
Introduction
Boutonniere deformity describes a medical condition in which the finger is flexed at the proximal interphalangeal joint (PIP) and hyperextended at the distal interphalangeal joint (DIP). This is usually a result of trauma in the acute setting and is caused by a rupture of the PIP central slip. This results in damage to the extensor function of the affected digit. A boutonniere deformity can also result from laceration injury to the central slip and dorsal capsule. [1] [2] Boutonniere deformities can also occur secondary to burn injury, with tension ischemia representing a possible etiology for tendon rupture. [3] Overall, Boutonniere deformities common represent sequela of inflammatory arthritides, such as rheumatoid arthritis.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Injury to the extensor tendon is the chief etiology for this flexion deformity of the PIP joint. The extensor tendon is disrupted and the lateral aspects of the tendon separate. The head of the proximal phalanx subsequently projects through the disrupted tendon elements. This deformity obtained its name presumably due to its appearance to a buttonhole on surgical exploration.[5] Football and basketball-related injuries are the most common sources of sports-related boutonniere deformities.
Epidemiology
While jam-injuries represent a heterogeneous group of trauma-related injuries, central slip injuries and subsequent development of boutonniere deformities constitute a well-known sequela of jam-injuries. [6] Up to half or 50% of patients with rheumatoid arthritis develop a boutonniere deformity in at least one digit. [7]
Pathophysiology
A boutonniere deformity results when the triangular ligament and the central slip of the extensor tendon of a digit are disrupted. This disruption of the ligament and tendon will cause the lateral bands to displace volarly. This results in forced flexion of the finger, and subsequent limitation of the DIP joint to extend. Over time, the oblique retinacular ligament gradually contracts. This ligament contracture will gradually worsen the hyperextension deformity of the joint. [8] The pathophysiology is different if it is secondary to rheumatoid arthritis (RA) or a burn injury. In the setting of inflammatory arthritides such as RA, inflammatory cells collect in the synovial fluid of the joint which forms a layer of fibrous tissue. This leads to bony erosion and damage to cartilage and ligaments. The joints gradually deform which leads to loss of function and pain.
History and Physical
A thorough history and physical should be obtained to determine the mechanism of injury to the affected digit. Treatment options vary depending on etiology and early identification of injury can prevent long-term complications and deformities from these injuries. A deformity can take several weeks to manifest. In the setting of a laceration injury, the area needs to be thoroughly cleaned and examined in a “bloodless field” for tendon integrity. [9] In the setting of "jam injuries," a central slip injury is oftentimes occult. The "Elson test" can be performed to assess tendon integrity, and involves the following steps [6]:
- The patient places his affected finger over the edge of a surface such as a table. The digits are placed in a flexed position along the surface edge at the level of the PIP joint.
- The examiner applies pressure to the digit at the level of the middle phalanx.
- The patient is instructed to extend the finger at the PIP joint(opposite to the vector of pressure).
- A positive test is confirmed when the DIP is noted to hyperextend at the DIP joint.
If rheumatoid arthritis causes a boutonniere deformity, a thorough history should include the duration of symptoms, medications (both previous and current), level of pain, and degree of disability.[10]
Evaluation
Radiographs are indicated to determine if there are any associated fractures. It is also important to identify any cortical disruption of the bones that attach to the central slip of the tendon. Lateral radiographs can be used to determine the degree of hyperextension.
Treatment / Management
The goal of treatment is to regain full range of motion of the affected finger. Treatment options include both surgical and nonsurgical modalities. Splinting is a nonsurgical treatment and involves immobilizing the affected joint to allow for PIP flexion(straightening) to occur. This also allows the tendon to heal and not continue to volarly separate. Splints are usually maintained for 3 to 6 weeks depending on the patient’s age and severity of the injury. [11] Patients will often be instructed to wear the splint at night for several more weeks. Management should also include exercises to improve the strength and flexibility of the affected digit. If the injury is a result of sports activity, the affected area may be taped or further splinted for protection on activity resumption. Surgical correction can be employed if the tendon is severed or if there is a significant bone fragment displaced from its normal position of function. [12] It may also be an option if it does not improve with conservative measures, such as splinting. If a large avulsion is present, surgical fixation with a wire or screw is used to correct for the extensor injury. The deformity becomes more difficult to correct if the deformity has been left untreated for greater than three weeks.
The treatment options for a boutonniere deformity if it represents a chronic sequela of rheumatoid arthritis. The classes of medications to treat rheumatoid arthritis are disease-modifying anti-rheumatic drugs (DMARDs), biologic response modifiers, glucocorticoids, nonsteroidal anti-inflammatory medications (NSAIDs), and analgesics. DMARDs are used to delay the progression of rheumatoid arthritis. DMARDs have different mechanisms of action and are often used in combination therapy. Although the mechanism of action varies, they have a similar impact on the disease process. Biologic response modifiers are genetically engineered and work by interrupting a patient’s immune system signals that are responsible for tissue damage. Most of these medications attempt to interfere with the activity of tumor necrosis factor. Glucocorticoids are used to reduce inflammation and also to curb the autoimmune activity. They are often used in conjunction with DMARDs. NSAIDs can aid with pain control, swelling, and inflammation, but do not affect slowing the disease process. Analgesics are used to control pain only.
If nonsurgical measures are unsuccessful, surgical joint replacement may be necessary. Joint fusion is another surgical procedure that involves fusing the two joint surfaces of the affected digit together. The benefits of joint fusion are pain improvement, increased the stability of the joint, and prevention of worsening joint deformity. After surgery, patients are instructed to wear a splint or brace for several weeks to keep the proximal interphalangeal joint straight. [7] Physical or occupational therapy often follows splinting.
Differential Diagnosis
- Dislocation of the PIP joint. Classically this is traumatic in etiology and the deformity is often more pronounced.
- Skin contracture at the proximal finger from burn injury.
- Less common causes of contractures from other pathologies (Hansen's disease, epidermolysis bullosa, etc).
Prognosis
Preventing progression to a boutonniere deformity is the chief goal of good treatment outcomes. Serial digital casting has been shown to be moderately successful. [11] Depending on severity of the injury, a complete recovery with relation to range of motion is infrequently seen. [11]
Complications
Complications with or without treatment include [13]:
- Chronic joint stiffness
- Reinjury/redislocation
- Post-traumatic arthritis
- Chronic swelling
- Decreased range of motion
Deterrence and Patient Education
Considering that prognosis and outcomes are often varied with patients rarely returning to baseline functionality, the physician plays an important role in managing expectations. Patients should be educated on various complications such as limited chronic range of motion, early arthritis, and predisposition to reinjury. A physician managing athletes, especially those predisposed to finger injuries such as football and basketball players, should advice his/her patients to present early in the setting of jam-injuries of the fingers. Educating patients that a delay in management can have possible long term sequela that could limit further participation in sports.
Enhancing Healthcare Team Outcomes
The diagnosis and management of boutonniere deformity is complex and requires an interprofessional team that includes a primary care provider, nurse practitioner, physical therapist, hand surgeon, and orthopedic surgeon. The goal of treatment is to regain full range of motion of the affected finger. Treatment options include both surgical and nonsurgical modalities. If nonsurgical measures are unsuccessful, surgical joint replacement may be necessary. Joint fusion is another surgical procedure that involves fusing the two joint surfaces of the affected digit together. The benefits of joint fusion are pain improvement, increased the stability of the joint, and prevention of worsening joint deformity. After surgery, patients are instructed to wear a splint or brace for several weeks to keep the proximal interphalangeal joint straight.[7] Physical or occupational therapy often follows splinting. The outcomes for boutonniere deformity are guarded. While recovery is possible, it may take a long time to improve range of motion and function.[14][15] (Level V)
Media
(Click Image to Enlarge)
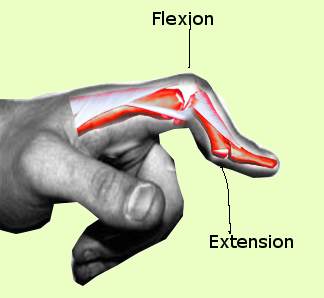
Boutonniere Deformity Contributed by Steve Bhmiji, MD, MS, PhD
(Click Image to Enlarge)

Boutonniere deformity of the 5th digit. Contributed by Dr.Rebecca Flores.
(Click Image to Enlarge)

Boutonniere deformity of the 5th digit. Contributed by Dr.Rebecca Flores.
(Click Image to Enlarge)

Boutonniere deformity of the 5th digit. Contributed by Dr.Rebecca Flores.
References
Pencle FJ, Doehrmann R, Waseem M. Fingertip Injuries. StatPearls. 2023 Jan:(): [PubMed PMID: 28613777]
Boussakri H, Azarkane M, Dahmani O, Elidrissi M, Shimi M, Elibrahimi A, Elmrini A. Unusual combination of lesions of the traumatic hand: closed central slip laceration of the extensor and interphalangeal thumb joint's dislocation (a case report). The Pan African medical journal. 2014:18():230. doi: 10.11604/pamj.2014.18.230.3240. Epub 2014 Jul 18 [PubMed PMID: 25426188]
Level 3 (low-level) evidenceSabapathy SR, Bajantri B, Bharathi RR. Management of post burn hand deformities. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2010 Sep:43(Suppl):S72-9. doi: 10.4103/0970-0358.70727. Epub [PubMed PMID: 21321661]
Vedel PN, Tranum-Jensen J, Dahlin LB, Brogren E, Søe NH. [Deformities of the finger joints]. Ugeskrift for laeger. 2017 Nov 27:179(48):. pii: V04170324. Epub [PubMed PMID: 29208202]
Grau L, Baydoun H, Chen K, Sankary ST, Amirouche F, Gonzalez MH. Biomechanics of the Acute Boutonniere Deformity. The Journal of hand surgery. 2018 Jan:43(1):80.e1-80.e6. doi: 10.1016/j.jhsa.2017.07.011. Epub 2017 Sep 7 [PubMed PMID: 28888567]
Carruthers KH, Skie M, Jain M. Jam Injuries of the Finger: Diagnosis and Management of Injuries to the Interphalangeal Joints Across Multiple Sports and Levels of Experience. Sports health. 2016 Sep:8(5):469-78. doi: 10.1177/1941738116658643. Epub 2016 Jul 15 [PubMed PMID: 27421747]
Sood A, Kotamarti VS, Granick MS. Boutonnière Deformity Following Volar Proximal Interphalangeal Joint Dislocation. Eplasty. 2016:16():ic25 [PubMed PMID: 27347279]
Bai RJ, Zhang HB, Zhan HL, Qian ZH, Wang NL, Liu Y, Li WT, Yin YM. Sports Injury-Related Fingers and Thumb Deformity Due to Tendon or Ligament Rupture. Chinese medical journal. 2018 May 5:131(9):1051-1058. doi: 10.4103/0366-6999.230721. Epub [PubMed PMID: 29692376]
Level 2 (mid-level) evidenceTaqi M, Collins A. Finger Dislocation. StatPearls. 2023 Jan:(): [PubMed PMID: 31855352]
Sharif K, Sharif A, Jumah F, Oskouian R, Tubbs RS. Rheumatoid arthritis in review: Clinical, anatomical, cellular and molecular points of view. Clinical anatomy (New York, N.Y.). 2018 Mar:31(2):216-223. doi: 10.1002/ca.22980. Epub 2017 Oct 27 [PubMed PMID: 28833647]
McCue FC, Honner R, Johnson MC, Gieck JH. Athletic injuries of the proximal interphalangeal joint requiring surgical treatment. The Journal of bone and joint surgery. American volume. 1970 Jul:52(5):937-56 [PubMed PMID: 5479483]
Fox PM, Chang J. Treating the Proximal Interphalangeal Joint in Swan Neck and Boutonniere Deformities. Hand clinics. 2018 May:34(2):167-176. doi: 10.1016/j.hcl.2017.12.006. Epub [PubMed PMID: 29625636]
Kamnerdnakta S, Huetteman HE, Chung KC. Complications of Proximal Interphalangeal Joint Injuries: Prevention and Treatment. Hand clinics. 2018 May:34(2):267-288. doi: 10.1016/j.hcl.2017.12.014. Epub [PubMed PMID: 29625645]
Hirth MJ, Howell JW, O'Brien L. Relative motion orthoses in the management of various hand conditions: A scoping review. Journal of hand therapy : official journal of the American Society of Hand Therapists. 2016 Oct-Dec:29(4):405-432. doi: 10.1016/j.jht.2016.07.001. Epub 2016 Oct 25 [PubMed PMID: 27793417]
Level 2 (mid-level) evidenceMcKeon KE, Lee DH. Posttraumatic Boutonnière and Swan Neck Deformities. The Journal of the American Academy of Orthopaedic Surgeons. 2015 Oct:23(10):623-32. doi: 10.5435/JAAOS-D-14-00272. Epub 2015 Aug 28 [PubMed PMID: 26320165]