Introduction
The carotid sheath is an important landmark in head and neck anatomy and contains several vital neurovascular structures, including the carotid artery, jugular vein, vagus nerve, and sympathetic plexus (see Image. Carotid Sheath). It extends upwards from the arch of the aorta and terminates at the skull base. While the carotid sheath is rarely the primary disease source, understanding its anatomy is essential for clinicians to address problems that may affect the crucial neurovascular structures that travel through it. See Image. Anatomy of the Carotid Sheath.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The function of the carotid sheath is to separate and help protect the vital structures within it. It facilitates the passage of intrathoracic structures through the neck to terminate in the head and face. It is a fibrous connective tissue sheath encircling several key structures within the neck.[1] These structures include:
- Common carotid artery
- Internal carotid artery
- Internal jugular vein
- Glossopharyngeal nerve (cranial nerve IX)
- Vagus nerve (cranial nerve X)
- Accessory nerve (cranial nerve XI)
- Hypoglossal nerve (cranial nerve XII)
- Sympathetic plexus of nerves
- Deep cervical lymph nodes
The carotid sheath is located posterior to the sternocleidomastoid muscle and is a part of the deep cervical fascia of the neck. Superiorly, the carotid sheath encircles the margins of the carotid canal and the jugular fossa at the skull base. From here, it extends downwards, terminating at the aortic arch. It is divided in the craniocaudal direction into 2 regions, the suprahyoid and infrahyoid spaces, the boundary between which is the bifurcation of the common carotid artery.[2] The immediate relations of the carotid sheath are the pharynx medially, the parotid gland laterally (in the suprahyoid region), the infratemporal fossa anteriorly (in the suprahyoid region), and the prevertebral fascia posteriorly.
Embryology
The carotid sheath, like other fascial tissues, is derived from mesoderm. The adventitia of the cervical great arteries becomes apparent by 15 weeks gestation and is 1 of the earliest components of the fetal deep cervical fascia.[3][4] The carotid sheath does not appear until approximately 20 weeks gestation. Currently, it is fused with the pretracheal fascia but has not yet been integrated into the prevertebral lamina of the deep cervical fascia.[5][6]
Blood Supply and Lymphatics
The 2 vascular structures within the carotid sheath are the common carotid artery, which becomes the external carotid artery, and the internal jugular vein. At the base of the carotid sheath, the common carotid artery arises directly on the left side of the arch of the aorta and directly on the right side of the brachiocephalic trunk. Proximal to its bifurcation, there are no branches from the common carotid artery. The bifurcation of the common carotid artery commonly occurs at the level of the thyroid cartilage (C4 level).
The external carotid artery exits the carotid sheath at this point to travel within the parotid gland. The internal carotid artery continues within the sheath and is initially bulbous as it contains the carotid sinus, a baroreceptor regulating blood pressure, within its arterial wall. The carotid body is a separate structure situated behind the bifurcation. This chemoreceptor is primarily receptive to changes in oxygen partial pressures and is thus involved in respiratory reflexes. The glossopharyngeal and vagus nerves innervate the carotid sinus and the carotid body. The common carotid artery gives off no branches of its own and enters the skull base through the carotid canal in the anteromedial part of the temporal bone.[7]
The internal jugular vein continues the sigmoid sinus and begins its descent towards the heart at the jugular foramen, running with the vagus nerve. It travels within the carotid sheath, lateral to the internal and common carotid arteries in its descent, draining into the subclavian vein and ultimately forming the brachiocephalic vein. While moving posteriorly, the internal jugular vein receives venous blood from the facial, lingual, superior thyroid, and middle thyroid veins. Deep cervical lymph nodes are also contained within the carotid sheath, specifically, those within levels II (upper internal jugular), III (middle internal jugular), and IV (lower internal jugular) of the neck, comprising together the group of nodes termed the deep cervical chain.[8]
Nerves
The nerves that travel within the carotid sheath are the vagus, hypoglossal, accessory cranial nerves, and branches of the ansa cervicalis and sympathetic nerves.
Vagus Nerve
The vagus nerve (CN X) has the longest course of any cranial nerve, beginning by passing through the middle part of the jugular foramen with the internal jugular vein and descending within the carotid sheath. It runs posteriorly and between the carotid artery (initially internal, then common) and the internal jugular vein.[9] Within the neck, the vagus nerve gives off the pharyngeal branch and the superior laryngeal nerve. The pharyngeal branch supplies motor fibers to the pharyngeal muscles, except for the stylopharyngeus. Lesions affecting the pharyngeal branch of the vagus nerve cause deviation of the uvula to the side opposite the injury. The superior laryngeal nerve divides into the internal and external laryngeal nerves. These nerves supply sensory fibers to the larynx above the vocal cord, the lower pharynx, and the epiglottis and taste fibers to the root of the tongue near the epiglottis. Passing into the mediastinum at the root of the neck, the vagus nerve travels anteriorly over the subclavian artery to supply the thoracic and abdominal viscera.
Glossopharyngeal Nerve
The glossopharyngeal nerve (CN IX) descends from the anterior part of the jugular foramen, running within the carotid sheath at the lateral aspect of the carotid artery.[10] It then exits the carotid sheath along the lateral border of the stylopharyngeus muscle (supplying it with a motor branch), behind the external carotid artery, before coursing forward towards the tongue and branching further into pharyngeal, tonsillar, and lingual branches.
Accessory Nerve
The accessory nerve (CN XI) exits the skull base in the middle part of the jugular foramen, sharing a meningeal sleeve with the vagus nerve. It travels in the suprahyoid region of the carotid sheath briefly anteriorly to the internal jugular vein, continuing laterally and exiting the sheath.
Hypoglossal Nerve
The hypoglossal nerve (CN XII) exits the skull base through the hypoglossal canal and descends initially in the carotid sheath posteriorly to the vagus nerve. It then exits the carotid sheath by emerging between the internal carotid artery and the internal jugular vein before traveling on the anterior aspect of the outside, deep to the styloid muscles. In addition, the ansa cervicalis is embedded in the anterior portion of the carotid sheath.
Muscles
As previously stated, the carotid sheath is derived from all 3 layers of the deep cervical fascia. While there are no muscles within the carotid sheath, there are muscles whose relation to the carotid sheath provides valuable landmarks. The sternocleidomastoid muscle forms the anterolateral boundary of the carotid sheath. In the suprahyoid section of the carotid sheath, the stylopharyngeus muscle lies obliquely over the internal carotid artery, and its inferior border is closely associated with the glossopharyngeal nerve as it leaves the sheath. Similarly, inferior to the stylopharyngeus muscle in the suprahyoid region of the carotid sheath, the posterior belly of the digastric muscle lies obliquely over the internal jugular vein and internal carotid artery close to the bifurcation of the common carotid artery [11]. The accessory nerve passes under this muscle as it exits the sheath.
Physiologic Variants
There are no significant physiologic or anatomic variants of the carotid sheath; it can be disrupted or lay in an unusual fascial plane if the common carotid arteries have an atypical course through the neck. Carotid variations are common (ie, the right common carotid branching off the aorta directly.)[12][7] Furthermore, the extracranial course of the cranial nerves traveling in the carotid sheath has significant inter-individual variability, which can provide difficulty when operating within the region [10][11]. Thus, access to the contents of the carotid sheath should be performed with care and can be done with the aid of ultrasound or other imaging if an anatomic variation is suspected.
Surgical Considerations
Carotid Endarterectomy
Carotid endarterectomy is performed to excise atherosclerotic thickening of the intima within the internal carotid artery to reduce strokes in patients with significant carotid artery stenosis (typically greater than 70 to 80% stenosis +/- symptoms). The opening incision is made, and the sternocleidomastoid muscle is retracted. At this point, it is important to visualize the carotid sheath, where the structure is vital to the procedure. The carotid artery lies on the medial side of the internal jugular vein, and the vagus nerve is situated posteriorly. The carotid sheath may also contain the hypoglossal, glossopharyngeal, and accessory nerves. These structures pass horizontally and cross the internal carotid artery. It is important to identify these structures before incising any structure. The surgeon opens the carotid sheath to gain exposure to the common carotid bifurcation, as this is the most common site for atherosclerosis due to non-laminar blood flow. Once access is gained to the carotid sheath and the carotid bifurcation is located, the surgeon removes any atherosclerotic plaque and repairs the vessel. Possible complications include air embolism and laceration of the internal jugular vein or carotid artery.[13][14][15]
Penetrating Neck Trauma
An ongoing debate among trauma surgeons is over a no-zone approach, which leans heavily on multidetector CT angiography, versus a zoned approach to surgical exploration.[16][17]
Zones of the Neck
The neck is divided into 3 zones. These become important when assessing and managing trauma in those with penetrating neck injuries.
- Zone I - cricoid cartilage to the sternal notch: trachea, lung, esophagus, thoracic duct, vertebral arteries, the origin of the common carotid artery, and subclavian vessels, spinal cord, thoracic duct, thyroid gland
- Zone II - cricoid cartilage to the angle of the mandible: carotid sheath and its components (carotid artery, internal jugular vein, vagus nerve), trachea, esophagus, spinal cord, larynx, pharynx
- Zone III - the angle of the mandible to the base of the skull: distal portion of the internal carotid artery, vertebral arteries, jugular veins, pharynx, spinal cord, sympathetic chain, CN IX, X, XI, XII
The decision to surgically explore these areas is based on hard and soft signs. Surgical exploration is the best management course regardless of the zone if the patient becomes unstable.
Soft Signs
- History of arterial bleeding
- Tracheal deviation
- Nonexpanding large hematoma
- Apical capping on chest radiograph
- Stridor
- Hoarseness
- Vocal cord paralysis
- Subcutaneous emphysema
- Facial nerve (cranial nerve VII) injury
- Unexplained bradycardia (without CNS injury)
Hard Signs
- Hypotension
- Active arterial bleeding
- Diminished carotid pulse
- Expanding hematoma
- Audible bruit or palpable thrill
- Neurologic deficit
- Hemothorax greater than 1000 mL
- Air bubbling of wound
- Hemoptysis
- Hematemesis
If the patient presents with hard signs, emergent management is needed (ie, airway and circulation management, immediate decompression, and repair of the injured vessel). Serial physical examination and non-emergent imaging may be appropriate if soft signs are present.
Clinical Significance
Internal Jugular Central Venous Line
An internal jugular central venous line is placed to gain vascular access, enabling venous monitoring and administration of medications and fluid resuscitation. The procedure begins by placing the patient in a slight Trendelenburg and locating the internal jugular vein within the apex of the triangular interval between the clavicular and sternal heads of the sternocleidomastoid muscle. It may help to have the patient turn the head to the contralateral side to visualize these anatomical landmarks better. If the patient is conscious, begin by applying a local anesthetic. Next, posteriorly insert the needle at a 45° angle while applying negative pressure. The needle passes through the carotid sheath, and the internal jugular vein produces blood within the syringe. An ultrasound can help assist with visualization and cannulation and ensure the proper placement of the guide needle into the vein. While keeping the guide needle in place, begin threading the guidewire. Once in place, remove the needle, introduce the dilator, and then the catheter. The catheter should now be within the superior vena cava.[18] It is essential to understand the relationships of the structures within the carotid sheath to properly perform an internal central venous line insertion.
Carotid Body Tumor
Carotid body tumors are typically slow-growing, painless masses found most commonly in the fourth and fifth decades.[8] Given the anatomical relationship of the carotid body within the sheath to these nerves, these tumors may present with lower cranial nerve signs. Although the pathogenesis of these tumors is unclear, they are paragangliomas arising from the neural tissue in the carotid body. Surgical removal is recommended; this involves ligation and bypass of the carotid artery bypass and, as such, is a high-risk procedure.[19]
Lemierre Syndrome
Lemierre syndrome, suppurative jugular thrombophlebitis, is a serious odontogenic or oropharyngeal infection sequela. Infection typically spreads from the lateral pharyngeal space to the carotid sheath, which can seed the internal jugular vein, precipitate septicemia, generate septic emboli, and erode the carotid artery. It is typically due to Fusobacterium or Bacteroides species. While it is uncommon in the antibiotic era, patients with poor dental hygiene and limited access to the healthcare system are still at risk.[20]
Other Issues
The carotid sheath should not be confused with the carotid space or triangle. The carotid space is the anatomic area that the sheath encloses, while the carotid triangle is a specific portion of the anterior aspect of the neck through which the carotid sheath passes.
Media
(Click Image to Enlarge)
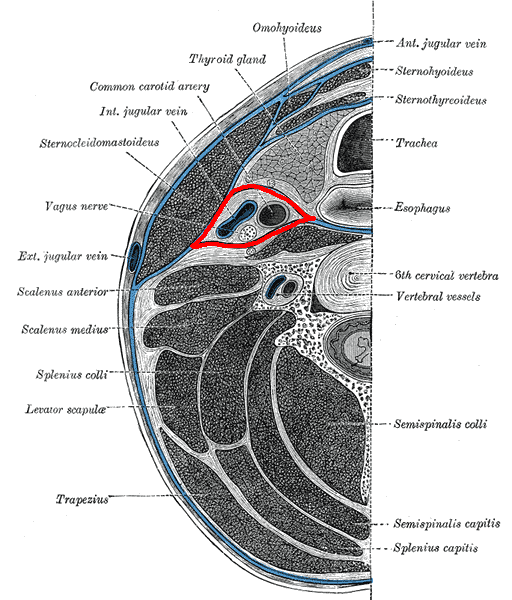
Carotid Sheath. Illustrated image of the axial section of the neck showing carotid sheath.
Mikael Häggström, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
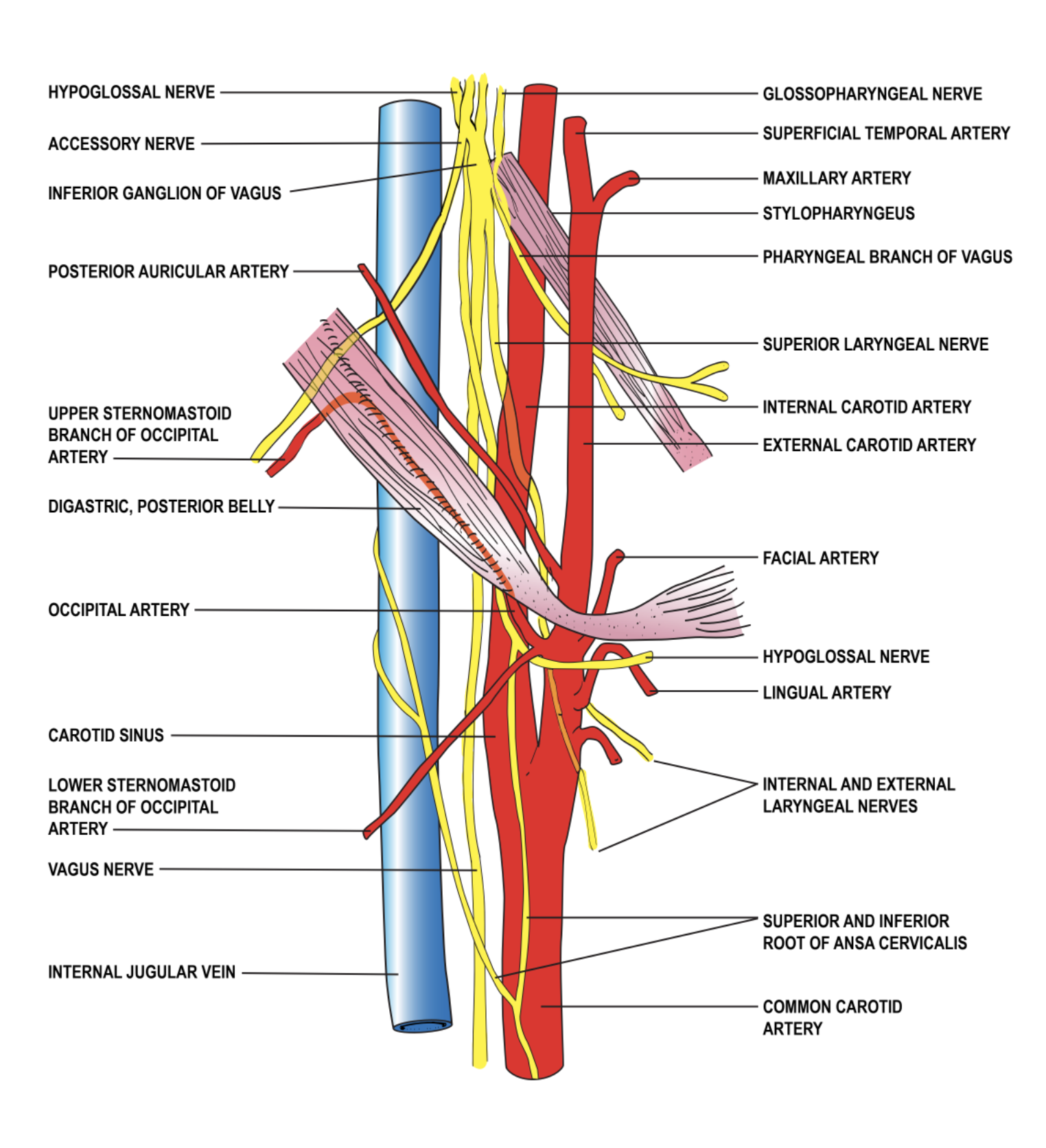
Anatomy of the Carotid Sheath
Illustrated by P Dellavalle
References
Feigl G, Hammer GP, Litz R, Kachlik D. The intercarotid or alar fascia, other cervical fascias, and their adjacent spaces - a plea for clarification of cervical fascia and spaces terminology. Journal of anatomy. 2020 Jul:237(1):197-207. doi: 10.1111/joa.13175. Epub 2020 Feb 20 [PubMed PMID: 32080853]
Gervasio A, D'Orta G, Mujahed I, Biasio A. Sonographic anatomy of the neck: The suprahyoid region. Journal of ultrasound. 2011 Sep:14(3):130-5. doi: 10.1016/j.jus.2011.06.001. Epub 2011 Jun 29 [PubMed PMID: 23396801]
Miyake N, Hayashi S, Kawase T, Cho BH, Murakami G, Fujimiya M, Kitano H. Fetal anatomy of the human carotid sheath and structures in and around it. Anatomical record (Hoboken, N.J. : 2007). 2010 Mar:293(3):438-45. doi: 10.1002/ar.21089. Epub [PubMed PMID: 20169562]
Shvedavchenko AI, Oganesyan MV, Hammer CM, Paulsen F, Bakhmet AA. Ansa cervicalis - A new classification approach. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2019 Mar:222():55-60. doi: 10.1016/j.aanat.2018.10.010. Epub 2018 Nov 17 [PubMed PMID: 30458237]
Rivard AB, Kortz MW, Burns B. Anatomy, Head and Neck: Internal Jugular Vein. StatPearls. 2025 Jan:(): [PubMed PMID: 30020630]
Ii N, Fuwa N, Toyomasu Y, Takada A, Nomura M, Kawamura T, Sakuma H, Nomoto Y. A Novel External Carotid Arterial Sheath System for Intra-arterial Infusion Chemotherapy of Head and Neck Cancer. Cardiovascular and interventional radiology. 2017 Jul:40(7):1099-1104. doi: 10.1007/s00270-017-1635-z. Epub 2017 Mar 29 [PubMed PMID: 28357576]
Baz RA, Scheau C, Niscoveanu C, Bordei P. Morphometry of the Entire Internal Carotid Artery on CT Angiography. Medicina (Kaunas, Lithuania). 2021 Aug 17:57(8):. doi: 10.3390/medicina57080832. Epub 2021 Aug 17 [PubMed PMID: 34441039]
Chengazi HU, Bhatt AA. Pathology of the carotid space. Insights into imaging. 2019 Feb 15:10(1):21. doi: 10.1186/s13244-019-0704-z. Epub 2019 Feb 15 [PubMed PMID: 30771026]
Planitzer U, Hammer N, Bechmann I, Glätzner J, Löffler S, Möbius R, Tillmann BN, Weise D, Winkler D. Positional Relations of the Cervical Vagus Nerve Revisited. Neuromodulation : journal of the International Neuromodulation Society. 2017 Jun:20(4):361-368. doi: 10.1111/ner.12557. Epub 2017 Feb 1 [PubMed PMID: 28145065]
Yigit E, Dursun E, Omeroglu E, Sunter AV, Edizer DT, Terzi S, Coskun ZO, Demirci M. The course of lower cranial nerves within the neck: a cadaveric dissection study. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2018 Oct:275(10):2541-2548. doi: 10.1007/s00405-018-5091-4. Epub 2018 Aug 13 [PubMed PMID: 30105404]
Cavalcanti DD, Garcia-Gonzalez U, Agrawal A, Tavares PL, Spetzler RF, Preul MC. A clear map of the lower cranial nerves at the superior carotid triangle. World neurosurgery. 2010 Jul:74(1):188-94. doi: 10.1016/j.wneu.2010.03.024. Epub [PubMed PMID: 21300012]
Allardyce H, Shepherd E, Bailey EL. Anatomical variation of the aorta in the West of Scotland - A population with high cardiovascular disease burden. Implications for stent design and deployment. Journal of anatomy. 2023 Jan:242(1):112-120. doi: 10.1111/joa.13652. Epub 2022 Mar 17 [PubMed PMID: 35301720]
Melamed H, Harris MB, Awasthi D. Anatomic considerations of superior laryngeal nerve during anterior cervical spine procedures. Spine. 2002 Feb 15:27(4):E83-6 [PubMed PMID: 11840114]
Choi J, Ha DH, Kwon S, Jung Y, Yu J, Kim M, Min K. Needle Entry Angle to Prevent Carotid Sheath Injury for Fluoroscopy-Guided Cervical Transforaminal Epidural Steroid Injection. Annals of rehabilitation medicine. 2018 Dec:42(6):814-821. doi: 10.5535/arm.2018.42.6.814. Epub 2018 Dec 28 [PubMed PMID: 30613074]
Jusufovic M, Skagen K, Krohg-Sørensen K, Skjelland M. Current Medical and Surgical Stroke Prevention Therapies for Patients with Carotid Artery Stenosis. Current neurovascular research. 2019:16(1):96-103. doi: 10.2174/1567202616666190131162811. Epub [PubMed PMID: 30706783]
Doshi PB, Bhatt YC. Passage through the carotid sheath: An alternative path to the pre-spinal route for direct repair of contralateral C7 to the lower trunk in total brachial plexus root avulsion injury. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2016 May-Aug:49(2):159-163 [PubMed PMID: 27833275]
Cheah T, Ha JF. Carotid sheath 'intubation' during an emergency surgical cricothyroidotomy. BMJ case reports. 2016 May 25:2016():. doi: 10.1136/bcr-2016-214898. Epub 2016 May 25 [PubMed PMID: 27226126]
Level 3 (low-level) evidenceLockwood J, Desai N. Central venous access. British journal of hospital medicine (London, England : 2005). 2019 Aug 2:80(8):C114-C119. doi: 10.12968/hmed.2019.80.8.C114. Epub [PubMed PMID: 31437056]
Liu J, Mu H, Zhang W. Diagnosis and treatment of carotid body tumors. American journal of translational research. 2021:13(12):14121-14132 [PubMed PMID: 35035757]
Gore MR. Lemierre Syndrome: A Meta-analysis. International archives of otorhinolaryngology. 2020 Jul:24(3):e379-e385. doi: 10.1055/s-0039-3402433. Epub 2020 Apr 24 [PubMed PMID: 32754251]
Level 1 (high-level) evidence