 Cryoballoon Pulmonary Vein Catheter Ablation of Atrial Fibrillation
Cryoballoon Pulmonary Vein Catheter Ablation of Atrial Fibrillation
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in the United States with about 3 million people reported being diagnosed with the disorder.[1] The prevalence of atrial fibrillation dramatically increases with advancing age. As our population has enjoyed greater longevity, along with the increasing presence of risk factors known associated with atrial fibrillation such as hypertension and obesity, the incidence and prevalence of AF is expected to continue to increase.[2]
There is significant morbidity associated with the development and perpetuation of AF, including stroke, heart failure, cognitive impairment, renal failure, increased mortality and a negative impact to the quality of life.[3] As such, controlling the arrhythmia is often essential to patient quality of life and prognosis, but has been difficult to attain.
Since Haussaiguarre et al. reported that AF most often began in the posterior left atrium surrounding the ostia of the pulmonary veins,[4] pulmonary vein electrical isolation via catheter ablation has been the cornerstone of nonpharmacological treatment of AF. Treatment of AF may be medical or surgical, depending on patient characteristics, duration of disease, symptoms, and patient preference. The two most frequently used energy sources used for ablation are electrocautery (known as radio-frequency), and cryoenergy,[5]; although other energy sources are being actively investigated for their efficacy and safety. Both methods have been employed during open-heart surgery with equal efficacy.[6] Catheter radiofrequency ablation, where electrocautery is delivered to the tip of a steerable wire, has been used to treat cardiac arrhythmias since the 1980s.[7] Catheter cryoablation, where liquid nitrogen is introduced to scar arrhythmic cardiac tissue, was more recently introduced to deliver less severe burns and thus a more controlled degree of injury.[7] It is most widely used in pediatrics due to the ability to reverse its effects if not applied for a long period due to its slow injury rate.[8]
As radio-frequency energy has been the primary energy source used to electrically isolate all four pulmonary veins,[9] an extensive number of ablation lesions are needed to be delivered by wire to encircle the vein ostia. This posed a challenge of completely encircling the peri-ostial pulmonary veins to produce complete conduction block, leaving gaps in the ablation lines and less control in the degree of injury delivered, which could lead to injury to contiguous structures such as the esophagus.[10] In 2012 the FDA approved a multicenter examination of second-generation cryoballoon which is delivered through a catheter over a wire and can deliver a continuous encircling freeze lesion to the left atrial tissue surrounding the ostia of the pulmonary veins, thus being more consistent in ablation delivery and being less prone to gaps in the ablation field.[11] Cryoenergy's greater lesion control should also theoretically have less risk to injure deeper tissues and thus, safer.[12] A large multicenter trial in Europe showed both methods were equally effective in electrically isolating pulmonary veins and were equally effective in preventing recurrent atrial fibrillation.[13] This activity reviews the methodology of catheter cryoballoon ablation using a multicenter examination of second-generation cryoballoon to treat symptomatic AF and its expected outcomes and risks.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Before outlining methods to produce electrical pulmonary vein isolation an understanding of the left atrium and pulmonary venous anatomy, variants, and anomalies and how it relates to the cardiac conduction system is essential. Oxygenated blood returning to the heart enters the left atrium via pulmonary veins. In 60% of patients, there are 4 distinct pulmonary vein ostia.[14] The most common variant anatomy is a left common pulmonary vein trunk, followed by a right middle pulmonary vein. The right pulmonary veins lie posterior to the right atrium, and the left pulmonary veins are located between the descending aorta and left atrial appendage. The right and left superior pulmonary veins project forward and upward, whereas the right and left inferior pulmonary veins usually project backward and downward.[14] Extending onto and around the pulmonary veins are sleeves of cardiac tissue originating from the atria and cava. These sleeves are formed by fascicles of fibers running peripherally around the area of the openings of the pulmonary veins, with fibers continuing off these fascicles to immediately surround the ostia forming sphincter-like structures, but also extending somewhat up the veins, contributing to the formation of myocardial sleeves.[15] The coronary sinus drains 85% of the cardiac venous flow into the RA; surrounding this sinus are muscular bundles of fascicles that extend to the LA serving as interatrial electrical conduits.[15] In comparison to left atrial myocytes, it is believed that pulmonary vein myocytes are prone to arrhythmogenesis secondary to their shorter refractoriness and increased triggered activity, while the muscular sleeves at the atrial-pulmonary venous junction have a propensity for re-entry circuits.[16] In addition, there are also several autonomic ganglia at the pulmonary venous and left atrial junction which have been found to spontaneously induce AF in mice introduced with parasympathomimetics, suggesting a hyperactive autonomic system may play a role in AF.[17] Thus, catheter ablation to electrically isolate the pulmonary veins should be able to prevent atrial fibrillation by preventing propagation of ectopic electrical activity into the atrium, reducing the amount of mass available for propagation of the foci, and/or partially interrupting vagal stimulation to the heart.[18]
Indications
The primary selection criterion for ablation of atrial fibrillation is symptomatic AF.[19] The 2017 Expert Consensus Document on Catheter Ablation of Atrial fibrillation states as a Class I recommendation, ablation of paroxysmal AF refractory to at least one Class I or III antiarrhythmic medication. There is less consensus for the use of catheter ablation as first-line therapy for paroxysmal or persistent AF, carrying a class IIa recommendation.[19] In long-standing persistent atrial fibrillation, catheter ablation carries a class IIB recommendation, where there is less evidence of its impact on long-term prognosis. For patients with any AF who have not been placed on at least one antiarrhythmic drug, catheter ablation as first-line is still a class II recommendation.[19] Although the recently reported CABANA trial[20] did show a statistical benefit of catheter ablation as first-line therapy for AF in patients under 75 years and minorities who received the therapy, there was no difference in the 5-year survival or cardiovascular events comparing primary catheter ablation versus antiarrhythmic drug therapy when considered as an intention to treat. Other reasonable indications (Class II recommendations) for ablation of AF include age younger than 75, heart failure, the presence of hypertrophic cardiomyopathy, tachycardia-bradycardia syndrome to avoid a pacemaker, and competitive athletes.[19] Asymptomatic patients could be candidates after careful discussion and consideration by the patient although there is not sufficient data to indicate a survival benefit. Professionals hope that such data will be forthcoming as the results of the CABANA trial are uncovered.
Contraindications
The presence of a left atrial thrombus is an absolute contraindication to catheter ablation for AF as this may cause embolism of the thrombus into the arterial system. There is no large-scale data yet that has shown catheter ablation of atrial fibrillation mitigates stroke risk. Thus, patients not amenable to anti-coagulation represent a relative contraindication to this procedure.[19]
Technique or Treatment
Cryoballoon catheter pulmonary vein electrical isolation is performed along with a full diagnostic cardiac electrophysiology study. Such procedures are performed in either a dedicated cardiac electrophysiology laboratory, which is preferred or in a cardiac catheterization laboratory. Either must have a cine-fluoroscopy capability that can save images for review as well as a recording system for simultaneous surface 12-lead ECG and multiple intracardiac electrograms. The lab must be able to perform intravenous (IV) contrast dye injections as well as record multiple pressure waveforms to facilitate transeptal catheterization. Intracardiac ECHO (ICE) is used extensively to assist in transeptal catheterization as well as rule out atrial thrombi and recreate real-time images of the patient’s left atrial anatomy. This can be imported into a 3-dimensional imaging program to identify variants in left atrial anatomy to guide the procedure. Certain laboratories will obtain preoperative CT or MR angiograms, but these are inaccurate unless they are obtained in real-time during the procedure as the left atrial volume can change dramatically with changes in patient hydration and cardiac rhythm. Intraoperative ECHO can also minimize the need for contrast dye, and reports have been published of completely fluoro-less cryoballoon pulmonary vein isolation.[21] ICE using color flow Doppler can inform the operator of regions of inadequate occlusion at the vein ostia, thus resulting in inadequate freezing of the tissue without necessitating repeated venograms to test for adequate circumferential occlusion, which is necessary to deliver continuous cryoinjury surrounding the pulmonary veins.
In 2012, the second-generation cryoballoon was approved by the FDA for the use of percutaneous catheter ablation. It has undergone a 2-generation evolution that now comes equipped with an 8-pole circular recording catheter compatible with the balloon. Begin by inserting 5 introducer sheaths via the femoral venous approach. Patients are premedicated with oral anticoagulation, either with warfarin or a direct oral anticoagulant, for at least 2 weeks prior to the procedure, and the medication is held for a single dose. In the right femoral vein, place an 8-Fr sheath that will act as access for the transeptal sheath, and a 5-Fr sheath that will act as access for a 5-Fr quadripolar catheter, with 5-mm spacing. The catheter will initially be placed in the high right atrium near the RA/SVC border for recording and pacing if the patient is not in atrial fibrillation at the time of the procedure. It can then be passed to the junction of the SVC and right subclavian vein to pace the right phrenic nerve during cryoablation to the right pulmonary veins. This allows for monitoring for phrenic nerve injury during application of the balloon to those veins. Three introducer sheaths are placed in the left femoral vein acting as access for: (1) a 6-Fr hexapolar catheter for recording and locating the His-bundle site, a fluoroscopic marker of the tricuspid valve anteriorly, helping to locate the fossa ovalis for transeptal access; (2) a 6 Fr decapolar catheter to record and pace the coronary sinus; and (3) a pulse wave ICE catheter, which can remain in the right atrium but record anatomy of all cardiac structures.
If the patient is in sinus rhythm, a full diagnostic study is performed first to rule out a reentrant supraventricular tachycardia (SVT) or a concealed accessory pathway. If none are found, we proceed directly to transseptal catheterization. Start by exchanging the 8-Fr introducer sheath in the right femoral vein for a transseptal sheath, and utilize a radiofrequency transseptal needle to cross the septum posteriorly and somewhat low in the fossa ovalis, to improve the ability to manipulate the cryoballoon to the right pulmonary veins when needed. The needle in the transseptal sheath is exposed and visualized using ICE and/or fluoroscopy. Radiofrequency/electrocautery is delivered to 10 watts for 2 seconds when the intracardiac ECHO confirms the proper location. The needle should be pointing at the left pulmonary veins when entering the left atrium (see figure). On fluoroscopy in the 30-degree LAO position, the needle will face parallel to the coronary sinus catheter but posterior (away from) to the catheter recording the His-bundle.
Patients are treated with heparin 1500 IU per hour at the start of the procedure, but once across the septum, the patient immediately receives a heparin bolus of 200 IU/kg, and a continuous drip is maintained at 20 IU per hour to assure the ACT is kept greater than 300 seconds throughout the rest of the procedure. ACT measurements are drawn every 15 minutes while any catheter remains across the interatrial septum. The needle is removed, and a 210-cm exchange stiff J-wire is then passed as deep as possible into preferably a superior branch of the left superior pulmonary vein. The preformed guiding sheath is then removed leaving the wire in position. If the left superior vein is too difficult to cannulate, the wire can be placed deep into the left inferior vein or right superior vein. This way the path across the atrial septum is the straightest when passing the larger cryoballoon flex sheath steerable through the fossa.
The insertion site in the right femoral vein is then gradually enlarged using a 12 Fr introducer and then exchanged over the stainless steel wire with a flat-wire coil and PTFE coating with the larger 14-Fr cryoballoon steerable delivery flex sheath. The sheath is then passed across the fossa slowly so as not to dislodge the wire from the anchored pulmonary vein. The dilator and sheath can be steered up and down to ease the passing through the fossa ovalis, which can be viewed under fluoroscopy and ICE. The sheath is then passed first into the left superior pulmonary vein over the stainless steel wire with a flat-wire coil and PTFE coating. The tip of the sheath is positioned at the PV os, and the sheath’s dilator and the wire are withdrawn, and the sheath is then continuously flushed using an irrigation pump at 2 mL per hr.
At this point, the appropriately sized cryoballoon (either 23 or 28 mm in diameter) is chosen based on measurements of the PV ostia diameter taken via ICE. Use the 28-mm balloon universally except when one of the veins bifurcates very shallow preventing the larger balloon from sitting adequately, preventing complete occlusion of the vein. The cryoballoon is then flushed manually, twice forward as well as backward, through the connection, to ensure all air-bubbles have been eliminated. The 22-mm diameter mapping loop catheter is then inserted, and the cryoballoon is again flushed manually, twice forward and backward. The balloon is inserted into the introducer sheath for only approximately 1 to 3 cm, and then 10 to 20 mL of blood is withdrawn from the sheath before further introducing the cryoballoon, until no air bubbles are detected, to completely bathe the balloon in blood before passing into the sheath further to prevent advancement of air bubbles.
The cryoballoon is then inserted until its tip is at the tip of the sheath, which can be denoted by the indicator on the cryoballoon reaching the entrance to the sheath. The 8-pole circular catheter is then pushed forward and exposed, and intracardiac electrogram recordings of the electrical activity of the PV os (PV potentials) are visualized (see figure). If the patient is in sinus rhythm, pacing around the vein at 5 mA ensues to confirm baseline PV conduction to the left atrium performed before ablation. After this, the cryoballoon is inflated within the body of the atrium first, and liquid nitrogen is allowed to fill the balloon and chill to 0 C, after which it is then manually deflated to remove any humidity that may have built up within the balloon or hoses attached. After this, the cryoballoon is once again inflated and advanced and pressed against the ostium of the superior PV. A 50/50 mixture of IV dye and saline is then flushed into the tip of the balloon to demonstrate that no, or minimal, leaks surrounding the balloon are present. If complete occlusion is achieved, keeping constant heavy forward pressure on the balloon, cryoablation is then initiated. A drop in temperature of 1 C per second is ideal for the first 30 seconds. At 1 minute of cryoablation, the end-tidal CO2 (ETCO2) pressure is measured. Loss of PVP on IEGM recording, a drop of ETCO2 by 4 mm Hg from baseline, and a nadir temperature of -50 dC all are indicators of successful, durable PV electrical isolation (Kroman, et al). Goal temperature troughs should be less than -40 C as lower temperatures coupled with tighter occlusions are predictive of PVI. A study by Furnkranz et al demonstrated that a minimal cryoablation temperature of less than -51 C was invariably associated with PVI. After 120 seconds of freezing, a CBT of equal to -36 C/-33 C (superior/inferior PVs) predicted failed PVI with 97%/95% specificity.[22] If PVPs are eliminated with 1 minute, cryoablation is delivered for 3 minutes. If they are not eliminated after 1 minute, cryoablation is delivered for 4 minutes. An additional application for 3 minutes is then delivered, after allowing the balloon to thaw following the application that eliminated PV electrical activity fully. A freeze-thaw-freeze approach is commonly practiced, although a single 240-ms freezing cycle may also be used. A thaw time of 1 minute or greater indicates a successful application to produce PV isolation of that vein.
During PV cryoablation, the esophageal temperature is continuously monitored with an esophageal probe that is moved up or down by anesthesia to position the sensor equidistant to the balloon. Thus, this procedure must be performed under general anesthesia with no paralytic agents given so as not to impact the ability to test phrenic nerve function during cryoablation to the right pulmonary veins. Cryoablation is performed stepwise starting with the left superior pulmonary vein, the left inferior pulmonary vein, the right inferior pulmonary and last, the right superior pulmonary vein. Phrenic nerve function is closely monitored when delivering cryoablation to the right pulmonary veins because of the proximity of the path of the right phrenic nerve to the right pulmonary veins ostia. One monitors the right phrenic nerve function using the quadripolar right atrial catheter by repositioning the catheter to the junction of the right subclavian vein and superior vena cava and deliver bipolar stimulation at high output pacing at 50 bpm. At the same time, one should use the tactile feel of the abdomen as well as C-MAP recording (recording the muscle action potential across the diaphragm through the skin) to monitor the phrenic nerve function during application of cryotherapy to the right pulmonary veins.
Once all PVPs are confirmed to be eliminated 30 minutes after the last application to the veins, if the patient is in sinus rhythm, programmed stimulation is performed to atrial refractoriness, and burst at 230 ms (atrial rate of 260 bpm) is delivered at the coronary sinus os to try to re-induce an atrial tachyarrhythmias. If none is induced, no further ablation is performed. If an atrial flutter that sustains greater than 10 minutes is induced, we will remove the balloon catheter and insert an 8-mm tip or 3.5-mm tip irrigation RF ablation catheter to intracardiac map and ablate the flutter. 3-dimensional electroanatomic mapping guides locating the reentrant circuit. If the patient is in sustained AF after PVI, we electrically cardiovert them and assure entrance and exit block at the vein ostia by pacing inside and outside all the PVs.
Once the ablation catheter and sheath are retracted into the venous system, anticoagulation is reversed with protamine, but oral anticoagulation continues uninterrupted.
Complications
In a worldwide survey of 7000 patients who had undergone catheter ablation, complications included cardiac tamponade, thromboembolism causing cerebrovascular accidents, atrioesophageal fistula, pulmonary vein stenosis, and nerve injury-either phrenic or periesophageal vagal nerve.[23] The rate of death was .98 per 1000 patients. Less prevalent causes of death described in the study included myocardial infarction, torsades de pointes, septicemia, sudden respiratory arrest, extrapericardial pulmonary vein perforation, hemothorax, anaphylaxis, esophageal perforation from an intraoperative esophageal probe, and hematoma formation at the site of entry.[23] Ablation may be proarrhythmic itself and may lead to other tachyarrhythmias post-ablation. Exclusive to cryoballoon ablation and the most common complication is phrenic nerve palsy, due to its proximity to the right superior or inferior pulmonary veins.[24] This can be avoided by immediately stopping delivery of cryo energy, and immediately deflating the balloon by tapping the "stop cryo-ablate" button twice, at the first detection of loss of strength of diaphragmatic excursion by palpation or loss in amplitude of C-MAP on the surface ECG. The rate of pulmonary vein stenosis is less common in cryoablation.[25] Although cryoballoon ablation is considered less technically challenging compared to radiofrequency catheter ablation, more radiation is often required during cryoablation as cineangiography is often used to confirm complete PV ostial occlusion by the balloon, necessary for optimal freezing.[26]
Clinical Significance
In the Sustained Treatment of Paroxysmal Atrial Fibrillation (STOP-AF) trial, 245 patients were randomized to either cryoballoon-based PV isolation with the first-generation cryoballoon or antiarrhythmic drug therapy. At 12 months of follow-up, 69.9% of the cryoballoon group versus 7.3% of the drug therapy group, were free of recurrent AF (p < 0.001).[27] Moreover, there was a statistically significant improvement in symptoms and quality of life in the cryoablation group. For all quality-of-life metrics, the improvement was greater in the cryoballoon group when compared to the drug therapy group.[27] In the largest systematic review of studies reporting on cryoballoon PVI ablation for all types of AF, cryoballoon ablation alone (without focal ablation) resulted in PVI in 93% of targeted veins. When using a prespecified exclusive cryoballoon ablation strategy, a 99% complete PVI rate was achieved. The rates were higher in studies using intracardiac or transesophageal echocardiography.[28] Excluding a 3-month blanking period (a time during which episodic arrhythmias are not considered important to long-term recurrences), the 1year freedom from recurrent Atrial Fibrillation was 73%. This is relatively high compared to RF catheter ablation, which has freedom from recurrence rates of 50% to 64%.[29]
Because of its historical development, radiofrequency ablation is the most frequent method used to perform pulmonary-vein electrical isolation. However, cryoballoon ablation is rapidly becoming the more frequently used technology. One multicenter randomized trial by Kuck et al. comparing radiofrequency ablation to cryoballoon catheter ablation found that cryoballoon ablation was non-inferior to radiofrequency ablation, with primary endpoints including recurrence of atrial fibrillation, occurrence of atrial flutter or atrial tachycardia, use of antiarrhythmic drugs, or repeat ablation occurring in 34.6% in the cryoballoon group versus 35.9% occurring in the radiofrequency group (P<.001). The complication rate in both groups was also non-significant.[30] Additionally, balloon-based ablation offers a faster means of achieving PVI, that is less reliant on operator skills compared to point-by-point ablation. Cryothermal energy also decreases endothelial disruption lowering thromboembolic risk, and causes minimal tissue contraction with healing, resulting in less PV stenosis and esophageal damage.[31]
As expansion of the balloon to a certain size requires ideal pulmonary venous anatomy, cryoablation may not be feasible for every patient with paroxysmal atrial fibrillation. This has been shown in a study by Kubala et al. which demonstrated that patients with a left common ostium had more recurrences compared to normal PV anatomy.[32] In contrast, one study by Khoueiry et al looking at outcomes of cryoablation versus radiofrequency in patients with paroxysmal AF, the authors found no significant difference in the incidence of recurrent atrial fibrillation regardless of pulmonary vein anatomical variation.[33] Additionally, Sorgente et al. reported no significant difference in PV occlusion and longer duration between endpoints in patients with variant anatomy including a left common ostium versus normal discrete left ostia.[34] Thus, the presence of anatomical variation in patients should not discourage physicians from the use of cryoballoon ablation.
In conclusion, cryoballoon ablation for atrial fibrillation offers an effective, safer, less operator-dependant, means of achieving pulmonary vein isolation, with greater improvement in the quality of life, compared to medical therapy. As such, physicians should present the option to patients with symptomatic atrial fibrillation, not responding to medical therapy.
Enhancing Healthcare Team Outcomes
An interprofessional approach to catheter ablation of the pulmonary vein is recommended. Effective communication among specialty trained nurses and clinicians will produce the best outcomes. [Level 5]
AF is associated with enormous morbidity and mortality, costing billions of healthcare dollars each year. Catheter ablation of the pulmonary vein is one way to manage symptomatic AF. Primary care providers and nurse practitioners should consult with a cardiologist about the options for treatment of AF patients. Today, catheter ablation has shown good results but a significant number of patients do develop recurrences, and the procedure is not benign. In any case, catheter ablation remains the choice of symptomatic patients who do not respond to antiarrhythmic drugs.
Media
(Click Image to Enlarge)
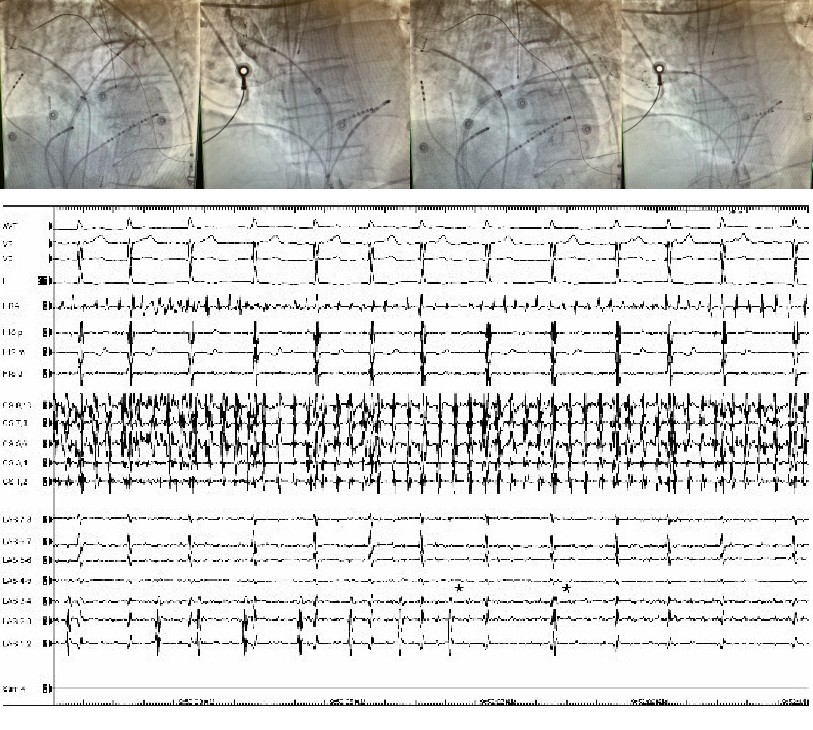
Pulmonary Vein Radiographs and EKG Contributed by Mena Yacoub
References
January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW, American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Journal of the American College of Cardiology. 2014 Dec 2:64(21):e1-76. doi: 10.1016/j.jacc.2014.03.022. Epub 2014 Mar 28 [PubMed PMID: 24685669]
Level 1 (high-level) evidenceMiyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006 Jul 11:114(2):119-25 [PubMed PMID: 16818816]
Schnabel RB, Sullivan LM, Levy D, Pencina MJ, Massaro JM, D'Agostino RB Sr, Newton-Cheh C, Yamamoto JF, Magnani JW, Tadros TM, Kannel WB, Wang TJ, Ellinor PT, Wolf PA, Vasan RS, Benjamin EJ. Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study. Lancet (London, England). 2009 Feb 28:373(9665):739-45. doi: 10.1016/S0140-6736(09)60443-8. Epub [PubMed PMID: 19249635]
Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. The New England journal of medicine. 1998 Sep 3:339(10):659-66 [PubMed PMID: 9725923]
Brick AV, Braile DM. Surgical Ablation of Atrial Fibrillation Using Energy Sources. Brazilian journal of cardiovascular surgery. 2015 Nov-Dec:30(6):636-43. doi: 10.5935/1678-9741.20150078. Epub [PubMed PMID: 26934404]
Garg J, Chaudhary R, Palaniswamy C, Shah N, Krishnamoorthy P, Bozorgnia B, Natale A. Cryoballoon versus Radiofrequency Ablation for Atrial Fibrillation: A Meta-analysis of 16 Clinical Trials. Journal of atrial fibrillation. 2016 Oct-Nov:9(3):1429. doi: 10.4022/jafib.1429. Epub 2016 Oct 31 [PubMed PMID: 28496925]
Level 1 (high-level) evidenceGoel R, Anderson K, Slaton J, Schmidlin F, Vercellotti G, Belcher J, Bischof JC. Adjuvant approaches to enhance cryosurgery. Journal of biomechanical engineering. 2009 Jul:131(7):074003. doi: 10.1115/1.3156804. Epub [PubMed PMID: 19640135]
Level 3 (low-level) evidenceBarnett AS, Bahnson TD, Piccini JP. Recent Advances in Lesion Formation for Catheter Ablation of Atrial Fibrillation. Circulation. Arrhythmia and electrophysiology. 2016 May:9(5):. doi: 10.1161/CIRCEP.115.003299. Epub [PubMed PMID: 27103088]
Level 3 (low-level) evidenceWittkampf FH, Derksen R, Wever EF, Simmers TA, Boersma LV, Vonken EP, Velthuis BK, Sreeram N, Rensing BJ, Cramer MJ. Technique of pulmonary vein isolation by catheter ablation. Netherlands heart journal : monthly journal of the Netherlands Society of Cardiology and the Netherlands Heart Foundation. 2002 May:10(5):241-244 [PubMed PMID: 25696100]
Katz-Agranov N, Nevah Rubin MI. Severe esophageal injury after radiofrequency ablation - a deadly complication. World journal of gastroenterology. 2017 May 14:23(18):3374-3378. doi: 10.3748/wjg.v23.i18.3374. Epub [PubMed PMID: 28566899]
Ozcan C, Ruskin J, Mansour M. Cryoballoon catheter ablation in atrial fibrillation. Cardiology research and practice. 2011:2011():256347. doi: 10.4061/2011/256347. Epub 2011 Jun 20 [PubMed PMID: 21747987]
Leila R, Raluca P, Yves G, Dirk S, Bruno S. Cryoablation Versus Radiofrequency Ablation in AVNRT: Same Goal, Different Strategy. Journal of atrial fibrillation. 2015 Jun-Jul:8(1):1220. doi: 10.4022/jafib.1220. Epub 2015 Jun 30 [PubMed PMID: 27957174]
Kuck K, Brugada J, Albenque J. Cryoballoon or Radiofrequency Ablation for Atrial Fibrillation. The New England journal of medicine. 2016 Sep 15:375(11):1100-1. doi: 10.1056/NEJMc1609160. Epub [PubMed PMID: 27626535]
Kato R, Lickfett L, Meininger G, Dickfeld T, Wu R, Juang G, Angkeow P, LaCorte J, Bluemke D, Berger R, Halperin HR, Calkins H. Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: lessons learned by use of magnetic resonance imaging. Circulation. 2003 Apr 22:107(15):2004-10 [PubMed PMID: 12681994]
Level 1 (high-level) evidenceNathan H, Eliakim M. The junction between the left atrium and the pulmonary veins. An anatomic study of human hearts. Circulation. 1966 Sep:34(3):412-22 [PubMed PMID: 5922708]
Stiles MK, John B, Wong CX, Kuklik P, Brooks AG, Lau DH, Dimitri H, Roberts-Thomson KC, Wilson L, De Sciscio P, Young GD, Sanders P. Paroxysmal lone atrial fibrillation is associated with an abnormal atrial substrate: characterizing the "second factor". Journal of the American College of Cardiology. 2009 Apr 7:53(14):1182-91. doi: 10.1016/j.jacc.2008.11.054. Epub [PubMed PMID: 19341858]
Chen PS, Chen LS, Fishbein MC, Lin SF, Nattel S. Role of the autonomic nervous system in atrial fibrillation: pathophysiology and therapy. Circulation research. 2014 Apr 25:114(9):1500-15. doi: 10.1161/CIRCRESAHA.114.303772. Epub [PubMed PMID: 24763467]
Level 3 (low-level) evidencePellman J, Sheikh F. Atrial fibrillation: mechanisms, therapeutics, and future directions. Comprehensive Physiology. 2015 Apr:5(2):649-65. doi: 10.1002/cphy.c140047. Epub [PubMed PMID: 25880508]
Level 3 (low-level) evidenceCalkins H,Hindricks G,Cappato R,Kim YH,Saad EB,Aguinaga L,Akar JG,Badhwar V,Brugada J,Camm J,Chen PS,Chen SA,Chung MK,Nielsen JC,Curtis AB,Davies DW,Day JD,d'Avila A,de Groot NMSN,Di Biase L,Duytschaever M,Edgerton JR,Ellenbogen KA,Ellinor PT,Ernst S,Fenelon G,Gerstenfeld EP,Haines DE,Haissaguerre M,Helm RH,Hylek E,Jackman WM,Jalife J,Kalman JM,Kautzner J,Kottkamp H,Kuck KH,Kumagai K,Lee R,Lewalter T,Lindsay BD,Macle L,Mansour M,Marchlinski FE,Michaud GF,Nakagawa H,Natale A,Nattel S,Okumura K,Packer D,Pokushalov E,Reynolds MR,Sanders P,Scanavacca M,Schilling R,Tondo C,Tsao HM,Verma A,Wilber DJ,Yamane T, 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: Executive summary. Journal of arrhythmia. 2017 Oct [PubMed PMID: 29021841]
Level 3 (low-level) evidencePacker DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Moretz K, Poole JE, Mascette A, Rosenberg Y, Jeffries N, Al-Khalidi HR, Lee KL, CABANA Investigators. Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) Trial: Study Rationale and Design. American heart journal. 2018 May:199():192-199. doi: 10.1016/j.ahj.2018.02.015. Epub 2018 Mar 7 [PubMed PMID: 29754661]
Liu X, Palmer J. Outcomes of 200 consecutive, fluoroless atrial fibrillation ablations using a new technique. Pacing and clinical electrophysiology : PACE. 2018 Nov:41(11):1404-1411. doi: 10.1111/pace.13492. Epub 2018 Sep 19 [PubMed PMID: 30194724]
Fürnkranz A, Köster I, Chun KR, Metzner A, Mathew S, Konstantinidou M, Ouyang F, Kuck KH. Cryoballoon temperature predicts acute pulmonary vein isolation. Heart rhythm. 2011 Jun:8(6):821-5. doi: 10.1016/j.hrthm.2011.01.044. Epub 2011 Apr 11 [PubMed PMID: 21315836]
Level 2 (mid-level) evidenceCappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005 Mar 8:111(9):1100-5 [PubMed PMID: 15723973]
Level 3 (low-level) evidenceParikh V, Kowalski M. Comparison of Phrenic Nerve Injury during Atrial Fibrillation Ablation between Different Modalities, Pathophysiology and Management. Journal of atrial fibrillation. 2015 Dec:8(4):1314. doi: 10.4022/jafib.1314. Epub 2015 Dec 31 [PubMed PMID: 27957229]
Canpolat U, Kocyigit D, Aytemir K. Complications of Atrial Fibrillation Cryoablation. Journal of atrial fibrillation. 2017 Dec:10(4):1620. doi: 10.4022/jafib.1620. Epub 2017 Dec 31 [PubMed PMID: 29487676]
Mujović N, Marinković M, Lenarczyk R, Tilz R, Potpara TS. Catheter Ablation of Atrial Fibrillation: An Overview for Clinicians. Advances in therapy. 2017 Aug:34(8):1897-1917. doi: 10.1007/s12325-017-0590-z. Epub 2017 Jul 21 [PubMed PMID: 28733782]
Level 3 (low-level) evidencePacker DL, Kowal RC, Wheelan KR, Irwin JM, Champagne J, Guerra PG, Dubuc M, Reddy V, Nelson L, Holcomb RG, Lehmann JW, Ruskin JN, STOP AF Cryoablation Investigators. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Arctic Front (STOP AF) pivotal trial. Journal of the American College of Cardiology. 2013 Apr 23:61(16):1713-23. doi: 10.1016/j.jacc.2012.11.064. Epub 2013 Mar 21 [PubMed PMID: 23500312]
Level 1 (high-level) evidenceAndrade JG, Dubuc M, Guerra PG, Macle L, Rivard L, Roy D, Talajic M, Thibault B, Khairy P. Cryoballoon ablation for atrial fibrillation. Indian pacing and electrophysiology journal. 2012 Mar:12(2):39-53 [PubMed PMID: 22557842]
Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y, Martin A, Williams CJ, Sledge I. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. Circulation. Arrhythmia and electrophysiology. 2009 Aug:2(4):349-61. doi: 10.1161/CIRCEP.108.824789. Epub 2009 Jun 2 [PubMed PMID: 19808490]
Level 1 (high-level) evidenceKuck KH, Fürnkranz A. Cryoballoon ablation of atrial fibrillation. Journal of cardiovascular electrophysiology. 2010 Dec:21(12):1427-31. doi: 10.1111/j.1540-8167.2010.01944.x. Epub 2010 Nov 23 [PubMed PMID: 21091966]
Level 3 (low-level) evidenceAndrade JG, Khairy P, Guerra PG, Deyell MW, Rivard L, Macle L, Thibault B, Talajic M, Roy D, Dubuc M. Efficacy and safety of cryoballoon ablation for atrial fibrillation: a systematic review of published studies. Heart rhythm. 2011 Sep:8(9):1444-51. doi: 10.1016/j.hrthm.2011.03.050. Epub 2011 Mar 30 [PubMed PMID: 21457789]
Level 1 (high-level) evidenceKubala M, Hermida JS, Nadji G, Quenum S, Traulle S, Jarry G. Normal pulmonary veins anatomy is associated with better AF-free survival after cryoablation as compared to atypical anatomy with common left pulmonary vein. Pacing and clinical electrophysiology : PACE. 2011 Jul:34(7):837-43. doi: 10.1111/j.1540-8159.2011.03070.x. Epub 2011 Mar 21 [PubMed PMID: 21418249]
Khoueiry Z, Albenque JP, Providencia R, Combes S, Combes N, Jourda F, Sousa PA, Cardin C, Pasquie JL, Cung TT, Massin F, Marijon E, Boveda S. Outcomes after cryoablation vs. radiofrequency in patients with paroxysmal atrial fibrillation: impact of pulmonary veins anatomy. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2016 Sep:18(9):1343-51. doi: 10.1093/europace/euv419. Epub 2016 Jan 27 [PubMed PMID: 26817755]
Sorgente A, Chierchia GB, de Asmundis C, Sarkozy A, Namdar M, Capulzini L, Yazaki Y, Müller-Burri SA, Bayrak F, Brugada P. Pulmonary vein ostium shape and orientation as possible predictors of occlusion in patients with drug-refractory paroxysmal atrial fibrillation undergoing cryoballoon ablation. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2011 Feb:13(2):205-12. doi: 10.1093/europace/euq388. Epub 2010 Oct 25 [PubMed PMID: 20974756]
Level 2 (mid-level) evidence