
Introduction
The multifocal dissemination of cancer cells from its primary site to subarachnoid, pia mater, and CSF in the brain and spinal cord is referred to as carcinomatous meningitis (CM). It is also termed as ‘leptomeningeal meningitis,’ ‘leptomeningeal carcinomatosis,’ ‘leptomeningeal metastasis,’ or ‘neoplastic meningitis.’ Beerman, in 1912, used the term ‘carcinomatous meningitis’ for a condition in which cancer cells metastasized to the meninges without involving brain parenchyma.[1]
CM can occur in the advanced stage of many malignancies when cancer cells seed through CSF and deposit in the meninges. Involvement is usually multifocal and can cause a wide variety of symptoms. CSF analysis, along with imaging techniques, aid in the diagnosis. Treatment options include radiotherapy and chemotherapy. However, early diagnosis is challenging, and prognosis generally remains dismal. The development of newer techniques for diagnosis and novel therapeutic strategies may improve prognosis and limit morbidity.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Primary cancers that metastasize to the leptomeninges are intracranial or extracranial. The most common extracranial malignancies include breast cancer, lung cancer, and melanoma. Intracranial malignancies include cerebellar medulloblastoma, malignant ependymomas, neuromas, and gliomas.
Epidemiology
The incidence of leptomeningeal metastasis from solid tumors is 5% to 8%, and from hematological malignancies is 5 to 15%.[2] Among hematological malignancies, B-cell lymphoma is the most common etiology. However, the incidence may be as high as 20%, given the instances of undiagnosed cases, which are only reported at autopsies.[3]
The most common solid organ tumors causing carcinomatous meningitis are lung cancer, melanoma, and breast cancer, with a varying incidence reported in several studies.[4][5] Parenchymal brain malignancies causing carcinomatous meningitis include gliomas, ependymomas, and medulloblastomas. CM is usually associated with underlying parenchymal involvement in about 60% of the cases.[5] In 1 to 7% of the cases, the primary site of the disease cannot be located despite extensive evaluation.[6]
Pathophysiology
Cancer is an abnormal and uncontrolled proliferation of cells at a certain location that has the potential to spread to a distant site. These malignant cells develop vascularity, which in turn increases its ability to proliferate. About 14.1 million cases of cancers are registered every year, out of which about 8.8 million are eventually fatal, making cancer one of the leading causes of death.[7][8] Though the preferential metastatic site is not definite, certain cancers are more likely to metastasize to specific locations.
The central nervous system (CNS) has three layers of meninges called the dura mater, the arachnoid, and the pia mater. The dura mater is known as the patchy-meningeal layer. The arachnoid and pia meningeal layers are called the leptomeninges. The cerebrospinal fluid (CSF) lies in the space between the arachnoid and pia mater, known as the subarachnoid space.
The CSF is the main route for the malignant cells to gain access to the leptomeninges. However, to do so, the cancer cells must cross the blood-brain barrier (BBB). The BBB is an anatomical structure that consists of brain microvascular endothelial cells (BMECs), which form tight intercellular junctions with astrocyte foot processes and regulate transport from blood to CSF. It is hypothesized that tumor cells bind to endothelial cells via receptors and confer changes in the endothelium. This exposes the vascular basement membrane to tumor cells, which then binds to specific components and enters the CSF. Certain genomic functions mediate this whole process of extravasation of cancer cells. This metastatic potential is acquired over time. The Massague’ group suggested that overlapped genes like COX-2, EGFR ligand, ANGPTL4, and LTBP1 are responsible for causing disruption of BBB and tumor proliferation in different parts of the brain.[9]
Refer to figure 1:[9] Schematic presentation of tumor cell penetration across BBB.
Routes of Spread
The routes of spread to BBB from primary tumor site includes:
- Hematogenous spread
- Direct invasion from primary tumors in the brain parenchyma and meninges
- Choroid plexus metastasis into CSF
- Epidural, subdural, and vertebral metastasis
- Perineural and endoneurial spread from the brain and spinal cord in a retrograde manner
- Iatrogenic spread via neurosurgical procedures
CSF is known to be rich in high amounts of oxygen and glucose, enough to support the high metabolic demands of the rapidly multiplying malignant cells. Therefore, tumor proliferation in leptomeninges is not dependent upon angiogenesis, a limiting factor for tumors in other locations, including brain parenchymal metastasis.[10]
Risk Factors
The major risk factors associated with CM are:
- Incomplete surgical resection of brain metastasis
- The Omission of postoperative radiation therapy
- Presence of parenchymal brain metastasis in young (age <40 years)
- Advanced systemic disease
Neurosurgical resection is the preferred treatment option for solitary brain metastasis. Many studies indicate that the risk of CM is 2.81 times more with piecemeal resection than in en-bloc resection.[11]
Due to the selective permeability of BBB, conventional systemic therapy may not be effective in brain metastasis. Radiotherapy (RT) is a feasible option for radiosensitive tumors, especially if the primary site is unknown. Adjuvant RT is recommended after neurosurgical resection. Whole-brain radiation therapy (WBRT) reduces the risk of recurrence but is associated with increased adverse effects, and therefore stereotactic radiosurgery (SRS) is increasingly becoming the preferred option. Studies have shown that the risk of CM after prior neurosurgical resection is 6.5 times higher than SRS without previous surgery.[12]
Location of brain metastasis and tumor volume has not been found to increase the possibility of occurrence of CM. It is the chance of CSF exposure for the spilling of the tumor cells that is rather significant.[13] In patients receiving SRS for brain metastases, certain independent factors that influence the risk of CM are the type of primary tumor, number of intracranial metastases, young age, and distant brain failure (defined as development of new metastatic lesion outside of the treated radiation field).[14]
History and Physical
Clinical features of carcinomatous meningitis are pleomorphic because of the extensive involvement of neuraxis. Different pathophysiological mechanisms include:
- Increased intracranial pressure (ICP) caused by obstruction to CSF flow; if this obstruction occurs at convexities, communicating hydrocephalus emanates; if the blockage occurs at the ventricles, non-communicating hydrocephalus ensues.
- Disruption of the blood-brain barrier causing cerebral edema.
- Direct tumor cell invasion into cranial and spinal nerves from subarachnoid space.
- Malignant cells invade the brain parenchyma, usually via Virchow-Robin spaces, which are pia matter lined perivascular spaces in different regions of the brain and utilize the oxygen and glucose required for neuronal cell growth and functioning. This competition can cause widespread depression of metabolism in the cerebral cortex, causing encephalopathy.[10] The tumor burden in the cerebral vessels of the spaces can also cause stroke-like symptoms in patients with CM.
- The coexistence of leptomeningeal metastasis with brain parenchymal metastatic lesions present with focal signs of intraparenchymal disease.
The most common presenting symptom is a headache and is found in about 39% of patients.[15][16] Headache is caused by either meningeal irritation or by raised ICP. In meningeal irritation, headaches are associated with nuchal rigidity worsened by leg flexion (Kernig sign). In raised ICP, headaches are accompanied by nausea, which is worse in the morning. Confusion is the second most common presentation and occurs because of the metabolic depression of the cortex by active malignant cells. This results in an altered state of consciousness or cognitive impairment. It can also cause temporal lobe seizures presenting as deja vu, stereotypical movements, euphoria, hallucinations, and amnesia.
Posterior fossa involvement causes both cerebellar signs and cranial neuropathies. These are observed in 65% of the cases and incorporate nausea, vomiting, dizziness, ataxia, and diplopia.[16][17] Cranial neuropathies present as diplopia, visual loss, facial weakness, hearing loss, balance disturbances, dysphagia, dysarthria, and hoarseness. Among cranial nerves, CN 6, 7, and 8 are more frequently impacted.
CM may also involve the spinal cord and its exiting nerve roots. The spinal nerve roots that are affected produce symptoms in the anatomically associated regions. Symptoms may include segmental numbness, dysesthesia, pain, and lower motor neuron pattern limb weakness. The involvement of sacral nerve roots may cause bowel and bladder dysfunction. Cauda equina and conus medullaris syndromes can be the only presentation in CM patients. Leg weakness (28%) and back pain/paralysis (18%) are the initial presenting symptoms of leptomeningeal metastases of the spinal cord.[18]
CM can be asymptomatic in 2% of the patients.[16]
Evaluation
The first and foremost step in the evaluation of carcinomatous meningitis is obtaining a comprehensive history and physical exam. An accurate neurological exam helps determine whether the involvement is focal or multifocal and leads the clinician to suspect leptomeningeal involvement. CSF evaluation and neuroimaging study is the next step in the diagnosis. A pragmatic approach for both diagnosis and prognosis may require testing of tumor markers as well.
Cerebral Spinal Fluid
CSF findings typically include the following:
- High CSF pressure (greater than 25 cmH2O) is observed in about 50% of CM patients.[19]
- Pleocytosis is detected in 33-79% of CM.[20] White blood cells are mostly lymphocytes, but eosinophils are also identified in lymphomas and leukemia. The presence of RBCs or xanthochromia in CM may develop due to a traumatic tap.
- The protein level in CSF is elevated in about 80% of the cases.[21] The normal range of protein in CSF is between 15-45 mg/dl, and elevated values are due to proteins produced by the tumor cells or breakdown of the blood-brain barrier.
- The glucose level in CSF in CM are decreased in about 25-40% of the cases and is called hypoglycorrhachia.[19] Normal glucose levels in CSF range between 50-80 mg/dl. Hypoglycorrhachia occurs because of the metabolism of tumor cells or defective transport mechanisms. This is also seen in infective meningitis, and cytology is necessary to differentiate between the two in such cases.
- Initial CSF cytology is positive in 55% of the cases.[22] Repeat CSF cytology is done if the first sample is negative and if clinical suspicion remains high. This increases the sensitivity to 80%.[23] Moreover, higher volumes of CSF (>10 ml) also improves yield. The sensitivity of CSF cytology for the diagnosis of CM ranges from 80 to 95%, but the specificity is very high.
The standardization of the method for CSF collection is an indispensable requirement. An appropriate site (producing symptoms preferably) and sufficient volume (minimum 10 ml) are the prerequisites for the spinal tap. Analysis of CSF via lumbar puncture (LP) and CSF tested from an indwelling catheter produces varying results.
Although CSF cytology is the gold standard for diagnosis, immunohistochemical staining of the cells is recommended, particularly if the primary site of the tumor remains unknown. Flow cytometry is a rapid, quantifiable measure of a specific type of cell with certain characteristics such as cancer cells that are associated with specific antigens. It provides a highly sensitive method for the detection of hematological malignancies. FISH (fluorescent in situ hybridization) is a cytogenetic technique for localizing particular DNA sequences or genes and may yield information on metastatic lesions but with a lower sensitivity.[2] PCR (polymerase chain reaction) is used to identify immunoglobulin gene arrangements in malignant cells, specifically for lymphoma. Hence the study of cytological, morphological, molecular, and cytogenetic characteristics is vital for identification of the tumor type and, at times, the prognosis.[24]
Tumor markers have a role in making an early diagnosis and monitoring response to treatment. However, it may also be imperative in determining the prognosis. The nonspecific markers include LDH (lactate dehydrogenase), beta-2 microglobulin, and specific markers include AFP (alpha-fetoprotein), BHCG (beta-human chorionic gonadotropin), and CEA (carcinoembryonic antigen). CSF value of more than 1% of the serum level of these markers is diagnostic.[2] A study done at Memorial Sloan-Kettering Cancer Center demonstrated that patients with CM from breast cancer, lung cancer, and melanoma have abnormal levels of at least one tumor marker in CSF in 74-90% of the cases.[25] CEA is helpful in adenocarcinoma of the lung, AFP in germ cell tumors, and Beta-2 microglobulin in hematological malignancies. The pro-angiogenic factor VEGF (vascular endothelial growth factor) in CSF also has a diagnostic significance. The VEGF index, defined as the ratio of CSF/serum VEGF concentration to CSF/serum albumin levels, is found to be higher in CM and is a promising reliable diagnostic tool.[26] Moreover, the detection of several tumor markers in CSF can increase sensitivity, specificity, and predictive value.[25]
The glucose levels in CSF also have a prognostic value. The probability of CM is less with hyperglycorrhachia, and levels greater than 2.7 mmol/L are associated with better outcomes.[27][28]
CSF Flow Studies
In CM, obstructions in CSF flow are common because of the adhesion of tumor cells in the subarachnoid space and occur in 30 to 70% of the cases.[3] Obstruction to CSF flow is hazardous as it decreases treatment efficacy and increases toxicity and mortality by hindering chemotherapy drug distribution. Hence, it is essential to ensure appropriate CSF flow during chemotherapy. CSF dynamics are monitored by 111Indium-DPTA ventriculography or Technetium-99m-DPTA flow studies before starting intrathecal therapy.[29] Furthermore, it will decrease treatment-related mortality and improve survival by reducing tumor progression, neurological, and systemic toxicity.[30]
Neuroimaging
Gadolinium-enhanced MRI scan is a pertinent test for the diagnosis of CM. Radiographic findings may include hydrocephalus and leptomeningeal enhancement of the brain in the T1 weighted image with contrast. T2/FLAIR hyperintensities may be seen in the subarachnoid space. The cerebral convexities, cerebellar folia, basal cisterns, and ventricular ependymal regions are the common areas that display enhancement or nodular deposits in CM.[20] In the spinal cord, linear and nodular leptomeningeal enhancements may occur along the nerve roots, particularly in the cauda equina.[31]
For solid tumors, the sensitivity of MRI is 76%, and it increases to 95% for spinal MRI in patients presenting with cauda equina syndrome.[32]
MRI shows enhancement in both inflammatory and carcinomatous meningitis. Hence, it is imperative to pair it with CSF cytology. False-positive leptomeningeal enhancement may be seen in patients undergoing treatment due to therapy-induced inflammatory reaction, as seen with radiotherapy and immunotherapy. The prevalence is low (<1%) but still should be considered as a possibility in patients.[33]
Refer to Figure 2:[34] MRI T1 weighted images showing leptomeningeal enhancement, and
Figure 3: [35] MRI T1 weighted images showing leptomeningeal enhancement in lower portions of the spinal cord and post-treatment images.
Treatment / Management
The management of carcinomatous meningitis is complex and involves a combination of multiple treatment modalities. The goal of treatment is to improve the quality of life, prolong survival, and stabilize neurological deterioration while minimizing iatrogenic toxicity. The therapeutic options depend on ‘good risk’ versus ‘poor risk’ disease and are determined by the patient’s KPS score, tumor grade, systemic disease burden, and neurological status.
The KPS (Karnofsky performance score) and ECOG (Eastern Cooperative Oncology Group) are the two common performance status scoring systems to document the functional status of patients with cancer. Palliative care is recommended for patients with low KPS and high ECOG scores, as the risks associated with treatment outweigh potential benefits. Evaluation of treatment response and toxicity is also essential during every stage of treatment.
Guidelines on the management of patients with CM have been formulated by NCCN and ESMO. The three primary therapeutic modalities are:
- Radiation therapy
- Intrathecal chemotherapy
- Systemic chemotherapy
Radiation Therapy
Radiation therapy of CM includes focal radiation to nodular plaque-like deposits of malignant cells in meninges or diffuse radiation therapy to linear leptomeningeal contrast-enhancement lesions. It is usually targeted to sites of symptomatic or bulky disease.
Cranial irradiation is helpful in isolated cranial neuropathies and obstructive hydrocephalus. Focal spinal irradiation is helpful for lower extremity weakness and bladder or bowel involvement. Even though the neurological deficits may not improve, it decreases radicular pain. The dose used for cranial and spinal irradiation is typically 30 Gy in 10 daily fractions.[36] For patients with poor prognosis, 20 Gy in 5 daily fractions can be used.
Whole-brain radiation therapy (WBRT) is helpful in patients with hydrocephalus secondary to CM. It decreases the ICP by breaking down adhesions caused by tumor cells and minimize the requirement of ventriculoperitoneal (VP) shunt. It enables intrathecal chemotherapy to work effectively by restoring CSF flow. WBRT is also helpful in bulky tumors and can be used in patients with low KPS scores, multiple metastatic lesions, severe systemic illness, and reduced survival. The dose is 30 Gy in 10 daily fractions.[37]
Radiosensitive tumors include hematological malignancies, gynecological tumors, pediatric gliomas, and rhabdomyosarcomas.[38] Focal radiation therapy rarely causes adverse effects. Alopecia, seizures, encephalopathy, mucositis, myelopathy, and myelosuppression can occur with more extensive fields. In patients with good-risk disease (Karnofsky performance status ≥60, no major neurologic deficits, minimal systemic disease), a multimodal approach comprising of both chemotherapy and radiation therapy is preferred.[39](B2)
Chemotherapy
Chemotherapy options in CM include both intrathecal and systemic chemotherapy.
Intrathecal Chemotherapy
Intrathecal chemotherapy (IT) is the mainstay of treatment for CM due to the selective BBB that limits the therapeutic efficacy of most systemic chemotherapy agents. It cannot be used with a VP shunt in place as it leads to toxic drugs entering the peritoneal cavity. IT is done either by injecting the drug into the subarachnoid space after performing an LP or by using an Ommaya catheter. Ommaya catheter is a small circular device placed beneath the scalp and drains into the lateral ventricle by a tube, thereby facilitating access to the CSF in the ventricles for the introduction of chemotherapy agents.
Lumbar puncture (LP) is easy to perform but has certain limitations. The requirement of frequent LPs increases the risk of bleeding with severe thrombocytopenia, and an unpredictable path of drug distribution in the brain after the spinal tap. As compared to LP, the Ommaya reservoir offers several merits. Drug administration is relatively painless and can be performed frequently. It ensures a uniform drug distribution in the subarachnoid space. However, it can be a source of infection that can prove dangerous in an already immunocompromised patient and requires surgery, which may not be possible in some patients. The intraventricular approach has been noted to have a better response than the intralumbar method and also offers a survival benefit.[40] A randomized controlled trial done by Glantz et al. showed an increase in progression-free survival with the intraventricular route for methotrexate compared to intrathecal (43 vs. 19 days, p=0.048).[41](A1)
Conventional drugs for the intrathecal route (IT) include methotrexate, cytarabine, and less commonly, thiotepa. Methotrexate is the most common agent and can cause myelosuppression and neurological complications, including aseptic meningitis. Hematological malignancies are more responsive to IT. Early studies have described therapeutic efficacy with intrathecal administration of monoclonal antibodies, including trastuzumab in human epidermal growth factor receptor 2 (HER2) positive breast cancer and rituximab in lymphoma.[42](B3)
Systemic Chemotherapy
Systemic chemotherapy helps treat leptomeningeal disease as well as a systemic disease. As the BBB may only be partially disrupted in CM, agents used must be safe at high doses or lipid-soluble, so that therapeutic levels can be attained in CSF.[2] Methotrexate and cytarabine require higher doses due to their low permeability.[16](B3)
It is convenient for high-risk surgical patients as it does not require Ommaya reservoir placement, and practical in cases of CSF flow obstruction. It may also provide uniform drug distribution in CSF. Several agents can be used, and the choice depends on the primary tumor. High dose systemic methotrexate along with leucovorin rescue, is used as an alternative to IT. Capecitabine, an oral 5-fluorouracil drug, is effective in breast cancers with CM.[43] Several newer molecularly targeted therapies also have efficacy in CM.(B3)
Some examples of targeted therapy effective in CM include:
- Epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (EGFR-TKI) are used in lung cancers with EGFR mutations.[44] Erlotinib, gefitinib, and osimertinib are EGFR inhibitors.
- HER2 TKI is used in breast cancers. Lapatinib and tucatinib are examples.[45]
- BRAF inhibitors like vemurafenib have shown good clinical response and improved survival with leptomeningeal metastasis in patients with melanoma.[46]
- Anaplastic lymphoma kinase (ALK) inhibitors are used in lung cancers with ALK rearrangements. Drugs include crizotinib, ceritinib, alectinib, brigatinib, and lorlatinib.[47] (A1)
A combined multimodality approach may improve clinical outcomes.[48] In breast cancer, a combination of intrathecal liposomal cytarabine and intravenous high dose methotrexate has shown promising results.[49] A retrospective study done on patients with non-small cell lung cancer showed that the use of IT, WBRT, and EGFR-TKI were predictors for improved survival.[50](B2)
Refer to Figure 4: Management of Carcinomatous Meningitis
Differential Diagnosis
Numerous conditions can present with similar symptomatology as carcinomatous meningitis and should be taken into consideration whenever patients present with indistinguishable signs and symptoms.
- Intraparenchymal primary brain lesions or metastasis can present with similar symptoms. Calvarial and dura matter involvement should be ruled out. Leptomeningeal metastasis can present separately or co-exist with the involvement of these regions.
- Chronic or recurrent meningitis caused by a variety of bacterial, fungal, viral, or protozoal organisms can also resemble CM. Autoimmune and drug-induced causes of meningitis should also be considered.
- Paraneoplastic syndromes, including Lambert Eaton syndrome, Myasthenic crises, cerebellar degeneration, encephalomyelitis, neuropathies, and limbic encephalitis, can mimic CM and are associated with advanced-stage disease.
Prognosis
Carcinomatous meningitis represents advanced-stage disease and usually has a dismal prognosis. The median time of survival is 2 to 4 months, even with treatment.[5] Early diagnosis, normal CSF protein levels, and low disease burden are factors associated with a better prognosis.[51] Patients with KPS score >60, minimal systemic disease, minimal neurological deficits, and options for effective systemic therapy are considered to have a good-risk disease. In these patients, systemic therapy combined with IT or RT may be beneficial. In poor-risk patients, palliative care is the best option. CM, due to lymphomas and leukemias, has a better prognosis compared to solid tumors.[52]
Enhancing Healthcare Team Outcomes
Several future directions may help improve survival in patients with carcinomatous meningitis. This includes early diagnosis by analyzing circulating tumor DNA in CSF (CSF-ctDNA). These are shed from the cancer cells as a result of apoptosis and necrosis. Identification can help avoid subjecting the patient to high-risk surgeries or biopsies. The amount of CSF-ct DNA can provide information about tumor burden, recurrence, and treatment response. The identification of novel mutations in CSF-ctDNA can also provide newer therapeutic targets. There is a need for discovery of non-invasive methods like ultrasonography or CT scan guided drug delivery. Novel biological agents and immunomodulatory drugs may help in achieving better survival and improved quality of life.
The multidisciplinary team comprising of neurologists, neurosurgeons, medical oncologists, radiation oncologists, psychiatrists, and nurses must manage the biological, psychological, and social aspects of this disease.
Media
(Click Image to Enlarge)
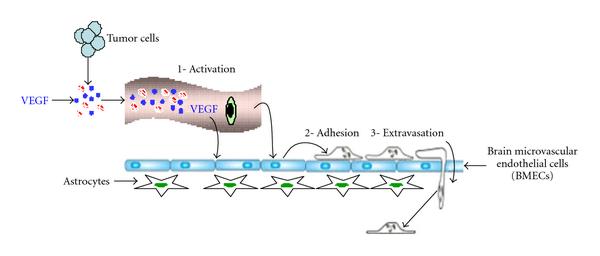
Figure one Referring PMID 21253507, Blood-brain barrier integrity and breast cancer metastasis to the brain. Contributed by Ayesha Anwar, MBBS
(Click Image to Enlarge)
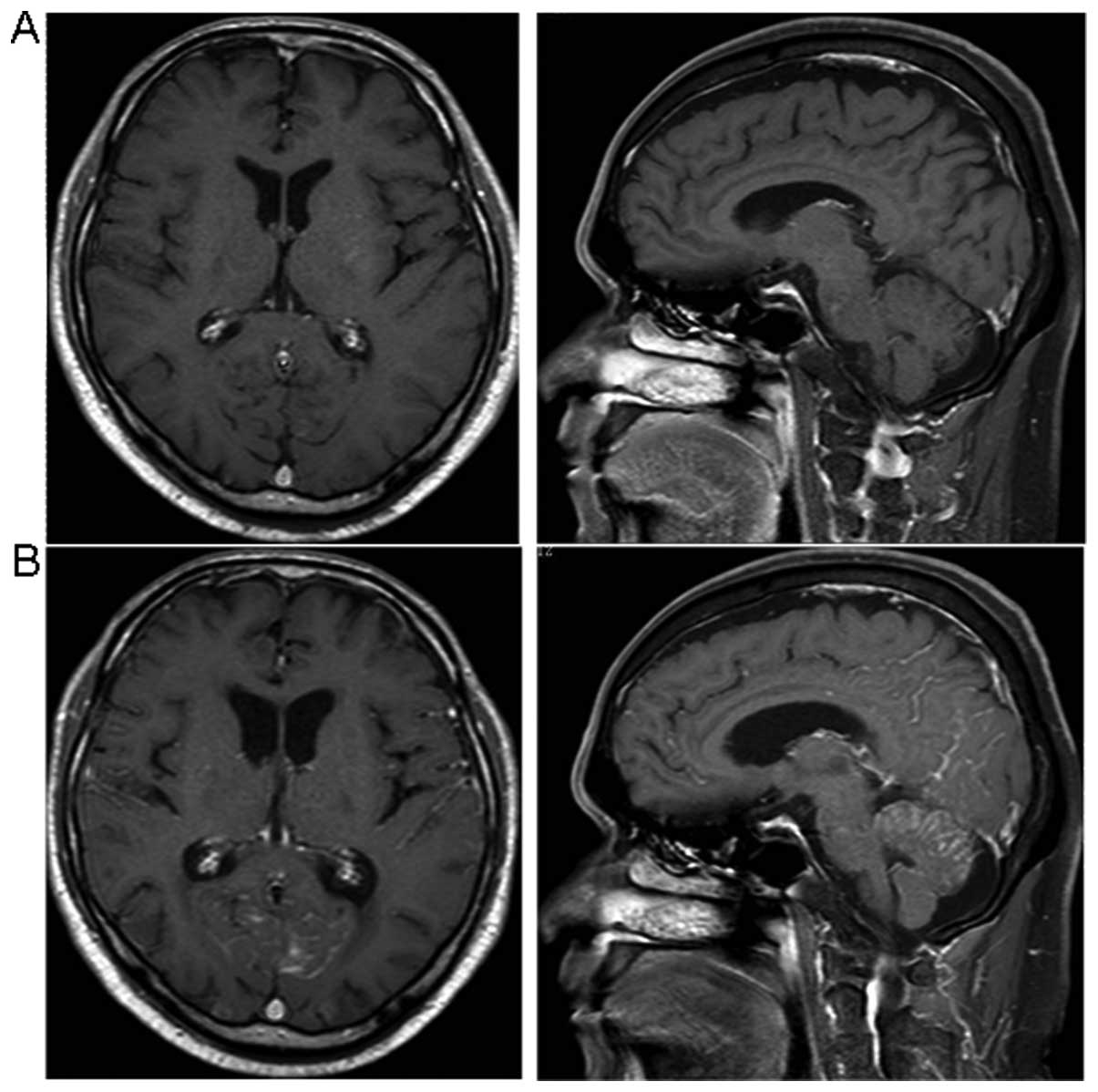
Figure 2 Referencing PMID 27017242, Sanctuary Site Leptomeningeal Metastases in HER-2 Positive Breast Cancer: A Review in the Era of Trastuzumab Contributed by Ayesha Anwar, MBBS
(Click Image to Enlarge)
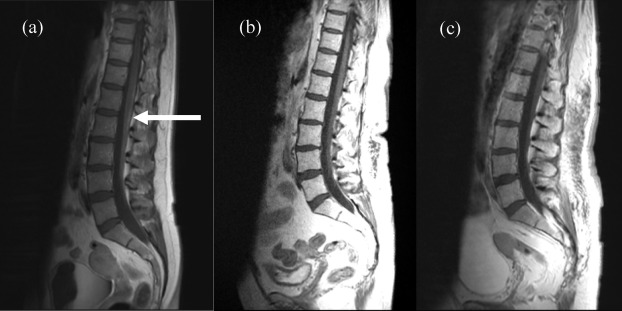
Figure 3 has a reference of PMID 22844374, A case of carcinomatous meningitis despite prophylactic cranial irradiation in small cell lung cancer during treatment with amrubicin. Contributed by Ayesha Anwar, MBBS
(Click Image to Enlarge)
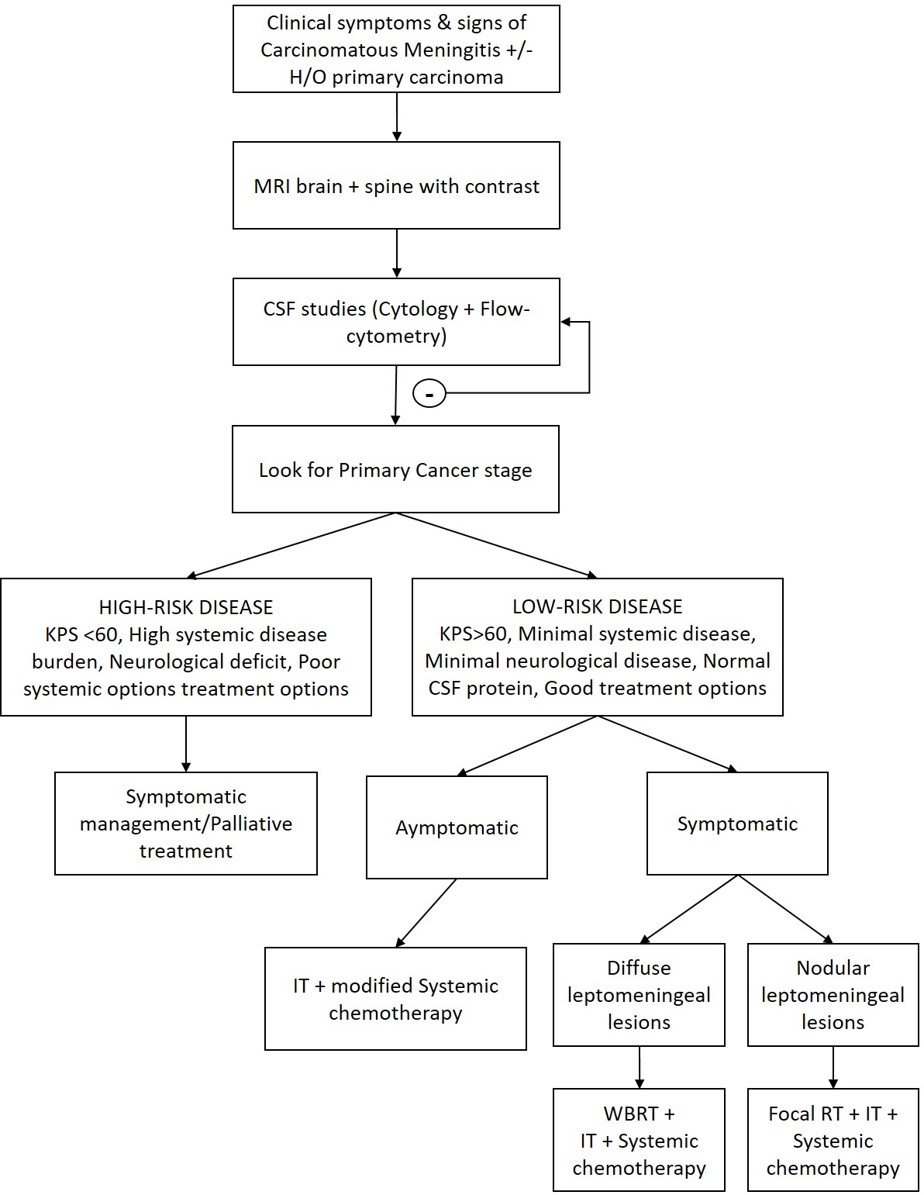
Meningitis, Carcinomatous Flow Chart Contributed by Ayesha Anwar, MBBS
References
Delle Grottaglie B, Girotti F, Ghisolfi A, Tafi A, Pescia M. A case of carcinomatous meningitis with papilledema as the only symptom: favorable response to intrathecal chemotherapy. Italian journal of neurological sciences. 1983 Apr:4(1):95-7 [PubMed PMID: 6688066]
Level 3 (low-level) evidenceWang N, Bertalan MS, Brastianos PK. Leptomeningeal metastasis from systemic cancer: Review and update on management. Cancer. 2018 Jan 1:124(1):21-35. doi: 10.1002/cncr.30911. Epub 2017 Nov 22 [PubMed PMID: 29165794]
Le Rhun E, Taillibert S, Chamberlain MC. Carcinomatous meningitis: Leptomeningeal metastases in solid tumors. Surgical neurology international. 2013:4(Suppl 4):S265-88. doi: 10.4103/2152-7806.111304. Epub 2013 May 2 [PubMed PMID: 23717798]
Clarke JL, Perez HR, Jacks LM, Panageas KS, Deangelis LM. Leptomeningeal metastases in the MRI era. Neurology. 2010 May 4:74(18):1449-54. doi: 10.1212/WNL.0b013e3181dc1a69. Epub [PubMed PMID: 20439847]
Level 2 (mid-level) evidenceThakkar JP, Kumthekar P, Dixit KS, Stupp R, Lukas RV. Leptomeningeal metastasis from solid tumors. Journal of the neurological sciences. 2020 Apr 15:411():116706. doi: 10.1016/j.jns.2020.116706. Epub 2020 Jan 23 [PubMed PMID: 32007755]
Moosavi L, D'Assumpcao C, Bowen J, Heidari A, Cobos E. Leptomeningeal Carcinomatosis From Carcinoma of Unknown Primary in a Young Patient: A Case Report and a Literature Review. Journal of investigative medicine high impact case reports. 2019 Jan-Dec:7():2324709619869380. doi: 10.1177/2324709619869380. Epub [PubMed PMID: 31423841]
Level 3 (low-level) evidenceMcGuire S. World Cancer Report 2014. Geneva, Switzerland: World Health Organization, International Agency for Research on Cancer, WHO Press, 2015. Advances in nutrition (Bethesda, Md.). 2016 Mar:7(2):418-9. doi: 10.3945/an.116.012211. Epub 2016 Mar 15 [PubMed PMID: 26980827]
Level 3 (low-level) evidenceGBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (London, England). 2016 Oct 8:388(10053):1459-1544. doi: 10.1016/S0140-6736(16)31012-1. Epub [PubMed PMID: 27733281]
Level 1 (high-level) evidenceArshad F, Wang L, Sy C, Avraham S, Avraham HK. Blood-brain barrier integrity and breast cancer metastasis to the brain. Pathology research international. 2010 Dec 29:2011():920509. doi: 10.4061/2011/920509. Epub 2010 Dec 29 [PubMed PMID: 21253507]
Sagar SM. Carcinomatous Meningitis: it does not have to be a death sentence. Oncology (Williston Park, N.Y.). 2002 Feb:16(2):237-43; discussion 244, 249-50 [PubMed PMID: 11866138]
Level 3 (low-level) evidencePicarelli H, Oliveira ML, Marta GN, Solla DJF, Teixeira MJ, Figueiredo EG. Mortality, Morbidity, and Prognostic Factors in the Surgical Resection of Brain Metastases: A Contemporary Cohort Study. Journal of neurological surgery. Part A, Central European neurosurgery. 2020 Jul:81(4):279-289. doi: 10.1055/s-0039-1696997. Epub 2020 Feb 27 [PubMed PMID: 32107755]
Ma R, Levy M, Gui B, Lu SE, Narra V, Goyal S, Danish S, Hanft S, Khan AJ, Malhotra J, Motwani S, Jabbour SK. Risk of leptomeningeal carcinomatosis in patients with brain metastases treated with stereotactic radiosurgery. Journal of neuro-oncology. 2018 Jan:136(2):395-401. doi: 10.1007/s11060-017-2666-7. Epub 2017 Nov 20 [PubMed PMID: 29159778]
Jung JM, Kim S, Joo J, Shin KH, Gwak HS, Lee SH. Incidence and risk factors for leptomeningeal carcinomatosis in breast cancer patients with parenchymal brain metastases. Journal of Korean Neurosurgical Society. 2012 Sep:52(3):193-9. doi: 10.3340/jkns.2012.52.3.193. Epub 2012 Sep 30 [PubMed PMID: 23115660]
Huang AJ, Huang KE, Page BR, Ayala-Peacock DN, Lucas JT Jr, Lesser GJ, Laxton AW, Tatter SB, Chan MD. Risk factors for leptomeningeal carcinomatosis in patients with brain metastases who have previously undergone stereotactic radiosurgery. Journal of neuro-oncology. 2014 Oct:120(1):163-9. doi: 10.1007/s11060-014-1539-6. Epub 2014 Jul 22 [PubMed PMID: 25048529]
Level 2 (mid-level) evidenceLara-Medina F, Crismatt A, Villarreal-Garza C, Alvarado-Miranda A, Flores-Hernández L, González-Pinedo M, Gamboa-Vignolle C, Ruiz-González JD, Arrieta O. Clinical features and prognostic factors in patients with carcinomatous meningitis secondary to breast cancer. The breast journal. 2012 May-Jun:18(3):233-41. doi: 10.1111/j.1524-4741.2012.01228.x. Epub 2012 Apr 5 [PubMed PMID: 22487060]
Clarke JL. Leptomeningeal metastasis from systemic cancer. Continuum (Minneapolis, Minn.). 2012 Apr:18(2):328-42. doi: 10.1212/01.CON.0000413661.58045.e7. Epub [PubMed PMID: 22810130]
Level 3 (low-level) evidenceRigakos G, Liakou CI, Felipe N, Orkoulas-Razis D, Razis E. Clinical Presentation, Diagnosis, and Radiological Findings of Neoplastic Meningitis. Cancer control : journal of the Moffitt Cancer Center. 2017 Jan:24(1):9-21 [PubMed PMID: 28178708]
Waki F, Ando M, Takashima A, Yonemori K, Nokihara H, Miyake M, Tateishi U, Tsuta K, Shimada Y, Fujiwara Y, Tamura T. Prognostic factors and clinical outcomes in patients with leptomeningeal metastasis from solid tumors. Journal of neuro-oncology. 2009 Jun:93(2):205-12. doi: 10.1007/s11060-008-9758-3. Epub 2008 Nov 29 [PubMed PMID: 19043775]
Level 2 (mid-level) evidenceTaillibert S, Laigle-Donadey F, Chodkiewicz C, Sanson M, Hoang-Xuan K, Delattre JY. Leptomeningeal metastases from solid malignancy: a review. Journal of neuro-oncology. 2005 Oct:75(1):85-99 [PubMed PMID: 16215819]
Nayar G, Ejikeme T, Chongsathidkiet P, Elsamadicy AA, Blackwell KL, Clarke JM, Lad SP, Fecci PE. Leptomeningeal disease: current diagnostic and therapeutic strategies. Oncotarget. 2017 Sep 22:8(42):73312-73328. doi: 10.18632/oncotarget.20272. Epub 2017 Aug 16 [PubMed PMID: 29069871]
Foo CT, Burrell LM, Johnson DF. An unusual presentation of carcinomatous meningitis. Oxford medical case reports. 2016 Aug:2016(8):omw068. doi: 10.1093/omcr/omw068. Epub 2016 Aug 25 [PubMed PMID: 27574561]
Level 3 (low-level) evidenceChamberlain MC, Corey-Bloom J. Leptomeningeal metastases: 111indium-DTPA CSF flow studies. Neurology. 1991 Nov:41(11):1765-9 [PubMed PMID: 1944906]
Taillibert S, Chamberlain MC. Leptomeningeal metastasis. Handbook of clinical neurology. 2018:149():169-204. doi: 10.1016/B978-0-12-811161-1.00013-X. Epub [PubMed PMID: 29307353]
Bigner SH. Cerebrospinal fluid (CSF) cytology: current status and diagnostic applications. Journal of neuropathology and experimental neurology. 1992 May:51(3):235-45 [PubMed PMID: 1583530]
Malkin MG, Posner JB. Cerebrospinal fluid tumor markers for the diagnosis and management of leptomeningeal metastases. European journal of cancer & clinical oncology. 1987 Jan:23(1):1-4 [PubMed PMID: 3297711]
Corsini E, Bernardi G, Gaviani P, Silvani A, de Grazia U, Ciusani E, Croci D, Salmaggi A. Intrathecal synthesis of tumor markers is a highly sensitive test in the diagnosis of leptomeningeal metastasis from solid cancers. Clinical chemistry and laboratory medicine. 2009:47(7):874-9. doi: 10.1515/CCLM.2009.183. Epub [PubMed PMID: 19453289]
Level 3 (low-level) evidenceBruna J, González L, Miró J, Velasco R, Gil M, Tortosa A, Neuro-Oncology Unit of the Institute of Biomedical Investigation of Bellvitge. Leptomeningeal carcinomatosis: prognostic implications of clinical and cerebrospinal fluid features. Cancer. 2009 Jan 15:115(2):381-9. doi: 10.1002/cncr.24041. Epub [PubMed PMID: 19109820]
Warley F, Bonella MB, Giunta DH, Elizondo CM, Ferreyro BL. [Associated factors with the presence of secondary neoplastic cells in the cerebrospinal fluid of patients with suspected carcinomatous meningitis]. Revista de la Facultad de Ciencias Medicas (Cordoba, Argentina). 2017:74(1):26-32 [PubMed PMID: 28379128]
Grossman SA, Trump DL, Chen DC, Thompson G, Camargo EE. Cerebrospinal fluid flow abnormalities in patients with neoplastic meningitis. An evaluation using 111indium-DTPA ventriculography. The American journal of medicine. 1982 Nov:73(5):641-7 [PubMed PMID: 6814249]
Glantz MJ, Hall WA, Cole BF, Chozick BS, Shannon CM, Wahlberg L, Akerley W, Marin L, Choy H. Diagnosis, management, and survival of patients with leptomeningeal cancer based on cerebrospinal fluid-flow status. Cancer. 1995 Jun 15:75(12):2919-31 [PubMed PMID: 7773943]
Freilich RJ, Krol G, DeAngelis LM. Neuroimaging and cerebrospinal fluid cytology in the diagnosis of leptomeningeal metastasis. Annals of neurology. 1995 Jul:38(1):51-7 [PubMed PMID: 7611725]
Ko Y, Gwak HS, Park EY, Joo J, Lee YJ, Lee SH, Kwon JW, Shin SH, Yoo H. Association of MRI findings with clinical characteristics and prognosis in patients with leptomeningeal carcinomatosis from non-small cell lung cancer. Journal of neuro-oncology. 2019 Jul:143(3):553-562. doi: 10.1007/s11060-019-03190-3. Epub 2019 May 14 [PubMed PMID: 31089925]
Bier G, Klumpp B, Roder C, Garbe C, Preibsch H, Ernemann U, Hempel JM. Meningeal enhancement depicted by magnetic resonance imaging in tumor patients: neoplastic meningitis or therapy-related enhancement? Neuroradiology. 2019 Jul:61(7):775-782. doi: 10.1007/s00234-019-02215-y. Epub 2019 Apr 18 [PubMed PMID: 31001647]
Kordbacheh T, Law WY, Smith IE. Sanctuary site leptomeningeal metastases in HER-2 positive breast cancer: A review in the era of trastuzumab. Breast (Edinburgh, Scotland). 2016 Apr:26():54-8. doi: 10.1016/j.breast.2015.11.005. Epub 2016 Jan 22 [PubMed PMID: 27017242]
Oguri T, Uemura T, Kunii E, Ozasa H, Ohkubo H, Miyazaki M, Maeno K, Sato S. A case of carcinomatous meningitis despite prophylactic cranial irradiation in small cell lung cancer during treatment with amrubicin. Oncology letters. 2012 Aug:4(2):305-306 [PubMed PMID: 22844374]
Level 3 (low-level) evidenceEl Shafie RA, Böhm K, Weber D, Lang K, Schlaich F, Adeberg S, Paul A, Haefner MF, Katayama S, Hörner-Rieber J, Hoegen P, Löw S, Debus J, Rieken S, Bernhardt D. Palliative Radiotherapy for Leptomeningeal Carcinomatosis-Analysis of Outcome, Prognostic Factors, and Symptom Response. Frontiers in oncology. 2018:8():641. doi: 10.3389/fonc.2018.00641. Epub 2019 Jan 8 [PubMed PMID: 30671384]
Roth P, Weller M. Management of neoplastic meningitis. Chinese clinical oncology. 2015 Jun:4(2):26. doi: 10.3978/j.issn.2304-3865.2015.05.02. Epub [PubMed PMID: 26112812]
Chang EL, Maor MH. Standard and novel radiotherapeutic approaches to neoplastic meningitis. Current oncology reports. 2003 Jan:5(1):24-8 [PubMed PMID: 12493147]
Level 3 (low-level) evidenceBuszek SM, Chung C. Radiotherapy in Leptomeningeal Disease: A Systematic Review of Randomized and Non-randomized Trials. Frontiers in oncology. 2019:9():1224. doi: 10.3389/fonc.2019.01224. Epub 2019 Nov 15 [PubMed PMID: 31803614]
Level 2 (mid-level) evidenceHitchins RN, Bell DR, Woods RL, Levi JA. A prospective randomized trial of single-agent versus combination chemotherapy in meningeal carcinomatosis. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 1987 Oct:5(10):1655-62 [PubMed PMID: 3309199]
Level 1 (high-level) evidenceGlantz MJ, Van Horn A, Fisher R, Chamberlain MC. Route of intracerebrospinal fluid chemotherapy administration and efficacy of therapy in neoplastic meningitis. Cancer. 2010 Apr 15:116(8):1947-52. doi: 10.1002/cncr.24921. Epub [PubMed PMID: 20151421]
Level 1 (high-level) evidenceLeal T, Chang JE, Mehta M, Robins HI. Leptomeningeal Metastasis: Challenges in Diagnosis and Treatment. Current cancer therapy reviews. 2011 Nov:7(4):319-327 [PubMed PMID: 23251128]
Level 3 (low-level) evidenceMaur M, Omarini C, Piacentini F, Fontana A, Pettorelli E, Cascinu S. Metronomic Capecitabine Effectively Blocks Leptomeningeal Carcinomatosis From Breast Cancer: A Case Report and Literature Review. The American journal of case reports. 2017 Feb 28:18():208-211 [PubMed PMID: 28242865]
Level 3 (low-level) evidenceMorichika D, Kubo T, Gotoda H, Tamura T, Ohashi K, Hotta K, Tabata M, Kurozumi K, Tanimoto M, Kiura K. Efficacy of multimodal treatment for leptomeningeal metastases in a lung cancer harboring an EGFR mutation. OncoTargets and therapy. 2016:9():1753-8. doi: 10.2147/OTT.S95721. Epub 2016 Mar 22 [PubMed PMID: 27042125]
Duchnowska R, Loibl S, Jassem J. Tyrosine kinase inhibitors for brain metastases in HER2-positive breast cancer. Cancer treatment reviews. 2018 Jun:67():71-77. doi: 10.1016/j.ctrv.2018.05.004. Epub 2018 May 9 [PubMed PMID: 29772459]
Kim DW, Barcena E, Mehta UN, Rohlfs ML, Kumar AJ, Penas-Prado M, Kim KB. Prolonged survival of a patient with metastatic leptomeningeal melanoma treated with BRAF inhibition-based therapy: a case report. BMC cancer. 2015 May 13:15():400. doi: 10.1186/s12885-015-1391-x. Epub 2015 May 13 [PubMed PMID: 25962795]
Level 3 (low-level) evidenceLi G, Dai WR, Shao FC. Effect of ALK-inhibitors in the treatment of non-small cell lung cancer: a systematic review and meta-analysis. European review for medical and pharmacological sciences. 2017 Aug:21(15):3496-3503 [PubMed PMID: 28829490]
Level 1 (high-level) evidenceLi N, Yang BY, Li JL, Zhu JQ, Zou BH, Wang YF, Yu L, Yao XY. [Clinical features and prognostic factors in patients with leptomeningeal metastases]. Zhonghua zhong liu za zhi [Chinese journal of oncology]. 2013 Nov:35(11):867-70 [PubMed PMID: 24447488]
Level 2 (mid-level) evidenceMrugala MM, Kim B, Sharma A, Johnson N, Graham C, Kurland BF, Gralow J. Phase II Study of Systemic High-dose Methotrexate and Intrathecal Liposomal Cytarabine for Treatment of Leptomeningeal Carcinomatosis From Breast Cancer. Clinical breast cancer. 2019 Oct:19(5):311-316. doi: 10.1016/j.clbc.2019.04.004. Epub 2019 Apr 18 [PubMed PMID: 31175053]
Lee SJ, Lee JI, Nam DH, Ahn YC, Han JH, Sun JM, Ahn JS, Park K, Ahn MJ. Leptomeningeal carcinomatosis in non-small-cell lung cancer patients: impact on survival and correlated prognostic factors. Journal of thoracic oncology : official publication of the International Association for the Study of Lung Cancer. 2013 Feb:8(2):185-91. doi: 10.1097/JTO.0b013e3182773f21. Epub [PubMed PMID: 23328548]
Level 2 (mid-level) evidenceHyun JW, Jeong IH, Joung A, Cho HJ, Kim SH, Kim HJ. Leptomeningeal metastasis: Clinical experience of 519 cases. European journal of cancer (Oxford, England : 1990). 2016 Mar:56():107-114. doi: 10.1016/j.ejca.2015.12.021. Epub 2016 Feb 1 [PubMed PMID: 26841095]
Level 3 (low-level) evidenceDeAngelis LM. Current diagnosis and treatment of leptomeningeal metastasis. Journal of neuro-oncology. 1998 Jun-Jul:38(2-3):245-52 [PubMed PMID: 9696379]