Introduction
Best disease (Best vitelliform macular dystrophy, BVMD) is a rare autosomal dominant disorder due to the mutation of BEST1 (or VMD2, TU15B, OMIM #607854) gene with incomplete penetrance and variable expression which typically presents in childhood. However, there are also reports of autosomal recessive BVMD.[1][2][3]
Its characteristic presentation is by bilateral fundus changes of egg-yolk appearance (as in a fried egg with sunny side up) at the macula in both eyes. Retinal pigment epithelium (RPE) is primarily affected. The electrooculogram (EOG) is typically affected, with reduced Arden ratio both in carriers and patients. The visual prognosis of the disease is usually good, usually maintaining driving/reading capability in at least one eye throughout life.
Other names of the condition include Best macular dystrophy, Best disease, vitelliform dystrophy, early or juvenile-onset vitelliform macular dystrophy, vitelline dystrophy, and vitelliruptive degeneration. The disease gets its name from a German ophthalmologist Dr. Friedrich Best who described a pedigree suffering from various stages of the disease in 1905.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The cause of the disease is a mutation in the VMD2 or BEST1 gene at chromosome 11q12-q13.[5][6] The product of this gene is a transmembrane protein called Bestrophin 1, located predominantly at the basolateral membrane of the RPE.[7] Bestrophin 1 acts as both a regulator of intracellular Ca++ signaling and a pentameric anion channel.[7] Bestrophin 1 functions as a calcium-activated chloride channel and also may work as a channel for other anions, including bicarbonate.[7] Also, it plays a significant role in the calcium homeostasis of the RPE.[7] In effect, bestrophin plays a crucial part in the regulation of the ionic environment of the RPE and/or subretinal space. The ionic balance of the RPE is an important factor for adhesion between the retina and the RPE. Also, the mutation causes reduced Arden ratio in EOG in Best vitelliform macular dystrophy both in the carrier and the affected individuals.
Approximately 5% of individuals with BEST1 mutation will have normal or near-normal macular findings.[8]
The mutation BEST1 causes multiple diseases, including:
- Vitelliform macular dystrophy 2 or BVMD (Phenotype MIM No. 153700)
- Autosomal recessive bestrophinopathy (Phenotype MIM No. 611809)
- Retinitis pigmentosa 50 (RP50)/concentric retinitis pigmentosa (Phenotype MIM No. 613194)
- Autosomal dominant microcornea, rod-cone dystrophy, cataract, and posterior staphyloma 193220 (Phenotype MIM No. 193220)
- Autosomal dominant vitreoretinochoroidopathy (Phenotype MIM No. 193220)
- Adult-onset vitelliform macular dystrophy[7]
Epidemiology
The prevalence of Best vitelliform macular dystrophy was noted to be between 1 in 16,500 to 1 in 21,000 in a study conducted at Olmsted County, Minnesota.[9] Both males and females are affected. The usual age at presentation is within the first two decades, and detection is usually incidental. The macular lesion may be noted for the first time as late as at 75 years of age.[8]
Pathophysiology
There is deposition of yellow material within the retinal pigment epithelium (RPE), the subretinal space, and the photoreceptor zone.[10] A break/disturbance in the RPE/Bruch's membrane[11] results in a late complication of a choroidal neovascular membrane (CNVM).
Histopathology
Only a few reports have investigated the histopathological features of Best vitelliform macular dystrophy.
Histopathology of a 69-year-old male with BVMD showed[12]:
- Accumulation of lipofuscin within the RPE, particularly at the fovea. Lipofuscin was confirmed by staining, ultrastructural appearance, and autofluorescence properties.
- Other features included:
- Accumulation of heterogeneous material between RPE and Bruch's membrane, which likely derived from degenerating RPE cells containing lipofuscin
- Loss of foveal photoreceptors above the lesion
- Photoreceptor outer segment debris and phagocytic cells in the subretinal space
Histology of another eye showed 'well-circumscribed area of RPE hyperplasia, accumulation of lipofuscin in the RPE, deposition of granular material in the photoreceptors, macrophages, and drusen.'[13]
Mullin and colleagues reported a male who was noted to have small macular vitelliform lesions and extramacular subretinal flecks in both eyes for the first time at 75 years of age.[8] On histopathology at 93 years, the eye showed attenuated outer nuclear layer (ONL) usually associated with normal RPE, degeneration of photoreceptors with loss of RPE at the central macula, and drusen and basal laminar deposits at the peripheral flecks. Bestrophin was noted to be present at the basolateral and apical membrane of RPE.
Histopathological evaluation of a 28-year-old male with vitelliruptive stage 'with some features of a pseudohypopyon' revealed diffuse RPE abnormality with an accumulation of lipofuscin. Lipopigment was noted 'within the RPE, within macrophages in the subretinal space, and within the choroid.'[14]
Frangieh and colleagues suggested that the changes in the neurosensory retina were primary, and RPE changes were secondary.[15] The choriocapillaris was normal, and they noted abnormal fibrillar material underneath RPE cells at the area of photoreceptor loss. Disruption in Bruch's membrane with CNVM was also noted. They found lipofuscin and melanolipofuscin deposit in RPE, and 'PAS-positive, acid-mucopolysaccharide-negative, electron-dense, finely granular material was deposited in the inner segments of the degenerating photoreceptors and the Mueller cells.'[15] This material corresponds mainly to A2E.[16]
Also, the brilliant autofluorescence of the vitelliform lesion might suggest the deposited material to be A2E or lipofuscin. However, angiographic evidence of generalized deposition of lipofuscin in RPE causing block fluorescence (dark choroid in fluorescein angiogram as seen in Stargardt disease) is not a feature in BVMD.
History and Physical
The lesions are usually detected incidentally, but symptoms may include dimness of vision, metamorphopsia or scotoma.
Evaluation
The disease usually involves the eye only with no systemic manifestations.
Refractive error (usually hypermetropia) may be present. The fundus appearance is drastic and shows a single egg-yolk like symmetrical subretinal deposit at the macula bilaterally, but the visual acuity is usually normal. However, there are reports of unilateral cases in patients with BEST1 mutation and bilateral reduced EOG Arden ratio with normal electroretinogram.[17] Best vitelliform macular dystrophy with affected EOG may have multifocal vitelliform lesions.[18]
Typically, the optic nerve and retinal vessels are normal, and bony spicules are not seen.
The vitelliform macular lesion may progress through the typical stages, may regress with time, or may be associated with newer extramacular lesions.
Visual field - Usually, there is no peripheral visual field defect. Central scotoma may be present.
Autofluorescence - The vitelliform material is typically brilliantly autofluorescent and has a round or oval shape in the vitelliform stage. In pseudohypopyon stage, the autofluorescence is visible in the inferiorly deposited yellow material. Vitelliruptive disease shows speckled autofluorescence. The atrophic stage shows hypo-autofluorescence. Peripheral ring/small circumferential dots of hyper-autofluorescence may be noted in the vitelliruptive stage.[19] Late stages characteristically show central hypo autofluorescence and peripheral hyper-autofluorescence.[20] Retinal dysfunction and autofluorescence revealed a centrifugal pattern of loss from center to periphery in a study.[20] The central area of atrophy correlates with low visual acuity, reduced autofluorescence, central scotoma, reduced color vision, and reduced pattern ERG (PERG) response.[20]
Fundus fluorescein angiogram (FFA)- FFA is crucial to rule out choroidal neovascular membrane (CNVM), which shows fluorescence that increases in size and intensity with time. The vitelliform deposit usually causes hypofluorescence secondary to blocked fluorescence. The atrophic stage reveals a window defect. There is no 'black choroid' appearance on FFA, as seen in Stargardt disease.
Optical coherence tomography (OCT) - In the vitelliform stage, the OCT reveals the deposit of homogenous hyperreflective material.[21] In the pseudohypopyon stage, the vertical OCT scan shows clear fluid superiorly and a sharp margin of the deposited vitelliform material. In the atrophic phase, retinal thinning may be noted similar to geographic atrophy in age-related macular degeneration. Subretinal/intraretinal fluid, and/or subretinal hemorrhage may characterize the CNVM stage. The location of vitelliform material has undergone study with both time-domain and spectral-domain OCT.
In the subclinical stage, the middle highly reflective layer or middle HRL (interdigitation zone or IZ/cone outer segment tip line or COST) showed notable thickening throughout the macula, especially at the fovea.[22] The location of this middle HRL is between inner HRL (inner-segment outer segment junction/ellipsoid zone or EZ) and the outer HRL (RPE-Bruch's membrane complex). There was thinning of ONL. In the vitelliform stage, the hyper-reflective vitelliform material exists between middle HRL and outer HRL. The middle HRL showed thickening at areas of the macula not involved with a vitelliform deposit, and there was thinning of ONL. Pseudohypopyon characteristically shows as optically clear space between the neurosensory retina and outer HRL, some disruptions in the inner HRL, lengthening of the outer segment of photoreceptors, small hyperreflective mounds over the outer HRL, and thinning of ONL. The OCT in vitelliruptive stage showed disruption in both inner and middle HRL, shortening of outer segments, and hyperreflective deposits over the outer HRL.[22] OCT may show fibrotic pillars.
In another study, the outer retinal layers were noted to be disrupted in stage 2 through 4 disease (vitelliform, pseudohypopyon, and vitelliruptive stage), and absent outer retinal layers were noted in the atrophic or cicatricial stage.[23] Poor visual acuity is associated with subretinal fluid and disruptions of EZ.[21][23]
EOG - The normal light peak to dark trough ratio (Arden ratio) is at least 1.85. In BVMD (all stages, even with no apparent fundus lesion, all patients, and carriers with normal fundus), the light peak is universally reduced, resulting in an Arden ratio of 1.50 or less usually.
The diagnosis of BVMD needs the following criteria
- Presence of one of the typical lesions of BVMD
- Abnormal EOG
- Dominant mode of inheritance
- Typical natural course and onset of the disease as in BVMD
ERG - Typically, the ERG is normal.
Dark adaptometry is normal.
Color vision and contrast sensitivity may be affected.
Treatment / Management
Best vitelliform macular dystrophy without a choroidal neovascular membrane (CNVM) needs no treatment. Dilated fundus evaluation of family members, electrophysiological testing (EOG, ERG), and genetic analysis are essential in establishing the diagnosis. Regular follow-up is vital for the early detection of complications, especially CNVM.
The CNVM may respond favorably with anti-vascular endothelial growth factor agents (anti-VEGF agents like bevacizumab, ranibizumab, or aflibercept).[24] Other options include laser and photodynamic therapy.[25] The CNVM may regress spontaneously also, but the visual outcome may be better with anti-VEGF agents.[24] On average, one bevacizumab injection was necessary for BVMD with CNVM in the study by Khan and colleagues.[24](B3)
All patients should receive good refraction.
In patients with significant cataracts, cataract surgery may lead to visual improvement.
Amsler grid is an important tool for home monitoring and may detect metamorphopsia early.
Low vision aids, including magnifiers and telescopes, may help to rehabilitate patients with atrophic disease with poor vision.
Differential Diagnosis
The differential diagnoses include:
- Central serous chorioretinopathy with fibrin
- There is the presence of serous pigment epithelial detachment and area of subretinal lucency at the location of the leak[26]
- FFA features are typical and show leaks (ink-blot, smoke-stack or diffuse) and pigment epithelial detachment
- Adult-onset vitelliform macular dystrophy (a variant of pattern dystrophy)
- The patients present at late-middle or old age with visual decline
- The lesion is smaller and may not pass through the typical stages of BVMD
- There may be a mutation of the BEST1 or PRPH2 (RDS) gene. Up to one-third of patients have abnormal EOG and the disease is dominantly inherited
- Subretinal granuloma due to choroidal tuberculosis/sarcoidosis
- There is clinical or angiographic evidence of inflammation
- Wet age-related macular degeneration
- Distinguishing features are old age and irregular lesion
- Disciform scar has a whitish appearance rather than the typical yellow, smooth appearance of BVMD
- Acute exudative vitelliform maculopathy
- Fundus flavimaculatus with large flecks
- Large dehemoglobinized subretinal hemorrhage
- Basal laminar drusen
Staging
The disease usually goes through several stages:
- Previtelliform/subclinical stage - The fundus is normal in an asymptomatic infant or child. However, EOG is abnormal.
- Vitelliform stage or egg yolk stage - Best vitelliform macular dystrophy gets its name from this stage, and this stage typically presents in infancy or early childhood. An egg-yolk like round or oval yellow smooth elevated lesion with a well-defined margin is seen at the macula. The size is 0.5 to 2 disc diameters, and the lesion usually centers on the fovea but not in every case. The size/site/shape/stage of the lesion may not be very symmetrical. Vision is usually normal or minimally affected despite the drastic fundus appearance. The lesion(s) may be multiple and extramacular and be very large with a geographic shape.
- Pseudohypopyon stage - The vitelliform deposits gravitate down in the subretinal space with a horizontal upper level, usually at puberty. The fluid above this deposit is clear. One hypothesis is that the retinal pigment epithelium takes up the yellow deposit, and heavier material gravitates down. Vision is usually good at this stage. After a change of head position for 60 to 90 minutes, the pseudohypopyon may shift.
- Vitelliruptive stage or scrambled egg stage is due to the breakup of the smooth and uniform vitelliform material giving a nonhomogenous look. Visual acuity starts to deteriorate at this stage. A small area or areas of pigmentation/atrophy may be noted.
- Atrophic stage- The vitelliform material is no longer visible, and there is an area of atrophy and pigmentation which may simulate geographic atrophy due to age-related macular degeneration. Marked visual deterioration is present. This stage usually occurs after 40 years of age.
- Cicatricial and choroidal neovascularization - Subretinal bleed may be present due to CNVM. This stage is associated with poor vision and may lead to subretinal fibrosis.
Prognosis
The visual prognosis is usually good. Best-corrected visual acuity is:
- 20/20 in the pre-vitelliform stage
- 20/20-20/60 in the vitelliform or pseudohypopyon stage
- 20-20-20/120- in the vitelliruptive stage
- The visual acuity may be worse than 20/200 in the atrophic or cicatricial/CNVM stage
In a large series,[27] 77% of the eyes with Best vitelliform macular dystrophy had at least 20/40. In 8-10 years, 19% of the eyes with atrophic stage or fibrous scar lost at least two lines.
Complications
The complications of the disease include
- Choroidal neovascular membrane leading to disciform scar
- Subretinal fibrosis
- Macular hole (rare)
Consultations
- Specialist in vitreoretinal conditions for evaluation, management, and follow up, specifically to detect choroidal neovascular membrane early
- Consultant visual electrophysiology for EOG & ERG
- Consultant genetics for genetic evaluation
- Low vision aid specialist for visual rehabilitation
- Occupational counseling, given the possibility of visual deterioration with age
- Marriage counseling and genetic analysis of the partner
Deterrence and Patient Education
The patients should receive education about the risk of late complications and the need for regular follow up. Amsler chart should be used regularly to detect metamorphopsia early, which may be related to the formation of a choroidal neovascular membrane.
Enhancing Healthcare Team Outcomes
The exact primary histopathological location and nature of the vitelliform material needs further evaluation. A retina specialist is best equipped to manage this disease. Interprofessional coordination with various specialties including ophthalmology and genetics is important in the prognostication, management, and follow up of the disease. Specialty trained nurses in ophthalmology and genetics can improve outcomes by coordination communication between the interprofessional team and by assisting with patient coordination and family education. Pharmacists should review drug treatments, check for drug-drug interactions, and assess compliance. Concerns should be reported to the team. Due to its rarity, this is a difficult disease to evaluate and manage. Outcomes will be improved if an interprofessional team manages the care of these patients. [Level 5]
Media
(Click Image to Enlarge)
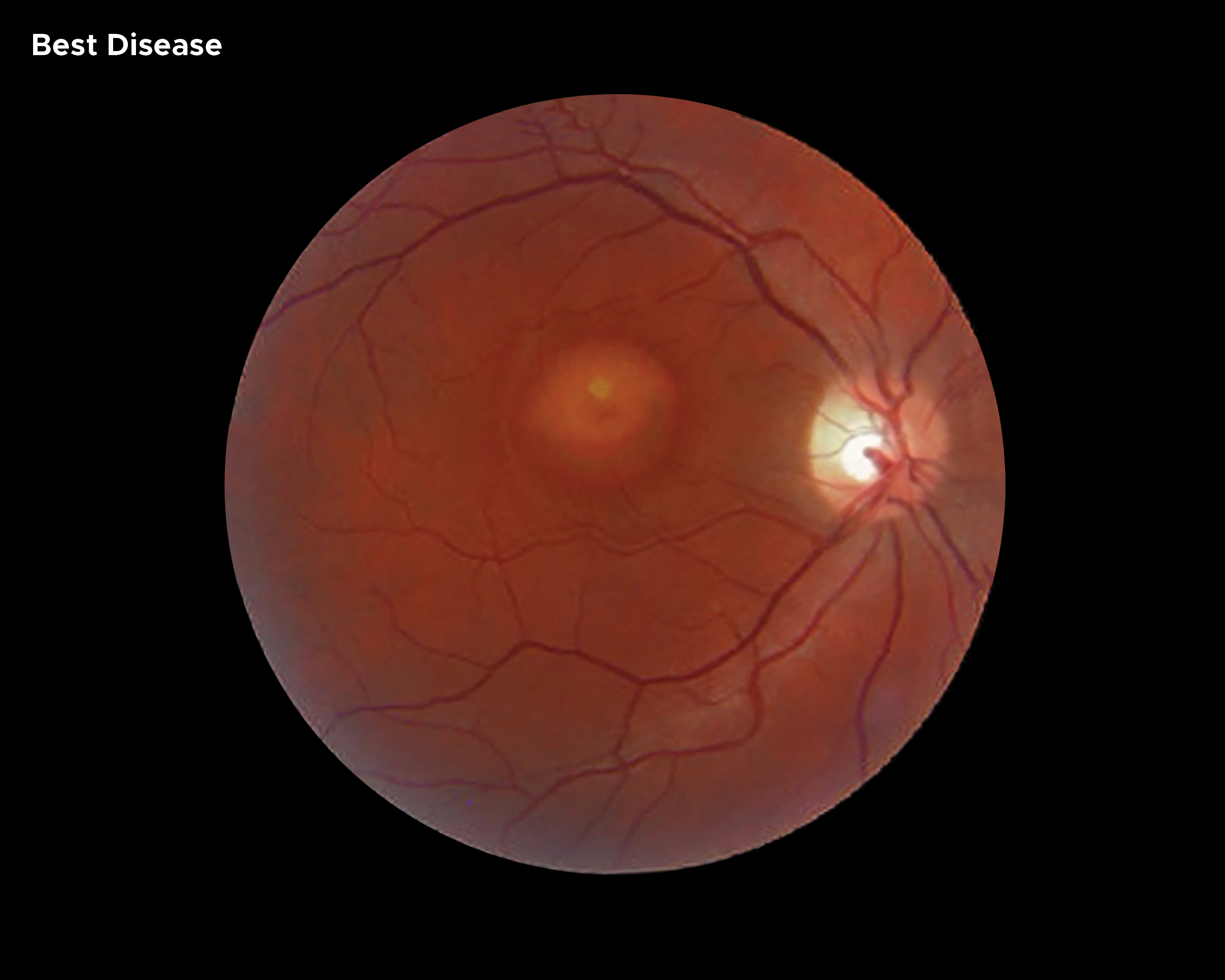
Image of eye with Best Disease Contributed by Chelsea Rowe
References
Zhao L,Grob S,Corey R,Krupa M,Luo J,Du H,Lee C,Hughes G,Lee J,Quach J,Zhu J,Shaw PX,Kozak I,Zhang K, A novel compound heterozygous mutation in the BEST1 gene causes autosomal recessive Best vitelliform macular dystrophy. Eye (London, England). 2012 Jun; [PubMed PMID: 22422030]
Level 3 (low-level) evidenceBitner H,Mizrahi-Meissonnier L,Griefner G,Erdinest I,Sharon D,Banin E, A homozygous frameshift mutation in BEST1 causes the classical form of Best disease in an autosomal recessive mode. Investigative ophthalmology [PubMed PMID: 21467170]
Iannaccone A,Kerr NC,Kinnick TR,Calzada JI,Stone EM, Autosomal recessive best vitelliform macular dystrophy: report of a family and management of early-onset neovascular complications. Archives of ophthalmology (Chicago, Ill. : 1960). 2011 Feb; [PubMed PMID: 21320969]
Level 3 (low-level) evidenceQuerques G,Zerbib J,Santacroce R,Margaglione M,Delphin N,Rozet JM,Kaplan J,Martinelli D,Delle Noci N,Soubrane G,Souied EH, Functional and clinical data of Best vitelliform macular dystrophy patients with mutations in the BEST1 gene. Molecular vision. 2009 Dec 31; [PubMed PMID: 20057903]
Stone EM,Nichols BE,Streb LM,Kimura AE,Sheffield VC, Genetic linkage of vitelliform macular degeneration (Best's disease) to chromosome 11q13. Nature genetics. 1992 Jul; [PubMed PMID: 1302019]
Level 3 (low-level) evidenceLin Y,Li T,Ma C,Gao H,Chen C,Zhu Y,Liu B,Lian Y,Huang Y,Li H,Wu Q,Liang X,Jin C,Huang X,Ye J,Lu L, Genetic variations in Bestrophin‑1 and associated clinical findings in two Chinese patients with juvenile‑onset and adult‑onset best vitelliform macular dystrophy. Molecular medicine reports. 2018 Jan; [PubMed PMID: 29115605]
Johnson AA, Guziewicz KE, Lee CJ, Kalathur RC, Pulido JS, Marmorstein LY, Marmorstein AD. Bestrophin 1 and retinal disease. Progress in retinal and eye research. 2017 May:58():45-69. doi: 10.1016/j.preteyeres.2017.01.006. Epub 2017 Jan 30 [PubMed PMID: 28153808]
Mullins RF,Oh KT,Heffron E,Hageman GS,Stone EM, Late development of vitelliform lesions and flecks in a patient with best disease: clinicopathologic correlation. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 Nov; [PubMed PMID: 16286623]
Level 3 (low-level) evidenceDalvin LA,Pulido JS,Marmorstein AD, Vitelliform dystrophies: Prevalence in Olmsted County, Minnesota, United States. Ophthalmic genetics. 2017 Mar-Apr; [PubMed PMID: 27120116]
Spaide RF,Noble K,Morgan A,Freund KB, Vitelliform macular dystrophy. Ophthalmology. 2006 Aug; [PubMed PMID: 16877078]
Level 2 (mid-level) evidenceTripathy K. Choroidal neovascular membrane in intraocular tuberculosis. GMS ophthalmology cases. 2017:7():Doc24. doi: 10.3205/oc000075. Epub 2017 Sep 1 [PubMed PMID: 28944155]
Level 3 (low-level) evidenceO'Gorman S,Flaherty WA,Fishman GA,Berson EL, Histopathologic findings in Best's vitelliform macular dystrophy. Archives of ophthalmology (Chicago, Ill. : 1960). 1988 Sep; [PubMed PMID: 3415551]
Level 3 (low-level) evidenceZhang Q,Small KW,Grossniklaus HE, Clinicopathologic findings in Best vitelliform macular dystrophy. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2011 May; [PubMed PMID: 21136072]
Level 3 (low-level) evidenceWeingeist TA, Kobrin JL, Watzke RC. Histopathology of Best's macular dystrophy. Archives of ophthalmology (Chicago, Ill. : 1960). 1982 Jul:100(7):1108-14 [PubMed PMID: 7092654]
Level 3 (low-level) evidenceFrangieh GT,Green WR,Fine SL, A histopathologic study of Best's macular dystrophy. Archives of ophthalmology (Chicago, Ill. : 1960). 1982 Jul; [PubMed PMID: 7092655]
Level 3 (low-level) evidenceBakall B,Radu RA,Stanton JB,Burke JM,McKay BS,Wadelius C,Mullins RF,Stone EM,Travis GH,Marmorstein AD, Enhanced accumulation of A2E in individuals homozygous or heterozygous for mutations in BEST1 (VMD2). Experimental eye research. 2007 Jul; [PubMed PMID: 17477921]
Arora R,Khan K,Kasilian ML,Strauss RW,Holder GE,Robson AG,Thompson DA,Moore AT,Michaelides M, Unilateral BEST1-Associated Retinopathy. American journal of ophthalmology. 2016 Sep; [PubMed PMID: 27287821]
Pece A,Gaspari G,Avanza P,Magni R,Brancato R, Best's multiple vitelliform degeneration. International ophthalmology. 1992 Nov; [PubMed PMID: 1490837]
Level 3 (low-level) evidenceDuncker T,Greenberg JP,Ramachandran R,Hood DC,Smith RT,Hirose T,Woods RL,Tsang SH,Delori FC,Sparrow JR, Quantitative fundus autofluorescence and optical coherence tomography in best vitelliform macular dystrophy. Investigative ophthalmology [PubMed PMID: 24526438]
Jarc-Vidmar M,Kraut A,Hawlina M, Fundus autofluorescence imaging in Best's vitelliform dystrophy. Klinische Monatsblatter fur Augenheilkunde. 2003 Dec; [PubMed PMID: 14704944]
Level 3 (low-level) evidenceTripathy K,Chawla R,Mittal K,Temkar S, Egg yolk in the eye: an ultrawide field evaluation. BMJ case reports. 2016 Jan 27 [PubMed PMID: 26818692]
Level 3 (low-level) evidenceFerrara DC, Costa RA, Tsang S, Calucci D, Jorge R, Freund KB. Multimodal fundus imaging in Best vitelliform macular dystrophy. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2010 Oct:248(10):1377-86. doi: 10.1007/s00417-010-1381-2. Epub 2010 Apr 23 [PubMed PMID: 20414784]
Battaglia Parodi M,Iacono P,Romano F,Bandello F, SPECTRAL DOMAIN OPTICAL COHERENCE TOMOGRAPHY FEATURES IN DIFFERENT STAGES OF BEST VITELLIFORM MACULAR DYSTROPHY. Retina (Philadelphia, Pa.). 2018 May; [PubMed PMID: 28376040]
Khan KN,Mahroo OA,Islam F,Webster AR,Moore AT,Michaelides M, FUNCTIONAL AND ANATOMICAL OUTCOMES OF CHOROIDAL NEOVASCULARIZATION COMPLICATING BEST1-RELATED RETINOPATHY. Retina (Philadelphia, Pa.). 2017 Jul; [PubMed PMID: 27764019]
Sodi A,Murro V,Caporossi O,Passerini I,Bacci GM,Caputo R,Menchini U, Long-Term Results of Photodynamic Therapy for Choroidal Neovascularization in Pediatric Patients with Best Vitelliform Macular Dystrophy. Ophthalmic genetics. 2015 Jun; [PubMed PMID: 25675349]
Level 3 (low-level) evidenceYannuzzi NA,Mrejen S,Capuano V,Bhavsar KV,Querques G,Freund KB, A Central Hyporeflective Subretinal Lucency Correlates With a Region of Focal Leakage on Fluorescein Angiography in Eyes With Central Serous Chorioretinopathy. Ophthalmic surgery, lasers [PubMed PMID: 26431298]
Mohler CW,Fine SL, Long-term evaluation of patients with Best's vitelliform dystrophy. Ophthalmology. 1981 Jul; [PubMed PMID: 7267039]