Introduction
Bile acids are steroidal acids found in bile. Primary bile acids are steroids produced via the liver, specifically in peroxisomes.[1][2][3] There, the acids conjugate/connect to hydrophilic amino acids, namely glycine/taurine (i.e., conjugated bile acids called glycocholic and taurocholic acids, respectively); alongside sodium/potassium, they are termed bile salts.[4][5] Secondary bile acids, however, are made via colonic bacteria. Of the organic compounds found in bile, bile acids constitute the large majority.[6][7] Right after being synthesized, bile acids are secreted into bile and concentrated for storage in the gallbladder. Eating then stimulates cholecystokinin release, which causes gallbladder contraction--releasing its bile acids into the duodenum through the sphincter of Oddi.[8][9] The more bile acid that gets secreted, the faster that bile flows. The primary purpose of bile acids is to facilitate the digestion of fat via its surfactant properties, which emulsify fats into micelles.[10] Hormonally, bile acids are also ligands for the farnesoid X receptor (FXR) and GPBAR1 (TGR5).[11] In sum, the three main functions of bile acids are to (1) emulsify fat, (2) excrete cholesterol, and (3) have an antimicrobial effect.[1]
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
Bile acids get conjugated in the liver to increase their water solubility because bile salts have a decreased pK, which favors the basic anionic form in the acidic duodenum. As amphiphiles, conjugated bile salts have a hydrophobic and hydrophilic side that, hence, their function as surfactants. The hydrophobic portion faces lipids, the hydrophilic portion facing the water, which allows them to act as bridges at the lipid/water interface, where they can make micelles when sufficiently concentrated.[2] Micelles, with their bile acids, can support the function of lipases in digesting lipids and also bring them close to the intestine's brush border, augmenting their absorption. Lipids are normally water-insoluble, and the stomach and intestines are full of water. If not for the action of bile, dietary lipids and water would not separate, and water-soluble lipases would inefficiently exert their effects at the small interface between water and lipids. The emulsification of lipids by bile salts thus suspends lipid particles in water to dissolve them, accordingly granting significantly more surface area for lipase action.[10][11]
Other functions of bile acids include removing the body's cholesterol, powering bile flow to remove various metabolites (like bilirubin), and facilitating the removal of bacterial flora of the small bowel and biliary tree (e.g., by disrupting their cellular membranes).[6] Bile acids also hormonally act on the FXR and TGR5 receptors. Control over bile acid concentrations is important because of their potential cytotoxicity, so FXR elicits functions primarily in the liver/intestines that include feedback regulation of bile acid concentration, in addition to regulating triglyceride levels and other biochemical functions.[12][13][14][15] Secondary bile acids, e.g., deoxycholic acid, may have implications in more strongly downregulating bile acid synthesis than primary bile acids when it comes to negative feedback.[16] The TGR5 receptor is involved in the regulation of energy homeostasis by bile acids.[17][18] In addition to its effects on the above-mentioned hormone receptors, bile acids target other proteins like N-acyl phosphatidylethanolamine-specific phospholipase D, involved in pathways related to stress/pain responses, appetite, and lifespan via crosstalk between lipid amide signals with bile acids. Other miscellaneous functions under the purview of bile acids potentially include the regulation of particular enzymes/ion channels and the synthesis of various substances.[19][20][21][17]
Mechanism
Altogether, bile salts comprise a broad variety of different molecules, each being a steroid with the following basic components: (1) 4 rings, (2) a 5-/8-carbon side chain that ends with a carboxylic acid, and (3) a number of hydroxyl groups (whose position/number changes among the various salts). The rings are ascribed the letters A, B, C, and D based on their distance from the side chain with the -COOH group, the D ring being the most distant (as well as being 1 C smaller than the other rings). Beta hydroxyl groups face up/out, alpha groups down, and every bile acid has a 3-hydroxyl group that came from their cholesterol precursor.[1]
Primary bile acids are made by hepatocytes either by the classic or acidic pathway. The former, which constitutes 95% of bile acid synthesis, is via cytochrome P450-mediated oxidation of cholesterol that requires NADPH and oxygen and occurs in a series of steps, the most important of which is the rate-limiting hydroxylation of the 7th steroid nucleus of cholesterol by cholesterol 7alpha-hydroxylase (CYP7A1) to create 7alpha-hydroxycholesterol. That then gets metabolized into 7alpha-hydroxy-4 cholesten-3-one in the second step. In sum, primary bile acid synthesis requires 14 enzymatic steps. The most common bile acids are cholic and chenodeoxycholic acid (CDCA). Cholic acid (3alpha, 7alpha, 12alpha-trihydroxy-5beta-cholan-24-oic acid) is the commonest bile acid, and CDCA is the prototypical and most basic of bile acids produced and is also known as 3alpha,7alpha-dihydroxy-5beta-cholan-24-oic acid.[4]
The alternative/acidic pathway acts via mitochondrial sterol 27-hydroxylase (CYP27A1), found in the liver, macrophages, and other tissues. Before secretion of bile acids, hepatocytes conjugate them with the amino acids taurine or glycine, thereby creating eight different conjugated bile acids/salts (including cholic and chenocholic acids). CYP27A1 significantly adds to bile acid synthesis by facilitating the oxidation of sterol side chains, followed by a peroxisomal cleavage of a 3-C unit to generate a C24 bile acid. Miscellaneous pathways, in addition to these two, include those started by the liver's 25-hydroxylase and the brain's 24-hydroxylase.
The purpose of conjugation is so that the bile acids can become water-soluble and thereby emulsify fats.[2] Secondary bile acids are formed from bacterial deconjugation/dehydroxylation and removal of those amino acid groups, creating four more different types of bile acids (including deoxycholic and lithocholic acids). These acids are absorbed through the bloodstream and brought back to the liver via the enterohepatic circulation to then be resecreted. Most triglyceride absorption occurs at the jejunum, but the conjugated bile acids do not get absorbed along with them. Instead, the bile salts remain in the small intestine, where most are later absorbed and recycled by active transport at the terminal ileum (the remaining undergo fecal elimination). The end of the small intestine acting the site of bile salt absorption allows for a high concentration of bile salts to exist throughout the entire organ, maximizing lipid digestion and absorption.[5]
Pathophysiology
Bile acid synthesis defects comprise about 1 to 2% of the cholestatic diseases found in children.[22] With an autosomal recessive inheritance pattern, these defects have a spectrum of disease severity based on what they affect. Most commonly, these manifest as progressive cholestasis of infancy, in addition to other disorders like an advanced liver disease at birth or neonatal hepatitis; patients may also develop a liver disease later in childhood. Typically, an earlier onset of liver disease occurs with those enzymatic defects that result in a buildup of oxo-bile acids, which tend to be cholestatic.[23] Adult liver disease may also have a connection to inherited defects in bile synthesis, as well.[24]
Clinical Significance
Impairing enterohepatic circulation of bile acids decreases cholesterol because the liver is driven to use more cholesterol to make more. This state is the basis behind treating hyperlipidemia with bile acid resins like cholestyramine, colestipol, and colesevelam, which bind bile acids in the gut, preventing their reabsorption in the intestines. The bound bile acids are then fecally removed. However, because bile acid sequestrants also interfere with the absorption of fat, the absorption of drugs and fat-soluble vitamins are impaired.[25]
Structural/functional abnormalities of the biliary tract can produce an increase in bilirubin, causing jaundice, as well as an increase in serum bile acids. This observed cholestasis (disrupted bile flow to intestines) may also present with primary sclerosing cholangitis, intrahepatic cholestasis of pregnancy, and primary biliary cholangitis, where the buildup of bile acids can lead to pruritus because of the bile salts in skin.[26] Treating these disorders has involved ursodeoxycholic acid (ursodiol), a non-toxic bile acid that increases bile secretion and decreases cholesterol secretion/absorption. Obeticholic acid is a semisynthetic bile acid that can also treat primary biliary cirrhosis by stimulating FXR.[27][28]
Bile that has diluted concentrations of bile acids or phospholipids, in addition to increased cholesterol, leads to a decrease in the solubilization of cholesterol. This situation increases the risk for microcrystal formation from this supersaturated bile--eventually leading to the formation of cholesterol stones. Fibrates like gemfibrozil, bezafibrate, and fenofibrate also increase the risk of cholesterol gallstones by inhibiting cholesterol-7alpha-hydroxylase, resulting in decreased bile acid production.[29] Dissolution or prevention of these gallstones occurs with bile acid administration, in the form of chenodeoxycholic and/or ursodeoxycholic acid.[30][31]
Too much bile acid in the colon may precipitate chronic diarrhea, which may occur in conditions that impair the ileal absorption of bile salts, as seen with surgical removal for Crohn disease (which normally causes fat malabsorption by affecting the terminal ileum). Such malabsorption of bile acids is treatable with bile acid resins.[32]
There may also exist a link between bile acids and colorectal cancer.[33] Specifically, low fecal concentrations of bile acids have correlations with lower rates of colorectal cancer.[34][35][36] One potential explanation is that high concentrations of deoxycholic acid, a type of bile acid, can increase the generation of reactive oxygen species that can go on to damage DNA.[37][34]
Bile acids have also been used to get rid of undesired fat, i.e., mesotherapy, with deoxycholic acid being one such drug.[38][39]
Media
(Click Image to Enlarge)
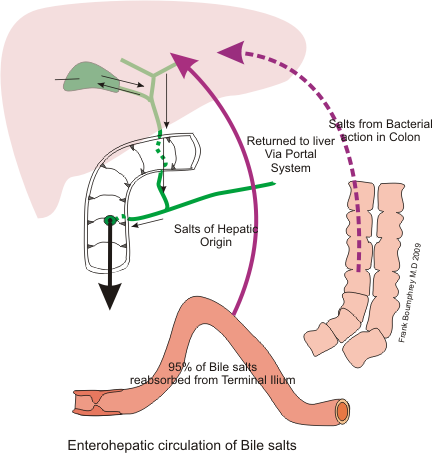
Recycling of bile Image courtesy: https://commons.wikimedia.org/wiki/File:Bile_recycling.png
References
Hofmann AF, Hagey LR, Krasowski MD. Bile salts of vertebrates: structural variation and possible evolutionary significance. Journal of lipid research. 2010 Feb:51(2):226-46. doi: 10.1194/jlr.R000042. Epub 2009 Jul 28 [PubMed PMID: 19638645]
Level 3 (low-level) evidenceHOFMANN AF. THE FUNCTION OF BILE SALTS IN FAT ABSORPTION. THE SOLVENT PROPERTIES OF DILUTE MICELLAR SOLUTIONS OF CONJUGATED BILE SALTS. The Biochemical journal. 1963 Oct:89(1):57-68 [PubMed PMID: 14097367]
Ferdinandusse S, Houten SM. Peroxisomes and bile acid biosynthesis. Biochimica et biophysica acta. 2006 Dec:1763(12):1427-40 [PubMed PMID: 17034878]
Level 3 (low-level) evidenceCarey MC, Small DM. Micelle formation by bile salts. Physical-chemical and thermodynamic considerations. Archives of internal medicine. 1972 Oct:130(4):506-27 [PubMed PMID: 4562149]
Chiang JY. Bile acids: regulation of synthesis. Journal of lipid research. 2009 Oct:50(10):1955-66. doi: 10.1194/jlr.R900010-JLR200. Epub 2009 Apr 3 [PubMed PMID: 19346330]
Level 3 (low-level) evidenceHofmann AF. The continuing importance of bile acids in liver and intestinal disease. Archives of internal medicine. 1999 Dec 13-27:159(22):2647-58 [PubMed PMID: 10597755]
Staels B, Fonseca VA. Bile acids and metabolic regulation: mechanisms and clinical responses to bile acid sequestration. Diabetes care. 2009 Nov:32 Suppl 2(Suppl 2):S237-45. doi: 10.2337/dc09-S355. Epub [PubMed PMID: 19875558]
Li T, Chiang JY. Bile acid signaling in metabolic disease and drug therapy. Pharmacological reviews. 2014 Oct:66(4):948-83. doi: 10.1124/pr.113.008201. Epub [PubMed PMID: 25073467]
Level 3 (low-level) evidence. . :(): [PubMed PMID: 31196634]
HOFMANN AF, BORGSTROEM B. THE INTRALUMINAL PHASE OF FAT DIGESTION IN MAN: THE LIPID CONTENT OF THE MICELLAR AND OIL PHASES OF INTESTINAL CONTENT OBTAINED DURING FAT DIGESTION AND ABSORPTION. The Journal of clinical investigation. 1964 Feb:43(2):247-57 [PubMed PMID: 14162533]
Fiorucci S, Mencarelli A, Palladino G, Cipriani S. Bile-acid-activated receptors: targeting TGR5 and farnesoid-X-receptor in lipid and glucose disorders. Trends in pharmacological sciences. 2009 Nov:30(11):570-80. doi: 10.1016/j.tips.2009.08.001. Epub 2009 Sep 14 [PubMed PMID: 19758712]
Level 3 (low-level) evidenceKim I, Ahn SH, Inagaki T, Choi M, Ito S, Guo GL, Kliewer SA, Gonzalez FJ. Differential regulation of bile acid homeostasis by the farnesoid X receptor in liver and intestine. Journal of lipid research. 2007 Dec:48(12):2664-72 [PubMed PMID: 17720959]
Level 3 (low-level) evidenceMakishima M, Okamoto AY, Repa JJ, Tu H, Learned RM, Luk A, Hull MV, Lustig KD, Mangelsdorf DJ, Shan B. Identification of a nuclear receptor for bile acids. Science (New York, N.Y.). 1999 May 21:284(5418):1362-5 [PubMed PMID: 10334992]
Level 3 (low-level) evidenceParks DJ, Blanchard SG, Bledsoe RK, Chandra G, Consler TG, Kliewer SA, Stimmel JB, Willson TM, Zavacki AM, Moore DD, Lehmann JM. Bile acids: natural ligands for an orphan nuclear receptor. Science (New York, N.Y.). 1999 May 21:284(5418):1365-8 [PubMed PMID: 10334993]
Level 3 (low-level) evidenceWang H, Chen J, Hollister K, Sowers LC, Forman BM. Endogenous bile acids are ligands for the nuclear receptor FXR/BAR. Molecular cell. 1999 May:3(5):543-53 [PubMed PMID: 10360171]
Level 3 (low-level) evidenceStange EF, Scheibner J, Ditschuneit H. Role of primary and secondary bile acids as feedback inhibitors of bile acid synthesis in the rat in vivo. The Journal of clinical investigation. 1989 Jul:84(1):173-80 [PubMed PMID: 2738150]
Level 3 (low-level) evidenceJiao Y, Lu Y, Li XY. Farnesoid X receptor: a master regulator of hepatic triglyceride and glucose homeostasis. Acta pharmacologica Sinica. 2015 Jan:36(1):44-50. doi: 10.1038/aps.2014.116. Epub 2014 Dec 15 [PubMed PMID: 25500875]
Baxter JD, Webb P. Metabolism: bile acids heat things up. Nature. 2006 Jan 26:439(7075):402-3 [PubMed PMID: 16437098]
Level 3 (low-level) evidenceNagahashi M, Takabe K, Liu R, Peng K, Wang X, Wang Y, Hait NC, Wang X, Allegood JC, Yamada A, Aoyagi T, Liang J, Pandak WM, Spiegel S, Hylemon PB, Zhou H. Conjugated bile acid-activated S1P receptor 2 is a key regulator of sphingosine kinase 2 and hepatic gene expression. Hepatology (Baltimore, Md.). 2015 Apr:61(4):1216-26. doi: 10.1002/hep.27592. Epub 2015 Mar 9 [PubMed PMID: 25363242]
Level 3 (low-level) evidenceWiemuth D, Sahin H, Falkenburger BH, Lefèvre CM, Wasmuth HE, Gründer S. BASIC--a bile acid-sensitive ion channel highly expressed in bile ducts. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2012 Oct:26(10):4122-30. doi: 10.1096/fj.12-207043. Epub 2012 Jun 26 [PubMed PMID: 22735174]
Level 3 (low-level) evidenceMagotti P, Bauer I, Igarashi M, Babagoli M, Marotta R, Piomelli D, Garau G. Structure of human N-acylphosphatidylethanolamine-hydrolyzing phospholipase D: regulation of fatty acid ethanolamide biosynthesis by bile acids. Structure (London, England : 1993). 2015 Mar 3:23(3):598-604. doi: 10.1016/j.str.2014.12.018. Epub 2015 Feb 12 [PubMed PMID: 25684574]
Bove KE, Heubi JE, Balistreri WF, Setchell KD. Bile acid synthetic defects and liver disease: a comprehensive review. Pediatric and developmental pathology : the official journal of the Society for Pediatric Pathology and the Paediatric Pathology Society. 2004 Jul-Aug:7(4):315-34 [PubMed PMID: 15383928]
Stieger B, Zhang J, O'Neill B, Sjövall J, Meier PJ. Differential interaction of bile acids from patients with inborn errors of bile acid synthesis with hepatocellular bile acid transporters. European journal of biochemistry. 1997 Feb 15:244(1):39-44 [PubMed PMID: 9063443]
Level 3 (low-level) evidenceFischler B, Bodin K, Stjernman H, Olin M, Hansson M, Sjövall J, Björkhem I. Cholestatic liver disease in adults may be due to an inherited defect in bile acid biosynthesis. Journal of internal medicine. 2007 Aug:262(2):254-62 [PubMed PMID: 17645593]
Level 3 (low-level) evidenceDavidson MH. A systematic review of bile acid sequestrant therapy in children with familial hypercholesterolemia. Journal of clinical lipidology. 2011 Mar-Apr:5(2):76-81. doi: 10.1016/j.jacl.2011.01.005. Epub 2011 Jan 31 [PubMed PMID: 21392720]
Level 1 (high-level) evidencePusl T, Beuers U. Intrahepatic cholestasis of pregnancy. Orphanet journal of rare diseases. 2007 May 29:2():26 [PubMed PMID: 17535422]
Poupon RE, Balkau B, Eschwège E, Poupon R. A multicenter, controlled trial of ursodiol for the treatment of primary biliary cirrhosis. UDCA-PBC Study Group. The New England journal of medicine. 1991 May 30:324(22):1548-54 [PubMed PMID: 1674105]
Level 1 (high-level) evidenceGlantz A, Marschall HU, Lammert F, Mattsson LA. Intrahepatic cholestasis of pregnancy: a randomized controlled trial comparing dexamethasone and ursodeoxycholic acid. Hepatology (Baltimore, Md.). 2005 Dec:42(6):1399-405 [PubMed PMID: 16317669]
Level 1 (high-level) evidencePost SM, Duez H, Gervois PP, Staels B, Kuipers F, Princen HM. Fibrates suppress bile acid synthesis via peroxisome proliferator-activated receptor-alpha-mediated downregulation of cholesterol 7alpha-hydroxylase and sterol 27-hydroxylase expression. Arteriosclerosis, thrombosis, and vascular biology. 2001 Nov:21(11):1840-5 [PubMed PMID: 11701475]
Level 3 (low-level) evidenceDanzinger RG, Hofmann AF, Schoenfield LJ, Thistle JL. Dissolution of cholesterol gallstones by chenodeoxycholic acid. The New England journal of medicine. 1972 Jan 6:286(1):1-8 [PubMed PMID: 5006919]
Thistle JL, Hofmann AF. Efficacy and specificity of chenodeoxycholic acid therapy for dissolving gallstones. The New England journal of medicine. 1973 Sep 27:289(13):655-9 [PubMed PMID: 4580472]
Level 1 (high-level) evidencePattni S, Walters JR. Recent advances in the understanding of bile acid malabsorption. British medical bulletin. 2009:92():79-93. doi: 10.1093/bmb/ldp032. Epub [PubMed PMID: 19900947]
Level 3 (low-level) evidenceDegirolamo C, Modica S, Palasciano G, Moschetta A. Bile acids and colon cancer: Solving the puzzle with nuclear receptors. Trends in molecular medicine. 2011 Oct:17(10):564-72. doi: 10.1016/j.molmed.2011.05.010. Epub 2011 Jul 2 [PubMed PMID: 21724466]
Level 3 (low-level) evidenceReddy BS, Hanson D, Mangat S, Mathews L, Sbaschnig M, Sharma C, Simi B. Effect of high-fat, high-beef diet and of mode of cooking of beef in the diet on fecal bacterial enzymes and fecal bile acids and neutral sterols. The Journal of nutrition. 1980 Sep:110(9):1880-7 [PubMed PMID: 7411244]
Level 3 (low-level) evidenceHill MJ. Bile flow and colon cancer. Mutation research. 1990 May:238(3):313-20 [PubMed PMID: 2188127]
Level 3 (low-level) evidenceCheah PY. Hypotheses for the etiology of colorectal cancer--an overview. Nutrition and cancer. 1990:14(1):5-13 [PubMed PMID: 2195469]
Level 3 (low-level) evidenceBernstein H, Bernstein C, Payne CM, Dvorak K. Bile acids as endogenous etiologic agents in gastrointestinal cancer. World journal of gastroenterology. 2009 Jul 21:15(27):3329-40 [PubMed PMID: 19610133]
Level 3 (low-level) evidenceAscher B, Hoffmann K, Walker P, Lippert S, Wollina U, Havlickova B. Efficacy, patient-reported outcomes and safety profile of ATX-101 (deoxycholic acid), an injectable drug for the reduction of unwanted submental fat: results from a phase III, randomized, placebo-controlled study. Journal of the European Academy of Dermatology and Venereology : JEADV. 2014 Dec:28(12):1707-15. doi: 10.1111/jdv.12377. Epub 2014 Mar 8 [PubMed PMID: 24605812]
Level 1 (high-level) evidenceWollina U, Goldman A. ATX-101 for reduction of submental fat. Expert opinion on pharmacotherapy. 2015 Apr:16(5):755-62. doi: 10.1517/14656566.2015.1019465. Epub 2015 Feb 27 [PubMed PMID: 25724831]
Level 3 (low-level) evidence