Introduction
Atheroembolic renal disease (AERD), also known as cholesterol atheroembolic renal disease, atheroembolism, cholesterol embolism, or cholesterol crystal embolization, is often an underdiagnosed clinical illness.[1][2][3] AERD is often a diagnosis of exclusion as definitive findings are rare, and clinical history often overlaps with many other conditions. However, the incidence is increasing with the increasing use of catheter-based treatment approaches and increased prevalence of risk factors. A clinical triad of an inciting event, acute or subacute renal injury, and skin findings should raise suspicion for AERD.[4][5]
Cholesterol emboli are an important cause of renal impairment. Irregularly shaped atheroemboli can cause partial or complete obstruction of small renal vessels, resulting in ischemia. A vasculitis-like picture is commonly seen with an inflammatory reaction and, ultimately, giant cell formation.[6] The relation of these emboli may be temporally found to the use of anticoagulants, vascular manipulation, or thrombolytic drug use.[7] However, spontaneous cases have also been reported. Patients who develop atheroembolic renal disease may present with a spectrum of clinical presentations of acute renal failure ranging from mild or asymptomatic to life-threatening conditions.
Atheroembolic renal disease is caused by the occlusion of the small renal arteries by cholesterol crystal emboli from ulcerated atherosclerotic plaques and is a part of systemic atheroembolism disease.[8][9] The proximity of the kidneys to the abdominal aorta and high renal blood flow makes them a frequent target of cholesterol emboli. Results from one autopsy study revealed that 74% of cases with cholesterol atheroembolic disease involved the kidneys.[6]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Atheroembolic renal disease occurs in patients with atherosclerotic vascular disease, and typically, these patients have significant atherosclerotic plaques in the aorta and large-to-medium-sized vessels. These plaques have a lipid-rich core and a thin fibrous cap. Mechanical and hemodynamic stresses can rupture the fibrous cap and release the underlying extracellular cholesterol-rich matrix, which enters circulation and eventually lodges at a distal site, causing vascular occlusion.[10]
Frequently an iatrogenic disease, AERD may follow surgical procedures like coronary artery bypass grafting, coronary stenting, abdominal aortic aneurysm repair, angiography, angioplasty, or endovascular grafting. In a small number of patients, atheroembolic renal disease may occur spontaneously without any inciting or triggering factors.[11][12][13] The release of cholesterol emboli into the circulation may occur spontaneously, post-intravascular trauma caused by angiographic catheters, or due to the use of anticoagulants and thrombolytics. Like the native kidneys, atheroembolic renal disease can also affect a transplanted kidney and must be considered when diagnosing a patient with worsening renal allograft function.[14][15][16]
The most common cause of AERD is coronary angiography with an estimated incidence of 0.06% to 1.8%. This condition can also result from hemodynamic stress, reported in up to 30% of cases.[4] A transbrachial artery approach may cause fewer renal emboli than a transfemoral, but this has not been definitively proven.[17] Cholesterol emboli can cause damage to other organs in the vascular territory of the embolic source. Extra-renal manifestations can include pancreatitis, gastric ulcers, and intestinal ischemia.[18]
There are 3 forms of atheroembolic renal disease:
- An acute form that develops a few days after the inciting event and is due to a massive embolization.
- The second type of AERD develops subacutely or in a stepwise fashion, probably due to recurrent embolization or endothelial inflammation that follows an initial ischemic insult and which results in further vessel occlusion. This is the most frequently observed form of AERD.
- A third variety presents as chronic and slowly progressive impairment of renal function and is often mistaken for nephrosclerosis or ischemic nephropathy.[19][20][21]
In the first type involving massive embolization, a rise in creatinine will be immediate. On the other hand, with subacute or chronic embolization, the rise in creatinine may occur days or weeks after the initial insult.[22]
Epidemiology
Atheroembolic renal disease occurs in patients with systemic generalized atherosclerosis. Risk factors include older age, male sex, diabetes, hypertension, hyperlipidemia, and smoking. These patients frequently have coronary artery disease, cerebrovascular disease, renal artery stenosis, renal insufficiency, aortic aneurysm, or other similar atherosclerotic diseases.[8][22]
The reported incidence ranges between 1% and 5% based on different study protocols and criteria used for diagnosis.[9][11][13][18] In older adults with atherosclerosis, atheroembolic renal disease is being increasingly seen. Results from a study found that 60% of patients with atheroembolic renal disease were older than 70.[19] The exact prevalence of atheroembolic renal disease is unknown; AERD is likely an underdiagnosed condition.[8] Clinical data is based on isolated case reports, case series, and clinicopathologic case discussions.
Pathophysiology
During surgical procedures, mechanical trauma (incision, clamping, or manipulation of the vessel) may disrupt the atherosclerotic plaques. During angiography or angioplasty, catheter manipulations disrupt the plaques, exposing the soft, cholesterol-laden core of the plaque to the arterial circulation. Anticoagulants and thrombolytic therapy prevent the formation of a protective thrombus overlying an ulcerated plaque and can also initiate disruption of a plaque by causing hemorrhage into it, therefore exposing plaques to the hemodynamic stress of circulating blood.[13] Once in circulation, cholesterol crystal emboli lodge in small arteries, 150 mm to 200 mm in diameter. These emboli cause partial occlusion of the vessel and distal ischemia, and this is followed by an inflammatory reaction, intimal proliferation, and intravascular fibrosis. The entire process results in further obliteration of the lumen and more ischemic changes.[6]
The exact mechanism underlying atheroembolic renal disease is not fully known. The local tissue necrosis and inflammatory response invoked by cholesterol crystals play a significant role. Furthermore, the renin-angiotensin-aldosterone system and complement activation also contribute to the development of atheroembolic renal disease.
Necroinflammation
Cholesterol crystals cause tissue damage directly by a mechanical obstruction, leading to vessel obstruction, tissue ischemia, and cell necrosis, which is referred to as “necroinflammation.”[23] The local inflammatory cascade initiated by cholesterol crystals plays a crucial part in luminal occlusion and consequent renal insufficiency. The cholesterol crystals set off a foreign-body inflammatory response around the arterioles, causing infiltration of the macrophages and a giant cell reaction.
Cholesterol crystals appear as an endogenous instigator of inflammation. Results from one study reported that cholesterol crystals induce activation of interleukin (IL)-1β in mononuclear phagocytes via the nucleotide-binding and oligomerization domain (NOD)-like receptor protein 3 (NLRP3) inflammasome.[24] This inflammasome is an intracellular platform for the translation of several danger signals into the activation of caspase-1 and the release of interleukin-1β. The NLRP3 inflammasome activates the macrophages to secrete mature IL-1β and α, causing cell necrosis.[25] Additionally, the cholesterol emboli induce the production of IL-α/β via the activation of PI3K and Syk in macrophages and dendritic cells.[26] Moreover, the atheroemboli directly adhere to the human macrophage-inducible C-type lectin, releasing pro-inflammatory cytokines, such as macrophage inflammatory protein 2 (MIP-2) and tumor necrosis factor (TNF).[27][6][27]
Activation of the Renin-Angiotensin-Aldosterone System
Blood pressure in patients with AERD can be difficult to control, as it activates the renin-angiotensin-aldosterone system. Obstruction of the renal vasculature by cholesterol crystals reduces focal blood perfusion and increases oxidative stress. This, in turn, leads to apoptosis, inflammation, and fibrosis.[25]
Complement Activation
Complement activation is associated with the inflammatory response secondary to atherosclerosis. Cholesterol crystals trigger both the classical and alternative complement pathways.[28][29] Emboli can activate the classical complement cascade and cause TNF release, which leads to endothelial activation in vitro.[30]
Histopathology
In the kidney, emboli typically lodge in the arcuate and interlobar arteries and are seen on light microscopy as elongated biconvex transparent needle-shaped clefts. These clefts represent the cholesterol crystals that are dissolved during tissue processing and are sometimes called "ghost cells".[22] Endothelial inflammatory response ensues and eventually leads to complete obliteration of blood flow within weeks or months.[31] Distal to the occlusion, inflammatory and necrotic changes may be present.[22] Glomeruli may appear normal in the initial stages, but eventually, there may be glomerular collapse or shrinkage. Other changes in histology may include acute tubular necrosis, interstitial fibrosis, and tubular atrophy.[31] Please see Images. Cholesterol Emboli in Glomerulus.
History and Physical
Atheroembolic renal disease is usually part of generalized atheroembolic disease, and the most commonly affected sites are the skin, lower extremity skeletal muscles, gastrointestinal tract, kidneys, and brain. Constitutional symptoms may include fever, weight loss, fatigue, or anorexia. Clinical manifestations include livedo reticularis, blue toe/purple toe syndrome, abdominal pain, and neurological deficits. Neurologic deficits may include amaurosis fugax, tia, stroke, headache, mental status changes, neuropathy, or spinal cord infarction.[6] AERD presents with acute/subacute/chronic renal failure, mild-to-moderate proteinuria, hematuria, accelerated hypertension, or new onset hypertension.[4][8][32]
If the embolic source is the ascending aorta (although a descending aortic source would be more common), Hollenhorst plaques may be visualized on the retina. See StatPearls' companion review, "Hollenhorst Plaque," for further review and imagery. Skin findings suggestive of cholesterol emboli include livedo reticularis, blue toe syndrome (painful bluish/purple discoloration), and purpura, although these findings can also be seen with vasculitis.[22][33] Changes associated with these emboli may include edema.[34]
The most common extra-renal manifestation is in the skin, with abnormalities noted in 75% to 96% of known cholesterol emboli cases. Extra-renal manifestations are possible, especially in the gastrointestinal territory, given the proximity of its vascular territory. If this is the case, manifestations such as abdominal pain, nausea, or vomiting may occur. Pancreatic infarcts can cause pancreatitis and its associated symptoms.[6][18]
Evaluation
The combination of risk factors, inciting or triggering events, acute/subacute renal failure, and signs of peripheral emboli suggest an AERD diagnosis. If these are present, the diagnosis of AERD can be made without a kidney biopsy. Renal biopsy, however, may be required in some cases to exclude processes like vasculitis, acute tubular necrosis, and allergic interstitial nephritis and may provide a definite diagnosis.
If there are skin lesions (digital infarcts, livedo reticularis), a skin biopsy may be a simple and minimally invasive way to diagnose the condition. If muscle damage is present and a specific muscle can be identified, a muscle biopsy may be another minimally invasive way to establish the diagnosis.[18] One laboratory finding suggestive of AERD is eosinophilia (present in about 80% of cases), but this may be a transitory sign.[22] Eosinophiluria, elevated C-reactive peptide, and hypocomplementemia may also occur, but these are not sensitive nor specific to AERD.[6][8][32]
Treatment / Management
There is no specific therapy for atheroembolic renal disease and treatment is mostly symptomatic and supportive. Anticoagulation should be discontinued, and the performance of more invasive diagnostic/therapeutic vascular procedures or surgery should be avoided or delayed, if possible. Treatment with aspirin and statins, smoking cessation, blood pressure control, and glycemic control are part of atherosclerosis management. Distal protection vascular devices are being used in interventional procedures to prevent embolic material from lodging in distal sites.[8]
The aim of treatment is to slow or halt the progression of ischemia of the tissues and further showering of cholesterol crystals. Avoiding nephrotoxins and limiting contrast exposure can also help decrease the incidence of AERD. Animal studies have also shown that hyperglycemia and hyperuricemia worsen cholesterol emboli-associated renal disease through different mechanisms. Renal replacement therapy may be required for supportive management if renal function does not improve.[5][35]
Corticosteroids
The purpose of corticosteroid use is to decrease the inflammatory response to atheroembolization. However, the effects of steroids remain controversial. Some studies demonstrate that the administration of oral prednisolone at a dose of 1 mg/kg/day results in overall clinical improvement and better renal outcomes.[36] However, other studies reveal that steroids do not have a significant long-term effect on renal outcomes and may even result in an increased risk of mortality.[37](B3)
Lipid-lowering Therapies
Statins may have a positive effect on AERD by contributing to the stabilization of plaque and its regression through their anti-inflammatory and lipid-lowering properties.[38](B3)
Dialysis and Other Therapies
Patients with acute kidney injury may need renal replacement therapy. Both peritoneal dialysis and hemodialysis are useful means of treating renal failure in such patients.
Differential Diagnosis
Several other entities can have similar clinical presentations.
- In contrast nephropathy, an increase in serum creatinine starts a day or two after exposure to contrast. The serum creatinine peaks in approximately one week and returns to baseline within 10 to 14 days. On the other hand, AERD frequently has a delayed onset, usually days to weeks, and a protracted course. The outcome is often poor, resulting in progressive renal failure requiring dialysis.[32]
- Systemic vasculitis is another consideration since there is multisystem involvement and complement levels can be decreased in both atheroembolic renal disease and systemic vasculitis. Serological testing, biopsy of the affected organ, or angiography may be needed to rule out this disease, since the management and outcomes of vasculitis are very different.
- Subacute bacterial endocarditis may also enter into differential diagnosis due to multisystem manifestations and low complement levels.
- Rising serum creatinine, mild-to-moderate proteinuria, hematuria, and eosinophilia may also raise the possibility of acute interstitial nephritis.[9][31]
- Chronic forms of atheroembolic renal disease may be mistaken for hypertensive nephrosclerosis or ischemic nephropathy if peripheral manifestations are subtle or missed. Renal biopsy may be crucial in these cases to make the diagnosis.[6]
Prognosis
AERD is often associated with irreversible organ damage with a poor prognosis. The renal outcome varies, with some patients requiring maintenance dialysis and others improving but with a variable degree of residual chronic renal impairment. Renal function may improve in approximately one-third of these patients after variable time without further embolic events.[8][9] Some study results show that patients with AERD have the potential to recover renal function after a longer dialysis-dependent time than other etiologies of end-stage renal disease.[13]
Around 30% to 55% of cases of acute/subacute AERD need renal replacement therapy. Improvement in renal function has been observed in only 21% to 28% of these patients.[39][40] One- and 2-year survival rates of 87% and 75%, respectively, have been reported. However, mortality is linked more to the causes of AERD than the renal disease itself.[13][41] The most common cause of mortality is cardiovascular disease.[42]
Complications
Atheroembolic disease can lead to the following complications of which providers should be aware:
- Irreversible organ damage
- End-stage renal disease
- Visceral ischemia
- Membranous nephropathy
Deterrence and Patient Education
Prevention is critical for atheroembolic renal disease, as no effective treatment is available at present. Acting in anticipation and initiating prophylaxis against further atheroembolization is useful. As it is a serious complication of many invasive vascular procedures, excess anticoagulation, surgical procedures, and angiography should be limited as much as possible, particularly in cases of known atherosclerosis. Newer noninvasive diagnostic investigations, such as spiral computed tomography, angiography, duplex ultrasonography, and geomagnetic resonance, may reduce iatrogenic AERD. Patients should be made aware of their disease and its implications for different body systems. If renal replacement is indicated, a thorough education program on the different modalities and renal transplant options, if applicable, should be implemented.
Pearls and Other Issues
Pearls and other vital information on AERD include:
- ARED is caused by the occlusion of the small renal arteries by cholesterol crystal emboli from ulcerated atherosclerotic plaques and is a part of systemic atheroembolism disease.
- AERD of often missed or misdiagnosed due to non-specific presentations and overlapping risk factors with other common renal diseases.
- A clinical triad of an inciting event, acute or subacute renal injury, and skin findings should raise suspicion for AERD.
- Common extrarenal manifestations include skin findings such as livedo reticularis, blue of purple toe syndrome, and less commonly, purpura.
- Gastrointestinal manifestations are also common and can include abdominal pain, ulcers, or pancreatitis.
- Laboratory findings may include eosinophilia, eosinophiluria, low complement levels, and elevated C-reactive protein. However, these findings are neither specific nor sensitive.
- No specific treatment exists for AERD other than mitigating risk factors such as hypertension, hyperlipidemia, hyperglycemia, and hyperuricemia.
Enhancing Healthcare Team Outcomes
Restricting the use of angiography and interventional or surgical vascular procedures in those with a high risk of atheroembolic events is imperative for the primary prevention of this disease. The use of alternate diagnostic procedures like magnetic resonance angiography or computer-assisted topographic angiography should be considered in those who have a higher risk if the alternate procedure can provide adequate information. Minimizing direct trauma of the tip of the catheter to the atheromatous wall of the vessel may also reduce the risk of atheroembolization. Further, using embolic protection devices during vascular procedures may catch the atheromatous debris and prevent migration to distal sites, thereby reducing the risk of embolization. Interprofessional coordination among surgical providers, primary care providers, nephrologists, and radiologists is key to mitigating adverse outcomes. Nurses are crucial in relaying a patient's daily clinical status to appropriate providers, pharmacists help educate patients and avoid nephrotoxins, and social workers help coordinate discharge planning and appropriate follow-up care.
A strategic approach is equally crucial, involving strategies to optimize treatment plans and minimize adverse effects. Ethical considerations must guide decision-making, ensuring informed consent and respecting patient autonomy in treatment choices and awareness of possible complications. Each healthcare professional must be aware of their responsibilities and contribute their unique expertise to the patient's care plan, fostering a multidisciplinary approach. Effective interprofessional communication is paramount, allowing seamless information exchange and collaborative decision-making among the team members. Care coordination plays a pivotal role in ensuring that the patient's journey from diagnosis to treatment and follow-up is well-managed, minimizing errors and enhancing patient safety. By embracing these principles of skill, strategy, ethics, responsibilities, interprofessional communication, and care coordination, healthcare professionals can deliver patient-centered care, ultimately improving patient outcomes and enhancing team performance in the management of renal atheroembolic disease.
Media
(Click Image to Enlarge)
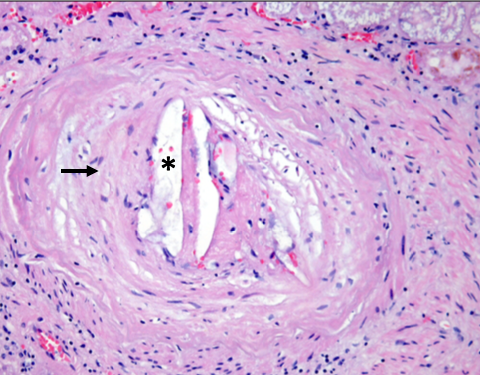
Cholesterol Emboli in the Glomerulus, Histology, H&E. Artery showing atheroembolus with cholesterol clefts embedded within prominent intimal fibrosis (arrow), hematoxylin & eosin stain.
Seker P. Kidney biopsy of the month: atheroembolic kidney disease. Renal Fellow Network Web site. https://www.renalfellow.org/2020/02/14/kidney-biopsy-of-the-month-atheroembolic-kidney-disease/. Published February 14, 2020. Accessed June 16, 2024.
(Click Image to Enlarge)
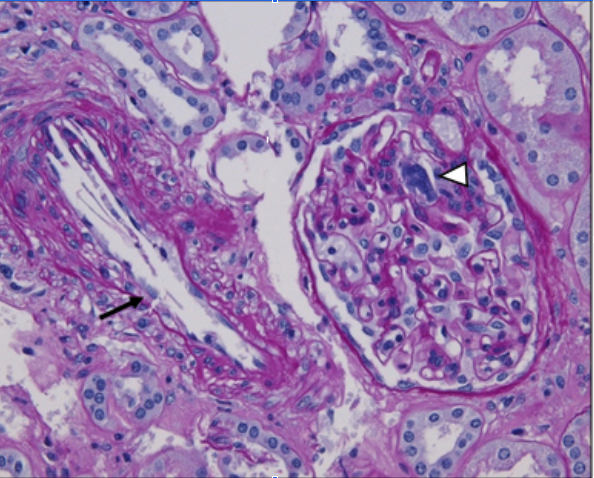
Cholesterol Emboli in the Glomerulus, Histology, PAS. Large atheroembolus occluding the renal artery (black arrow) and a glomerulus showing a cholesterol cleft (white arrowhead), Periodic acid-Schiff.
Seker P. Kidney biopsy of the month: atheroembolic kidney disease. Renal Fellow Network Web site. https://www.renalfellow.org/2020/02/14/kidney-biopsy-of-the-month-atheroembolic-kidney-disease/. Published February 14, 2020. Accessed June 16, 2024.
References
Carvajal JA, Anderson WR, Weiss L, Grismer J, Berman R. Atheroembolism. An etiologic factor in renal insufficiency, gastrointestinal hemorrhages, and peripheral vascular diseases. Archives of internal medicine. 1967 Jun:119(6):593-9 [PubMed PMID: 5298059]
Darsee JR. Cholesterol embolism: the great masquerader. Southern medical journal. 1979 Feb:72(2):174-80 [PubMed PMID: 371003]
Cappiello RA, Espinoza LR, Adelman H, Aguilar J, Vasey FB, Germain BF. Cholesterol embolism: a pseudovasculitic syndrome. Seminars in arthritis and rheumatism. 1989 May:18(4):240-6 [PubMed PMID: 2727705]
Level 3 (low-level) evidenceȘtefan G, Zugravu A, Stancu S, Gherghiceanu M, Terinte-Balcan G. Atheroembolic kidney disease: The under-recognized silent killer. Clinical case reports. 2021 Mar:9(3):1824-1825. doi: 10.1002/ccr3.3874. Epub 2021 Jan 28 [PubMed PMID: 33768956]
Level 3 (low-level) evidenceChaudhary S, Kashani KB. Acute Kidney Injury Management Strategies Peri-Cardiovascular Interventions. Interventional cardiology clinics. 2023 Oct:12(4):555-572. doi: 10.1016/j.iccl.2023.06.008. Epub 2023 Aug 5 [PubMed PMID: 37673499]
Li X, Bayliss G, Zhuang S. Cholesterol Crystal Embolism and Chronic Kidney Disease. International journal of molecular sciences. 2017 May 24:18(6):. doi: 10.3390/ijms18061120. Epub 2017 May 24 [PubMed PMID: 28538699]
Vassalotti JA, Delgado FA, Whelton A. Atheroembolic Renal Disease. American journal of therapeutics. 1996 Jul:3(7):544-549 [PubMed PMID: 11862288]
Scolari F, Ravani P. Atheroembolic renal disease. Lancet (London, England). 2010 May 8:375(9726):1650-60. doi: 10.1016/S0140-6736(09)62073-0. Epub 2010 Apr 8 [PubMed PMID: 20381857]
Mittal BV, Alexander MP, Rennke HG, Singh AK. Atheroembolic renal disease: a silent masquerader. Kidney international. 2008 Jan:73(1):126-30 [PubMed PMID: 17667989]
Kronzon I, Saric M. Cholesterol embolization syndrome. Circulation. 2010 Aug 10:122(6):631-41. doi: 10.1161/CIRCULATIONAHA.109.886465. Epub [PubMed PMID: 20697039]
Fukumoto Y, Tsutsui H, Tsuchihashi M, Masumoto A, Takeshita A, Cholesterol Embolism Study(CHEST) Investigators. The incidence and risk factors of cholesterol embolization syndrome, a complication of cardiac catheterization: a prospective study. Journal of the American College of Cardiology. 2003 Jul 16:42(2):211-6 [PubMed PMID: 12875753]
Modi KS, Rao VK. Atheroembolic renal disease. Journal of the American Society of Nephrology : JASN. 2001 Aug:12(8):1781-1787. doi: 10.1681/ASN.V1281781. Epub [PubMed PMID: 11461954]
Level 3 (low-level) evidenceScott T, Ethier I, Hawley C, Pascoe EM, Viecelli AK, Ng A, Cho Y, Johnson DW. Burden of kidney failure from atheroembolic disease and association with survival in people receiving dialysis in Australia and New Zealand: a multi-centre registry study. BMC nephrology. 2021 Dec 2:22(1):401. doi: 10.1186/s12882-021-02604-7. Epub 2021 Dec 2 [PubMed PMID: 34856938]
Pirson Y, Honhon B, Cosyns JP, van Ypersele C. Cholesterol embolism in a renal graft after treatment with streptokinase. British medical journal (Clinical research ed.). 1988 Feb 6:296(6619):394-5 [PubMed PMID: 3125916]
Level 3 (low-level) evidenceSingh I, Killen PD, Leichtman AB. Cholesterol emboli presenting as acute allograft dysfunction after renal transplantation. Journal of the American Society of Nephrology : JASN. 1995 Aug:6(2):165-70 [PubMed PMID: 7579080]
Level 3 (low-level) evidenceRipple MG, Charney D, Nadasdy T. Cholesterol embolization in renal allografts. Transplantation. 2000 May 27:69(10):2221-5 [PubMed PMID: 10852632]
Level 3 (low-level) evidenceRudnick MR, Berns JS, Cohen RM, Goldfarb S. Nephrotoxic risks of renal angiography: contrast media-associated nephrotoxicity and atheroembolism--a critical review. American journal of kidney diseases : the official journal of the National Kidney Foundation. 1994 Oct:24(4):713-27 [PubMed PMID: 7942832]
Yamamoto N, Sakai N, Kaikoi D, Yomogida D, Kajikawa S, Wada T, Yuasa T, Ogura H, Sato K, Miyagawa T, Kitajima S, Toyama T, Hara A, Shimizu M, Wada T, Iwata Y. Cholesterol Crystal Embolism: Autopsy-proven Gastrointestinal Lesions, Pancreatitis, and End-stage Kidney Disease Which Developed after Undergoing Selective Abdominal Angiography. Internal medicine (Tokyo, Japan). 2024 May 9:():. doi: 10.2169/internalmedicine.3469-24. Epub 2024 May 9 [PubMed PMID: 38719599]
Scolari F, Ravani P, Gaggi R, Santostefano M, Rollino C, Stabellini N, Colla L, Viola BF, Maiorca P, Venturelli C, Bonardelli S, Faggiano P, Barrett BJ. The challenge of diagnosing atheroembolic renal disease: clinical features and prognostic factors. Circulation. 2007 Jul 17:116(3):298-304 [PubMed PMID: 17606842]
Level 2 (mid-level) evidenceScolari F, Tardanico R, Zani R, Pola A, Viola BF, Movilli E, Maiorca R. Cholesterol crystal embolism: A recognizable cause of renal disease. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2000 Dec:36(6):1089-109 [PubMed PMID: 11096032]
Polu KR, Wolf M. Clinical problem-solving. Needle in a haystack. The New England journal of medicine. 2006 Jan 5:354(1):68-73 [PubMed PMID: 16394304]
Level 3 (low-level) evidencePiranavan P, Rajan A, Jindal V, Verma A. A rare presentation of spontaneous atheroembolic renal disease: A case report. World journal of nephrology. 2019 Jun 28:8(3):67-74. doi: 10.5527/wjn.v8.i3.67. Epub 2019 Jun 10 [PubMed PMID: 31363463]
Level 3 (low-level) evidenceMulay SR, Anders H-J. Crystallopathies. The New England journal of medicine. 2016 Sep 29:375(13):e29. doi: 10.1056/NEJMc1609332. Epub [PubMed PMID: 27682056]
Martinon F, Pétrilli V, Mayor A, Tardivel A, Tschopp J. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. 2006 Mar 9:440(7081):237-41 [PubMed PMID: 16407889]
Level 3 (low-level) evidenceDuewell P, Kono H, Rayner KJ, Sirois CM, Vladimer G, Bauernfeind FG, Abela GS, Franchi L, Nuñez G, Schnurr M, Espevik T, Lien E, Fitzgerald KA, Rock KL, Moore KJ, Wright SD, Hornung V, Latz E. NLRP3 inflammasomes are required for atherogenesis and activated by cholesterol crystals. Nature. 2010 Apr 29:464(7293):1357-61. doi: 10.1038/nature08938. Epub [PubMed PMID: 20428172]
Level 3 (low-level) evidenceCorr EM, Cunningham CC, Dunne A. Cholesterol crystals activate Syk and PI3 kinase in human macrophages and dendritic cells. Atherosclerosis. 2016 Aug:251():197-205. doi: 10.1016/j.atherosclerosis.2016.06.035. Epub 2016 Jun 22 [PubMed PMID: 27356299]
Kiyotake R, Oh-Hora M, Ishikawa E, Miyamoto T, Ishibashi T, Yamasaki S. Human Mincle Binds to Cholesterol Crystals and Triggers Innate Immune Responses. The Journal of biological chemistry. 2015 Oct 16:290(42):25322-32. doi: 10.1074/jbc.M115.645234. Epub 2015 Aug 20 [PubMed PMID: 26296894]
Samstad EO, Niyonzima N, Nymo S, Aune MH, Ryan L, Bakke SS, Lappegård KT, Brekke OL, Lambris JD, Damås JK, Latz E, Mollnes TE, Espevik T. Cholesterol crystals induce complement-dependent inflammasome activation and cytokine release. Journal of immunology (Baltimore, Md. : 1950). 2014 Mar 15:192(6):2837-45. doi: 10.4049/jimmunol.1302484. Epub 2014 Feb 19 [PubMed PMID: 24554772]
Niyonzima N, Samstad EO, Aune MH, Ryan L, Bakke SS, Rokstad AM, Wright SD, Damås JK, Mollnes TE, Latz E, Espevik T. Reconstituted High-Density Lipoprotein Attenuates Cholesterol Crystal-Induced Inflammatory Responses by Reducing Complement Activation. Journal of immunology (Baltimore, Md. : 1950). 2015 Jul 1:195(1):257-64. doi: 10.4049/jimmunol.1403044. Epub 2015 May 29 [PubMed PMID: 26026058]
Nymo S, Niyonzima N, Espevik T, Mollnes TE. Cholesterol crystal-induced endothelial cell activation is complement-dependent and mediated by TNF. Immunobiology. 2014 Oct:219(10):786-92. doi: 10.1016/j.imbio.2014.06.006. Epub 2014 Jul 5 [PubMed PMID: 25053140]
Scoble JE, O'Donnell PJ. Renal atheroembolic disease: the Cinderella of nephrology? Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 1996 Aug:11(8):1516-7 [PubMed PMID: 8856200]
Nasri H, Mubarak M. Contrast induced nephropathy has to be differentiated from kidney injury due to atheroembolic disease. Journal of renal injury prevention. 2013:2(3):107-8. doi: 10.12861/jrip.2013.34. Epub 2013 Sep 1 [PubMed PMID: 25340143]
Level 3 (low-level) evidenceSakan H, Nakatani K, Asai O, Matsui M, Iwano M, Saito Y. [Case of purpura nephritis accompanied by idiopathic cholesterol embolism]. Nihon Jinzo Gakkai shi. 2012:54(5):622-8 [PubMed PMID: 22991843]
Level 3 (low-level) evidenceChu JK, Folkert VW. Renal function recovery in chronic dialysis patients. Seminars in dialysis. 2010 Nov-Dec:23(6):606-13. doi: 10.1111/j.1525-139X.2010.00769.x. Epub 2010 Dec 20 [PubMed PMID: 21166875]
Yang L, Steiger S, Shi C, Gudermann T, Mammadova-Bach E, Braun A, Anders HJ. Both hyperglycemia and hyperuricemia aggravate acute kidney injury during cholesterol embolism syndrome despite opposite effects on kidney infarct size. Kidney international. 2023 Jul:104(1):139-150. doi: 10.1016/j.kint.2023.03.016. Epub 2023 Mar 30 [PubMed PMID: 37001603]
Desai M, Ram R, Prayaga A, Dakshinamurty KV. Cholesterol crystal embolization (CCE): Improvement of renal function with high-dose corticosteroid treatment. Saudi journal of kidney diseases and transplantation : an official publication of the Saudi Center for Organ Transplantation, Saudi Arabia. 2011 Mar:22(2):327-30 [PubMed PMID: 21422636]
Level 3 (low-level) evidenceKronzon I, Tunick PA. Aortic atherosclerotic disease and stroke. Circulation. 2006 Jul 4:114(1):63-75 [PubMed PMID: 16818829]
Abela GS, Vedre A, Janoudi A, Huang R, Durga S, Tamhane U. Effect of statins on cholesterol crystallization and atherosclerotic plaque stabilization. The American journal of cardiology. 2011 Jun 15:107(12):1710-7. doi: 10.1016/j.amjcard.2011.02.336. Epub 2011 Apr 18 [PubMed PMID: 21507364]
Level 3 (low-level) evidenceThériault J, Agharazzi M, Dumont M, Pichette V, Ouimet D, Leblanc M. Atheroembolic renal failure requiring dialysis: potential for renal recovery? A review of 43 cases. Nephron. Clinical practice. 2003:94(1):c11-8 [PubMed PMID: 12806187]
Level 3 (low-level) evidenceScolari F, Ravani P, Pola A, Guerini S, Zubani R, Movilli E, Savoldi S, Malberti F, Maiorca R. Predictors of renal and patient outcomes in atheroembolic renal disease: a prospective study. Journal of the American Society of Nephrology : JASN. 2003 Jun:14(6):1584-90 [PubMed PMID: 12761259]
Level 2 (mid-level) evidenceFaria B, Vidinha J, Pêgo C, Garrido J, Lemos S, Lima C, Sorbo G, Gomes EL, Carvalho T, Loureiro P, Sousa T. Atheroembolic renal disease with rapid progression and fatal outcome. Clinical and experimental nephrology. 2011 Feb:15(1):159-63. doi: 10.1007/s10157-010-0363-3. Epub 2010 Nov 11 [PubMed PMID: 21069411]
Level 3 (low-level) evidenceFrank RD. [Cholesterol embolism syndrome: a rare, but severe complication in patients with atherosclerosis]. Deutsche medizinische Wochenschrift (1946). 2012 May:137(21):1130-4. doi: 10.1055/s-0032-1305005. Epub 2012 May 15 [PubMed PMID: 22588660]