. The New England journal of medicine. 2013 Jun 20:368(25):2355-65. doi: 10.1056/NEJMoa1214609. Epub 2013 May 29 [PubMed PMID: 23713578]
Level 1 (high-level) evidenceArima H, Anderson CS, Wang JG, Huang Y, Heeley E, Neal B, Woodward M, Skulina C, Parsons MW, Peng B, Tao QL, Li YC, Jiang JD, Tai LW, Zhang JL, Xu E, Cheng Y, Morgenstern LB, Chalmers J, Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial Investigators. Lower treatment blood pressure is associated with greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension (Dallas, Tex. : 1979). 2010 Nov:56(5):852-8. doi: 10.1161/HYPERTENSIONAHA.110.154328. Epub 2010 Sep 7 [PubMed PMID: 20823381]
Level 1 (high-level) evidenceMorgenstern LB, Hemphill JC 3rd, Anderson C, Becker K, Broderick JP, Connolly ES Jr, Greenberg SM, Huang JN, MacDonald RL, Messé SR, Mitchell PH, Selim M, Tamargo RJ, American Heart Association Stroke Council and Council on Cardiovascular Nursing. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2010 Sep:41(9):2108-29. doi: 10.1161/STR.0b013e3181ec611b. Epub 2010 Jul 22 [PubMed PMID: 20651276]
Schwarz S, Häfner K, Aschoff A, Schwab S. Incidence and prognostic significance of fever following intracerebral hemorrhage. Neurology. 2000 Jan 25:54(2):354-61 [PubMed PMID: 10668696]
Level 2 (mid-level) evidenceWu YT, Li TY, Lu SC, Chen LC, Chu HY, Chiang SL, Chang ST. Hyperglycemia as a predictor of poor outcome at discharge in patients with acute spontaneous cerebellar hemorrhage. Cerebellum (London, England). 2012 Jun:11(2):543-8. doi: 10.1007/s12311-011-0317-7. Epub [PubMed PMID: 21975857]
Level 2 (mid-level) evidenceKimura K, Iguchi Y, Inoue T, Shibazaki K, Matsumoto N, Kobayashi K, Yamashita S. Hyperglycemia independently increases the risk of early death in acute spontaneous intracerebral hemorrhage. Journal of the neurological sciences. 2007 Apr 15:255(1-2):90-4 [PubMed PMID: 17350046]
Godoy DA, Di Napoli M, Rabinstein AA. Treating hyperglycemia in neurocritical patients: benefits and perils. Neurocritical care. 2010 Dec:13(3):425-38. doi: 10.1007/s12028-010-9404-8. Epub [PubMed PMID: 20652767]
Finfer S,Chittock DR,Su SY,Blair D,Foster D,Dhingra V,Bellomo R,Cook D,Dodek P,Henderson WR,Hébert PC,Heritier S,Heyland DK,McArthur C,McDonald E,Mitchell I,Myburgh JA,Norton R,Potter J,Robinson BG,Ronco JJ, Intensive versus conventional glucose control in critically ill patients. The New England journal of medicine. 2009 Mar 26; [PubMed PMID: 19318384]
Level 1 (high-level) evidenceNICE-SUGAR Study Investigators for the Australian and New Zealand Intensive Care Society Clinical Trials Group and the Canadian Critical Care Trials Group, Finfer S, Chittock D, Li Y, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Hebert P, Henderson W, Heyland D, Higgins A, McArthur C, Mitchell I, Myburgh J, Robinson B, Ronco J. Intensive versus conventional glucose control in critically ill patients with traumatic brain injury: long-term follow-up of a subgroup of patients from the NICE-SUGAR study. Intensive care medicine. 2015 Jun:41(6):1037-47. doi: 10.1007/s00134-015-3757-6. Epub 2015 Jun 19 [PubMed PMID: 26088909]
Sjöblom L, Hårdemark HG, Lindgren A, Norrving B, Fahlén M, Samuelsson M, Stigendal L, Stockelberg D, Taghavi A, Wallrup L, Wallvik J. Management and prognostic features of intracerebral hemorrhage during anticoagulant therapy: a Swedish multicenter study. Stroke. 2001 Nov:32(11):2567-74 [PubMed PMID: 11692018]
Level 2 (mid-level) evidenceSiegal DM, Garcia DA, Crowther MA. How I treat target-specific oral anticoagulant-associated bleeding. Blood. 2014 Feb 20:123(8):1152-8. doi: 10.1182/blood-2013-09-529784. Epub 2014 Jan 2 [PubMed PMID: 24385535]
Pernod G, Albaladejo P, Godier A, Samama CM, Susen S, Gruel Y, Blais N, Fontana P, Cohen A, Llau JV, Rosencher N, Schved JF, de Maistre E, Samama MM, Mismetti P, Sié P, Working Group on Perioperative Haemostasis. Management of major bleeding complications and emergency surgery in patients on long-term treatment with direct oral anticoagulants, thrombin or factor-Xa inhibitors: proposals of the working group on perioperative haemostasis (GIHP) - March 2013. Archives of cardiovascular diseases. 2013 Jun-Jul:106(6-7):382-93. doi: 10.1016/j.acvd.2013.04.009. Epub 2013 Jun 25 [PubMed PMID: 23810130]
Dammann P, Asgari S, Bassiouni H, Gasser T, Panagiotopoulos V, Gizewski ER, Stolke D, Sure U, Sandalcioglu IE. Spontaneous cerebellar hemorrhage--experience with 57 surgically treated patients and review of the literature. Neurosurgical review. 2011 Jan:34(1):77-86. doi: 10.1007/s10143-010-0279-0. Epub 2010 Aug 10 [PubMed PMID: 20697766]
Yanaka K, Meguro K, Fujita K, Narushima K, Nose T. Postoperative brainstem high intensity is correlated with poor outcomes for patients with spontaneous cerebellar hemorrhage. Neurosurgery. 1999 Dec:45(6):1323-7; discussion 1327-8 [PubMed PMID: 10598699]
Level 3 (low-level) evidenceOtt KH, Kase CS, Ojemann RG, Mohr JP. Cerebellar hemorrhage: diagnosis and treatment. A review of 56 cases. Archives of neurology. 1974 Sep:31(3):160-7 [PubMed PMID: 4546748]
Level 3 (low-level) evidenceHauer EM, Stark D, Staykov D, Steigleder T, Schwab S, Bardutzky J. Early continuous hypertonic saline infusion in patients with severe cerebrovascular disease. Critical care medicine. 2011 Jul:39(7):1766-72. doi: 10.1097/CCM.0b013e318218a390. Epub [PubMed PMID: 21494103]
Level 2 (mid-level) evidenceZiai WC, Toung TJ, Bhardwaj A. Hypertonic saline: first-line therapy for cerebral edema? Journal of the neurological sciences. 2007 Oct 15:261(1-2):157-66 [PubMed PMID: 17585941]
Videen TO, Zazulia AR, Manno EM, Derdeyn CP, Adams RE, Diringer MN, Powers WJ. Mannitol bolus preferentially shrinks non-infarcted brain in patients with ischemic stroke. Neurology. 2001 Dec 11:57(11):2120-2 [PubMed PMID: 11739839]
Diringer MN,Scalfani MT,Zazulia AR,Videen TO,Dhar R, Cerebral hemodynamic and metabolic effects of equi-osmolar doses mannitol and 23.4% saline in patients with edema following large ischemic stroke. Neurocritical care. 2011 Feb; [PubMed PMID: 21042881]
Level 1 (high-level) evidenceYanaka K, Meguro K, Fujita K, Narushima K, Nose T. Immediate surgery reduces mortality in deeply comatose patients with spontaneous cerebellar hemorrhage. Neurologia medico-chirurgica. 2000 Jun:40(6):295-9; discussion 299-300 [PubMed PMID: 10892265]
Level 2 (mid-level) evidenceKobayashi S, Sato A, Kageyama Y, Nakamura H, Watanabe Y, Yamaura A. Treatment of hypertensive cerebellar hemorrhage--surgical or conservative management? Neurosurgery. 1994 Feb:34(2):246-50; discussion 250-1 [PubMed PMID: 8177384]
Level 2 (mid-level) evidenceTaneda M, Hayakawa T, Mogami H. Primary cerebellar hemorrhage. Quadrigeminal cistern obliteration on CT scans as a predictor of outcome. Journal of neurosurgery. 1987 Oct:67(4):545-52 [PubMed PMID: 3655893]
Luparello V, Canavero S. Treatment of hypertensive cerebellar hemorrhage--surgical or conservative management? Neurosurgery. 1995 Sep:37(3):552-3 [PubMed PMID: 7501127]
Level 3 (low-level) evidenceLee JH, Kim DW, Kang SD. Stereotactic burr hole aspiration surgery for spontaneous hypertensive cerebellar hemorrhage. Journal of cerebrovascular and endovascular neurosurgery. 2012 Sep:14(3):170-4. doi: 10.7461/jcen.2012.14.3.170. Epub 2012 Sep 28 [PubMed PMID: 23210043]