Introduction
Basophilia refers to an increased number of basophils, a type of leukocyte, in the blood.[1] Basophils are typically the least numerous myeloid cells in a peripheral blood smear (see Image. Monocyte, Neutrophil, and Basophil). These cells' numerous dark azurophilic granules easily distinguish them from other white blood cells.[2] Basophilia is not a frequent finding in peripheral blood. This condition most commonly manifests as a reactive mechanism associated with eosinophilia and an absolute basophil count exceeding 200 cells/µL. Different ranges are set depending on the laboratory and the local population.
If performed, bone marrow aspirates may show an increase in basophils or precursors. Basophils express cluster of differentiation (CD) 45 and are positive for CD13, CD11b, and CD33 myeloid markers. These leukocytes also express CD22 (also positive in B-cells), bright CD38, and bright CD123.[3] CD203c is a distinct marker specific to basophils, frequently utilized to distinguish basophils from other white blood cells, such as mast cells, eosinophils, and neutrophils.[4]
Basophils originate from a cell type similar to a myeloblast. The earliest identifiable stage is a basophil myelocyte, which exhibits the characteristic basophil granules. These granules, measuring approximately 0.2 to 1 μm in diameter, are larger than the azurophilic granules found in promyelocytes and are often irregular. As the cell develops, the granules become more metachromatic (red-purple) due to an increasing content of acid mucopolysaccharides, particularly heparin. During maturation, the cytoplasmic ribonucleic acid (RNA) decreases, and the nucleus partially segments. Stages analogous to those observed in neutrophils are not easily distinguishable due to incomplete nuclear segmentation.[5] The nucleus of mature basophils condenses but smudges chromatin, and the background cytoplasm lacks basophilia, which marks residual RNA.[6]
Basophils have a lifespan comparable to eosinophils. The maturation process in the bone marrow takes approximately 7 days. Basophils circulate in the bloodstream and are not typically found in tissues. Several cytokines influence basophil production, including granulocyte-macrophage colony-stimulating factor, interleukin (IL)-3, and IL-5. However, IL-3 is the primary growth factor for basophil development and proliferation.[7]
Basophil granules comprise several key components, including histamine, heparin, and peroxidase. Basophils can synthesize and store histamine and eosinophil chemotactic factors of anaphylaxis (ECF-A). These leukocytes also synthesize and release slow-reacting substances of anaphylaxis (SRS-A) and, likely, platelet-activating factor (PAF) upon stimulation but do not store these substances. Notably, as demonstrated by cytochemical analysis, basophils lack significant amounts of certain hydrolytic enzymes, such as alkaline and acid phosphatases.[8]
Basophils (as well as mast cells) appear to be involved in immediate hypersensitivity reactions, such as allergic asthma. Immunoglobulin E (IgE) binds readily to basophil and mast cell membranes. Degranulation occurs when a specific antigen reacts with the membrane-bound IgE and releases mediators of immediate hypersensitivity (eg, histamine, SRS-A, PAF, heparin, ECF-A).[9] Basophils are also involved in some delayed hypersensitivity reactions or cutaneous basophil hypersensitivity, such as contact allergies, where they appear to undergo a different degranulation response.[10]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Basophil count elevation may represent an underlying neoplasm such as chronic myeloid leukemia (CML), polycythemia vera, primary myelofibrosis, essential thrombocythemia, acute myeloid leukemia (AML), and, rarely, solid tumors. Common causes include allergic reactions or chronic inflammation related to infections (including influenza and tuberculosis), inflammatory bowel disease, and autoimmune disease. Drug-related causes and food ingestion also correlate with symptoms and degree of basophilia.
Epidemiology
Basophilia is a condition without a gender predilection. Basophilia's frequency often depends on the etiology.
Histopathology
A peripheral blood review is often required to interpret the cause of basophilia. The most striking basophil feature is the markedly intense azurophilic granules with dark blue segmented nuclei.[11] Basophilia is usually a nonspecific finding under microscopic examination. Thus, other findings may suggest the need for additional workup. For example, basophilia in the left-shifted neutrophilia setting should raise concerns about myeloproliferative neoplasm, especially CML.[12] The presence of basophilia with circulating blasts suggests the possibility of AML.[13] Review under oil immersion is usually required to avoid misclassifying degranulated basophils, which may resemble hypogranular neutrophils.[14]
History and Physical
The clinical presentation of basophilia is diverse and related to the underlying cause. A myeloproliferative syndrome may be suspected if splenomegaly is evident. Constitutional symptoms such as fever, malaise, itching, and fatigue may be present. Patients may report right upper quadrant pain. Erythromelalgia, or burning of the palms and soles, is common in polycythemia vera, and pruritus after a warm shower may also be a symptom. However, patients with basophilia may manifest with far more severe symptomatology, such as thrombosis; skin rashes may be elicited in cases of underlying allergic or hypersensitivity reactions.
Spleen examination requires the patient to be in the supine position with a relaxed abdomen. The examiner then inserts 3 fingers into Traube space underneath the left side of the rib cage during inspiration. Another sensitive technique is ultrasound examination, which can lead to the same results. Hypereosinophilic syndrome may be considered if concurrent eosinophilia is greater than 1500 cells/uL.[15] Symptomatology and other systemic manifestations are related to skin or pulmonary involvement.
Evaluation
Modern automated hematology analyzers typically provide a comprehensive 5-part differential count, which includes neutrophils, monocytes, eosinophils, basophils, and lymphocytes. Basophil counts are usually the least accurate and tend to underestimate the number of cells. However, this inaccuracy is generally not clinically significant due to basophils' low concentration in peripheral blood.[16] Automated hematology analyzers combine the Coulter principle and flow cytometry to assess cellular granularity, diameter, and internal complexity.[17]
White blood cell differential parameters must be defined to flag specimens requiring manual technologist or pathologist review. These flags may be user-defined or instrument-defined. Manufacturer-defined thresholds for these flags should be validated in the individual laboratory, considering the patient population being tested. The flag criteria should minimize unnecessary manual review of blood smears while still catching clinically significant abnormalities. The suspect flags indicate the presence of cells that cannot be accurately subclassified by the automated instrument, often due to unexpected light scatter and volume characteristics. Such flags generally require manual review. A blood smear manual review is essential to identify abnormal or immature cell types that automated methods may miss.[18]
Current hematology analyzers have a high degree of precision for cell counting and cell sizing. These analyzers need to be calibrated at regular intervals according to guidelines and quality control procedures to ensure their operation. The quality control of hematology analyzers encompasses internal quality control using stable hematology control material and participating in external quality assurance programs. Automated hematology and coagulation test systems require 2 levels of control every 8 hours of testing, and each time, a change in reagent occurs.[19]
If the results of controls and calibration materials do not meet the laboratory's established acceptability criteria, all patient test results from the unacceptable test run or since the last acceptable test run must be reviewed to determine if they have been impacted. The laboratory must take necessary remedial actions to ensure the accuracy and reliability of patient test results.[20]
According to the Clinical and Laboratory Standards Institute H20-A2 standard, the reference method for determining the basophil count is the microscopic examination of a blood smear with a manual differential count of 400 leukocytes. This manual microscopic method serves as the reference against which automated hematology analyzers are evaluated for their accuracy in determining the basophil count.[21] Cytogenetic testing is indicated to rule out CML when left-shifted neutrophilia with basophilia is detected and cannot be explained.[22] Fluorescence in situ hybridization for BCR-ABL1 fusion may be performed on peripheral blood and, if positive, supports the diagnosis of CML.[23]
The other major myeloproliferative neoplasms, polycythemia vera, primary myelofibrosis (PMF), and essential thrombocythemia, often harbor specific mutations. Janus kinase 2, an acquired genetic mutation, is found in most patients with polycythemia vera. Over 50% of patients have PMF and essential thrombocythemia. A minority of patients with essential thrombocythemia or PMF have mutations in either CALR or MPL. The finding of one of these mutations is not specific to a myeloproliferative neoplasm and must be correlated with morphology and clinical findings.[24]
Cytogenetic analysis is required when a bone marrow biopsy is performed for a suspected myeloid neoplasm. This analysis involves karyotyping or genetic screening of the chromosomes in each white blood cell tested. Significant abnormalities in a conventional karyotype support the diagnosis of a neoplastic process. Fluorescence in situ hybridization may be performed concurrently to expedite the identification of BCR-ABL fusion in suspected CML cases.[25][26] Each leukocyte component is reported as a percentage of total WBCs and an absolute number per microliter (μL). Reference white blood cell intervals may vary depending on the laboratory. Sources of variation include characteristics of different patient populations, age, sex, and testing methodology.[27]
Treatment / Management
The underlying condition determines the appropriate intervention. Treating the underlying cause is critical in cases associated with allergies or chronic inflammation. Allergic reaction management strategies include discontinuing the offending agent and administering antihistamines. Parasitic infections should be addressed with concomitant pharmacologic therapy such as albendazole. Discussion of therapy specific to an underlying neoplasia is beyond the scope of this topic.
Differential Diagnosis
Toxic neutrophils may have azurophilic granules and are rarely mistaken for basophils. However, neutrophil granules are much smaller and often accompanied by Dohle bodies, which are not seen in basophils.[28]
Prognosis
Basophilia has a good prognosis, depending on the etiology. Infection-related basophilia is treated with antibiotics to address the underlying cause, whereas neoplasm-related basophilia may have a more complicated clinical course. CML management includes chemotherapeutic drugs such as imatinib and other modalities, whereas polycythemia vera and essential thrombocythemia require aspirin therapy and intermittent phlebotomy. Overall survival for these patients depends on the degree of care, persistence of patient follow-up, and methods used to prevent thrombotic complications.[29]
Complications
Complications associated with basophilia are primarily related to the underlying condition rather than the increase in basophils themselves. Basophils can degranulate in tissue, potentially causing local damage, so early intervention is crucial to prevent such damage. Additionally, complications related to basophilia in conditions like CML, polycythemia vera, and essential thrombocythemia include arterial and venous thrombosis. Patients should undergo adequate screening and receive preventative measures to address these risks.
Pearls and Other Issues
Key facts to remember about basophilia are as follows:
- Any patient with chronic anemia with a rise in basophils for longer than 6 months should be worked up for an underlying cause.
- Patients with basophilia should be worked up for CML or AML when no systemic infection or possible drug-related cause fits.
- Always rule out drug ingestion and parasitic infection.
- Look for clues to underlying neoplasia (left-shifted neutrophilia or circulating blasts) on a peripheral blood smear.
Enhancing Healthcare Team Outcomes
The pathologist should contact the clinical team when neoplasia is suspected in basophilia. Recommendations should be communicated and reflect the peripheral smear findings. For example, if unexplained basophilia with left-shifted neutrophilia is present, the pathologist may recommend that the clinician order BCR-ABL1 fluorescence in situ hybridization to rule out CML.
Media
(Click Image to Enlarge)
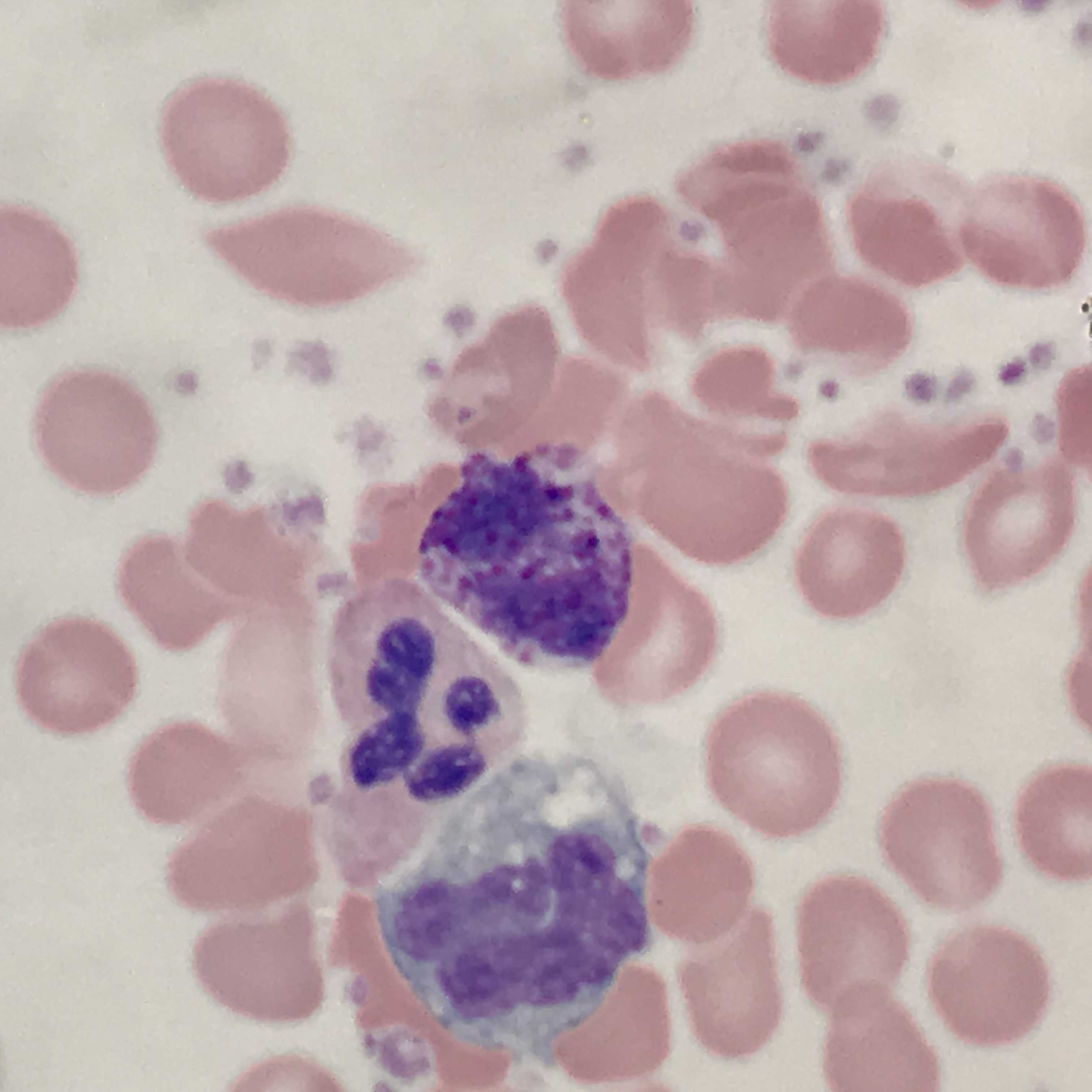
Monocyte, Neutrophil, and Basophil. This image shows a peripheral blood smear with red blood cells in the background and 3 leukocytes, a monocyte, a neutrophil, and a basophil.
Contributed by D Lynch, MD
References
Valent P, Sotlar K, Blatt K, Hartmann K, Reiter A, Sadovnik I, Sperr WR, Bettelheim P, Akin C, Bauer K, George TI, Hadzijusufovic E, Wolf D, Gotlib J, Mahon FX, Metcalfe DD, Horny HP, Arock M. Proposed diagnostic criteria and classification of basophilic leukemias and related disorders. Leukemia. 2017 Apr:31(4):788-797. doi: 10.1038/leu.2017.15. Epub 2017 Jan 16 [PubMed PMID: 28090091]
Boiten HJ, de Jongh E. Atypical basophilia. Blood. 2018 Aug 2:132(5):551. doi: 10.1182/blood-2018-05-849901. Epub [PubMed PMID: 30072416]
Han X, Jorgensen JL, Brahmandam A, Schlette E, Huh YO, Shi Y, Awagu S, Chen W. Immunophenotypic study of basophils by multiparameter flow cytometry. Archives of pathology & laboratory medicine. 2008 May:132(5):813-9 [PubMed PMID: 18466030]
Sadovnik I, Ivanov D, Smiljkovic D, Stefanzl G, Degenfeld-Schonburg L, Herndlhofer S, Eisenwort G, Hauswirth AW, Sliwa T, Keil F, Sperr WR, Valent P. Identification of CD203c as a New Basophil-Specific Flow-Marker in Ph(+) Chronic Myeloid Leukemia. Cells. 2022 Dec 20:12(1):. doi: 10.3390/cells12010003. Epub 2022 Dec 20 [PubMed PMID: 36611797]
Arinobu Y, Iwasaki H, Akashi K. Origin of basophils and mast cells. Allergology international : official journal of the Japanese Society of Allergology. 2009 Mar:58(1):21-8. doi: 10.2332/allergolint.08-RAI-0067. Epub 2009 Jan 25 [PubMed PMID: 19153533]
Arock M, Schneider E, Boissan M, Tricottet V, Dy M. Differentiation of human basophils: an overview of recent advances and pending questions. Journal of leukocyte biology. 2002 Apr:71(4):557-64 [PubMed PMID: 11927641]
Level 3 (low-level) evidenceMin B, Brown MA, Legros G. Understanding the roles of basophils: breaking dawn. Immunology. 2012 Mar:135(3):192-7. doi: 10.1111/j.1365-2567.2011.03530.x. Epub [PubMed PMID: 22044049]
Level 3 (low-level) evidenceStone KD, Prussin C, Metcalfe DD. IgE, mast cells, basophils, and eosinophils. The Journal of allergy and clinical immunology. 2010 Feb:125(2 Suppl 2):S73-80. doi: 10.1016/j.jaci.2009.11.017. Epub [PubMed PMID: 20176269]
Level 3 (low-level) evidenceKorošec P, Gibbs BF, Rijavec M, Custovic A, Turner PJ. Important and specific role for basophils in acute allergic reactions. Clinical and experimental allergy : journal of the British Society for Allergy and Clinical Immunology. 2018 May:48(5):502-512. doi: 10.1111/cea.13117. Epub 2018 Mar 23 [PubMed PMID: 29431885]
Siracusa MC, Kim BS, Spergel JM, Artis D. Basophils and allergic inflammation. The Journal of allergy and clinical immunology. 2013 Oct:132(4):789-801; quiz 788. doi: 10.1016/j.jaci.2013.07.046. Epub [PubMed PMID: 24075190]
Tanaka Y, Tanaka A, Hashimoto A, Hayashi K, Shinzato I. Acute Myeloid Leukemia with Basophilic Differentiation Transformed from Myelodysplastic Syndrome. Case reports in hematology. 2017:2017():4695491. doi: 10.1155/2017/4695491. Epub 2017 Mar 27 [PubMed PMID: 28428897]
Level 3 (low-level) evidenceThapa B, Fazal S, Parsi M, Rogers HJ. Myeloproliferative Neoplasms. StatPearls. 2024 Jan:(): [PubMed PMID: 30285359]
Vakiti A, Reynolds SB, Mewawalla P. Acute Myeloid Leukemia. StatPearls. 2024 Jan:(): [PubMed PMID: 29939652]
Chirumbolo S. State-of-the-art review about basophil research in immunology and allergy: is the time right to treat these cells with the respect they deserve? Blood transfusion = Trasfusione del sangue. 2012 Apr:10(2):148-64. doi: 10.2450/2011.0020-11. Epub 2011 Dec 21 [PubMed PMID: 22244003]
Kovalszki A, Weller PF. Eosinophilia. Primary care. 2016 Dec:43(4):607-617. doi: 10.1016/j.pop.2016.07.010. Epub 2016 Oct 14 [PubMed PMID: 27866580]
Chhabra G. Automated hematology analyzers: Recent trends and applications. Journal of laboratory physicians. 2018 Jan-Mar:10(1):15-16. doi: 10.4103/JLP.JLP_124_17. Epub [PubMed PMID: 29403197]
Arneth BM, Menschikowki M. Technology and new fluorescence flow cytometry parameters in hematological analyzers. Journal of clinical laboratory analysis. 2015 May:29(3):175-83. doi: 10.1002/jcla.21747. Epub 2014 May 5 [PubMed PMID: 24797912]
Sireci A, Schlaberg R, Kratz A. A method for optimizing and validating institution-specific flagging criteria for automated cell counters. Archives of pathology & laboratory medicine. 2010 Oct:134(10):1528-33 [PubMed PMID: 20923310]
Michael HT, Nabity MB, Couto CG, Moritz A, Harvey JW, DeNicola DB, Hammond JM. Improving quality control for in-clinic hematology analyzers: Common myths and opportunities. Veterinary clinical pathology. 2022 Sep:51(3):302-310. doi: 10.1111/vcp.13154. Epub [PubMed PMID: 36097323]
Level 2 (mid-level) evidenceGiannoli JM, Albarede S, Avellan T, Bouilloux JP, Cartier R, Cohen R, Colard N, Essemilaire L, Galinier JL, Kuentz M, Paris M, Portugal H, Scherrer F, Siest JP, Vassault A, Vialle JM. Recommendations for the application and follow-up of quality controls in medical laboratories. Biochemia medica. 2021 Jun 15:31(2):020501. doi: 10.11613/BM.2021.020501. Epub 2021 Apr 15 [PubMed PMID: 33927549]
Level 2 (mid-level) evidenceGulati G, Song J, Florea AD, Gong J. Purpose and criteria for blood smear scan, blood smear examination, and blood smear review. Annals of laboratory medicine. 2013 Jan:33(1):1-7. doi: 10.3343/alm.2013.33.1.1. Epub 2012 Dec 17 [PubMed PMID: 23301216]
Thompson PA, Kantarjian HM, Cortes JE. Diagnosis and Treatment of Chronic Myeloid Leukemia in 2015. Mayo Clinic proceedings. 2015 Oct:90(10):1440-54. doi: 10.1016/j.mayocp.2015.08.010. Epub [PubMed PMID: 26434969]
May PC, Reid AG, Robinson ME, Khorashad JS, Milojkovic D, Claudiani S, Genomics England Research Consortium, Willis F, Apperley JF, Innes AJ. FISH-negative BCR::ABL1-positive e19a2 chronic myeloid leukaemia: the most cryptic of insertions. BMC medical genomics. 2023 Jul 26:16(1):172. doi: 10.1186/s12920-023-01607-7. Epub 2023 Jul 26 [PubMed PMID: 37496024]
Viny AD, Levine RL. Genetics of myeloproliferative neoplasms. Cancer journal (Sudbury, Mass.). 2014 Jan-Feb:20(1):61-5. doi: 10.1097/PPO.0000000000000013. Epub [PubMed PMID: 24445766]
Valent P, Horny HP, Arock M. The underestimated role of basophils in Ph(+) chronic myeloid leukaemia. European journal of clinical investigation. 2018 Oct:48(10):e13000. doi: 10.1111/eci.13000. Epub 2018 Aug 6 [PubMed PMID: 30019447]
Zhou J, Papenhausen P, Shao H. Therapy-related acute myeloid leukemia with eosinophilia, basophilia, t(4;14)(q12;q24) and PDGFRA rearrangement: a case report and review of the literature. International journal of clinical and experimental pathology. 2015:8(5):5812-20 [PubMed PMID: 26191303]
Level 3 (low-level) evidenceTigner A, Ibrahim SA, Murray IV. Histology, White Blood Cell. StatPearls. 2024 Jan:(): [PubMed PMID: 33085295]
Stock W, Hoffman R. White blood cells 1: non-malignant disorders. Lancet (London, England). 2000 Apr 15:355(9212):1351-7 [PubMed PMID: 10776761]
Pastoret C, Houot R. "Chronic myelogenous leukemia in primary blast crisis" rather than "de novo BCR-ABL1-positive acute myeloid leukemia". Clinical case reports. 2017 Jun:5(6):757-760. doi: 10.1002/ccr3.937. Epub 2017 Apr 4 [PubMed PMID: 28588805]
Level 3 (low-level) evidence