Introduction
The Ashman phenomenon, first described by James Gouaux and Richard Ashman in 1947, is an electrocardiogram (ECG) finding characterized by a wide QRS complex following a premature supraventricular activation and a longer preceding cycle.[1] This ECG finding does not generally impact mortality or morbidity apart from correcting a misinterpretation of the wide beats and premature ventricular complexes (PVCs).
Ashman phenomenon is often misinterpreted as a PVC due to its appearance on the ECG. This abnormality is frequently associated with atrial fibrillation and other supraventricular arrhythmias but does not typically cause symptoms itself. The Ashman phenomenon results in 1 or more wide QRS aberrant complexes following specific short-long or long-short R-R cardiac cycle patterns. Clinically, the Ashman phenomenon is asymptomatic, but patients may experience symptoms related to the underlying cardiac condition, which, in many cases, is atrial fibrillation.[2] The wider Ashman beat may be a weaker beat due to the reduction in contractile coordination. Still, it occurs in conjunction with a short cycle, which is an already weaker heartbeat due to less ventricular filling. Management involves addressing the underlying arrhythmia and associated conditions rather than the phenomenon itself.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The term Ashman phenomenon or Ashman beat is used when describing a particular occurrence on an ECG, which is defined as a wide QRS complex that follows a short R-R interval preceded by a long R-R interval. The QRS complex originates above the AV node and not within the right or left ventricle, usually as a partial or complete right bundle branch block (RBBB).[3] This occurs because the refractory period of the conduction system increases with the length of the prior R-R interval.[4]
A shorter R-R cardiac cycle induces a shorter refractory recovery period, and a longer R-R induces a longer recovery period. With a longer R-R cycle, there is an increase in the refractory period; if a subsequent short R-R triggers ventricular activation during the relative refractory period before the conduction system has recovered sufficiently to conduct normally, the conduction will be aberrant.[5] Since the refractory period of the right bundle branch is longer than the left bundle branch block, a right bundle branch block pattern is more common, but a left bundle branch pattern can still be observed, albeit less frequently. Additionally, an RBBB pattern can be associated with a left fascicular block.[6] (See Image. Atrial Fibrillation With a Wide QRS Complex).
Additionally, the degree of aberrant conduction may vary from beat to beat and patient to patient. While a right bundle branch block pattern is more common, a left bundle block pattern or combined block pattern may sometimes be observed in the same patient. In situations where both LBBB and RBBB are noted, the patient likely has an underlying conduction defect.[7]
Epidemiology
Data on the geographic differences noted with the Ashman phenomenon have not been reported. Ashman phenomenon is linked to the underlying pathology of the cardiac conduction system and thus is nearly always associated with a conduction irregularity. Ashman beat is a common ECG finding in clinical practice that is frequently misinterpreted.[8]
Pathophysiology
Ashman phenomenon has most widely been associated with atrial fibrillation, which has been noted to occur secondary to the chaotic impulses from the atrium. These chaotic impulses cause variability in the R-R cycle length, allowing aberrant conduction.[7] The Ashman beat is caused by inconsistency in R-R intervals. The refractory period of the cardiac conduction system (His-Purkinje system) depends on the preceding cycle length. Thus, a longer R-R interval is followed by a longer refractory period, while a shorter R-R interval is followed by a shorter refractory period.[9]
In the Ashman phenomenon, an elongated R-R interval followed by a shorter R-R interval is seen. As mentioned earlier, the longer R-R interval stretches the refractory period of the His-Purkinje system. If a shorter R-R interval follows that long interval, the cardiac conduction system may be found in the refractory period.[5] This electrical abnormality is often observed as a block on ECG; a right bundle branch block pattern is noted frequently as the right bundle branch has a relatively longer refractory period.[10]
History and Physical
Clinically, the Ashman phenomenon is asymptomatic. However, a patient may experience palpitations, shortness of breath, or lightheadedness due to an underlying baseline arrhythmia such as atrial fibrillation or supraventricular tachycardia. However, this is not due to the PVC itself, which is conducted with an aberration. An irregularly irregular rhythm is found on examination if associated with atrial fibrillation. Ashman phenomenon is a benign ECG finding commonly observed in atrial fibrillation due to variability in the R-R interval, atrial tachycardia, and atrial ectopy.[11]
Evaluation
Electrocardiography Evaluation
The workup would include a history, clinical examination, and a detailed evaluation of 12-lead electrocardiography during sinus rhythm and comparing it with the presenting ECG. In essence, evaluating the Ashman phenomenon involves understanding its context, like atrial fibrillation, excluding differential diagnoses, and addressing any underlying cardiac conditions. Tailoring the investigation and management to the individual patient is crucial for optimal outcomes.[12]
A clinician can diagnose the Ashman phenomenon using the Fisch criteria:
- Relatively long cycle immediately preceding the cycle terminated by the aberrant QRS complex
- A consistent pattern of a relatively long preceding R-R cycle immediately ahead of the short R-R cycle results in a wide QRS complex.
- A short-long-short interval is even more likely to initiate aberration
- Finding an example of a shorter-longer-shorter R-R cycle pattern with less QRS width is contrary to the Ashman phenomenon, and that would argue for other causes of at least some of the wide complexes.
- RBBB-form aberrancy with the normal orientation of the initial QRS vector (a series of wide QRS supraventricular beats is possible)
- The aberration is usually RBBB morphology with a normal initial force because the right bundle normally has the longest recovery time after a long preceding cycle length. However, the wide complex could be either LBBB or RBBB or a combination, and different patterns may be noticed even in the same patient.
- Concealed propagation is possible, such that a series of wide QRS supraventricular beats may occur.
- Irregular coupling of aberrant QRS complexes
- Irregular coupling of aberrant QRS complexes is common with Ashman phenomena and uncommon with PVCs, which typically have a fixed coupling interval between the preceding QRS and the wide premature QRS.
- Lack of fully compensatory pause
- The absence of a full compensatory pause is common in the Ashman phenomenon, even with a regular underlying rhythm. In contrast, a PVC in a regular underlying rhythm typically blocks the presentation of a supraventricular beat without resetting the supraventricular pacing source, so then the next narrow beat occurs at double the normal R-R interval, known as a "compensatory pause."[6][8][13]
Premature Ventricular Complexes and Ashman Phenomenon
The Ashman phenomenon is often confused with PVCs due to their similar appearance on ECG.[11] However, differentiating between PVCs and the Ashman phenomenon is crucial, as they have different clinical implications. While the Ashman phenomenon and PVCs can have a widened QRS, subtle differences can be noted. Regular coupling to a widened QRS complex would support the diagnosis of PVCs versus the Ashman phenomenon. Also, if the clinician observes a full compensatory pause, a ventricular origin of the noted beat is suggested. However, the lack of a compensatory pause favors aberrancy.[7] A long rhythm sequence should be reviewed to compare R-R sequences that lead to each wide complex and to assess that all wide complexes are consistent with the Ashman phenomenon. If a shorter-longer-shorter sequence does not result in the observed widening, that would be inconsistent with the Ashman phenomenon. In summary, QRS morphology is the most crucial clue when distinguishing between a supraventricular or ventricular origin of wide QRS complexes.
Treatment / Management
Management of the Ashman phenomenon primarily involves addressing the underlying arrhythmia and associated conditions rather than the phenomenon itself. Proper control of atrial arrhythmias while monitoring and managing associated cardiac conditions is crucial for ensuring effective treatment and improving patient outcomes.[8](B3)
Differential Diagnosis
The following differentials should be considered before confirming the diagnosis of the Ashman phenomenon:
- The baseline right bundle branch should be excluded before diagnosing the Ashman phenomenon.
- PVCs during atrial fibrillation or supraventricular arrhythmias usually do not present as a typical bundle branch block and are followed by a compensatory pause.[13][14]
- Intermittent preexcitation during supraventricular tachycardia can be identified by manifest ventricular preexcitation in delta waves.
- Artifacts due to movement or poor electrode contact can sometimes cause misleading QRS changes that could be mistaken for the Ashman phenomenon.[15][16]
In clinical practice, distinguishing the Ashman phenomenon from these differentials typically involves careful analysis of the ECG, including looking at the baseline ECG, QRS morphology during sinus rhythm and tachycardia, and the context of the heart rate.
Prognosis
Ashman phenomenon is a benign condition with no known impact on the mortality or morbidity of a patient.
Complications
No complications associated with the Ashman phenomenon have been described in the literature.
Consultations
A consultation with a cardiologist or electrophysiologist may be needed to help identify and treat the underlying rhythm.
Deterrence and Patient Education
Patients who feel palpitations, chest pain, shortness of breath, dizziness, or syncope should be promptly evaluated. While not a common presentation of the Ashman phenomenon, these symptoms could suggest a more serious underlying condition, eg, atrial fibrillation or other arrhythmias.
Enhancing Healthcare Team Outcomes
Identifying and managing the Ashman phenomenon as a benign, incidental ECG finding necessitates a multifaceted approach involving various healthcare professionals. Clinicians, including cardiologists and cardiac electrophysiologists, advanced clinicians, nurses, pharmacists, and other healthcare professionals, play critical roles in recognizing this electrocardiographic manifestation skillfully. This requires a comprehensive understanding of the specific ECG characteristics associated with the Ashman phenomenon, such as the wide QRS complex of right bundle branch morphology following specific R-R intervals.
Interprofessional communication and care coordination among the healthcare team are paramount to enhancing patient-centered care and overall outcomes. Effective communication and collaboration among healthcare professionals are essential to ensure accurate identification of the Ashman phenomenon, differentiating it from similar ECG abnormalities, including premature ventricular complex and ventricular preexcitation due to an accessory pathway. This often requires consultations with cardiologists and cardiac electrophysiologists to collectively develop and implement optimal management strategies. This interprofessional approach, encompassing diverse skills, strategic communication, shared responsibilities, and care coordination, is fundamental to advancing patient-centered care, minimizing unnecessary investigations and interventions, ensuring patient safety, and optimizing overall clinical outcomes related to the Ashman phenomenon.
Media
(Click Image to Enlarge)
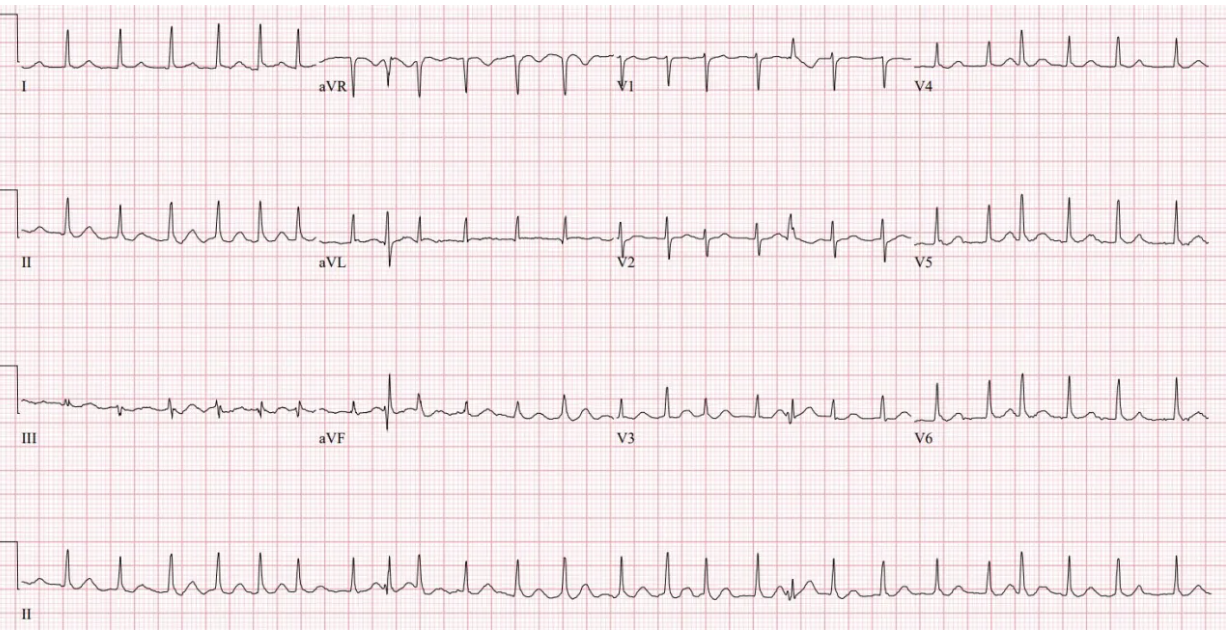
Atrial Fibrillation Wide QRS Complex. The short R-R interval following a longer R-R interval results in a right bundle branch aberrancy, consistent with the Ashman phenomenon.
Contributed by I Ahmed, MD
References
GOUAUX JL, ASHMAN R. Auricular fibrillation with aberration simulating ventricular paroxysmal tachycardia. American heart journal. 1947 Sep:34(3):366-73 [PubMed PMID: 20262631]
Costantini M, Crema A. [The electrocardiology of atrial fibrillation]. Italian heart journal. Supplement : official journal of the Italian Federation of Cardiology. 2000 May:1(5):632-40 [PubMed PMID: 10834128]
Bagliani G, De Ponti R, Gianni C, Padeletti L. The QRS Complex: Normal Activation of the Ventricles. Cardiac electrophysiology clinics. 2017 Sep:9(3):453-460. doi: 10.1016/j.ccep.2017.05.005. Epub 2017 Jun 27 [PubMed PMID: 28838550]
Lee CH, Shafi A, Scheinman MM. Beat-to-beat QRS alternans. Heart rhythm. 2023 Nov:20(11):1586-1588. doi: 10.1016/j.hrthm.2023.03.1524. Epub [PubMed PMID: 37914496]
Singla V, Singh B, Singh Y, Manjunath CN. Ashman phenomenon: a physiological aberration. BMJ case reports. 2013 May 24:2013():. doi: 10.1136/bcr-2013-009660. Epub 2013 May 24 [PubMed PMID: 23709552]
Level 3 (low-level) evidenceFisch C. Electrocardiography of arrhythmias: from deductive analysis to laboratory confirmation--twenty-five years of progress. Journal of the American College of Cardiology. 1983 Jan:1(1):306-16 [PubMed PMID: 6826940]
Longo D, Baranchuk A. Ashman phenomenon dynamicity during atrial fibrillation: the critical role of the long cycles. Journal of atrial fibrillation. 2017 Oct-Nov:10(3):1656. doi: 10.4022/jafib.1656. Epub 2017 Oct 31 [PubMed PMID: 29250245]
Lakusić N, Mahović D, Slivnjak V. Ashman phenomenon: an often unrecognized entity in daily clinical practice. Acta clinica Croatica. 2010 Mar:49(1):99-100 [PubMed PMID: 20635592]
Level 3 (low-level) evidenceKara M, Korkmaz A, Deveci B, Cimen T, Ozeke O, Cay S, Ozcan F, Topaloglu S, Aras D. The transition of the tachycardia from narrow to wide by a spontaneous atrial premature beat: What is the mechanism? Journal of arrhythmia. 2021 Apr:37(2):462-463. doi: 10.1002/joa3.12499. Epub 2021 Jan 29 [PubMed PMID: 33850594]
Spodick DH. Electrocardiology teacher analysis and review. 4:3 atrioventricular Wenckebach exit block with (probable) Ashman phenomenon during junctional tachycardia. The American journal of geriatric cardiology. 2004 Sep-Oct:13(5):285 [PubMed PMID: 15365295]
Level 3 (low-level) evidenceKennedy LB, Leefe W, Leslie BR. The Ashman phenomenon. The Journal of the Louisiana State Medical Society : official organ of the Louisiana State Medical Society. 2004 May-Jun:156(3):159-62 [PubMed PMID: 15233390]
Kang PW, Wong KE, Smith TW. Aberrant QRS morphologies during atrial tachycardia: What is the mechanism? Heart rhythm. 2023 Jul:20(7):1061-1063. doi: 10.1016/j.hrthm.2023.01.036. Epub 2023 Feb 4 [PubMed PMID: 36739956]
Fisch C. Aberration: seventy five years after Sir Thomas Lewis. British heart journal. 1983 Oct:50(4):297-302 [PubMed PMID: 6626389]
Early E. Ashman's phenomenon vs ventricular ectopy. Critical care nurse. 1988 May:8(3):30-2 [PubMed PMID: 3383590]
Smith DC. Ashman's phenomenon--a source of nonsustained wide complex tachycardia. The Journal of emergency medicine. 1993 Jan-Feb:11(1):98 [PubMed PMID: 8445196]
Morton MB,Morton JB,Mond HG, Aberrant Ventricular Conduction: Revisiting an Old Concept. Heart, lung [PubMed PMID: 36967303]