Introduction
The basilar artery (BA) is formed over the surface of the pons by two vertebral arteries to supply the critical areas of the brain and brainstem. Anatomically, it is subdivided into three arbitrary segments: proximal from the vertebral artery (VA) to anterior inferior cerebellar arteries (AICA), middle from AICA to the origin of superior cerebellar arteries (SCA), and finally, the distal segment from SCA to the terminal posterior cerebral arteries (PCA).[1] Basilar artery infarct or occlusion (BAO) results from the obliteration of blood supply to the posterior circulation or vertebrobasilar system of arteries to the brain. BAO was first described in 1828 by Scottish physician John Abercrombie.[2]
The most common causes are atherosclerosis and thromboembolism from large vessel occlusion (LVO) or the heart. The clinical presentation can be very mild as nausea, dizziness, headache, confusion, and vertigo to severe symptoms like aphasia, dysarthria, dysphagia, hemiparesis/quadriparesis, loss of consciousness, coma, cranial nerve abnormalities, vision loss, and even cardiac or respiratory compromise which is usually lethal unless immediately identified to achieve revascularization.[1][3]
Reduced consciousness is the hallmark of basilar artery occlusion. A patient presenting with these brainstem symptoms and signs qualifies for rapid evaluation, consult with the stroke and endovascular teams, and an urgent imaging confirmation with computed tomography (CT) scan of the head, CT angiography of the head and neck, and/or magnetic resonance imaging (MRI) with or without perfusion imaging are usually done.[4] The whole process should not delay the administration of intraarterial thrombolytics like alteplase (tPA) or tenecteplase and transfer to the angiography suite for mechanical thrombectomy (MT) in eligible patients to achieve potentially good clinical outcomes.[5][6][7][8]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The common causes of ischemic stroke can also cause infarction in the basal artery territory. Interruption to the blood supply due to atherosclerosis or from an embolus anywhere from the heart to the basilar artery can cause the obliteration of flow through the basilar artery leading to an infarct of the brainstem (mainly pons) or brain region supplied by the basilar artery and its branches. The most commonly involved segments are the proximal and middle segments of the basilar artery.[9]
Atherosclerosis is the phenomenon by which factors such as dyslipoproteinemia, diabetes, cigarette smoking, and hypertension lead to injury to the intimal side of blood vessels, exposing collagen and releasing factors leading to platelet adhesion to the surface and forming a thrombus or plaque. Fatty streak is formed by the uptake of oxidized lipids and the transformation of macrophages into lipid-laden foam cells. When the plaque ruptures, it can occlude the vessel causing high-grade vessel stenosis, or the organizing thrombus can further disintegrate and throw the emboli into the cerebral circulation.
Alternatively, a small part of the thrombus can detach and cause the occlusion of small vessels distally. Both mechanical symptoms can eventually cause the occlusion of several vessels leading to an infarct in the corresponding cerebral territories. Another mechanism is cardioembolism from the heart, where a clot in the heart, mainly composed of fibrinogen, usually forms due to dysrhythmias like atrial fibrillation, metallic valve, severe mitral stenosis, significant myocardial infarction (MI), acute heart failure and wall motion abnormalities, etc. Rarely, external compression of the vertebral artery (bow hunter syndrome or vertebrobasilar insufficiency) can cause posterior circulation stroke, which needs either endovascular deconstruction or reconstruction, external surgical decompression, or surgical bypass techniques.[10]
COVID-19 infection has been shown to worsen the prothrombotic state associated with pregnancy and produce BAO.[11][12] An "8-shaped" basilar artery fenestration malformation, acute myelogenous leukemia, and Crohn disease can also lead to BAO.[13][14][15][14][13]
Epidemiology
Although the exact incidence of basilar artery occlusion remains unknown, it is estimated to account for 1% of all ischemic strokes.[16] Data from the center, including 129 patients with an LVO, showed that the estimated incidence was four persons per 100000/year.[17] As per the Basilar Artery International Cooperation Study (BASICS) registry, among 592 patients with basilar artery occlusion, the average age of the aorta is 63 years, with females being 37%, and admission National Institutes of Health Stroke Scale (NIHSS) of 22 (11 to 30).[18]
In this era of advanced imaging in diagnosing techniques, we need further prospective randomized studies to determine the current incidence and prevalence of this disease, mainly because we have more treatment options for this patient population.
Pathophysiology
Almost 30 to 35% of the strokes in posterior circulation are due to an embolus originating from an LVO in VA, BA, and PCA. An occlusion of BA is often due to an LVO by an embolism from the heart, aorta, or VA (36%), atherosclerosis of BA (35%), dissection (5%) of BA, and occasionally dolichoectasia or vasculopathy or undetermined (24%) causes.[18] Emboli usually arise from the heart or large arteries to cause occlusion of BA. In contrast, a thrombus may arise directly from the basilar artery due to atherosclerosis to produce BAO or may propagate from a thrombus from a VA due to atherosclerosis or dissection. Both the proximal and middle segments often become occluded due to thrombi arising from bilateral vertebral arteries, and an embolus from VA can lodge directly into the distal section.[1]
The perfusion pressure drops due to the presence of an embolus in the proximal portion of the basilar artery, causing a reversal of blood flow from bilateral PCAs, and this reflux can prevent an embolus from reaching the distal segment of the BA.[19] The basilar syndrome is mainly caused by distal basilar artery occlusion and involves behavioral disturbance, confusion, oculomotor, and visual abnormalities but often spares motor findings. The extent of thromboembolism can be a single-segment occlusion of BA or may involve all three segments of BA, and we can visualize this on vessel imaging, preferably CT angiography of the head and neck. With time, as the occlusion ages, the embolus becomes harder to get extracted by thrombectomy. Hence time is of utmost importance.
Histopathology
Microscopic examination of the brain tissue in the autopsies shows ischemic changes due to a thrombus or an embolus. The histopathology examination of the thrombus shows an increased amount of aggregated platelets consistent with atherosclerotic disease. In contrast, an increased amount of fibrinogen in the emboli extracted from basilar arteries is consistent with the cardioembolic etiology.
History and Physical
- Ipsilateral cranial nerve deficits, contralateral hemiparesis, sensory impairment, coordination deficits, quadriparesis, nausea, dizziness, headache, vertigo, aphasia, dysarthria, dysphagia, loss of consciousness, coma, and cardiopulmonary compromise can be caused by a variable degree of BAO.
- Confusion, oculomotor abnormalities, bilateral central vision loss, and often seizures can result from basilar tip occlusion, also called the top of the basilar syndrome.[20]
- Dysphagia, ataxia, and ipsilateral sensory impairment over the face, as well as Horner syndrome, are caused by occlusion of VA and PICA.
- Convulsion-like movement with rigidity and twitching can be an early symptom.[21][22]
Several signs and symptoms can guide history and physical examination.[1] The following is a summary of specific signs or symptoms based on the infarct location:
- Spinothalamic tracts, medial lemnisci, and thalamic nuclei involvement lead to anesthesia or hypesthesia.
- Corticospinal tracts in the cerebral peduncles and pons cause hemiplegia or quadriplegia and extensor plantar sign.
- Ascending reticular activating system with coma or impaired consciousness.
- Cerebellar peduncles, cerebellum, and proprioceptive tract involvement cause loss of coordination of limbs and posture (ataxia).
- Labyrinth, vestibulocerebellum, and vestibular nuclei involvement leads to loss of balance, vertigo, and directional nystagmus.
- Dorsal longitudinal fascicle (sympathetic fibers) dysfunction causes Horner syndrome.
- Trigeminal fibers' involvement causes head and neck pain.
- Efferent and afferent fibers and medullary autonomic nuclei cause cardiopulmonary signs and symptoms.
- Sympathetic and parasympathetic fibers and hypothalamic nuclei involvement lead to incontinence.
- Cranial nerve III nuclei, dorsal commissure, and rostral interstitial nucleus of the medial longitudinal fascicle (MLF) involvement lead to variable oculomotor palsy, bilateral ptosis, vertical gaze paresis, non-reactive pupils, anisocoria, and loss of vestibulocochlear reflex.
- MLF involvement causes internuclear ophthalmoplegia.
- CN VI nucleus and paramedian pontine reticular formation (PPRF) involvement cause horizontal oculocephalic reflex loss and horizontal gaze paresis.
- CN VII nuclei and corticobulbar tract involvement cause facial palsy.
- Cerebellar involvement causes gaze-evoked nystagmus.
- Brainstem oculomotor system, and CN II, III, IV and VI cause diplopia and strabismus.
- CN VII nuclei and lateral lemniscus involvement cause hearing loss, vertigo, and tinnitus.
- Cerebellum, corticobulbar tracts, and caudal cranial nerve nuclei (X, XI) involvement cause dysarthria and dysphagia.
- Occipital lobe involvement leads to vision loss or hemianopia.
- The medial temporal lobe and thalamic nuclei involvement cause memory disturbance, confusion, and disorientation.
- Pyramidal tract involvement causes jerking, shaking, convulsive seizures, and extension posturing or rigidity.
- Vertical one-and-a-half syndrome with pseudoabducens palsy and midbrain horizontal gaze paresis can occur due to an embolic infarct in the territory of the posterior thalamosubthalamic artery (artery of Percheron) arising at the basilar bifurcation.[23]
Evaluation
On arrival at the ED, the first test should be a CT head without contrast to rule out hemorrhagic stroke. In the meantime, quickly gather information including blood pressure, blood glucose level, the time of last known normal (LKN) or onset of stroke signs/symptoms (s/s), National Institute of Health Stroke Scale (NIHSS), use of anticoagulants/antiplatelets, past medical and surgical history, renal function, and if indicated run the alteplase (tPA) checklist. If the CT head is negative for bleed and there is a concern for basilar artery occlusion (BAO), subsequent intravenous access and CT angiogram of the head and neck are advised to rule out an LVO. If a CT angiogram is unobtainable, an MR angiogram can be used to evaluate cerebral vessels, provided no contraindication. MRI brain without contrast can be done later to characterize the stroke further, but it should not delay the revascularization treatment with intraarterial thrombolysis (IAT) and mechanical thrombectomy (MT).[24]
In the diffusion-weighted imaging (DWI) sequence of the MRI scan, the nerve density of the tracts in the pons may appear "SMOGGY" or "hazy" due to the diffusion restriction in the axonal tracts. This "smog sign" is a predictor of a good predictor of neurologic outcomes after mechanical thrombectomy.[8] The mid-basilar artery angle can increase the plaque burden and lead to an increase in the incidence of pontine infarction.[25]
Target mismatch: An initial infarct size of <70ml and a ratio of ischemic tissue to infarct volume of ≥1.8. This is recently found to be a possible candidate selection standard for endovascular therapy.[26]
An extended Thrombolysis In Cerebral Infarction (eTICI) grade of 2c/3 may be a target for successful reperfusion after EVT in patients with acute BAO.[27]
After the initial management, a stroke workup should be done to evaluate the cause to guide the goal-directed treatment. After the evaluation of vertebral and basilar circulations, other workup includes a transcranial doppler (TCD to find out the stability of plaque), transthoracic echocardiogram (TTE or TEE to rule out the clot, valvular abnormalities, wall motion abnormalities, and PFO), electrocardiogram, telemetry, event monitor or loop recorder (to rule out arrhythmias), and blood workup (HbA1c, lipid panel, homocysteine, and other workup based on etiology: antiphospholipid antibody syndrome, verify-now for platelet function, malignancy workup, etc.).[28]
Treatment / Management
If the patient has arrived within the tPA window (less than 3 to 4.5 hours since LKN) and has no contraindication to tPA, they should immediately receive alteplase/tPA or tenecteplase for the intraarterial thrombolysis. If eligible, the patient should be transferred to the angiography suite for mechanical thrombectomy (MT) within 24 hours of LKN.[4][5][24] Everyone should be considered for tPA if the patient has arrived in the ED within the window and has no contraindication. The patient should first receive tPA if eligible, and after tPA administration, the patient should transfer to an angiography suite for MT. Admit patients to the neuroscience ICU for post-tPA and post-MT care, including neuromonitoring, hemicraniectomy watch, airway watch, respiratory support, blood pressure management, and symptomatic care.[28] Further management should occur at the stroke unit with a multidisciplinary team approach rather than an admission to the general ward.[29](A1)
First-pass effect (FPE): Successful reperfusion using a single stent retriever attempt without salvage treatment (modified Thrombolysis in Cerebral Infarction score 2b-3). This has recently been associated with a 90-day favorable outcome in patients with acute BAO who had stent retriever thrombectomy within 24 hours.[30]
First-line stent retrieval has been shown to be associated with significantly lower odds of modified Thrombolysis in Cerebral Infarction (mTICI) 2b/3 and mTICI 3 recanalization rates when compared with direct aspiration, even though the former is associated with higher complication rate (not statistically significant).[31](A1)
A recent study encouraged at least three mechanical thrombectomy passes before stopping the procedure as it had a significant advantage of recanalization in BAO patients.[32]
Patients who are not tPA candidates and have a plaque burden in the posterior circulation are manageable through acute anticoagulation or an antiplatelet regimen. Recent data support using single or dual antiplatelet therapy over anticoagulation for large artery atherosclerotic disease, particularly if there is a large infarct burden.[33][34] (A1)
For intracranial atherosclerosis, it is recommended to use dual antiplatelets for 90 days after stroke and followed by aspirin only.[35] Further details regarding the management of basilar artery occlusion and ischemic stroke of currently available and ongoing data can be found in the "pertinent studies and ongoing trial" section of this review. However, be advised that most of the currently available data came from anterior circulation strokes rather than posterior circulation strokes. Secondary prevention, including the use of aspirin, atorvastatin, and anticoagulants if indicated. At the time of discharge, vascular risk factor modification with an LDL goal below 70, a blood pressure goal less than 130/80, and reasonable glycemic control with an A1c goal under 6.5, as well as goal-directed treatment, should be considered based on the etiology of stroke.[36] Also, lifestyle modifications, including the Mediterranean diet, smoking cessation, limiting alcohol, and no illicit drugs, have proven benefits in preventing stroke recurrence.(A1)
Differential Diagnosis
- Basilar meningitis
- Basilar migraine
- Cerebellar infarct with brainstem compression and edema
- Drug-intoxication
- Encephalopathy
- Hemorrhagic stroke:
- Cerebellar hemorrhage with brainstem compression
- Pontine hemorrhage
- Focal deficits due to brainstem bleeding from ruptured cerebral cavernous malformations, atriovenous malformation, and fistulas[37]
- Multiple sclerosis[38]
- Seizures
- Tumors in the posterior fossa, leading to mass effect and brainstem compression
Pertinent Studies and Ongoing Trials
Heparin after an Acute Ischemic Stroke
TOAST (Trial of ORG 10172 in Acute Stroke Treatment) trial [1998] showed no favorable 3-months outcomes with the use of heparinoids after an acute ischemic stroke.[39]
TPA (tissue Plasminogen activator or alteplase) after an acute ischemic stroke
NINDS (National Institute of Neurological Disorders and Stroke- tPA/tissue plasminogen activator/alteplase) trial [1995] reported significantly improved outcomes with the use of tPA within 3 hours of acute ischemic stroke onset, despite the increased risk of symptomatic intracerebral hemorrhage.[40]
Thrombectomy in LVO
- The DAWN (Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention With Trevo) trial [2018] showed that in patients with acute ischemic stroke with LVO who received medical management (MM) only versus medical management plus mechanical thrombectomy (MM+MT), with the onset of symptoms between 6 and 24 hours and having a mismatch between infarct core and clinical signs and symptoms, the 90 disability was lower in thrombectomy group as compared to patients receiving standard of care treatment.[5]
- DEFUSE-3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3) trial [2018] showed that in patients with acute ischemic stroke (MCA or ICA LVO), with MR perfusion mismatch ratio of greater than 1.8 and infarct volume of less than 70 mL; who received either medical management (MM) alone or medical management plus mechanical thrombectomy (MM+MT), within the 6-16 hours of symptoms onset, the 90 disability was lower in thrombectomy group as compared to patients receiving standard of care treatment.[4]
- BEST (Endovascular treatment vs. standard medical treatment for vertebrobasilar artery occlusion) and BASICS (Basilar Artery International Cooperation Study) failed to demonstrate significant benefits of endovascular therapy within 6 or 8 hours after stroke symptom onset.[41]
- BAOCHE (Basilar Artery Occlusion Chinese Endovascular) trial (NCT02737189) tries to identify the usefulness of BAO mechanical thrombectomy in a more extended window from the last known well (6–24 hours).[42]
Carotid Endarterectomy (CEA) for Atherosclerotic LVO
- NASCET (North American Symptomatic Carotid Endarterectomy (CEA) Trial Collaborators) trial [1991] showed the benefit of CEA in preventing ischemic strokes in patients with over 70% carotid artery stenosis after TIA and small strokes.
- CREST (Carotid Revascularization Endarterectomy (CEA) Versus Stenting (CAS) Trial) trial [2016] is a huge trial. After a long-term 10-year follow-up showed no net outcome difference between the two procedures except in patients over 70 years old, CAS might have more bleeding and procedural complications.[43]
Aspirin+Clopidogrel (dual antiplatelets) Appeared to be Superior to Aspirin Alone in Preventing Strokes after TIA/Small Ischemic Strokes
- The CHANCE (Clopidogrel in High-risk Patients With Acute Non-disabling Cerebrovascular Events) trial [2013] is also a randomized, double-blinded, placebo-controlled trial (including 5170 subjects) that compared aspirin monotherapy versus aspirin/clopidogrel in 114 centers across China. The bottom line suggests that in patients with acute TIA or small ischemic stroke, starting dual antiplatelet therapy (clopidogrel load 300 mg then 75 mg/d, aspirin 75 to 300mg/d and placebo group with no other thrombolytics for 30 days) after the symptom onset decreases 90-day stroke risk at the cost of a slightly increased bleeding risk as compared to aspirin monotherapy.[34]
- The POINT (Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke) trial [2018] is a randomized, double-blind, placebo-controlled trial (including 4881 subjects) that compared aspirin monotherapy versus aspirin/clopidogrel in 269 centers in North America, Europe, Australia, and New Zealand. The bottom line suggests that in patients with acute TIA or small ischemic stroke, starting dual antiplatelet therapy (clopidogrel load 600 mg then 75 mg/d, aspirin 75 to 325mg/d, and placebo group with no other thrombolytics for 30 days) after the symptom onset decreases 90-day stroke risk at the cost of a slightly increased bleeding risk as compared to aspirin monotherapy.[44]
- Summary of POINT and CHANCE trials: In the POINT trial, the duration of treatment was longer (90 versus 30 days), and the clopidogrel dose was higher (600 versus 300), but it is unclear if this was the reason for the slightly higher bleeding rates in POINT trial. Although pooled analysis shows that after comparing these two trials, the benefit of dual-antiplatelet therapy appeared limited to 21 days after an ischemic stroke.[45]
- The ASCEND (A Study of Cardiovascular Events iN Diabetes) trial [2018] showed that the use of aspirin for primary prevention therapy reduces the risk of serious vascular events in patients with well-controlled diabetes (A1c<8; 50% of patients).[33]
Intracranial Arterial Stenosis
SAMMPRIS (Stenting versus aggressive medical therapy for intracranial arterial stenosis) trial [2011] for intracranial arterial stenosis comparing the roles of addressive medical management (MM) with percutaneous transluminal angioplasty and stenting (PTAS) to prevent recurrent stroke. It reports that MM (i.e., dual antiplatelets for 90 days and aspirin after that) is superior to intracranial stenting in reducing ischemic stroke risk.[46]
Lacunar Strokes (Small Vessel Disease)
SPS 3 (Secondary Prevention of Small Subcortical Strokes) trial [2012] reported that among patients with lacunar strokes use of starting dual antiplatelet therapy (Aspirin and Plavix) is not associated with significant stroke risk-reduction but instead showed an increased risk of bleeding and mortality as compared to aspirin alone. Hence, dual antiplatelet therapy is not indicated after lacunar strokes.[47]
Afib (Atrial Fibrillation)[48]
- EMBRACE (30-Day Cardiac Event Monitor Belt for Recording Atrial Fibrillation After a Cerebral Ischemic Event) trial [2014] recommends 30-day cardiac monitoring to increase the yield of AFib detection and subsequent goal-directed anticoagulation treatment to prevent recurrent strokes by risk factor modification.[49]
- CRYSTAL AF (Study of Continuous Cardiac Monitoring to Assess Atrial Fibrillation After Cryptogenic Stroke) trial [2014] for AFib detection using prolonged cardiac monitoring for 6 to 12 months using an insertable cardiac monitor was proved superior in identifying atrial fibrillation in patients after the admission of stroke.[50]
Cryptogenic Strokes and Atrial Cardiopathy
- ARCADIA (AtRial Cardiopathy and Antithrombotic Drugs In prevention After cryptogenic stroke) trial [2019] is currently enrolling patients with cryptogenic strokes based on atrial cardiopathy on echocardiogram, NTpBNP, and EKG V1 findings.[51]
Patent Foramen Ovale (PFO) Closure
- RESPECT (Randomized Evaluation of Recurrent Stroke Comparing PFO Closure to Established Current Standard of Care Treatment) trial [2017] showed that the combined PFO closure and antiplatelet therapy are superior to medical management (antiplatelets) alone in preventing recurrent ischemic strokes.[52]
- CLOSE (Patent Foramen Ovale Closure or Anticoagulants Versus Antiplatelet Therapy to Prevent Stroke Recurrence) trial [2017] reports that combined large PFO closure and antiplatelet therapy is superior to medical management (antiplatelets) alone to prevent recurrent ischemic strokes but with an increased risk of atrial fibrillation after PFO closure.[53]
Hyperlipidemia and Hypertriglyceridemia
- SPARCL (Lipitor In The Prevention Of Stroke, For Patients Who Have Had A Previous Stroke) trial [2006] for high-dose statin use in patients with TIA or ischemic stroke showed significant stroke risk-reduction with the use of high dose (81mg) atorvastatin by treating and preventing atherosclerosis.[54]
- REDUCE-IT (Reduction of Cardiovascular Events With EPA - Intervention Trial) [2019] trial reports a reduction in stroke risk in patients who received Icosapent Ethyl (highly purified eicosapentaenoic acid ethyl ester) twice daily (toral 4 g/Day)with hypertriglyceridemia despite being on high-dose statin therapy.[55]
Post-stroke depression, motor recovery, and the role of SSRI
FLAME (Fluoxetine on Motor Rehabilitation After Ischemic Stroke) trial [2011] showed improved motor recovery in patients with hemiplegia and hemiparesis with the use of fluoxetine.[56]
Endovascular Treatment in Ischemic Stroke (ETIS)
Safety, outcome, and quality of endovascular therapy for stroke due to acute BAO under either conscious sedation/local anesthesia or general anesthesia have been found to be similar.[57]
Treatment Planning
As described above, initial revascularization followed by secondary prevention should be performed in BAO patients.[28]
Toxicity and Adverse Effect Management
The most significant side effects of thrombolysis and mechanical thrombectomy are intracranial hemorrhagic transformation, groin/femoral artery perforation/bleeding complications, death, and disability. Prognosis and outcomes should be urgently discussed with the family while administering alteplase and wheeling patients for thrombectomy.
Prognosis
The prognosis of BAO depends on the severity of the stroke, time to LKN, the treatment offered, successful recanalization, and access to tertiary care hospitals and comprehensive stroke centers. Overall, mortality is very high in this population; patients with successful recanalization after thrombectomy has a lower mortality rate of 33 to 50% versus 74 to 100% in patients without thrombectomy or failed reperfusion.[58] With early arrival and appropriate management, as described above, the outcome may be good, with minimum deficits. But late arrival and failure of revascularisation of BAO invariably result in poor outcomes, including severe neurological deficits and very high mortality in these patients.
The pre-endovascular treatment diffusion-weighted imaging cerebellar infarct volume is an independent predictor of 90-day mortality.[59]
Complications
- Death
- Intracranial or extracranial bleeding
- Reperfusion syndrome
- Ischemic stroke
- Groin puncture site hematoma, fistula, and intraabdominal bleeding
- Infections (urinary tract infection, pneumonia)
- Pressure ulcers
- Contractures
- Dysphonia
- Dysphagia
- Deep vein thrombosis/pulmonary embolism[60]
Postoperative and Rehabilitation Care
- Respiratory therapy
- Physical therapy
- Occupational therapy
- Speech therapy
- Acupuncture therapy has been studied to improve the blood flow velocity of vertebrobasilar arteries in patients with posterior circulation infarction vertigo.[61]
Consultations
An interprofessional team approach, including the emergency department, neurology (stroke), neurosurgery, neurocritical teams, nursing, physical therapy, occupational therapy, and speech therapy collaboration, is essential and the key to good patient outcomes with basilar artery occlusion.
Deterrence and Patient Education
Counsel the patient and family regarding stroke that the risk of a stroke can be decreased by appropriately treating diabetes, hypertension, high cholesterol, cardiac diseases, and obesity, quitting smoking, reducing alcohol intake, and staying physically active. Discuss the BE-FAST (balance loss, eyesight, facial droop, arm weakness, slurry speech, time) symptoms awareness on all the media and public education channels and campaigns. Time is of the essence if they notice symptomatic onset.
As mentioned above, the risk of a stroke can be decreased by treating hypertension, high cholesterol, diabetes, heart disease, and obesity, quitting smoking, limiting alcohol, and staying physically active. Time is of the essence. It is essential to seek treatment within 3 to 4.5 hours of the start of symptoms because, during that time, thrombolytic drugs are an option. Even if one does not know when symptoms began, get treatment as soon as possible. After the 4.5-hour window has passed, treatment may include rest, oxygen, intravenous (IV) fluids, and medicines to thin the blood (anticoagulants). Treatment of stroke depends on the duration, severity, and cause of one's symptoms. Medications and diet may be used to address diabetes, high blood pressure, and other risk factors.
Physical, speech, and occupational therapists will assess and work to improve any functions impaired by the stroke. Measures will be taken to prevent short-term and long-term complications, including infection from breathing foreign material into the lungs (aspiration pneumonia), blood clots in the legs, bedsores, and falls. Rarely, surgery may be necessary to remove large blood clots or to open up blocked arteries.
Pearls and Other Issues
- For basilar artery infarction, currently available data is inadequate and needs further extensive randomized prospective clinical trials to study pathophysiology. A better scoring system must be developed dedicated to posterior circulation strokes for prognostication of ischemic strokes secondary to BAO. Also, educational programs and campaigns should be done regarding BAO for both healthcare providers and patients to improve the outcomes of this devastating disease process.
- Other emerging therapies include the MRI-guided high-intensity focused ultrasound (HIFU) technique, which uses thermal heating for sonothrombolysis and ablation.[62] Some in-vitro and in-vivo studies have evidenced it, but in both ischemic and hemorrhagic strokes, more extensive prospective studies are necessary. This technique should have research for basilar artery infarcts due to basilar artery anatomy and potential ease of access in performing thrombolysis.
- A small number of strokes occur after cardiac and cardiovascular bypass grafting surgeries. Using perioperative epiaortic ultrasound is potentially useful to detect thrombus during surgery to prevent perioperative ischemic strokes.[63]
- Elevated levels of cytokines like interleukin-37 are associated with an acute ischemic stroke, and further studies are being conducted to determine the role of these chemokines and cytokines in the CRISP trial (NCT03297827).[64]
Enhancing Healthcare Team Outcomes
Measures should be taken to prevent short-term and long-term complications, including infection from breathing foreign material into the lungs (aspiration pneumonia), UTI, DVT, PE, bedsores, dysphonia, dysphagia, and falls. Aggressive physical and occupational therapies should treat post-stroke complications like contractures, follow-up in the neurology clinic, and consideration of botox injection may help recover from contractures. Rarely, surgery may be needed to remove large blood clots or to open up blocked arteries. Another significant complication is post-stroke depression; we should be treated with citalopram or fluoxetine, which has been proven beneficial and recent studies for post-stroke depression and motor recovery after stroke.
There is a lot of high-quality evidence regarding the prevention and management of stroke, as described in any organized and comprehensive stroke guidelines in 2018.[65] Here is the summary of stroke prevention and management with the corresponding class of recommendation (COR=strength of study) and level of evidence (LOE=quality of study):
- Prehospital systems:
- "Time is brain," hence, time is of crucial importance that prehospital arrangements be made so that patients can be brought to the hospital for treatment as early as possible. There is a need for education like BE-FAST (dependence, eye or vision, facial droop, arm weakness, speech slurring, and time), etc., as well as education programs and awareness campaigns to make the general population aware of the importance of time. Especially, African-Americans, Native Americans, Hispanics, and other underserved populations are greatly affected due to the lack of awareness. This issue merits attention in a very systemized, targeted manner and campaign. [COR: I and LOE: B-R]
- Activating stroke alert by calling 9–1–1 for any stroke symptom should be encouraged to the public, including family members, who are bystanders witnessing someone with the symptoms described above. [COR-I and LOE B-NR]
- It is a strong recommendation that due to increased awareness and decreased time to transit to the hospital, more patients are treated, and expand programs for the education of healthcare professionals, including physicians, EMTs, and patients. [COR: I and LOE B-NR]
- Hospital stroke teams:
- There should be stress on very organized emergency and stroke teams in the hospital. For that, there should be a validated protocol for standard procedures established as soon as the hospital is alerted of stroke arrival by EMS so stroke alert can be activated. The stroke team should be readily available in the emergency department to manage the stroke appropriately. In summary, the recommendation is that the clinical staff sees the patient within 15 minutes of ED arrival, CT head without contrast takes place within 25 minutes of ED arrival, and TPA or door-to-needle time should be 60 minutes. [COR-I and LOE B-NR]
- Organization and capacity building:
- In small hospitals or primary stroke centers, realistic measures should be in place so that initial studies, including vascular imaging like CT angiograms, are possible in those hospitals before transferring to the larger centers are comprehensive stroke centers. [COR: IIb and LOE: C-LD]
- Mechanical thrombectomy should be performed in the larger stroke centers, with the capacities and capabilities of stroke teams, neurologists, neuro-interventionists, and the availability of advanced imaging, including perfusion scans, etc. [COR: I and LOE: C-EO]
- Data Repositories:
- It is highly encouraged to build date the repository and research registries in the centers so that adherence to the protocols and guidelines as well as improvement in patient outcomes is done [COR: I and LOE: B-NR]
- Telemedicine and telestroke services [COR: I and LOE: A]
- Use of Stroke Scales like NIH stroke scale [COR: I and LOE: B-NR]
- Quality improvement processes and system for stroke [COR: I and LOE: B-NR]
- To prevent a recurrence, the primary care providers and the stroke nurse should educate the patient on lowering the risk factors; this means discontinuing smoking, exercising regularly, controlling blood pressure and lipids, and eating a healthy diet.
An interprofessional team approach is necessary for improving outcomes in patients with basilar strokes. In addition to the various clinical specialties already covered, a pharmacist should consult for thrombolytic therapy; this may well be a cardiac board-certified pharmacist. The stroke-certified nursing staff is an invaluable resource, irrespective of which direction therapy takes; they can help evaluate the patient, assist during procedures, and monitor the patient's condition following interventions, charting, and reporting their findings for the clinician staff. These types of interprofessional actions enhance patient outcomes in basilar artery occlusion and other types of strokes. [Level 5]
Media
(Click Image to Enlarge)

Basilar artery infarct Image courtesy S Bhimji MD
(Click Image to Enlarge)

Diagram of the Posterior Cerebral Artery and its Branches. Each number corresponds to the following neuroanatomy: 1) basilar artery; 2) superior cerebellar artery; 3) posterior cerebral artery; 4) thalamic subthalamic arteries; 5) posterior communicating artery; 6) internal carotid artery; 7) polar artery of thalamus; 8) posterior choroidal artery; 9) thalamogeniculate artery; 10) anterior inferior temporal artery; 11) posterior inferior temporal artery; 12) occipitotemporal artery; 13) calcarine arteries; and 14) occipitoparietal artery.
Contributed by O Kuybu, MD
(Click Image to Enlarge)
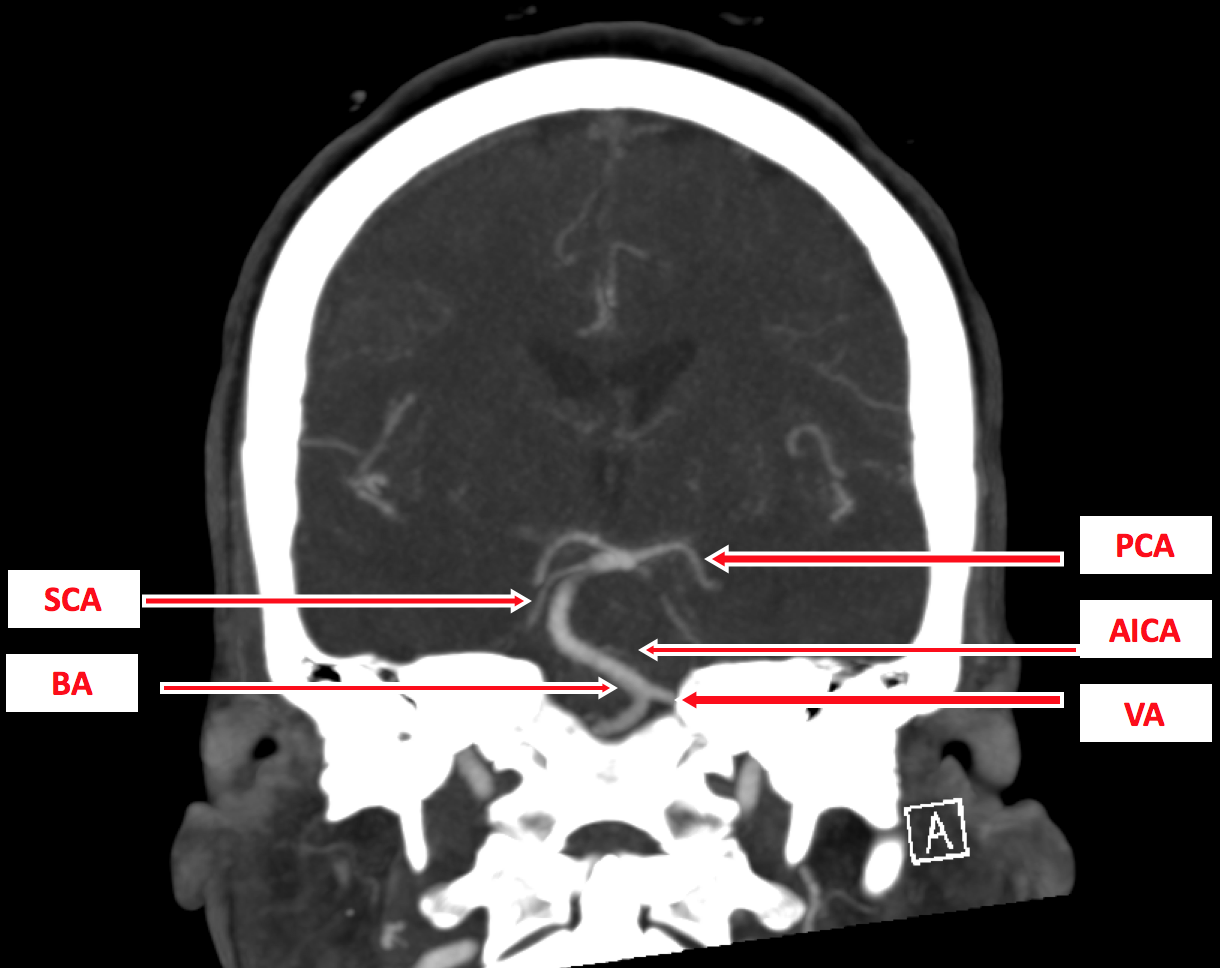
Figure 3 - A coronal section on CTA for posterior circulation: vertebral artery (VA); basilar artery (BA); anterior inferior cerebellar artery (AICA); superior cerebellar artery (SCA); posterior cerebral artery (PCA). Contributed by Okkes Kuybu, MD
(Click Image to Enlarge)
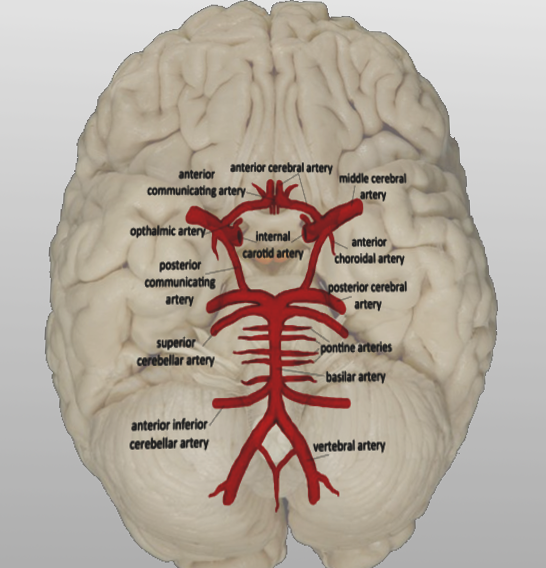
Vertebrobasilar system Image courtesy S Bhimji MD
References
Mattle HP, Arnold M, Lindsberg PJ, Schonewille WJ, Schroth G. Basilar artery occlusion. The Lancet. Neurology. 2011 Nov:10(11):1002-14. doi: 10.1016/S1474-4422(11)70229-0. Epub [PubMed PMID: 22014435]
Kompanje EJ, Walgaard C, de Groot YJ, Stevens M. Historical sources of basilar artery occlusion. Neurology. 2011 Apr 26:76(17):1520-3. doi: 10.1212/WNL.0b013e318217e755. Epub [PubMed PMID: 21519003]
Voetsch B, DeWitt LD, Pessin MS, Caplan LR. Basilar artery occlusive disease in the New England Medical Center Posterior Circulation Registry. Archives of neurology. 2004 Apr:61(4):496-504 [PubMed PMID: 15096396]
Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega-Gutierrez S, McTaggart RA, Torbey MT, Kim-Tenser M, Leslie-Mazwi T, Sarraj A, Kasner SE, Ansari SA, Yeatts SD, Hamilton S, Mlynash M, Heit JJ, Zaharchuk G, Kim S, Carrozzella J, Palesch YY, Demchuk AM, Bammer R, Lavori PW, Broderick JP, Lansberg MG, DEFUSE 3 Investigators. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. The New England journal of medicine. 2018 Feb 22:378(8):708-718. doi: 10.1056/NEJMoa1713973. Epub 2018 Jan 24 [PubMed PMID: 29364767]
Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, Yavagal DR, Ribo M, Cognard C, Hanel RA, Sila CA, Hassan AE, Millan M, Levy EI, Mitchell P, Chen M, English JD, Shah QA, Silver FL, Pereira VM, Mehta BP, Baxter BW, Abraham MG, Cardona P, Veznedaroglu E, Hellinger FR, Feng L, Kirmani JF, Lopes DK, Jankowitz BT, Frankel MR, Costalat V, Vora NA, Yoo AJ, Malik AM, Furlan AJ, Rubiera M, Aghaebrahim A, Olivot JM, Tekle WG, Shields R, Graves T, Lewis RJ, Smith WS, Liebeskind DS, Saver JL, Jovin TG, DAWN Trial Investigators. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. The New England journal of medicine. 2018 Jan 4:378(1):11-21. doi: 10.1056/NEJMoa1706442. Epub 2017 Nov 11 [PubMed PMID: 29129157]
Campbell BC, Mitchell PJ, Churilov L, Yassi N, Kleinig TJ, Yan B, Thijs V, Desmond PM, Parsons MW, Donnan GA, Davis SM. Determining the optimal dose of tenecteplase before endovascular therapy for ischemic stroke (EXTEND-IA TNK Part 2): A multicenter, randomized, controlled study. International journal of stroke : official journal of the International Stroke Society. 2020 Jul:15(5):567-572. doi: 10.1177/1747493019879652. Epub 2019 Sep 30 [PubMed PMID: 31564231]
Level 1 (high-level) evidenceRavindren J, Aguilar Pérez M, Hellstern V, Bhogal P, Bäzner H, Henkes H. Predictors of Outcome After Endovascular Thrombectomy in Acute Basilar Artery Occlusion and the 6hr Time Window to Recanalization. Frontiers in neurology. 2019:10():923. doi: 10.3389/fneur.2019.00923. Epub 2019 Sep 25 [PubMed PMID: 31608001]
Ikram A,Farooqui M,Suriya S,Quadri SA,Zafar A, Smog Sign: Hazy Diffusion-weighted Imaging Restriction in Dense Axonal Tracts in the Pons on Hyperacute MRI with Remarkable Clinical Improvement After Intra-arterial Thrombectomy. Cureus. 2019 Aug 22; [PubMed PMID: 31641558]
Savitz SI, Caplan LR. Vertebrobasilar disease. The New England journal of medicine. 2005 Jun 23:352(25):2618-26 [PubMed PMID: 15972868]
Berti AF, Zafar A, Ikram A, Calder CS, Sorte DE. Recurrent posterior circulation infarcts secondary to vertebral artery external compression treated with endovascular deconstruction. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2018 Apr:24(2):178-182. doi: 10.1177/1591019917747879. Epub 2017 Dec 14 [PubMed PMID: 29239686]
Gómez-Martí M, Boschín V, Puchades F, Cerdán A, Cunquero A, Sanz F, Tamarit JJ. [Ischaemic stroke due to basilar artery occlusion in a puerperal patient with SARS-CoV-2 infection]. Revista de neurologia. 2022 Aug 16:75(4):97-100. doi: 10.33588/rn.7504.2021373. Epub [PubMed PMID: 35866535]
Tsuchiya T,Koizumi S,Tomioka A,Miyawaki S,Saito N, Acute Ischemic Stroke Due to Basilar Artery Occlusion with Coronavirus Disease 2019: A Case Report. NMC case report journal. 2021 [PubMed PMID: 35079520]
Level 3 (low-level) evidenceZhang W, Xing W, Gu H, He J. Acute pontine infarction in a patient with 8-shaped basilar artery fenestration malformation: A case report. Medicine. 2022 Jul 8:101(27):e29445. doi: 10.1097/MD.0000000000029445. Epub 2022 Jul 8 [PubMed PMID: 35801744]
Level 3 (low-level) evidenceAoki T, Kuwayama K, Kobata H, Ito A, Fuji K, Sakamoto M, Furuno Y, Matsumoto K. Endovascular Mechanical Thrombectomy for Basilar Artery Occlusion Caused by Thrombosis as an Initial Manifestation of Acute Myelogenous Leukemia: A Case Report. NMC case report journal. 2021:8(1):767-772. doi: 10.2176/nmccrj.cr.2021-0212. Epub 2021 Nov 2 [PubMed PMID: 35079546]
Level 3 (low-level) evidenceDeshpande GG, Riffle RM, Meagher S. Basilar artery stroke in Crohn's disease treated with endovascular thromboembolectomy. BMJ case reports. 2022 Apr 11:15(4):. doi: 10.1136/bcr-2021-244652. Epub 2022 Apr 11 [PubMed PMID: 35410945]
Level 3 (low-level) evidenceIsraeli-korn SD,Schwammenthal Y,Yonash-Kimchi T,Bakon M,Tsabari R,Orion D,Bruk B,Molshatzki N,Merzeliak O,Chapman J,Tanne D, Ischemic stroke due to acute basilar artery occlusion: proportion and outcomes. The Israel Medical Association journal : IMAJ. 2010 Nov; [PubMed PMID: 21243866]
Level 2 (mid-level) evidenceRai AT, Seldon AE, Boo S, Link PS, Domico JR, Tarabishy AR, Lucke-Wold N, Carpenter JS. A population-based incidence of acute large vessel occlusions and thrombectomy eligible patients indicates significant potential for growth of endovascular stroke therapy in the USA. Journal of neurointerventional surgery. 2017 Aug:9(8):722-726. doi: 10.1136/neurintsurg-2016-012515. Epub 2016 Jul 15 [PubMed PMID: 27422968]
Schonewille WJ, Wijman CA, Michel P, Rueckert CM, Weimar C, Mattle HP, Engelter ST, Tanne D, Muir KW, Molina CA, Thijs V, Audebert H, Pfefferkorn T, Szabo K, Lindsberg PJ, de Freitas G, Kappelle LJ, Algra A, BASICS study group. Treatment and outcomes of acute basilar artery occlusion in the Basilar Artery International Cooperation Study (BASICS): a prospective registry study. The Lancet. Neurology. 2009 Aug:8(8):724-30. doi: 10.1016/S1474-4422(09)70173-5. Epub 2009 Jul 3 [PubMed PMID: 19577962]
Ferbert A, Brückmann H, Drummen R. Clinical features of proven basilar artery occlusion. Stroke. 1990 Aug:21(8):1135-42 [PubMed PMID: 2389292]
Conte WL,Gill CE,Biller J, Top of the Basilar Syndrome Presenting With Convulsions. JAMA neurology. 2017 Feb 1 [PubMed PMID: 27992635]
Wang TL, Wu G, Liu SZ. Convulsive-like movements as the first symptom of basilar artery occlusive brainstem infarction: A case report. World journal of clinical cases. 2022 May 16:10(14):4569-4573. doi: 10.12998/wjcc.v10.i14.4569. Epub [PubMed PMID: 35663090]
Level 3 (low-level) evidenceInui R, Fujiwara S, Kuroda T, Ohara N, Imamura H, Kohara N, Ariyoshi K, Kawamoto M, Sakai N. Convulsive-like symptoms as initial indications of basilar artery occlusion: A case series study. eNeurologicalSci. 2022 Sep:28():100410. doi: 10.1016/j.ensci.2022.100410. Epub 2022 Jun 16 [PubMed PMID: 35757457]
Level 2 (mid-level) evidenceAladdin Y, Shirah B, Khan K. Vertical One-and-a-Half Syndrome with Pseudoabducens Palsy and Midbrain Horizontal Gaze Paresis. Journal of binocular vision and ocular motility. 2022 Jul-Sep:72(3):156-160 [PubMed PMID: 35616639]
Meinel TR,Kaesmacher J,Chaloulos-Iakovidis P,Panos L,Mordasini P,Mosimann PJ,Michel P,Hajdu S,Ribo M,Requena M,Maegerlein C,Friedrich B,Costalat V,Benali A,Pierot L,Gawlitza M,Schaafsma J,Pereira VM,Gralla J,Fischer U, Mechanical thrombectomy for basilar artery occlusion: efficacy, outcomes, and futile recanalization in comparison with the anterior circulation. Journal of neurointerventional surgery. 2019 Jun 25; [PubMed PMID: 31239331]
Li Y, Chen F, Yang B, Xie S, Wang C, Guo R, Zhang X, Liu Z. Effect of Mid-Basilar Artery Angle and Plaque Characteristics on Pontine Infarction in Patients with Basilar Artery Plaque. Journal of atherosclerosis and thrombosis. 2023 Feb 1:30(2):182-191. doi: 10.5551/jat.63520. Epub 2022 Apr 13 [PubMed PMID: 35418542]
Yan S, Zhou Y, Zhao Y, Wang F, Tao A, Zhou L, Pan M, Zhong G, Hu L, Jiang X, Mao X, Tang H, Wang J, Qian S, Sun J, Gong X, Zhong W, Lou M, CASE II investigators. Effect of Imaging Markers on Reperfusion Therapy in Basilar Artery Occlusion. Annals of neurology. 2022 Jul:92(1):97-106. doi: 10.1002/ana.26376. Epub 2022 May 4 [PubMed PMID: 35438200]
Level 2 (mid-level) evidenceChen L, Zhao C, Song J, Zi W, Sang H, Yuan J, Huang J, Li L, Luo W, Fu X, Zhou P, Wan Y, Zeng G, Xie D, Gao F, Li F, Qiu Z, Yang Q. Extended Thrombolysis In Cerebral Infarction (eTICI) grade 2c: a potential angiographic target for endovascular treatment in acute basilar artery occlusion? Journal of neurointerventional surgery. 2022 Oct:14(10):1022-1026. doi: 10.1136/neurintsurg-2021-018026. Epub 2021 Nov 15 [PubMed PMID: 34782398]
Level 2 (mid-level) evidencePowers WJ,Rabinstein AA,Ackerson T,Adeoye OM,Bambakidis NC,Becker K,Biller J,Brown M,Demaerschalk BM,Hoh B,Jauch EC,Kidwell CS,Leslie-Mazwi TM,Ovbiagele B,Scott PA,Sheth KN,Southerland AM,Summers DV,Tirschwell DL, 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2018 Mar; [PubMed PMID: 29367334]
Stroke Unit Trialists' Collaboration. Organised inpatient (stroke unit) care for stroke. The Cochrane database of systematic reviews. 2013 Sep 11:2013(9):CD000197. doi: 10.1002/14651858.CD000197.pub3. Epub 2013 Sep 11 [PubMed PMID: 24026639]
Level 1 (high-level) evidenceZhao C, Hu T, Kong W, Yang D, Wan J, Lv K, Liao J, Chen Z, Jiang H, Wu D, Yang P, Zi W, Li F, Yang Q. First-pass effect in patients with acute basilar artery occlusions undergoing stent retriever thrombectomy. Journal of neurosurgery. 2023 Mar 1:138(3):693-700. doi: 10.3171/2022.5.JNS22751. Epub 2022 Jul 8 [PubMed PMID: 35901699]
Xenos D, Texakalidis P, Karras CL, Murthy NK, Kontzialis M, Rivet DJ, Reavey-Cantwell J. First-Line Stent Retriever versus Direct Aspiration for Acute Basilar Artery Occlusions: A Systematic Review and Meta-analysis. World neurosurgery. 2022 Feb:158():258-267.e1. doi: 10.1016/j.wneu.2021.11.013. Epub 2021 Nov 11 [PubMed PMID: 34775090]
Level 1 (high-level) evidencede Havenon A,Elhorany M,Boulouis G,Naggara O,Darcourt J,Clarençon F,Richard S,Marnat G,Bourcier R,Sibon I,Arquizan C,Dargazanli C,Maïer B,Seners P,Lapergue B,Consoli A,Eugene F,Vannier S,Caroff J,Denier C,Boulanger M,Gauberti M,Rouchaud A,Macian F,Rosso C,Turc G,Ozkul-Wermester O,Papagiannaki C,Albucher JF,Le Bras A,Evain S,Wolff V,Pop R,Timsit S,Gentric JC,Bourdain F,Veunac L,Fahed R,Finitsis SN,Gory B,ETIS Registry Investigators., Thrombectomy in basilar artery occlusions: impact of number of passes and futile reperfusion. Journal of neurointerventional surgery. 2022 Apr 21 [PubMed PMID: 35450929]
ASCEND Study Collaborative Group, Bowman L, Mafham M, Wallendszus K, Stevens W, Buck G, Barton J, Murphy K, Aung T, Haynes R, Cox J, Murawska A, Young A, Lay M, Chen F, Sammons E, Waters E, Adler A, Bodansky J, Farmer A, McPherson R, Neil A, Simpson D, Peto R, Baigent C, Collins R, Parish S, Armitage J. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. The New England journal of medicine. 2018 Oct 18:379(16):1529-1539. doi: 10.1056/NEJMoa1804988. Epub 2018 Aug 26 [PubMed PMID: 30146931]
Wang Y, Wang Y, Zhao X, Liu L, Wang D, Wang C, Wang C, Li H, Meng X, Cui L, Jia J, Dong Q, Xu A, Zeng J, Li Y, Wang Z, Xia H, Johnston SC, CHANCE Investigators. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. The New England journal of medicine. 2013 Jul 4:369(1):11-9. doi: 10.1056/NEJMoa1215340. Epub 2013 Jun 26 [PubMed PMID: 23803136]
Level 1 (high-level) evidenceDerdeyn CP, Chimowitz MI, Lynn MJ, Fiorella D, Turan TN, Janis LS, Montgomery J, Nizam A, Lane BF, Lutsep HL, Barnwell SL, Waters MF, Hoh BL, Hourihane JM, Levy EI, Alexandrov AV, Harrigan MR, Chiu D, Klucznik RP, Clark JM, McDougall CG, Johnson MD, Pride GL Jr, Lynch JR, Zaidat OO, Rumboldt Z, Cloft HJ, Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis Trial Investigators. Aggressive medical treatment with or without stenting in high-risk patients with intracranial artery stenosis (SAMMPRIS): the final results of a randomised trial. Lancet (London, England). 2014 Jan 25:383(9914):333-41. doi: 10.1016/S0140-6736(13)62038-3. Epub 2013 Oct 26 [PubMed PMID: 24168957]
Level 1 (high-level) evidenceKernan WN,Ovbiagele B,Black HR,Bravata DM,Chimowitz MI,Ezekowitz MD,Fang MC,Fisher M,Furie KL,Heck DV,Johnston SC,Kasner SE,Kittner SJ,Mitchell PH,Rich MW,Richardson D,Schwamm LH,Wilson JA, Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014 Jul; [PubMed PMID: 24788967]
Zafar A, Quadri SA, Farooqui M, Ikram A, Robinson M, Hart BL, Mabray MC, Vigil C, Tang AT, Kahn ML, Yonas H, Lawton MT, Kim H, Morrison L. Familial Cerebral Cavernous Malformations. Stroke. 2019 May:50(5):1294-1301. doi: 10.1161/STROKEAHA.118.022314. Epub [PubMed PMID: 30909834]
Zulfiqar M, Qeadan F, Ikram A, Farooqui M, Richardson SP, Calder CS, Quadri SA, Mathur P, Ford C, O Gutierrez S, Liera E, Snow H, N Gonzalez J, Zafar A. Intracerebral Hemorrhage in Multiple Sclerosis: A Retrospective Cohort Study. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2019 Feb:28(2):267-275. doi: 10.1016/j.jstrokecerebrovasdis.2018.09.050. Epub 2018 Oct 29 [PubMed PMID: 30385221]
Level 2 (mid-level) evidence. Low molecular weight heparinoid, ORG 10172 (danaparoid), and outcome after acute ischemic stroke: a randomized controlled trial. The Publications Committee for the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) Investigators. JAMA. 1998 Apr 22-29:279(16):1265-72 [PubMed PMID: 9565006]
Level 1 (high-level) evidenceTissue plasminogen activator for acute ischemic stroke. The New England journal of medicine. 1995 Dec 14; [PubMed PMID: 7477192]
Level 1 (high-level) evidenceYu W, Higashida RT. Endovascular Thrombectomy for Acute Basilar Artery Occlusion: Latest Findings and Critical Thinking on Future Study Design. Translational stroke research. 2022 Dec:13(6):913-922. doi: 10.1007/s12975-022-01008-5. Epub 2022 Mar 29 [PubMed PMID: 35349051]
Li C, Wu C, Wu L, Zhao W, Chen J, Ren M, Yao C, Yan X, Dong C, Song H, Ma Q, Duan J, Zhang Y, Zhang H, Jiao L, Wang Y, Jovin TG, Ji X, BAOCHE Investigators. Basilar Artery Occlusion Chinese Endovascular Trial: Protocol for a prospective randomized controlled study. International journal of stroke : official journal of the International Stroke Society. 2022 Jul:17(6):694-697. doi: 10.1177/17474930211040923. Epub 2021 Aug 28 [PubMed PMID: 34427475]
Level 1 (high-level) evidenceBrott TG, Howard G, Roubin GS, Meschia JF, Mackey A, Brooks W, Moore WS, Hill MD, Mantese VA, Clark WM, Timaran CH, Heck D, Leimgruber PP, Sheffet AJ, Howard VJ, Chaturvedi S, Lal BK, Voeks JH, Hobson RW 2nd, CREST Investigators. Long-Term Results of Stenting versus Endarterectomy for Carotid-Artery Stenosis. The New England journal of medicine. 2016 Mar 17:374(11):1021-31. doi: 10.1056/NEJMoa1505215. Epub 2016 Feb 18 [PubMed PMID: 26890472]
Johnston SC, Easton JD, Farrant M, Barsan W, Conwit RA, Elm JJ, Kim AS, Lindblad AS, Palesch YY, Clinical Research Collaboration, Neurological Emergencies Treatment Trials Network, and the POINT Investigators. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA. The New England journal of medicine. 2018 Jul 19:379(3):215-225. doi: 10.1056/NEJMoa1800410. Epub 2018 May 16 [PubMed PMID: 29766750]
Pan Y, Elm JJ, Li H, Easton JD, Wang Y, Farrant M, Meng X, Kim AS, Zhao X, Meurer WJ, Liu L, Dietrich D, Wang Y, Johnston SC. Outcomes Associated With Clopidogrel-Aspirin Use in Minor Stroke or Transient Ischemic Attack: A Pooled Analysis of Clopidogrel in High-Risk Patients With Acute Non-Disabling Cerebrovascular Events (CHANCE) and Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke (POINT) Trials. JAMA neurology. 2019 Dec 1:76(12):1466-1473. doi: 10.1001/jamaneurol.2019.2531. Epub [PubMed PMID: 31424481]
Chimowitz MI, Lynn MJ, Derdeyn CP, Turan TN, Fiorella D, Lane BF, Janis LS, Lutsep HL, Barnwell SL, Waters MF, Hoh BL, Hourihane JM, Levy EI, Alexandrov AV, Harrigan MR, Chiu D, Klucznik RP, Clark JM, McDougall CG, Johnson MD, Pride GL Jr, Torbey MT, Zaidat OO, Rumboldt Z, Cloft HJ, SAMMPRIS Trial Investigators. Stenting versus aggressive medical therapy for intracranial arterial stenosis. The New England journal of medicine. 2011 Sep 15:365(11):993-1003. doi: 10.1056/NEJMoa1105335. Epub 2011 Sep 7 [PubMed PMID: 21899409]
Level 1 (high-level) evidenceSPS3 Investigators, Benavente OR, Hart RG, McClure LA, Szychowski JM, Coffey CS, Pearce LA. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. The New England journal of medicine. 2012 Aug 30:367(9):817-25. doi: 10.1056/NEJMoa1204133. Epub [PubMed PMID: 22931315]
Level 1 (high-level) evidenceJanuary CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW, ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014 Dec 2:130(23):2071-104. doi: 10.1161/CIR.0000000000000040. Epub 2014 Mar 28 [PubMed PMID: 24682348]
Level 1 (high-level) evidenceGladstone DJ, Spring M, Dorian P, Panzov V, Thorpe KE, Hall J, Vaid H, O'Donnell M, Laupacis A, Côté R, Sharma M, Blakely JA, Shuaib A, Hachinski V, Coutts SB, Sahlas DJ, Teal P, Yip S, Spence JD, Buck B, Verreault S, Casaubon LK, Penn A, Selchen D, Jin A, Howse D, Mehdiratta M, Boyle K, Aviv R, Kapral MK, Mamdani M, EMBRACE Investigators and Coordinators. Atrial fibrillation in patients with cryptogenic stroke. The New England journal of medicine. 2014 Jun 26:370(26):2467-77. doi: 10.1056/NEJMoa1311376. Epub [PubMed PMID: 24963566]
Level 1 (high-level) evidenceSanna T, Diener HC, Passman RS, Di Lazzaro V, Bernstein RA, Morillo CA, Rymer MM, Thijs V, Rogers T, Beckers F, Lindborg K, Brachmann J, CRYSTAL AF Investigators. Cryptogenic stroke and underlying atrial fibrillation. The New England journal of medicine. 2014 Jun 26:370(26):2478-86. doi: 10.1056/NEJMoa1313600. Epub [PubMed PMID: 24963567]
Level 1 (high-level) evidenceKamel H, Longstreth WT Jr, Tirschwell DL, Kronmal RA, Broderick JP, Palesch YY, Meinzer C, Dillon C, Ewing I, Spilker JA, Di Tullio MR, Hod EA, Soliman EZ, Chaturvedi S, Moy CS, Janis S, Elkind MS. The AtRial Cardiopathy and Antithrombotic Drugs In prevention After cryptogenic stroke randomized trial: Rationale and methods. International journal of stroke : official journal of the International Stroke Society. 2019 Feb:14(2):207-214. doi: 10.1177/1747493018799981. Epub 2018 Sep 10 [PubMed PMID: 30196789]
Level 1 (high-level) evidenceSaver JL, Carroll JD, Thaler DE, Smalling RW, MacDonald LA, Marks DS, Tirschwell DL, RESPECT Investigators. Long-Term Outcomes of Patent Foramen Ovale Closure or Medical Therapy after Stroke. The New England journal of medicine. 2017 Sep 14:377(11):1022-1032. doi: 10.1056/NEJMoa1610057. Epub [PubMed PMID: 28902590]
Mas JL, Derumeaux G, Guillon B, Massardier E, Hosseini H, Mechtouff L, Arquizan C, Béjot Y, Vuillier F, Detante O, Guidoux C, Canaple S, Vaduva C, Dequatre-Ponchelle N, Sibon I, Garnier P, Ferrier A, Timsit S, Robinet-Borgomano E, Sablot D, Lacour JC, Zuber M, Favrole P, Pinel JF, Apoil M, Reiner P, Lefebvre C, Guérin P, Piot C, Rossi R, Dubois-Randé JL, Eicher JC, Meneveau N, Lusson JR, Bertrand B, Schleich JM, Godart F, Thambo JB, Leborgne L, Michel P, Pierard L, Turc G, Barthelet M, Charles-Nelson A, Weimar C, Moulin T, Juliard JM, Chatellier G, CLOSE Investigators. Patent Foramen Ovale Closure or Anticoagulation vs. Antiplatelets after Stroke. The New England journal of medicine. 2017 Sep 14:377(11):1011-1021. doi: 10.1056/NEJMoa1705915. Epub [PubMed PMID: 28902593]
Amarenco P, Bogousslavsky J, Callahan A 3rd, Goldstein LB, Hennerici M, Rudolph AE, Sillesen H, Simunovic L, Szarek M, Welch KM, Zivin JA, Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. High-dose atorvastatin after stroke or transient ischemic attack. The New England journal of medicine. 2006 Aug 10:355(6):549-59 [PubMed PMID: 16899775]
Level 1 (high-level) evidenceBhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, Doyle RT Jr, Juliano RA, Jiao L, Granowitz C, Tardif JC, Ballantyne CM, REDUCE-IT Investigators. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. The New England journal of medicine. 2019 Jan 3:380(1):11-22. doi: 10.1056/NEJMoa1812792. Epub 2018 Nov 10 [PubMed PMID: 30415628]
Chollet F, Tardy J, Albucher JF, Thalamas C, Berard E, Lamy C, Bejot Y, Deltour S, Jaillard A, Niclot P, Guillon B, Moulin T, Marque P, Pariente J, Arnaud C, Loubinoux I. Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): a randomised placebo-controlled trial. The Lancet. Neurology. 2011 Feb:10(2):123-30. doi: 10.1016/S1474-4422(10)70314-8. Epub 2011 Jan 7 [PubMed PMID: 21216670]
Level 1 (high-level) evidenceSkutecki J, Audibert G, Finitsis S, Consoli A, Lapergue B, Blanc R, Bourcier R, Sibon I, Eugène F, Vannier S, Dargazanli C, Arquizan C, Anxionnat R, Richard S, Fahed R, Marnat G, Gory B, Endovascular Treatment in Ischemic Stroke (ETIS) Investigators. General anesthesia or conscious sedation for endovascular therapy of basilar artery occlusions: ETIS registry results. Revue neurologique. 2022 Oct:178(8):771-779. doi: 10.1016/j.neurol.2022.03.020. Epub 2022 Jul 20 [PubMed PMID: 35871014]
Gory B,Mazighi M,Labreuche J,Blanc R,Piotin M,Turjman F,Lapergue B, Predictors for Mortality after Mechanical Thrombectomy of Acute Basilar Artery Occlusion. Cerebrovascular diseases (Basel, Switzerland). 2018 [PubMed PMID: 29393092]
Mourand I, Mahmoudi M, Dargazanli C, Pavillard F, Arquizan C, Labreuche J, Derraz I, Gaillard N, Blanchet-Fourcade G, Lefevre PH, Boukriche Y, Gascou G, Corti L, Costalat V, Le Bars E, Cagnazzo F. DWI cerebellar infarct volume as predictor of outcomes after endovascular treatment of acute basilar artery occlusion. Journal of neurointerventional surgery. 2021 Nov:13(11):995-1001. doi: 10.1136/neurintsurg-2020-016804. Epub 2020 Nov 26 [PubMed PMID: 33243771]
Khan MT, Ikram A, Saeed O, Afridi T, Sila CA, Smith MS, Irshad K, Shuaib A. Deep Vein Thrombosis in Acute Stroke - A Systemic Review of the Literature. Cureus. 2017 Dec 23:9(12):e1982. doi: 10.7759/cureus.1982. Epub 2017 Dec 23 [PubMed PMID: 29503776]
Li B, Zhao Q, Du Y, Li X, Li Z, Meng X, Li C, Meng Z, Chen J, Liu C, Cao B, Chi S. Cerebral Blood Flow Velocity Modulation and Clinical Efficacy of Acupuncture for Posterior Circulation Infarction Vertigo: A Systematic Review and Meta-Analysis. Evidence-based complementary and alternative medicine : eCAM. 2022:2022():3740856. doi: 10.1155/2022/3740856. Epub 2022 Jun 28 [PubMed PMID: 35800002]
Level 1 (high-level) evidenceZafar A, Quadri SA, Farooqui M, Ortega-Gutiérrez S, Hariri OR, Zulfiqar M, Ikram A, Khan MA, Suriya SS, Nunez-Gonzalez JR, Posse S, Mortazavi MM, Yonas H. MRI-Guided High-Intensity Focused Ultrasound as an Emerging Therapy for Stroke: A Review. Journal of neuroimaging : official journal of the American Society of Neuroimaging. 2019 Jan:29(1):5-13. doi: 10.1111/jon.12568. Epub 2018 Oct 8 [PubMed PMID: 30295987]
Ikram A, Mohiuddin H, Zia A, Siddiqui HU, Javadikasgari H, Koprivanac M, Raza S, Zafar A. Does epiaortic ultrasound screening reduce perioperative stroke in patients undergoing coronary surgery? A topical review. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2018 Apr:50():30-34. doi: 10.1016/j.jocn.2018.01.003. Epub 2018 Feb 3 [PubMed PMID: 29398195]
Zafar A,Ikram A,Jillella DV,Kempuraj D,Khan MM,Bushnaq S,Adam H,Ortega-Gutierrez S,Quadri SA,Farooqui M,Zaheer A,Leira EC, Measurement of Elevated IL-37 Levels in Acute Ischemic Brain Injury: A Cross-sectional Pilot Study. Cureus. 2017 Oct 11; [PubMed PMID: 29234571]
Level 2 (mid-level) evidencePowers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019 Dec:50(12):e344-e418. doi: 10.1161/STR.0000000000000211. Epub 2019 Oct 30 [PubMed PMID: 31662037]