
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by inflammatory arthritis and extra-articular involvement. It is a chronic inflammatory disorder caused in many cases by the interaction between genes and environmental factors, including tobacco, that primarily involves synovial joints.[1] It typically starts in small peripheral joints, is usually symmetric, and progresses to involve proximal joints if left untreated.[2][3][4] Joint inflammation over time leads to the destruction of the joint with loss of cartilage and bone erosions. RA with a symptom duration of fewer than six months is defined as early RA, and when the symptoms have been present for more than six months, it is defined as established RA.[3] RA, if untreated, is a progressive disease with morbidity and increased mortality.[5]
There is no pathognomonic laboratory test for rheumatoid arthritis, which makes the diagnosis of this disease challenging in the early stages. A comprehensive clinical approach is required to make the diagnosis and prevent debilitating joint damage.[2][3] The treatment of patients with rheumatoid arthritis requires both pharmacological and non-pharmacological therapy. Today, the standard of care is early treatment with disease-modifying anti-rheumatic drugs. Despite treatment, many patients progress to disability and suffer significant morbidity over time. A comprehensive pharmacological and non-pharmacological treatment (physical therapy, counseling, and patient education) is required to improve clinical outcomes.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of RA has a significant basis in genetics. It is thought to result from the interaction between patients' genotypes and environmental factors. In a nationwide study of 91 monozygotic (MZ) and 112 dizygotic (DZ) twin pairs in the United Kingdom, the overall MZ concordance rate was 15%, and in dizygotic twins, 5%.[6] The heritability of rheumatoid arthritis is approximately 40% to 65% for seropositive rheumatoid arthritis and 20% for seronegative rheumatoid arthritis.[7] The risk of developing rheumatoid arthritis has been associated with HLA-DRB1 alleles: HLA-DRB1*04, HLA-DRB1*01, and HLA-DRB1*10. These HLA-DRB1 alleles contain a stretch of a conserved sequence of 5 amino acids referred to as the "shared epitope" (SE) in the third hypervariable region of their DRB1 chain, which has been associated with the risk of developing RA.[8][9][10][11]
Polymorphisms in other genes are associated with RA, including PAD14, PTPN22, CTLA4, IL-2RA, STAT4, TRAF1, CCR6, and IRF5.[12][13][14] Single nucleotide polymorphism (SNP) in PSORS1C1, PTPN22, and MIR146A genes are associated with severe disease.[15] Some genetic polymorphisms are associated with RA in different ethnic groups.[13][15]
The term epigenetics refers to heritable changes without altering the DNA sequence. These changes may be present in chromatin or the DNA. These include DNA methylation, histone modification, and non-coding RNA-mediated regulation. RA-FLS (fibroblast-like synoviocytes) overexpress tyrosine phosphatase SHP-2, coded by gene PTPN11, compared to synoviocytes from osteoarthritis (OA) patients, promoting the invasive nature of RA-FLS. The enhancer region of the PTPN11 intron contained two hypermethylated sites, resulting in abnormal epigenetic regulation of the gene and alteration of the function of RA-FLS.[16]
Cigarette smoking is the strongest environmental risk factor associated with rheumatoid arthritis. Studies have shown in anti-citrullinated protein antibody (anti-CCP) positive individuals, there is an interaction between the shared epitope (SE) and smoking that increases the risk of RA.[17][18][19][20][21][22][23]
Other environmental triggers may play a role as a trigger for RA, which is more closely associated with seropositive RA. These include silica, asbestos, textile dust, and P gingivalis.[1] This suggests that external exposure to various antigens in parts of the host distant from the joints then triggers an autoimmune inflammatory response in the joints. These distant locations include the lungs, oropharynx, and GI tract.[1] Changes in the composition and function of the intestinal microbiome have been related to rheumatoid arthritis as well. The composition of the gut microbiome becomes altered in patients with rheumatoid arthritis (dysbiosis), where rheumatoid arthritis patients have decreased gut microbiome diversity compared with healthy individuals. There is an increase in these genera: Actinobacteria, Collinsella, Eggerthalla, and Faecalibacterium. Collinsella alters gut mucosal permeability and has been related to increased rheumatoid arthritis disease severity.[23]
Genes Associated with Increased Risk of RA[12][13]
Gene Gene product
| HLA-DRB1 | HLA Class II BRB1 beta chain: antigen presentation |
| PADI4 | Peptidyl Arginine Deiminase 4: an enzyme that converts arginine to citrulline |
| PTPN22 | Protein Tyrosine Phosphatase Non-Receptor Type 22: non-receptor class 4 subfamily of the protein-tyrosine phosphatase family involved in T cell signaling, a negative regulator of T cell receptor signaling. |
| CTLA4 | Cytotoxic T-Lymphocyte Associated Protein 4: engagement of this surface protein transmits an inhibitory signal to T cells |
| IL2RA | Interleukin 2 Receptor Subunit Alpha: part of the IL2 receptor protein involved in T cell activation (and also other lymphoid cells) |
| STAT4 | Signal Transducer And Activator Of Transcription 4: a member of the STAT family of transcription factors involved in signal transduction of INF-gamma and IL-12 stimulation |
| TRAF1 | TNF Receptor Associated Factor 1: TRAF proteins associate with and mediate the signal transduction from various receptors of the TNFR |
| CCR6 | C-C Motif Chemokine Receptor 6: a member of the beta chemokine receptor family, important in B cell maturation |
| IRF5 | Interferon Regulatory Factor 5: a member of the interferon regulatory factor (IRF) family of transcription factors involved in type 1 interferon signal transduction |
Environmental Factors Associated with an Increased Risk of Developing RA[1]
| Exposure | RA overall | Seropositive RA | Seronegative RA |
| Smoking | + | + | +/- |
| Silica | + | + | +/- |
| Asbestos | + | + | + |
| Textile dust | + | + | + |
| P. gingivalis | + | + | ? |
Epidemiology
The worldwide prevalence of RA in the Global Burden of Disease 2010 Study is about 0.24%.[24] The prevalence of RA is higher in Western and Northern Europe, North America, and other regions with people of European descent, such as Australia. The prevalence is lower in Central and South America and even lower in East Asia and Africa.[24] The annual incidence of RA in the United States and other western nations of northern Europe is about 40 per 100,000 persons.[25] According to epidemiologic data, RA is more prevalent in women compared to men, with a lifetime risk of RA of 3.6% in women compared to 1.7% in men.[26] RA risk also increases with age, with a peak incidence between age 65 to 80 years of age.[27][28][27] A systematic review of population-based studies (including 60 studies) showed a worldwide period prevalence of RA of 0.51% (1955-2015).[29]
The period prevalence of RA was more in urban areas (0.69%) than in rural areas (0.54%). The period prevalence of RA was higher in high-income countries (0.49%) compared to low-income countries (0.35.%).[30] RA prevalence was higher in North America and Europe and lower in Asia and South America (See Table below).[29] Data from Africa is limited and varies significantly by country, with RA being more common in North Africa and lower in sub-Saharan Africa.[30] RA is much less prevalent in East Asia compared to the rest of Asia.[30] There was an increase in the global period prevalence of 9.75% over time between 1980-2019 in a meta-analysis of 67 studies.[30]
As outlined above, there is a genetic disposition towards RA, which was demonstrated to be about 40% in a large study from Sweden in 2013.[31] The study also reported a higher heritability for seropositive RA and early-onset RA. According to their report, the risk of RA with a first-degree relative positive for RA is three-fold higher than a second-degree relative with RA giving a two-fold higher risk.[31] Multiple different genetic predispositions to explain this finding have now been identified. The strongest genetic predisposition for RA is from the HLA-DRB1 region (shared epitope).[8]
Among modifiable risk factors, cigarette smoking has the strongest association with RA.[22] Diet and nutrition have been shown to play a significant role as environmental triggers for RA. The typical 'western' diet that is rich, high in caloric content, and low in fiber increases the risk of RA.[32] Consumption of long-chain omega-3 polyunsaturated fatty acids is associated with a reduced risk of RA.[32]
Obesity is another well-established risk factor for RA. There is a 30% increase in the risk of RA for patients with a body mass index (BMI) of greater than 30 kg/m^2 and a 15% increased risk for those with a BMI of 25 to 29.9 kg/m^2.[33]
There is significant literature regarding the association of RA in patients with chronic mucosal or periodontal disease. However, no clear, consistent link has been identified in well-established studies. There is evidence that mucosal injury from occupational exposures and environmental pollutants can increase the risk of RA.[34][35][1][35]
Prevalence of RA (period prevalence 1955-2015)[30]
Continent/Number of Studies/RA Pooled Prevalence (95%CI)
| North America | 10 | 0.70% (0.57-0.86) |
| Europe | 26 | 0.54% (0.50-0.59) |
| Africa | 3 | 0.52% (0.00-1.74) |
| Asia | 26 | 0.30% (0.23-0.37) |
| South America | 2 | 0.30% (0.09-0.62) |
| Global | 67 | 0.46% (0.39-0.54) |
Pathophysiology
RA, in some patients, is triggered by some sort of environmental factor in a genetically predisposed host. The best example is tobacco use in a patient with the HLA-DRB1 "shared epitope" gene and the development of ACPA-positive RA.[1] RF and ACPA antibodies are the best-known autoantibodies in RA, but several other autoantibodies are relatively specific for RA. The presence of antibodies in rheumatoid arthritis is referred to as seropositive RA. RF is an antibody of any isotype that binds to the Fc portion of IgG.
RA patients often have antibodies to citrullinated proteins. These antibodies have been identified in patients with RA since 1964 (antiperinuclear factor)[36] and were also described in 1979 (anti-keratin antibodies)[37] by different assays. In the 1990s, these antibodies were determined to be the same antibodies with high specificity for RA.[38] The antibodies were found to have specificity for filaggrin, a citrullinated peptide.[39][38] The epitope for these antibodies is citrullinated peptides. A cyclic citrullinated peptide (CCP) was synthesized, which could be used in an ELISA to test for these antibodies in patients in a clinical situation.[40] These antibodies are called anti-cyclic citrullinated peptide antibodies (ACPA). Citrulline is derived from the post-transcriptional modification of arginine by peptidyl arginine deiminase (PAD). This reaction occurs at sites of tissue damage and inflammation, such as the lungs in smokers. HLA-DRB1 shared epitope preferentially presents epitopes containing citrulline. ACPA can be IgG, IgM, or IgA isotypes. ACPA can bind citrullinated residues on self-proteins like vimentin, fibronectin, fibrinogen, histones, and type 2 collagen.[23]
Anti-carbamylated protein antibodies(anti-CarP antibodies) are also found in patients with RA. Carbamlyation is the conversion of lysine to homocitrulline in the presence of urea and cyanate. Myeloperoxidase converts thiocyanate to cyanate. The molecular structure of homocitrulline is similar to citrulline; however, anti-CarP antibodies are distinct antibodies that have been associated with RA in both ACPA-positive and ACPA-negative patients.[23] There are other autoantibodies that have been described in RA patients, including those directed against fibrinogen, enolase, and vimentin.[41]
The immune response in RA starts at sites distant from the synovial joints, such as the lung, gums, and GI tract.[1] In these tissues, modified proteins are produced by biochemical reactions such as citrullination. The mechanism behind environment-triggered RA is thought to be due to the repeated activation of innate immunity. Using the lungs as an example, cigarette smoking induces peptidyl arginine deiminase (PAD) expression in alveolar macrophages, which leads to the conversion of arginine to citrulline in the airway.[42] This process creates a "neoantigen" that activates an immune response and leads to the formation of anti-citrullinated protein antibodies (ACPAs).[42][23]
Patients are genetically predisposed to develop an immune response to the modified proteins, anti-modified protein antibodies (AMPA). Citrullination is produced by the action of PAD on arginine. Isoforms PAD2 and PAD4 are most strongly implicated in RA. Anti-PAD4 antibodies are found in patients with RA, are highly specific for RA, and are associated with ACPA positivity.[43] in other mucosal areas, the inflammatory response in gingivitis is associated with the presence of Porphyromonas gingivalis, which causes an inflammatory reaction. There is an influx of leukocytes that produce PAD4. P gingivalis also produces a PAD-like enzyme. These enzymes can citrullinate resident proteins, which then can act as autoantigens.[44] Anti-acetylated protein antibodies have recently been associated with RA (in approximately 40% of RA patients), predominately in seropositive patients.[23] Acetylation is an enzymatic process converting lysine to acetyllysine, thought to be mediated by bacteria, which may provide a link to RA and microbiome dysbiosis. The exact mechanism at this time remains unclear.[23] So there are several types of modified proteins that can be the target of autoantibodies produced by citrullination, carbamylation, and acetylation.[45][46]
Autoantibodies appear before the onset of clinical arthritis.[47][41] Autoimmunity starts at the molecular and cellular level long before the clinical phase of RA, often referred to as pre-symptomatic or pre-clinical RA. During this phase, certain immunologic and biochemical abnormalities have been found, but the patients are asymptomatic.[48][49][47] RF and ACPA can be present in the serum up to 10 years before the onset of clinical symptoms. With time the concentration of ACPA and serum cytokine levels increase.[50][23] Many patients develop autoantibodies but do not develop the overt disease. Some patients will eventually transition from autoimmunity to immune-mediated inflammation primarily focused in the synovium.[1] These autoantibodies are produced by plasma cells in the synovium. The synovium in RA is infiltrated by immune cells, which include innate immune cells (monocytes, dendritic cells, mast cells) and adaptive immune cells (T-helper 1, Th1); T-helper 17, Th17), B cells, and plasma cells). Synovial fibroblast-like synovial cells (FSC) are activated. Neutrophils are not present in the synovium but egress from the blood to the synovial fluid.[51]
Cytokines and chemokines such as tumor necrosis factor (TNF), interleukin-6 (IL-6), and granulocyte-monocyte colony-stimulating factor (GM-CSF) activate endothelial cells and attract immune cells within the synovial compartment.[23] The FSC in the rheumatoid synovium changes to an invasive phenotype. FSC and inflammatory cells produce RANKL leads to osteoclast generation resulting in bone erosions, the hallmark feature of rheumatoid arthritis.[52] It is important to note that synovial biopsies in seropositive patients with arthralgia were essentially unremarkable.[53] It is theorized that a second environmental trigger is needed to cause clinically apparent disease. When this is established, a destructive inflammatory process begins. Fibroblast-like synoviocytes (FLS) migrate from joint to joint, leading to progressive joint damage.[52]
All elements of the immune system are involved, including innate immunity and adaptive immunity, which includes the cellular (T cell) immune response and the humeral (B cell) immune response.[54][46] The innate immune response includes macrophages which produce TNF, IL-6, IL-1, GM-CSF, IL-15, IL-18, IL-32, and chemokines which promote tissue inflammation.[54] Other elements of innate immunity include cells such as endothelial cells, which allow the egress of immune and inflammatory cells such as neutrophils which migrate to the synovial fluid and produce prostaglandins, proteases, and reactive oxygen intermediates, all of which are pro-inflammatory and cause destruction to the cartilage.[54][51]
Resident fibroblasts-like synoviocytes (FLS) are activated by proinflammatory cytokines, PGDF, and chemokines to proliferate with invasive characteristics and produce matrix metalloproteinases (MMP) and ADAMTS. Chondrocytes are activated by TNF, IL-1, and IL-17, producing matric enzymes resulting in cartilage damage. Resident mast cells produce vasoactive amines, leukotrienes, proteases, and TNF. Osteoclasts are activated by RANKL, which plays a vital role in producing bone erosions.[51] Another element of innate immunity is the complement system which is activated by RF and ACPA-containing immune complexes producing C3a and C5a, which are pro-inflammatory, attracting and activating neutrophils and also activating macrophages and mast cells.[51]
Adaptive immunity includes T cells and B cells which respond to antigenic stimuli. In RA, one of the main antigens triggering autoimmunity is modified proteins such as citrullinated proteins.[1][54][51][55][45][46][56] At mucosal sites, T cells are activated by these modified proteins, which trigger B cells to produce AMPA, including ACPA. In some patients, this immune response develops into an immune-mediated inflammation in the synovium.[54][51] T cells and B cells take up residence in the synovium populating the subsynovial region. The mononuclear cell infiltrate appears histologically like a lymphoid organ. Dendritic cells serve as a bridge between innate and adaptive immunity by presenting antigens to antigen-specific T cells.[54][51]
T cells interact with B cells, activating antigen-specific B cells to differentiate into plasma cells that produce RF and ACPA. These autoantibodies bind to their antigens forming immune complexes that can further the inflammatory response by activating the complement system.[51][57] Some activated T cells become type 1 helper T cells (Th1) and type 17 helper T cells (Th17). Th17 cells produce IL-17, a proinflammatory cytokine that attracts other T cells and neutrophils.[54][51]
Cytokines are produced in large amounts in the synovium and play an important role in propagating an intense inflammatory response resulting in bone erosions and cartilage loss.[51][54][58] Chronic inflammation also plays a role in associated comorbidities, such as the increased risk of cardiovascular disease. The following table outlines the most important cytokine involved in the pathogenesis of RA.
Cytokines and Chemokines (CXC) Involved in the Pathogenesis of RA
FLS = fibroblast-like synoviocytes; MCP-1 = macrophage chemoattractant protein-1; ILC3 = innate lymphoid cell group 3; MMP = matric metalloproteinase; NO = nitric oxide; PG = prostaglandins[51]
| Cytokine | Source of cytokine | Cytokine receptor | Biologic effects of cytokine |
| TNF-alpha | Macrophages, FLS, Endothelial cells | TNFRSF1, TNFRSF2 |
FLS activation and proliferation, resulting in pannus, activation of chondrocytes, osteoclasts, and endothelial cells. |
| IFN-gamma | T cells, NK cells, Macrophages, B cells, Dendritic cells | IFNGR1, IFNGR2 | Activation of antigen-presenting cells by upregulating MHC Class II genes. |
| IL-1 | Macrophages, FLS, Chondrocytes | IL-1R1, IL-1R2 | Activates FLS, macrophages, neutrophils, T and B cells, osteoclasts, and chondrocytes, promoting TNF-alpha and IL-6 production, PGE2 production, and production of MMPs. |
| IL-6 | Macrophages, FLS, T cells, endothelial cells | Heterodimer of IL-6R-alpha and gp 130 | B cell activation and differentiation, Th17 activation and differentiation, osteoclast formation, and stimulates the liver to synthesize acute phase proteins. |
| IL-15 | Macrophages, Dendritic cells, endothelial cells, FLS | Heterotrimer of IL-15R-alpha, IL-15R-beta, and gamma-c | Chemotactic and activation factor for T cells induces the production of TNF-alpha, MMP, MCP-1, and IL-8. |
| IL-17 | Th17 cells, ILC3 | Hertodimer of IL-17RA and IL-17RB, IL-17C, or IL-17E | Activates and attracts T cells and neutrophils, activates FLS, macrophages, endothelial cells, osteoclasts, and chondrocytes, stimulates the production of TNF-alpha, IL1-beta, IL-6, IL-8, IL-23, chemokines, nitric oxide (NO), PG, GM-CSF, MMPs, promotes RANKL |
| IL-18 | Macrophages, Dendritic cells, FLS | Heterodimer of IL-18R-alpha and IL-18R-beta | Stimulates macrophages, T cells, and NK cells to produce TNF-alpha, IL-1-beta, and GM-CSF, which activates neutrophils. |
| IL-23 | Macrophages, Dendritic cells, B cells | Heterodimer of IL-23R and IL-23R and IL-12R-beta-1 | Induces differentiation of Th17 cells and osteoclasts, production of IL-6, TNF-alpha, IL-1-beta, and chemokines. |
| IL-8 (Chemokine CXCL8) | Macrophages, FLS, endothelial cells | CXCR1, CXCR2 | Chemotactic and activation factors for neutrophils, T cells, and NK cells. |
| Other chemokines in the CXC and CC families | Neutrophils, Macrophages, FLS, T cells, etc. | Various CXC and CC receptors | Attracts and promotes activation of neutrophils, macrophages, T cells, FLS, etc. |
Histopathology
One of the earliest histopathologic findings in RA is new synovial blood vessel growth; this leads to the transmigration of lymphocytes and polymorphonuclear leukocytes into the synovial fluid. Angiogenesis is required to support the highly catabolic synovium and is accomplished via proinflammatory cytokines such as tumor necrosis factor (TNF).[59] With angiogenesis, cytokines activate endothelial cells to produce adhesion molecules which in turn facilitate cell migration into the synovium. Despite angiogenesis, RA synovial fluid is a hypoxic environment, leading to increased production of cyclooxygenase (COX) 2-derived nociceptive eicosanoids and matrix metalloproteinases (MMPs).[60] This further stimulates an inflammatory response in the synovium. During the early phase of the disease, the influx of inflammatory cells into the synovial membrane leads to a proliferation of monocytes and thickening of the synovial membrane with small villous projections into the joint space.[59]
The histopathology of rheumatoid synovium reviews intense FLS activation and proliferation and subsynovial accumulation of T cells, including Th1, Th17, and Treg cells. B cells also accumulate and differentiate into plasma cells. The appearance of synovial tissue can appear similar to secondary lymphoid tissues such as lymph nodes. Macrophages, dendritic cells, mast cells, and fibroblasts are also present in the subsynovial tissue. Rheumatoid synovial tissue becomes invasive, eroding into the bone and causing marginal erosions.[2]
Rheumatoid nodules initially have a small vessel vasculitis phenomenon followed by a chronic inflammatory granulomatous phase. The development of rheumatoid nodules is frequent in rheumatoid arthritis, involving the dermis or subcutis in peri-articular areas. When multiple, this phenomenon can be related to methotrexate therapy and is called accelerated rheumatoid nodulosis.[61] The size is variable and can range from a few millimeters to centimeters. It appears grossly as a whitish fibrous lesion with yellowish areas corresponding to collagenous necrobiosis. The histological appearance can be indistinguishable from granuloma annulare. There are areas of irregular geographic-like necrobiosis of the dermis and hypodermis surrounded by histiocytes arranged in a well-developed palisade, occasional lymphocytes, and neutrophils. Occasionally, giant cells and mast cells can be present. Fibrin and collagen are present in the center of the necrobiotic areas. The surrounding dermis and hypodermis have a perivascular infiltrate of plasma cells.[61] Very occasionally, rheumatoid nodules may occur in the lungs.
History and Physical
The most common and predominant symptoms include joint pain and swelling, usually starting insidiously over a period of weeks to months. Initial joint involvement is typically in the small joints of the hands and feet, followed by larger joints. One of the hallmarks is stiffness, particularly morning stiffness.[2][62] Usually, the onset of symptoms is slow and insidious; however, in some cases, an episodic pattern of symptoms can be seen and is defined as palindromic rheumatism.[63] Not all patients with palindromic rheumatism develop RA, and they respond to hydroxychloroquine which supports the idea that palindromic rheumatism is a distinct phenotype of RA.[64]
As discussed above, RA involves small peripheral joints, usually of the hands. The axial joints can be involved, but this is limited to the cervical spine as there are synovial joints in this part of the spine. The lumbar spine is not involved.[65] Although multiple small joint involvements are a frequent feature, some patients may present with monoarticular and extraarticular involvement (lungs).[4] RA is a chronic progressive disease, and without treatment with disease-modifying anti-rheumatic drugs (DMARDs), patients will develop joint damage, deformities, disability, and increased mortality.[4]
On physical examination, the affected joint will be painful if pressure is applied to the joint or on movement with or without joint swelling. Synovial thickening with a "boggy" feel on palpation will be noted. Joint erythema and warmth are usually absent, and wrist involvement may present with typical signs and symptoms of carpal tunnel syndrome. With multiple joint involvements, reduced grip strength will be seen on physical testing. The classical physical findings of ulnar deviation, metacarpophalangeal joint subluxation, ulnar deviation, swan neck deformity, Boutonniere deformity, and the "bowstring" sign are seen in advanced chronic disease. Other findings in the later stages of RA include a reduced range of motion in the shoulders, elbows, and knees. In the feet, hallux valgus is common, as well as other toe deformities.[4]
Rheumatoid nodules are the most common extraarticular manifestations of RA.[66] They are commonly found on pressure points such as the olecranon but may also occur over the joints of the hands and feet, the patella, and the Achilles tendons.
Interstitial lung disease (ILD) affects 5 to 16% of patients with RA and is associated RA specific autoantibodies and increased mortality.[67][68][69] Some patients may present with ILD before developing joint inflammation with positive RF and ACPA. RA-associated ILD is associated with ACPA, anti-carbamylated protein antibodies (anti-CarP), and anti-malondialdehyde-acetaldehyde antibodies (anti-MAA).[70][71][72] The MUC5B promoter variant rs35705950 is associated with ILD in patients with RA. This gene encodes mucin 5B, and this variant is a gain of function. RA-ILD compared to unaffected controls, the odds ratio is 3.8 (95% CI 2.8-5.2), and RA-ILD compared to RA without ILD, the odds ratio is 3.1 (95% CI 1.8-5.4).[73]
Ophthalmological manifestations include secondary Sjogren syndrome with dry eyes and also dry mouth.[74] Also, inflammatory eye diseases such as episcleritis and scleritis have become uncommon with new therapies for RA. Similarly, Felty syndrome, which is the combination of long-standing seropositive RA (including RF and ANA), leukopenia, and splenomegaly, is rarely seen today. These patients may have chronic non-healing ulcers and an increased risk of bacterial infection. Vasculitis involving both medium and small-sized blood vessels can also be seen as a presenting symptom of RA. However, the prevalence of vasculitis among patients with RA is low.[75] Patients with rheumatoid vasculitis may exhibit mononeuritis multiplex or asymmetric polyneuropathy.
Evaluation
Laboratory testing often reveals anemia of chronic disease and thrombocytosis. Neutropenia may be present if Felty syndrome is present (rare). RF is present in 80-90% of patients with RA, with a sensitivity of 69% and a specificity of 85%. ACPA is present in 70-80% of patients, with a sensitivity of 67% and a specificity of 95%.[76] Patients with RA with RF, ACPA, or both are designated as having seropositive RA. About 10% of RA patients are seronegative, meaning they do not have RF or ACPA. The presence of rheumatoid factor is not diagnostic of rheumatoid arthritis. It may be present in other connective tissue diseases such as systemic lupus erythematosus, Sjogren syndrome, scleroderma, and granulomatosis with polyangiitis. RF may also be found in patients with chronic infections and healthy individuals, albeit in low titers; if both RF and ACPA are positive, the sensitivity and specificity of the diagnosis increase substantially. RF and ACPA are present for months to years before the onset of clinical arthritis.[47]
Therefore, when a patient presents with inflammatory arthritis, serological studies should be positive. In patients who are asymptomatic or those that have arthralgias, a positive RF and especially CCP predicts the onset of clinical RA.[77][78][79] Healthy relatives of patients with RA who have a positive RF and even more so with a positive ACPA are at increased risk for developing RA.[80][81] Acute phase reactants, such as erythrocyte sedimentation rate (ESR) and levels of C-reactive protein (CRP), are usually elevated in patients with active disease and should be obtained and can be used to assess disease activity when following patients with RA.
Synovial fluid examination usually reveals a leukocyte count between 1500 to 25,000/cubic mm and is predominantly polymorphonuclear cells. Cell counts higher than 25000/cubic mm are rare and can be seen with very active disease; however, they warrant workup to rule out underlying infection. The synovial fluid in RA will also reveal low C3 and C4 levels despite elevated serum levels.[82]
With advanced disease, joint involvement on plain radiographs will reveal periarticular osteopenia, joint space narrowing, and bony erosions (marginal). Erosions of cartilage and bone are considered pathognomonic findings for RA, although not absolutely specific. However, these findings are consistent with advanced disease.[83] Magnetic resonance imaging (MRI) and ultrasonography are useful in early disease before radiographic evidence of bone erosion occurs.[84] A decreased signal from the bone marrow on T1-weighted images and gadolinium-enhanced images indicates bone marrow edema. MRI can also reveal synovial thickening, which has been shown to predict the future presence of bony erosions.[85] The clinical utility of MRI and its incorporation into the diagnostic criteria for RA remains to be determined.
Due to the varied clinical presentation and lack of universal pathognomonic testing for RA, diagnosing the disease can be challenging early in the course of the disease. Traditionally the presence of at least four of the following criteria for at least six weeks would classify the patient as having RA. These criteria were: morning stiffness, arthritis of three or more joints, arthritis of the hands, symmetric arthritis, elevated acute phase reactants, elevated rheumatoid factor, and radiologic evidence of RA. These criteria separated inflammatory from non-inflammatory arthritis but were not very specific for RA. It was also not sensitive to early-stage RA, which was a significant drawback.[86] With the development of serologic markers, the diagnostic criteria were redefined. The 2010 American College of Rheumatology and the European League Against Rheumatism (ACR/EULAR) diagnostic criteria for RA are outlined below. It includes four different domains, which are as follows:
2010 ACR/EULAR Classification Criteria for RA
- Number and size of involved joints[87]
- 2 to 10 large joints = 1 point (shoulders, elbows, hips, knees, and ankles)
- 1 to 3 small joints = 2 points (metacarpophalangeal joints, proximal interphalangeal joints, second through fifth metatarsophalangeal joints, thumb interphalangeal joints, and wrists)
- 4 to 10 small joints = 3 points
- Greater than 10 joints (including at least 1 small joint) = 5 points
- Serological testing for rheumatoid factor or anti-citrullinated peptide/protein antibody[87]
- Low positive = 2 points
- High positive = 3 points
- Elevated acute phase reactant (erythrocyte sedimentation rate [ESR] or C-reactive protein [CRP]) = 1 point[87]
- Symptom duration of at least six weeks = 1 point[87]
A total score greater than or equal to 6 classifies the patient as having RA. Note that these are classification and diagnostic criteria, so their primary purpose is being used in clinical studies of patients with RA, including clinical trials. It is important to note that joint involvement refers to any swollen or tender joint on examination. Imaging studies may also be used to determine the presence of synovitis/joint involvement. The 2010 ACR/EALAR criteria excluded distal interphalangeal joints, first carpometacarpal joints, and first metatarsophalangeal joints from this criteria. Also, these criteria may only be applied to those patients where the joint involvement is not better explained by other inflammatory diseases, such as systemic lupus erythematosus or psoriasis. Specific testing must be obtained to rule out these diseases. The new criteria were noted to better predict the probability of RA, have the same sensitivity as the previous criteria for the diagnosis of RA and have a higher specificity as well as a higher negative predictive value.[86]
Treatment / Management
The goal of treatment in patients with RA is early diagnosis and early initiation of treatment to prevent irreversible damage to the joints. The International Task Force Guidelines published in 2014 make the following recommendations regarding the treatment of RA:[88]
- The primary goal of treatment is to achieve long-term clinical remission and optimize quality of life with the absence of signs and symptoms associated with inflammatory disease activity.
- If clinical remission cannot be achieved, low disease activity is an acceptable alternative.
- Disease activity should be assessed every month in patients with moderate to severe disease activity.
- In patients with low disease activity or clinical remission, disease activity should be assessed every 3 to 6 months.
Multiple clinical assessment tools have been developed to assist clinicians in determining the disease activity of patients with RA. An updated recommendation from the American College of Rheumatology (ACR) in 2019 recommended using the following assessment tools because they met the minimum standard for evaluation per their recommendation.[89][90] In clinical practice, the combination of the DAS28, CDAI, and RAPID3 is easy to use and includes patient input, provider input, and laboratory tests.(A1)
- Clinical Disease Activity Index (CDAI)
- Disease Activity Score (DAS)
- Disease Activity Score 28 Joints (DAS28-ESR/CRP)
- Patient-Derived DAS28
- Hospital Universitario La Princesa Index (HUPI)
- Multi-Biomarker Disease Activity Score (MBDA score, VECTRA DA)
- Rheumatoid Arthritis Disease Activity Index (RADAI)
- Rheumatoid Arthritis Disease Activity Index 5 (RADAI-5)
- Routine Assessment of Patient Index Data 3 (RAPID3)
- Routine Assessment of Patient Index Data 5 (RAPID5)
- Simplified Disease Activity Index (SDAI)
Disease-modifying antirheumatic drugs (DMARDs) typically used in treating RA include methotrexate, hydroxychloroquine, sulfasalazine, and leflunomide. Anti-TNF-alpha inhibitors include etanercept, infliximab, adalimumab, golimumab, and certolizumab pegol. Other biologic DMARDs include interleukin (IL) 6 inhibitors such as tocilizumab and sarilumab, T-cell costimulation inhibitors such as abatacept (CTLA4-Ig), and the anti-CD20 B-cell depleting monoclonal antibody such as rituximab. Targeted synthetic DMARDs include Janus kinases (JAK) inhibitors such as tofacitinib, baricitinib, and upadacitinib.[2][4]
DMARD therapy, including biologic agents and targeted synthetic agents (tofacitinib), should be temporarily held in patients with a serious active infection. They can be resumed after the infection has resolved and antimicrobial treatment has been completed.[91] It is essential to remember that all patients starting treatment for RA should be screened for hepatitis B and C and tuberculosis. Methotrexate should be avoided in patients with liver disease.[91] Patients with latent tuberculosis should complete treatment for at least one month before initiating biologic and targeted synthetic agents. If patients cannot take or complete treatment for latent tuberculosis, conventional DMARD therapy should be used.[91] In patients with underlying skin cancer and lymphoproliferative disorders, biologic agents should be avoided except for rituximab in patients with lymphoproliferative disorders, as there is evidence of benefit from B-cell suppression in these cases.[91] The ACR also recommends that before starting therapy for RA, patients should receive vaccination for pneumococcus, hepatitis, influenza, human papillomavirus (HPV), herpes zoster virus (HZV), and COVID-19.
Non-steroidal Anti-inflammatory Drugs (NSAIDs)
NSAIDs do not have any disease-modifying effects but are commonly used to relieve symptoms related to joint inflammation and pain. There are about 20 such drugs (depending on what country you are in) that are all effective at full doses. There is some variation in side effects and toxicities. There is a class Black Box warning for cardiovascular disease, although there is variation in the cardiovascular effects among NSAIDs.[92][93] NSAIDs also have the potential for gastrointestinal, renal, and hematologic toxicity. The choice of a specific NSAID depends on the patient, their comorbidities, and the provider's familiarity with the specific drug. Non-acetylated salicylates (salsalate) have an excellent safety profile with little GI, renal, or hematologic effects but are not commonly used. There are recommendations for using NSAIDs with regard to a patient's cardiovascular and gastrointestinal comorbidities.[94](A1)
- Efficacy: indomethacin, piroxicam
- Convenience (1-2 doses per day): meloxicam, naproxen, celecoxib, nabumetone
- Overall safety: nabumetone[95]
- GI safety: celecoxib, nabumetone
- Renal safety: possible nabumetone
- Hematologic safety (no antiplatelet effect): celecoxib, meloxicam, nabumetone (B2)
Corticosteroids
Corticosteroids are commonly used in patients with RA. There are several situations in which corticosteroids should be considered. In a new patient with very active RA, corticosteroids can be used as bridge therapy while DMARD therapy is instituted. Some studies show that using corticosteroids early in RA patients improves outcomes and has disease-modifying effects, including radiographic progression.[96][97] Another study did not show long-term benefits from corticosteroid bridge therapy.[98] Short courses of corticosteroids can be used for mild flares of RA. Intra-articular corticosteroids can be used for single-joint flares. About 50% of patients with RA require low-dose corticosteroids (prednisone 2.5 to 7.5 mg daily to maintain control of their disease. Long-term corticosteroids are associated with numerous toxicities, including weight gain, osteoporosis, and increased risk of infections.(A1)
Nonbiologic DMARDs
This category includes methotrexate, hydroxychloroquine (HCQ), azathioprine (AZA), sulfasalazine, leflunomide, and cyclosporine. Methotrexate is the initial drug of choice for patients with RA. The recommended treatment plan recommends an initial dose of 10-15 mg/week of methotrexate with an escalation of 5 mg/month and a target dose of 20-25 mg/week.[99] Subcutaneous administration can be tried in patients who do not respond adequately or are intolerant to oral administration.[100] In patients on methotrexate, 15 mg/week or higher, who still have some disease activity, splitting the dose (10 mg in the morning and 10 mg in the evening every week) increased the bioavailability of methotrexate.[101] Triple therapy, consisting of the combination of methotrexate, hydroxychloroquine, and sulfasalazine, has been shown to be an effective regimen for RA.[102][103] However, triple therapy is not well tolerated, and a large percentage of patients do stay on this therapy.[104][105][106](A1)
TNF inhibitors
The TNF inhibitors include etanercept, infliximab, adalimumab, certolizumab, and golimumab. The ACR does not recommend using TNF inhibitors until a nonbiologic DMARD has been tried.[91] However, studies have shown that adding TNF inhibitors in patients who have failed methotrexate therapy is better than adding another nonbiologic DMARD.[107] The most concerning adverse effect of these agents is opportunistic infections and reactivation of latent tuberculosis. There is some concern about the generation of antibodies against these agents, which may decrease their efficacy over time; however, using methotrexate in combination with these agents has been shown to decrease this complication.[108] Acute infection, advanced heart failure, demyelinating disease, and recent malignancies are contraindications for using these agents.[91] (A1)
Rituximab
Rituximab is a biologic DMARD that can be added for treating RA if patients have uncontrolled RA and who did not respond to TNF inhibitors.[109] Rituximab is given as an intravenous infusion; it depletes CD20+ B-cells and decreases the immune response to vaccines in patients receiving rituximab. Responses to rituximab are better if the patients are seropositive and if the patients are also on methotrexate. As stated above, it is a preferred agent in patients with underlying lymphoproliferative disorders. (A1)
Abatacept
Abatacept inhibits T-cell activation by binding to CD80 and CD86. It is administered as a monthly intravenous infusion or as a weekly subcutaneous injection. Patients with uncontrolled RA, who have shown an inadequate response to methotrexate and TNF inhibitor therapy, benefit from abatacept therapy with proven efficacy from 6 months to 5 years of therapy.[110]
Interleukin 6 Inhibitors
Tocilizumab, an IL-6 receptor inhibitor, is indicated for moderate-to-severe active RA in adults who have had an inadequate response to TNF inhibitor therapy. These patients develop clinically meaningful improvement with the use of tocilizumab.[111] Sarilumab is another agent in this category that has been shown to improve clinical outcomes in patients with uncontrolled RA despite TNF inhibitor therapy.[112](B3)
Janus kinase (JAK) Inhibitors
JAK is a group of tyrosine kinases that participate in intracellular signal transduction for hematopoiesis and immune cell function. JAK inhibitors (such as tofacitinib) are oral agents that reduce the production of cytokines and are approved as second-line agents for the treatment of RA.[113](A1)
ACR and EULAR Treatment Guidelines
- According to the ACR treatment guidelines for early RA, patients who have not taken disease-modifying antirheumatic drug (DMARD) therapy should start DMARD therapy regardless of the disease activity level.
- In patients with low disease activity and early disease, monotherapy with methotrexate is the preferred treatment.
- Leflunomide or sulfasalazine are the first-line treatment in patients with a contraindication to methotrexate or intolerance to it.
- If monotherapy with DMARD does not control disease activity (regardless of concomitant glucocorticoid use), therapy should be altered. Methotrexate can be continued or discontinued at this point. Additional therapy options after failed monotherapy with DMARD are recommended as either dual traditional/nonbiologic DMARD therapy, tumor necrosis factor (TNF) inhibitors, or non-tumor necrosis factor biologic agents.
- In patients with established RA, who are DMARD naive, methotrexate is the preferred agent for initial monotherapy, regardless of the disease activity level.
- If monotherapy with DMARD does not control disease activity in established RA (regardless of concomitant glucocorticoid use), dual DMARD therapy, a TNF inhibitor, a non-TNF biologic agent, or tofacitinib therapy can be added.
- If disease activity remains high on TNF inhibitor monotherapy, DMARD therapy should be added in addition to the TNF inhibitor.
- If disease activity remains high despite a TNF inhibitor switch to a non-TNF biologic agent with or without methotrexate
- If disease activity remains high despite a trial of anti-TNF and non-TNF agents, use another non-TNF biologic agent before considering tofacitinib.
- If still uncontrolled despite the above trials, use tofacitinib
- If disease activity remains high despite the above combination therapies, short-term low-dose glucocorticoid therapy should be added.
- TNF inhibitors should be avoided in patients with congestive heart failure.
- Patients with hepatitis C who have not been treated or are currently not on treatment for it should receive nonbiologic DMARD therapy rather than TNF inhibitors.[91]
Safety Considerations with Biologic and Targeted Synthetic DMARDs
- Serious infections: All biologic and targeted synthetic DMARDs are associated with 2 to 3 times the number of infections. Hold all agents during an active infection, hold for surgical procedures, and avoid live vaccines. Opportunistic infections, including TB and fungal infections, all patients should be assessed for latent TB.
- Herpes zoster: JAK inhibitors
- Neutropenia: IL-6 inhibitors, JAK inhibitors, rituximab
- Elevated LFTs, elevated cholesterol: IL-6 inhibitors, JAK inhibitors
- Thrombosis: JAK inhibitors
- CHF: TNH inhibitors
- Cardiovascular events: JAK inhibitors (Black Box warning)
- Demyelinating diseases: TNF inhibitors
Differential Diagnosis
- Osteoarthritis
- Psoriatic arthritis
- Systemic lupus erythematosus
- Sjogren syndrome
- Polymyalgia rheumatic
- Chronic gouty arthritis
- Calcium pyrophosphate deposition disease
Staging
Stages of RA as Defined by the ACR
- Stage 1: No destructive changes on X-rays
- Stage 2: Presence of X-ray evidence of periarticular osteoporosis, subchondral bone destruction but no joint deformity
- Stage 3: X-ray evidence of cartilage and bone destruction in addition to joint deformity and periarticular osteoporosis
- Stage 4: Presence of bony or fibrous ankylosis along with stage 3 features[91]
Prognosis
Rheumatoid arthritis has no cure and is a progressive disease associated with morbidity and increased mortality. All individuals will experience multiple exacerbations and, without treatment, tend to have poor outcomes with disability and increased mortality.[114][5][114] Early treatment (within six months of symptom onset) has shown improved functional capacity and decreased disease activity as measured by swollen joint count and tender joint count. However, the mortality rate was similar in patients receiving early treatment and late treatment (after six months of symptoms), and both were significantly improved from no treatment.[114] Approximately 40% of patients with RA will have a functional disability affecting their ability to work and complete activities of daily living within ten years of the diagnosis.[115]
Patients with RA also develop other chronic medical conditions/complications which drastically affect their outcomes. The most notable of this correlation is the relationship between RA and atherosclerotic cardiovascular disease leading to accelerated coronary artery disease.[116][117] RA increases the risk of cardiovascular disease, lung diseases, and malignancies, which in turn increases the risk of premature mortality in these patients.[118]
Complications
Complications of RA span multiple organ systems and are known to worsen clinical outcomes in patients with RA. It is imperative to monitor patients for the development of these complications and quickly alter treatment plans if applicable. Frequent recurrent serious opportunistic infections occur in patients with RA, which warrants withholding DMARD therapy until they are treated. The increased frequency of infections in patients with RA is thought to be due to underlying immune dysfunction from the disease itself and the use of DMARD therapy.[119]
Complications and Comorbidities Associated with Uncontrolled Systemic Inflammation
- Chronic joint inflammation results in radiographic damage, progressive deformity, and functional disability.
- Anemia of chronic disease and Felty syndrome are well-documented complications of seropositive RA.[74]
- The secondary form of Sjögren syndrome is associated with RA and can have a prevalence of as high as 10% in patients with RA and pulmonary disease.[74] Other complications are uncommon to rare, including inflammatory eye disease and Felty's syndrome. Rheumatoid vasculitis is a rare phenomenon but can have severe complications if present. Clinical presentation ranges from focal digital involvement to severe systemic involvement resembling polyarteritis nodosa.[75]
- Pleuritis, bronchiolitis, and interstitial lung disease are also associated with RA. Although rare, RA treatment with methotrexate and anti-TNF agents can also lead to pulmonary injury. There is also an increased risk of pulmonary embolism in RA. Interstitial lung disease (ILD) affects 5 to 16% of RA patients and is associated with RA-specific autoantibodies and increased mortality.[67][68][69] Some patients may present with ILD before developing joint inflammation with positive RF and ACPA. RA-associated ILD is associated with ACPA, anti-carbamylated protein antibodies (anti-CarP), and anti-malondialdehyde-acetaldehyde antibodies (anti-MAA).[70][71][72] The MUC5B promoter variant rs35705950 is associated with ILD in patients with RA. This gene encodes mucin 5B, and this variant is a gain of function. RA-ILD compared to unaffected controls, the odds ratio is 3.8 (95% CI 2.8-5.2), and RA-ILD, compared to RA without ILD, the odds ratio is 3.1 (95% CI 1.8-5.4).[73]
- Coronary artery disease has a strong association with RA.[117] RA is an independent risk factor for the development of coronary artery disease (CAD) and accelerates the development of CAD in these patients.[116] Accelerated atherosclerosis is the primary cause of morbidity and mortality in patients with RA leading to CAD and peripheral vascular disease.[120] There is increased insulin resistance and diabetes mellitus associated with RA, and is thought to be due to chronic inflammation. When treated with specific DMARDs such as hydroxychloroquine, methotrexate, and TNF antagonists, there was a marked improvement in glucose control in these patients.[121] The use of conventional and biologic DMARDs is associated with a reduced risk of cardiovascular events.[122] TNF inhibitors and abatacept appear to have the greatest effect on cardiovascular disease, and the addition of methotrexate to biologic agents is associated with an even lower risk of cardiovascular events.[123][124]
- Patients with RA also have a greater risk of developing lymphoma, with a higher incidence of non-Hodgkin lymphoma in these patients. The clinical course of RA in these patients is accelerated, and diffuse B-cell lymphoma is often the most common subtype.[125] Non-Hodgkin's lymphoma is more common in patients with RA, but this occurs mainly in patients with persistently active disease.[126] The use of biologic DMARDs does not appear to increase the risk of lymphoma.[127]
Complications and Comorbidities Associated with RA Disease and Treatment
- Premature death
- Serious infections
- Osteopenia and osteoporosis are complications of the disease itself and can also be associated with drug therapies (glucocorticoids). Compared to the general population, patients with RA have a 60% to 100% increased risk of fracture.[128] Patient factors that increase the risk of this complication in patients with RA are the same as those of osteoporosis, including postmenopausal state, low body mass index, and advanced age.
- There is an increased risk of venous thromboembolic disease in patients with RA, as stated above, even after adjusting for other risk factors for thromboembolic disease.[129] Multiple studies have reported a higher risk of thromboembolic disease in patients receiving TNF inhibitor therapy and JAK inhibitors.[130][131] however, the consensus regarding this association is not well established. Some studies suggest that higher thromboembolic disease with the use of these agents is secondary to higher disease activity rather than an adverse effect of the agents.[131]
Others
- Depression is a significant complication of RA. It is present in patients with long-term active disease and debilitating physical dysfunction. A 2013 meta-analysis reported a 17% to 39% prevalence of depression in patients with RA.[132]
Deterrence and Patient Education
RA has a strong genetic component and cannot be entirely avoided; however, modifiable risk factors such as cigarette smoking and consuming a balanced diet should be addressed. Patients at risk for RA should be counseled to eat a well-balanced diet, exercise regularly, and maintain healthy body weight.
Enhancing Healthcare Team Outcomes
Rheumatoid arthritis is a chronic disorder with no cure. It affects many other organs and is best managed with an interprofessional team to provide comprehensive care. The key is patient education by nurses, pharmacists, rheumatologists, and primary care providers. The nurse should inform the patient about the signs and symptoms of different organ systems and when to seek medical care. The patient should enroll in an exercise program to recover joint function. An occupational therapy consult can help the patient manage daily living activities. The pharmacist should educate the patient on the types of drugs used to treat rheumatoid arthritis and their potential side effects while checking for interactions and reporting their findings to the team for therapy modification, if necessary.
At each clinic visit, clinicians and nurses should educate the patient to stop smoking, maintain a healthy body weight, get the recommended vaccinations and eat a healthy diet. The social worker should be involved in ensuring that the patient's home is liveable and the patient has ample support systems. The patient should be encouraged to join support groups. Due to progressive disability, chronic pain, and poor quality of life, many patients become depressed and need a mental health nurse and counselor to cope with their disease. A comprehensive interprofessional team can provide a multi-faceted approach to treating RA and improving patient outcomes. [Level 5]
RA has frequent relapses and remissions. While some patients have mild disease, others may have a disease that severely affects their quality of life. Worse outcomes are usually seen in patients with a high titer of autoantibodies, HLA-DRB1 genotypes, age younger than 30 years at onset, multiple joint involvements, female gender, and extra-articular involvement on presentation. In addition, the drugs used to treat rheumatoid arthritis also have potent side effects, which often are not well tolerated. As the disease progresses, many patients will develop adverse cardiac events leading to death. The overall mortality in patients with rheumatoid arthritis is three times higher than in the general population.[133][134] A comprehensive interprofessional team approach to treating and monitoring patients with RA can help improve clinical outcomes for these patients. [Level 5]
Media
(Click Image to Enlarge)

Summary keynotes on Rheumatoid Arthritis Contributed by StatPearls
(Click Image to Enlarge)

Ultrasound image of the thumb in a patient with a history of Rheumatoid Arthritis shows an abnormal amount of fluid within the flexor pollicus longus tendon sheath, consistent with an inflammatory tenosynovitis. Contributed by Mike Tall, MD
(Click Image to Enlarge)
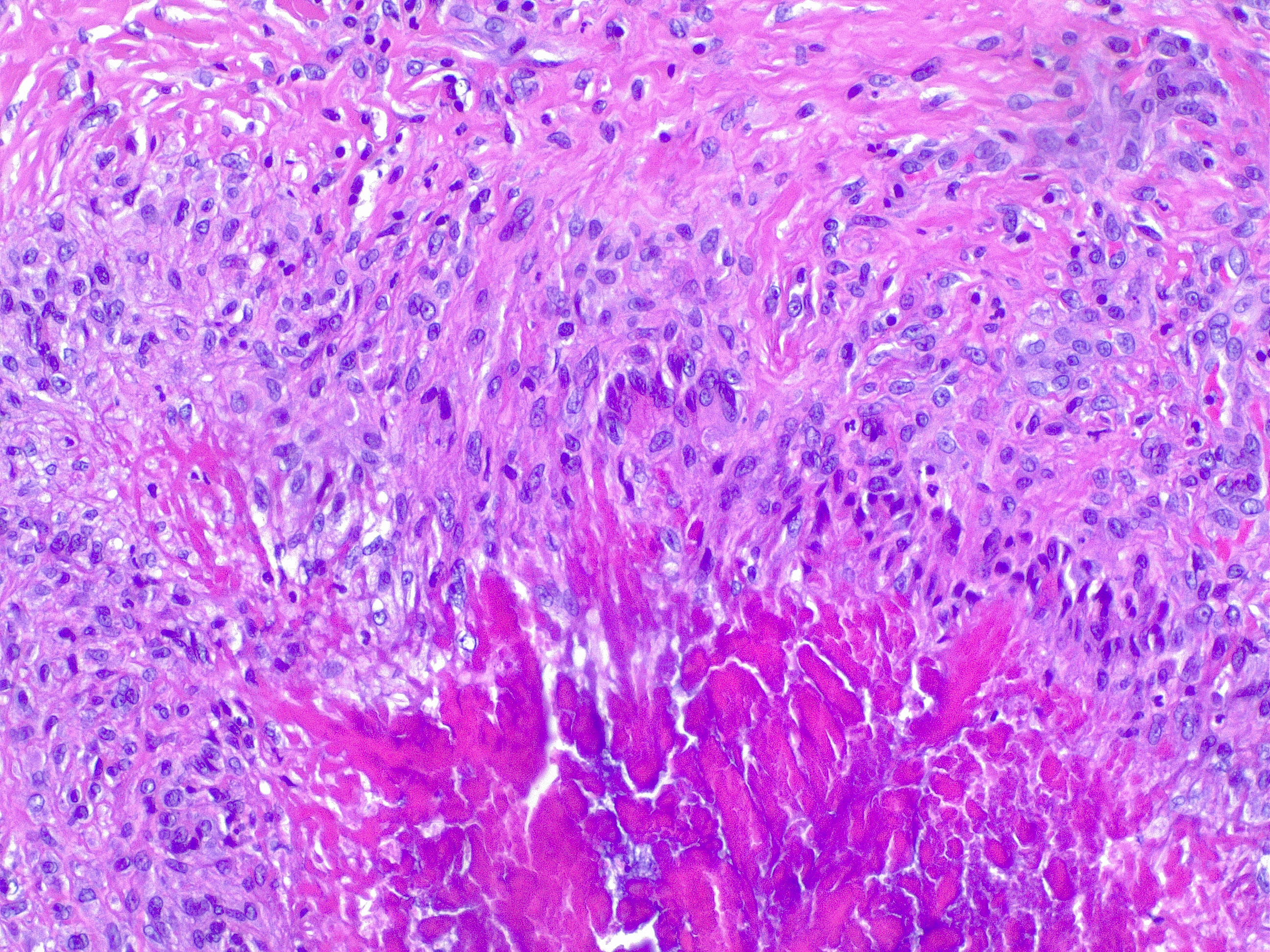
Granuloma annulare, H/E 20x. Palizading histiocytes and lymphocytes surround an area of necrobiotic collagen. Contributed by Fabiola Farci, MD
References
Klareskog L,Rönnelid J,Saevarsdottir S,Padyukov L,Alfredsson L, The importance of differences; On environment and its interactions with genes and immunity in the causation of rheumatoid arthritis. Journal of internal medicine. 2020 May [PubMed PMID: 32176395]
Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet (London, England). 2016 Oct 22:388(10055):2023-2038. doi: 10.1016/S0140-6736(16)30173-8. Epub 2016 May 3 [PubMed PMID: 27156434]
Bullock J,Rizvi SAA,Saleh AM,Ahmed SS,Do DP,Ansari RA,Ahmed J, Rheumatoid Arthritis: A Brief Overview of the Treatment. Medical principles and practice : international journal of the Kuwait University, Health Science Centre. 2018 [PubMed PMID: 30173215]
Level 3 (low-level) evidenceSparks JA, Rheumatoid Arthritis. Annals of internal medicine. 2019 Jan 1 [PubMed PMID: 30596879]
Pincus T,O'Dell JR,Kremer JM, Combination therapy with multiple disease-modifying antirheumatic drugs in rheumatoid arthritis: a preventive strategy. Annals of internal medicine. 1999 Nov 16; [PubMed PMID: 10577301]
Silman AJ,MacGregor AJ,Thomson W,Holligan S,Carthy D,Farhan A,Ollier WE, Twin concordance rates for rheumatoid arthritis: results from a nationwide study. British journal of rheumatology. 1993 Oct [PubMed PMID: 8402000]
Kłodziński Ł,Wisłowska M, Comorbidities in rheumatic arthritis. Reumatologia. 2018 [PubMed PMID: 30237627]
Gregersen PK,Silver J,Winchester RJ, The shared epitope hypothesis. An approach to understanding the molecular genetics of susceptibility to rheumatoid arthritis. Arthritis and rheumatism. 1987 Nov [PubMed PMID: 2446635]
Level 3 (low-level) evidenceWeyand CM,Hicok KC,Conn DL,Goronzy JJ, The influence of HLA-DRB1 genes on disease severity in rheumatoid arthritis. Annals of internal medicine. 1992 Nov 15; [PubMed PMID: 1416553]
Level 2 (mid-level) evidencedu Teil Espina M,Gabarrini G,Harmsen HJM,Westra J,van Winkelhoff AJ,van Dijl JM, Talk to your gut: the oral-gut microbiome axis and its immunomodulatory role in the etiology of rheumatoid arthritis. FEMS microbiology reviews. 2018 Sep 14 [PubMed PMID: 30219863]
Wu H,Liao W,Li Q,Long H,Yin H,Zhao M,Chan V,Lau CS,Lu Q, Pathogenic role of tissue-resident memory T cells in autoimmune diseases. Autoimmunity reviews. 2018 Sep [PubMed PMID: 30005862]
Okada Y,Eyre S,Suzuki A,Kochi Y,Yamamoto K, Genetics of rheumatoid arthritis: 2018 status. Annals of the rheumatic diseases. 2019 Apr [PubMed PMID: 30530827]
Dedmon LE, The genetics of rheumatoid arthritis. Rheumatology (Oxford, England). 2020 Oct 1 [PubMed PMID: 32638005]
Padyukov L, Genetics of rheumatoid arthritis. Seminars in immunopathology. 2022 Jan [PubMed PMID: 35088123]
Ciccacci C,Conigliaro P,Perricone C,Rufini S,Triggianese P,Politi C,Novelli G,Perricone R,Borgiani P, Polymorphisms in STAT-4, IL-10, PSORS1C1, PTPN2 and MIR146A genes are associated differently with prognostic factors in Italian patients affected by rheumatoid arthritis. Clinical and experimental immunology. 2016 Nov [PubMed PMID: 27342690]
Stanford SM,Maestre MF,Campbell AM,Bartok B,Kiosses WB,Boyle DL,Arnett HA,Mustelin T,Firestein GS,Bottini N, Protein tyrosine phosphatase expression profile of rheumatoid arthritis fibroblast-like synoviocytes: a novel role of SH2 domain-containing phosphatase 2 as a modulator of invasion and survival. Arthritis and rheumatism. 2013 May; [PubMed PMID: 23335101]
Stolt P,Bengtsson C,Nordmark B,Lindblad S,Lundberg I,Klareskog L,Alfredsson L,EIRA study group., Quantification of the influence of cigarette smoking on rheumatoid arthritis: results from a population based case-control study, using incident cases. Annals of the rheumatic diseases. 2003 Sep; [PubMed PMID: 12922955]
Level 2 (mid-level) evidencePadyukov L,Silva C,Stolt P,Alfredsson L,Klareskog L, A gene-environment interaction between smoking and shared epitope genes in HLA-DR provides a high risk of seropositive rheumatoid arthritis. Arthritis and rheumatism. 2004 Oct [PubMed PMID: 15476204]
Level 2 (mid-level) evidenceLinn-Rasker SP,van der Helm-van Mil AH,van Gaalen FA,Kloppenburg M,de Vries RR,le Cessie S,Breedveld FC,Toes RE,Huizinga TW, Smoking is a risk factor for anti-CCP antibodies only in rheumatoid arthritis patients who carry HLA-DRB1 shared epitope alleles. Annals of the rheumatic diseases. 2006 Mar; [PubMed PMID: 16014670]
Klareskog L,Stolt P,Lundberg K,Källberg H,Bengtsson C,Grunewald J,Rönnelid J,Harris HE,Ulfgren AK,Rantapää-Dahlqvist S,Eklund A,Padyukov L,Alfredsson L, A new model for an etiology of rheumatoid arthritis: smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis and rheumatism. 2006 Jan [PubMed PMID: 16385494]
Level 2 (mid-level) evidenceLundström E,Källberg H,Alfredsson L,Klareskog L,Padyukov L, Gene-environment interaction between the DRB1 shared epitope and smoking in the risk of anti-citrullinated protein antibody-positive rheumatoid arthritis: all alleles are important. Arthritis and rheumatism. 2009 Jun [PubMed PMID: 19479873]
Level 2 (mid-level) evidenceSugiyama D,Nishimura K,Tamaki K,Tsuji G,Nakazawa T,Morinobu A,Kumagai S, Impact of smoking as a risk factor for developing rheumatoid arthritis: a meta-analysis of observational studies. Annals of the rheumatic diseases. 2010 Jan [PubMed PMID: 19174392]
Level 1 (high-level) evidenceDerksen VFAM,Huizinga TWJ,van der Woude D, The role of autoantibodies in the pathophysiology of rheumatoid arthritis. Seminars in immunopathology. 2017 Jun [PubMed PMID: 28451788]
Cross M,Smith E,Hoy D,Carmona L,Wolfe F,Vos T,Williams B,Gabriel S,Lassere M,Johns N,Buchbinder R,Woolf A,March L, The global burden of rheumatoid arthritis: estimates from the global burden of disease 2010 study. Annals of the rheumatic diseases. 2014 Jul [PubMed PMID: 24550173]
Level 1 (high-level) evidenceMyasoedova E,Crowson CS,Kremers HM,Therneau TM,Gabriel SE, Is the incidence of rheumatoid arthritis rising?: results from Olmsted County, Minnesota, 1955-2007. Arthritis and rheumatism. 2010 Jun [PubMed PMID: 20191579]
Level 2 (mid-level) evidenceCrowson CS, Matteson EL, Myasoedova E, Michet CJ, Ernste FC, Warrington KJ, Davis JM 3rd, Hunder GG, Therneau TM, Gabriel SE. The lifetime risk of adult-onset rheumatoid arthritis and other inflammatory autoimmune rheumatic diseases. Arthritis and rheumatism. 2011 Mar:63(3):633-9. doi: 10.1002/art.30155. Epub [PubMed PMID: 21360492]
Level 3 (low-level) evidenceEriksson JK,Neovius M,Ernestam S,Lindblad S,Simard JF,Askling J, Incidence of rheumatoid arthritis in Sweden: a nationwide population-based assessment of incidence, its determinants, and treatment penetration. Arthritis care & research. 2013 Jun [PubMed PMID: 23281173]
Level 2 (mid-level) evidenceSafiri S,Kolahi AA,Hoy D,Smith E,Bettampadi D,Mansournia MA,Almasi-Hashiani A,Ashrafi-Asgarabad A,Moradi-Lakeh M,Qorbani M,Collins G,Woolf AD,March L,Cross M, Global, regional and national burden of rheumatoid arthritis 1990-2017: a systematic analysis of the Global Burden of Disease study 2017. Annals of the rheumatic diseases. 2019 Nov [PubMed PMID: 31511227]
Level 1 (high-level) evidenceAlmutairi KB,Nossent JC,Preen DB,Keen HI,Inderjeeth CA, The Prevalence of Rheumatoid Arthritis: A Systematic Review of Population-based Studies. The Journal of rheumatology. 2021 May; [PubMed PMID: 33060323]
Level 1 (high-level) evidenceAlmutairi K,Nossent J,Preen D,Keen H,Inderjeeth C, The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatology international. 2021 May; [PubMed PMID: 33175207]
Level 1 (high-level) evidenceFrisell T,Holmqvist M,Källberg H,Klareskog L,Alfredsson L,Askling J, Familial risks and heritability of rheumatoid arthritis: role of rheumatoid factor/anti-citrullinated protein antibody status, number and type of affected relatives, sex, and age. Arthritis and rheumatism. 2013 Nov [PubMed PMID: 23897126]
Level 2 (mid-level) evidencePhilippou E,Nikiphorou E, Are we really what we eat? Nutrition and its role in the onset of rheumatoid arthritis. Autoimmunity reviews. 2018 Nov [PubMed PMID: 30213695]
Qin B,Yang M,Fu H,Ma N,Wei T,Tang Q,Hu Z,Liang Y,Yang Z,Zhong R, Body mass index and the risk of rheumatoid arthritis: a systematic review and dose-response meta-analysis. Arthritis research & therapy. 2015 Mar 29 [PubMed PMID: 25890172]
Level 2 (mid-level) evidenceLi X,Sundquist J,Sundquist K, Socioeconomic and occupational risk factors for rheumatoid arthritis: a nationwide study based on hospitalizations in Sweden. The Journal of rheumatology. 2008 Jun [PubMed PMID: 18464310]
De Roos AJ,Koehoorn M,Tamburic L,Davies HW,Brauer M, Proximity to traffic, ambient air pollution, and community noise in relation to incident rheumatoid arthritis. Environmental health perspectives. 2014 Oct [PubMed PMID: 24905961]
Level 3 (low-level) evidenceNIENHUIS RL,MANDEMA E, A NEW SERUM FACTOR IN PATIENTS WITH RHEUMATOID ARTHRITIS; THE ANTIPERINUCLEAR FACTOR. Annals of the rheumatic diseases. 1964 Jul [PubMed PMID: 14178016]
Young BJ,Mallya RK,Leslie RD,Clark CJ,Hamblin TJ, Anti-keratin antibodies in rheumatoid arthritis. British medical journal. 1979 Jul 14 [PubMed PMID: 111762]
Level 3 (low-level) evidenceSebbag M,Simon M,Vincent C,Masson-Bessière C,Girbal E,Durieux JJ,Serre G, The antiperinuclear factor and the so-called antikeratin antibodies are the same rheumatoid arthritis-specific autoantibodies. The Journal of clinical investigation. 1995 Jun [PubMed PMID: 7539459]
Hoet RM,Boerbooms AM,Arends M,Ruiter DJ,van Venrooij WJ, Antiperinuclear factor, a marker autoantibody for rheumatoid arthritis: colocalisation of the perinuclear factor and profilaggrin. Annals of the rheumatic diseases. 1991 Sep; [PubMed PMID: 1718228]
Schellekens GA,Visser H,de Jong BA,van den Hoogen FH,Hazes JM,Breedveld FC,van Venrooij WJ, The diagnostic properties of rheumatoid arthritis antibodies recognizing a cyclic citrullinated peptide. Arthritis and rheumatism. 2000 Jan [PubMed PMID: 10643712]
van Delft MAM,Huizinga TWJ, An overview of autoantibodies in rheumatoid arthritis. Journal of autoimmunity. 2020 Jun [PubMed PMID: 31911013]
Level 3 (low-level) evidenceMakrygiannakis D,Hermansson M,Ulfgren AK,Nicholas AP,Zendman AJ,Eklund A,Grunewald J,Skold CM,Klareskog L,Catrina AI, Smoking increases peptidylarginine deiminase 2 enzyme expression in human lungs and increases citrullination in BAL cells. Annals of the rheumatic diseases. 2008 Oct [PubMed PMID: 18413445]
Curran AM,Naik P,Giles JT,Darrah E, PAD enzymes in rheumatoid arthritis: pathogenic effectors and autoimmune targets. Nature reviews. Rheumatology. 2020 Jun [PubMed PMID: 32341463]
Gómez-Bañuelos E,Mukherjee A,Darrah E,Andrade F, Rheumatoid Arthritis-Associated Mechanisms of {i}Porphyromonas gingivalis{/i} and {i}Aggregatibacter actinomycetemcomitans{/i}. Journal of clinical medicine. 2019 Aug 26; [PubMed PMID: 31454946]
Volkov M,van Schie KA,van der Woude D, Autoantibodies and B Cells: The ABC of rheumatoid arthritis pathophysiology. Immunological reviews. 2020 Mar [PubMed PMID: 31845355]
McInnes IB,Schett G, Pathogenetic insights from the treatment of rheumatoid arthritis. Lancet (London, England). 2017 Jun 10 [PubMed PMID: 28612747]
Nielen MM, van Schaardenburg D, Reesink HW, van de Stadt RJ, van der Horst-Bruinsma IE, de Koning MH, Habibuw MR, Vandenbroucke JP, Dijkmans BA. Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis and rheumatism. 2004 Feb:50(2):380-6 [PubMed PMID: 14872479]
Level 2 (mid-level) evidencevan Steenbergen HW,Huizinga TW,van der Helm-van Mil AH, The preclinical phase of rheumatoid arthritis: what is acknowledged and what needs to be assessed? Arthritis and rheumatism. 2013 Sep; [PubMed PMID: 23686440]
Mankia K,Emery P, Preclinical Rheumatoid Arthritis: Progress Toward Prevention. Arthritis & rheumatology (Hoboken, N.J.). 2016 Apr [PubMed PMID: 26814677]
Wegner N,Lundberg K,Kinloch A,Fisher B,Malmström V,Feldmann M,Venables PJ, Autoimmunity to specific citrullinated proteins gives the first clues to the etiology of rheumatoid arthritis. Immunological reviews. 2010 Jan; [PubMed PMID: 20192991]
Level 3 (low-level) evidenceFang Q,Zhou C,Nandakumar KS, Molecular and Cellular Pathways Contributing to Joint Damage in Rheumatoid Arthritis. Mediators of inflammation. 2020 [PubMed PMID: 32256192]
López-Mejías R,David Carmona F,Genre F,Remuzgo-Martínez S,González-Juanatey C,Corrales A,Vicente EF,Pulito-Cueto V,Miranda-Filloy JA,Ramírez Huaranga MA,Blanco R,Robustillo-Villarino M,Rodríguez-Carrio J,Alperi-López M,Alegre-Sancho JJ,Mijares V,Lera-Gómez L,Pérez-Pampín E,González A,Ortega-Castro R,López-Pedrera C,García Vivar ML,Gómez-Arango C,Raya E,Narvaez J,Balsa A,López-Longo FJ,Carreira P,González-Álvaro I,Rodríguez-Rodríguez L,Fernández-Gutiérrez B,Ferraz-Amaro I,Gualillo O,Castañeda S,Martín J,Llorca J,González-Gay MA, A genome-wide association study identifies a 3'UTR genetic variant of RARB associated with carotid intima-media thickness in rheumatoid arthritis. Arthritis [PubMed PMID: 30251476]
de Hair MJ, van de Sande MG, Ramwadhdoebe TH, Hansson M, Landewé R, van der Leij C, Maas M, Serre G, van Schaardenburg D, Klareskog L, Gerlag DM, van Baarsen LG, Tak PP. Features of the synovium of individuals at risk of developing rheumatoid arthritis: implications for understanding preclinical rheumatoid arthritis. Arthritis & rheumatology (Hoboken, N.J.). 2014 Mar:66(3):513-22. doi: 10.1002/art.38273. Epub [PubMed PMID: 24574210]
Level 3 (low-level) evidenceMcInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. The New England journal of medicine. 2011 Dec 8:365(23):2205-19. doi: 10.1056/NEJMra1004965. Epub [PubMed PMID: 22150039]
de Brito Rocha S,Baldo DC,Andrade LEC, Clinical and pathophysiologic relevance of autoantibodies in rheumatoid arthritis. Advances in rheumatology (London, England). 2019 Jan 17; [PubMed PMID: 30657101]
Level 3 (low-level) evidenceWeyand CM,Goronzy JJ, The immunology of rheumatoid arthritis. Nature immunology. 2021 Jan [PubMed PMID: 33257900]
Lin YJ,Anzaghe M,Schülke S, Update on the Pathomechanism, Diagnosis, and Treatment Options for Rheumatoid Arthritis. Cells. 2020 Apr 3 [PubMed PMID: 32260219]
Kondo N,Kuroda T,Kobayashi D, Cytokine Networks in the Pathogenesis of Rheumatoid Arthritis. International journal of molecular sciences. 2021 Oct 10 [PubMed PMID: 34681582]
Lally F,Smith E,Filer A,Stone MA,Shaw JS,Nash GB,Buckley CD,Rainger GE, A novel mechanism of neutrophil recruitment in a coculture model of the rheumatoid synovium. Arthritis and rheumatism. 2005 Nov [PubMed PMID: 16255036]
Demasi M,Cleland LG,Cook-Johnson RJ,James MJ, Effects of hypoxia on the expression and activity of cyclooxygenase 2 in fibroblast-like synoviocytes: interactions with monocyte-derived soluble mediators. Arthritis and rheumatism. 2004 Aug [PubMed PMID: 15334456]
Chua-Aguilera CJ,Möller B,Yawalkar N, Skin Manifestations of Rheumatoid Arthritis, Juvenile Idiopathic Arthritis, and Spondyloarthritides. Clinical reviews in allergy & immunology. 2017 Dec [PubMed PMID: 28752373]
Lee DM,Weinblatt ME, Rheumatoid arthritis. Lancet (London, England). 2001 Sep 15 [PubMed PMID: 11567728]
Koskinen E,Hannonen P,Sokka T, Palindromic rheumatism: longterm outcomes of 60 patients diagnosed in 1967-84. The Journal of rheumatology. 2009 Sep [PubMed PMID: 19648311]
Level 2 (mid-level) evidenceGonzalez-Lopez L,Gamez-Nava JI,Jhangri G,Russell AS,Suarez-Almazor ME, Decreased progression to rheumatoid arthritis or other connective tissue diseases in patients with palindromic rheumatism treated with antimalarials. The Journal of rheumatology. 2000 Jan [PubMed PMID: 10648016]
Level 2 (mid-level) evidenceLehtinen JT,Kaarela K,Belt EA,Kautiainen HJ,Kauppi MJ,Lehto MU, Incidence of acromioclavicular joint involvement in rheumatoid arthritis: a 15 year endpoint study. The Journal of rheumatology. 1999 Jun [PubMed PMID: 10381036]
Level 2 (mid-level) evidenceSayah A,English JC 3rd, Rheumatoid arthritis: a review of the cutaneous manifestations. Journal of the American Academy of Dermatology. 2005 Aug [PubMed PMID: 16021111]
Bongartz T,Nannini C,Medina-Velasquez YF,Achenbach SJ,Crowson CS,Ryu JH,Vassallo R,Gabriel SE,Matteson EL, Incidence and mortality of interstitial lung disease in rheumatoid arthritis: a population-based study. Arthritis and rheumatism. 2010 Jun; [PubMed PMID: 20155830]
Level 2 (mid-level) evidenceSparks JA,Jin Y,Cho SK,Vine S,Desai R,Doyle TJ,Kim SC, Prevalence, incidence and cause-specific mortality of rheumatoid arthritis-associated interstitial lung disease among older rheumatoid arthritis patients. Rheumatology (Oxford, England). 2021 Aug 2 [PubMed PMID: 33462611]
Samhouri BF,Vassallo R,Achenbach SJ,Kronzer VL,Davis JM 3rd,Myasoedova E,Crowson CS, Incidence, Risk Factors, and Mortality of Clinical and Subclinical Rheumatoid Arthritis-Associated Interstitial Lung Disease: A Population-Based Cohort. Arthritis care & research. 2022 Jan 7 [PubMed PMID: 34995017]
Correia CS,Briones MR,Guo R,Ostrowski RA, Elevated anti-cyclic citrullinated peptide antibody titer is associated with increased risk for interstitial lung disease. Clinical rheumatology. 2019 Apr [PubMed PMID: 30645754]
Castellanos-Moreira R,Rodriguez-Garcia SC,Cabrera-Villalba S,Gomara MJ,Salvador G,Ruiz-Esquide V,Ramirez J,Inciarte-Mundo J,Morla R,Garcia-Moreno C,Cuervo A,Gómez-Puerta JA,Cañete JD,Haro I,Sanmarti R, Anti-carbamylated protein antibody isotype pattern differs between palindromic rheumatism and rheumatoid arthritis. Therapeutic advances in musculoskeletal disease. 2020; [PubMed PMID: 33354232]
Level 3 (low-level) evidenceEngland BR,Duryee MJ,Roul P,Mahajan TD,Singh N,Poole JA,Ascherman DP,Caplan L,Demoruelle MK,Deane KD,Klassen LW,Thiele GM,Mikuls TR, Malondialdehyde-Acetaldehyde Adducts and Antibody Responses in Rheumatoid Arthritis-Associated Interstitial Lung Disease. Arthritis & rheumatology (Hoboken, N.J.). 2019 Sep [PubMed PMID: 30933423]
Juge PA,Lee JS,Ebstein E,Furukawa H,Dobrinskikh E,Gazal S,Kannengiesser C,Ottaviani S,Oka S,Tohma S,Tsuchiya N,Rojas-Serrano J,González-Pérez MI,Mejía M,Buendía-Roldán I,Falfán-Valencia R,Ambrocio-Ortiz E,Manali E,Papiris SA,Karageorgas T,Boumpas D,Antoniou K,van Moorsel CHM,van der Vis J,de Man YA,Grutters JC,Wang Y,Borie R,Wemeau-Stervinou L,Wallaert B,Flipo RM,Nunes H,Valeyre D,Saidenberg-Kermanac'h N,Boissier MC,Marchand-Adam S,Frazier A,Richette P,Allanore Y,Sibilia J,Dromer C,Richez C,Schaeverbeke T,Lioté H,Thabut G,Nathan N,Amselem S,Soubrier M,Cottin V,Clément A,Deane K,Walts AD,Fingerlin T,Fischer A,Ryu JH,Matteson EL,Niewold TB,Assayag D,Gross A,Wolters P,Schwarz MI,Holers M,Solomon JJ,Doyle T,Rosas IO,Blauwendraat C,Nalls MA,Debray MP,Boileau C,Crestani B,Schwartz DA,Dieudé P, MUC5B Promoter Variant and Rheumatoid Arthritis with Interstitial Lung Disease. The New England journal of medicine. 2018 Dec 6 [PubMed PMID: 30345907]
Conforti A,Di Cola I,Pavlych V,Ruscitti P,Berardicurti O,Ursini F,Giacomelli R,Cipriani P, Beyond the joints, the extra-articular manifestations in rheumatoid arthritis. Autoimmunity reviews. 2021 Feb [PubMed PMID: 33346115]
Abdulqader Y,Al-Ani M,Parperis K, Rheumatoid vasculitis: early presentation of rheumatoid arthritis. BMJ case reports. 2016 Nov 8 [PubMed PMID: 27873751]
Level 3 (low-level) evidenceNishimura K, Sugiyama D, Kogata Y, Tsuji G, Nakazawa T, Kawano S, Saigo K, Morinobu A, Koshiba M, Kuntz KM, Kamae I, Kumagai S. Meta-analysis: diagnostic accuracy of anti-cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Annals of internal medicine. 2007 Jun 5:146(11):797-808 [PubMed PMID: 17548411]
Level 1 (high-level) evidenceRantapää-Dahlqvist S,de Jong BA,Berglin E,Hallmans G,Wadell G,Stenlund H,Sundin U,van Venrooij WJ, Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis and rheumatism. 2003 Oct; [PubMed PMID: 14558078]
Level 2 (mid-level) evidencevan Gaalen FA,Linn-Rasker SP,van Venrooij WJ,de Jong BA,Breedveld FC,Verweij CL,Toes RE,Huizinga TW, Autoantibodies to cyclic citrullinated peptides predict progression to rheumatoid arthritis in patients with undifferentiated arthritis: a prospective cohort study. Arthritis and rheumatism. 2004 Mar [PubMed PMID: 15022309]
Level 2 (mid-level) evidenceAvouac J,Gossec L,Dougados M, Diagnostic and predictive value of anti-cyclic citrullinated protein antibodies in rheumatoid arthritis: a systematic literature review. Annals of the rheumatic diseases. 2006 Jul; [PubMed PMID: 16606649]
Level 2 (mid-level) evidenceRamos-Remus C,Castillo-Ortiz JD,Aguilar-Lozano L,Padilla-Ibarra J,Sandoval-Castro C,Vargas-Serafin CO,de la Mora-Molina H,Ramos-Gomez A,Sanchez-Ortiz A,Avila-Armengol H,Aceves-Avila FJ, Autoantibodies in prediction of the development of rheumatoid arthritis among healthy relatives of patients with the disease. Arthritis & rheumatology (Hoboken, N.J.). 2015 Nov [PubMed PMID: 26245885]
Bemis EA,Demoruelle MK,Seifert JA,Polinski KJ,Weisman MH,Buckner JH,Gregersen PK,Mikuls TR,ODell JR,Keating RM,Deane KD,Holers VM,Norris JM, Factors associated with progression to inflammatory arthritis in first-degree relatives of individuals with RA following autoantibody positive screening in a non-clinical setting. Annals of the rheumatic diseases. 2021 Feb [PubMed PMID: 32928740]
Kortekangas P,Aro HT,Tuominen J,Toivanen A, Synovial fluid leukocytosis in bacterial arthritis vs. reactive arthritis and rheumatoid arthritis in the adult knee. Scandinavian journal of rheumatology. 1992 [PubMed PMID: 1475638]
Level 2 (mid-level) evidenceFuchs HA,Kaye JJ,Callahan LF,Nance EP,Pincus T, Evidence of significant radiographic damage in rheumatoid arthritis within the first 2 years of disease. The Journal of rheumatology. 1989 May; [PubMed PMID: 2754663]
McQueen FM, The use of MRI in early RA. Rheumatology (Oxford, England). 2008 Nov [PubMed PMID: 18701537]
McQueen FM,Stewart N,Crabbe J,Robinson E,Yeoman S,Tan PL,McLean L, Magnetic resonance imaging of the wrist in early rheumatoid arthritis reveals progression of erosions despite clinical improvement. Annals of the rheumatic diseases. 1999 Mar [PubMed PMID: 10364913]
Cornec D,Varache S,Morvan J,Devauchelle-Pensec V,Berthelot JM,Le Henaff-Bourhis C,Hoang S,Martin A,Chalès G,Jousse-Joulin S,Saraux A, Comparison of ACR 1987 and ACR/EULAR 2010 criteria for predicting a 10-year diagnosis of rheumatoid arthritis. Joint bone spine. 2012 Dec; [PubMed PMID: 22405855]
Level 2 (mid-level) evidenceAletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, Birnbaum NS, Burmester GR, Bykerk VP, Cohen MD, Combe B, Costenbader KH, Dougados M, Emery P, Ferraccioli G, Hazes JM, Hobbs K, Huizinga TW, Kavanaugh A, Kay J, Kvien TK, Laing T, Mease P, Ménard HA, Moreland LW, Naden RL, Pincus T, Smolen JS, Stanislawska-Biernat E, Symmons D, Tak PP, Upchurch KS, Vencovský J, Wolfe F, Hawker G. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis and rheumatism. 2010 Sep:62(9):2569-81. doi: 10.1002/art.27584. Epub [PubMed PMID: 20872595]
Smolen JS,Breedveld FC,Burmester GR,Bykerk V,Dougados M,Emery P,Kvien TK,Navarro-Compán MV,Oliver S,Schoels M,Scholte-Voshaar M,Stamm T,Stoffer M,Takeuchi T,Aletaha D,Andreu JL,Aringer M,Bergman M,Betteridge N,Bijlsma H,Burkhardt H,Cardiel M,Combe B,Durez P,Fonseca JE,Gibofsky A,Gomez-Reino JJ,Graninger W,Hannonen P,Haraoui B,Kouloumas M,Landewe R,Martin-Mola E,Nash P,Ostergaard M,Östör A,Richards P,Sokka-Isler T,Thorne C,Tzioufas AG,van Vollenhoven R,de Wit M,van der Heijde D, Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Annals of the rheumatic diseases. 2016 Jan; [PubMed PMID: 25969430]
Anderson J,Caplan L,Yazdany J,Robbins ML,Neogi T,Michaud K,Saag KG,O'Dell JR,Kazi S, Rheumatoid arthritis disease activity measures: American College of Rheumatology recommendations for use in clinical practice. Arthritis care [PubMed PMID: 22473918]
Level 1 (high-level) evidenceEngland BR,Tiong BK,Bergman MJ,Curtis JR,Kazi S,Mikuls TR,O'Dell JR,Ranganath VK,Limanni A,Suter LG,Michaud K, 2019 Update of the American College of Rheumatology Recommended Rheumatoid Arthritis Disease Activity Measures. Arthritis care & research. 2019 Dec [PubMed PMID: 31709779]
Singh JA, Saag KG, Bridges SL Jr, Akl EA, Bannuru RR, Sullivan MC, Vaysbrot E, McNaughton C, Osani M, Shmerling RH, Curtis JR, Furst DE, Parks D, Kavanaugh A, O'Dell J, King C, Leong A, Matteson EL, Schousboe JT, Drevlow B, Ginsberg S, Grober J, St Clair EW, Tindall E, Miller AS, McAlindon T. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & rheumatology (Hoboken, N.J.). 2016 Jan:68(1):1-26. doi: 10.1002/art.39480. Epub 2015 Nov 6 [PubMed PMID: 26545940]
Solomon DH,Husni ME,Wolski KE,Wisniewski LM,Borer JS,Graham DY,Libby P,Lincoff AM,Lüscher TF,Menon V,Yeomans ND,Wang Q,Bao W,Berger MF,Nissen SE,PRECISION Trial Investigators., Differences in Safety of Nonsteroidal Antiinflammatory Drugs in Patients With Osteoarthritis and Patients With Rheumatoid Arthritis: A Randomized Clinical Trial. Arthritis & rheumatology (Hoboken, N.J.). 2018 Apr [PubMed PMID: 29266879]
Level 1 (high-level) evidenceSolomon DH,Husni ME,Libby PA,Yeomans ND,Lincoff AM,Lϋscher TF,Menon V,Brennan DM,Wisniewski LM,Nissen SE,Borer JS, The Risk of Major NSAID Toxicity with Celecoxib, Ibuprofen, or Naproxen: A Secondary Analysis of the PRECISION Trial. The American journal of medicine. 2017 Dec [PubMed PMID: 28756267]
Burmester G,Lanas A,Biasucci L,Hermann M,Lohmander S,Olivieri I,Scarpignato C,Smolen J,Hawkey C,Bajkowski A,Berenbaum F,Breedveld F,Dieleman P,Dougados M,MacDonald T,Mola EM,Mets T,Van den Noortgate N,Stoevelaar H, The appropriate use of non-steroidal anti-inflammatory drugs in rheumatic disease: opinions of a multidisciplinary European expert panel. Annals of the rheumatic diseases. 2011 May [PubMed PMID: 20833736]
Level 3 (low-level) evidenceAshworth NL,Peloso PM,Muhajarine N,Stang M, A population based historical cohort study of the mortality associated with nabumetone, Arthrotec, diclofenac, and naproxen. The Journal of rheumatology. 2004 May; [PubMed PMID: 15124256]
Level 2 (mid-level) evidencevan Everdingen AA,Jacobs JW,Siewertsz Van Reesema DR,Bijlsma JW, Low-dose prednisone therapy for patients with early active rheumatoid arthritis: clinical efficacy, disease-modifying properties, and side effects: a randomized, double-blind, placebo-controlled clinical trial. Annals of internal medicine. 2002 Jan 1 [PubMed PMID: 11777359]
Level 1 (high-level) evidenceBakker MF,Jacobs JW,Welsing PM,Verstappen SM,Tekstra J,Ton E,Geurts MA,van der Werf JH,van Albada-Kuipers GA,Jahangier-de Veen ZN,van der Veen MJ,Verhoef CM,Lafeber FP,Bijlsma JW,Utrecht Rheumatoid Arthritis Cohort Study Group., Low-dose prednisone inclusion in a methotrexate-based, tight control strategy for early rheumatoid arthritis: a randomized trial. Annals of internal medicine. 2012 Mar 6 [PubMed PMID: 22393128]
Level 1 (high-level) evidenceKrause D,Mai A,Klaassen-Mielke R,Timmesfeld N,Trampisch U,Rudolf H,Baraliakos X,Schmitz E,Fendler C,Klink C,Boeddeker S,Saracbasi-Zender E,Christoph HJ,Igelmann M,Menne HJ,Schmid A,Rau R,Wassenberg S,Sonuc N,Ose C,Schade-Brittinger C,Trampisch HJ,Braun J, The Efficacy of Short-Term Bridging Strategies With High- and Low-Dose Prednisolone on Radiographic and Clinical Outcomes in Active Early Rheumatoid Arthritis: A Double-Blind, Randomized, Placebo-Controlled Trial. Arthritis & rheumatology (Hoboken, N.J.). 2022 Oct [PubMed PMID: 35643951]
Level 1 (high-level) evidenceVisser K,van der Heijde D, Optimal dosage and route of administration of methotrexate in rheumatoid arthritis: a systematic review of the literature. Annals of the rheumatic diseases. 2009 Jul; [PubMed PMID: 19033290]
Level 1 (high-level) evidenceBraun J,Kästner P,Flaxenberg P,Währisch J,Hanke P,Demary W,von Hinüber U,Rockwitz K,Heitz W,Pichlmeier U,Guimbal-Schmolck C,Brandt A,MC-MTX.6/RH Study Group., Comparison of the clinical efficacy and safety of subcutaneous versus oral administration of methotrexate in patients with active rheumatoid arthritis: results of a six-month, multicenter, randomized, double-blind, controlled, phase IV trial. Arthritis and rheumatism. 2008 Jan; [PubMed PMID: 18163521]
Level 1 (high-level) evidenceHoekstra M,Haagsma C,Neef C,Proost J,Knuif A,van de Laar M, Splitting high-dose oral methotrexate improves bioavailability: a pharmacokinetic study in patients with rheumatoid arthritis. The Journal of rheumatology. 2006 Mar [PubMed PMID: 16463431]
O'Dell JR,Leff R,Paulsen G,Haire C,Mallek J,Eckhoff PJ,Fernandez A,Blakely K,Wees S,Stoner J,Hadley S,Felt J,Palmer W,Waytz P,Churchill M,Klassen L,Moore G, Treatment of rheumatoid arthritis with methotrexate and hydroxychloroquine, methotrexate and sulfasalazine, or a combination of the three medications: results of a two-year, randomized, double-blind, placebo-controlled trial. Arthritis and rheumatism. 2002 May [PubMed PMID: 12115219]
Level 1 (high-level) evidenceO'Dell JR,Mikuls TR,Taylor TH,Ahluwalia V,Brophy M,Warren SR,Lew RA,Cannella AC,Kunkel G,Phibbs CS,Anis AH,Leatherman S,Keystone E,CSP 551 RACAT Investigators., Therapies for active rheumatoid arthritis after methotrexate failure. The New England journal of medicine. 2013 Jul 25; [PubMed PMID: 23755969]
Level 1 (high-level) evidenceSauer BC,Teng CC,Tang D,Leng J,Curtis JR,Mikuls TR,Harrison DJ,Cannon GW, Persistence With Conventional Triple Therapy Versus a Tumor Necrosis Factor Inhibitor and Methotrexate in US Veterans With Rheumatoid Arthritis. Arthritis care & research. 2017 Mar [PubMed PMID: 27273801]
Erhardt DP,Cannon GW,Teng CC,Mikuls TR,Curtis JR,Sauer BC, Low Persistence Rates in Patients With Rheumatoid Arthritis Treated With Triple Therapy and Adverse Drug Events Associated With Sulfasalazine. Arthritis care & research. 2019 Oct [PubMed PMID: 30221485]
Curtis JR,Palmer JL,Reed GW,Greenberg J,Pappas DA,Harrold LR,Kremer JM, Real-World Outcomes Associated With Methotrexate, Sulfasalazine, and Hydroxychloroquine Triple Therapy Versus Tumor Necrosis Factor Inhibitor/Methotrexate Combination Therapy in Patients With Rheumatoid Arthritis. Arthritis care & research. 2021 Aug [PubMed PMID: 32374918]
Karlsson JA,Neovius M,Nilsson JÅ,Petersson IF,Bratt J,van Vollenhoven RF,Ernestam S,Geborek P, Addition of infliximab compared with addition of sulfasalazine and hydroxychloroquine to methotrexate in early rheumatoid arthritis: 2-year quality-of-life results of the randomised, controlled, SWEFOT trial. Annals of the rheumatic diseases. 2013 Dec [PubMed PMID: 23196701]
Level 1 (high-level) evidenceGarcês S,Demengeot J,Benito-Garcia E, The immunogenicity of anti-TNF therapy in immune-mediated inflammatory diseases: a systematic review of the literature with a meta-analysis. Annals of the rheumatic diseases. 2013 Dec; [PubMed PMID: 23223420]
Level 1 (high-level) evidencePorter D,van Melckebeke J,Dale J,Messow CM,McConnachie A,Walker A,Munro R,McLaren J,McRorie E,Packham J,Buckley CD,Harvie J,Taylor P,Choy E,Pitzalis C,McInnes IB, Tumour necrosis factor inhibition versus rituximab for patients with rheumatoid arthritis who require biological treatment (ORBIT): an open-label, randomised controlled, non-inferiority, trial. Lancet (London, England). 2016 Jul 16 [PubMed PMID: 27197690]
Level 1 (high-level) evidenceGenovese MC,Pacheco-Tena C,Covarrubias A,Leon G,Mysler E,Keiserman M,Valente RM,Nash P,Simon-Campos JA,Box J,Legerton CW 3rd,Nasonov E,Durez P,Elegbe A,Wong R,Li X,Banerjee S,Alten R, Longterm Safety and Efficacy of Subcutaneous Abatacept in Patients with Rheumatoid Arthritis: 5-year Results from a Phase IIIb Trial. The Journal of rheumatology. 2018 Aug [PubMed PMID: 29657147]
Smolen JS,Schoels MM,Nishimoto N,Breedveld FC,Burmester GR,Dougados M,Emery P,Ferraccioli G,Gabay C,Gibofsky A,Gomez-Reino JJ,Jones G,Kvien TK,Murakami M,Betteridge N,Bingham CO 3rd,Bykerk V,Choy EH,Combe B,Cutolo M,Graninger W,Lanas A,Martin-Mola E,Montecucco C,Ostergaard M,Pavelka K,Rubbert-Roth A,Sattar N,Scholte-Voshaar M,Tanaka Y,Trauner M,Valentini G,Winthrop KL,de Wit M,van der Heijde D, Consensus statement on blocking the effects of interleukin-6 and in particular by interleukin-6 receptor inhibition in rheumatoid arthritis and other inflammatory conditions. Annals of the rheumatic diseases. 2013 Apr; [PubMed PMID: 23172750]
Level 3 (low-level) evidenceFleischmann R,van Adelsberg J,Lin Y,Castelar-Pinheiro GD,Brzezicki J,Hrycaj P,Graham NM,van Hoogstraten H,Bauer D,Burmester GR, Sarilumab and Nonbiologic Disease-Modifying Antirheumatic Drugs in Patients With Active Rheumatoid Arthritis and Inadequate Response or Intolerance to Tumor Necrosis Factor Inhibitors. Arthritis & rheumatology (Hoboken, N.J.). 2017 Feb [PubMed PMID: 27860410]
Wallenstein GV,Kanik KS,Wilkinson B,Cohen S,Cutolo M,Fleischmann RM,Genovese MC,Gomez Reino J,Gruben D,Kremer J,Krishnaswami S,Lee EB,Pascual-Ramos V,Strand V,Zwillich SH, Effects of the oral Janus kinase inhibitor tofacitinib on patient-reported outcomes in patients with active rheumatoid arthritis: results of two Phase 2 randomised controlled trials. Clinical and experimental rheumatology. 2016 May-Jun [PubMed PMID: 27156561]
Level 1 (high-level) evidenceGwinnutt JM,Symmons DPM,MacGregor AJ,Chipping JR,Marshall T,Lunt M,Verstappen SMM, Twenty-Year Outcome and Association Between Early Treatment and Mortality and Disability in an Inception Cohort of Patients With Rheumatoid Arthritis: Results From the Norfolk Arthritis Register. Arthritis & rheumatology (Hoboken, N.J.). 2017 Aug [PubMed PMID: 28425173]
Paul BJ,Kandy HI,Krishnan V, Pre-rheumatoid arthritis and its prevention. European journal of rheumatology. 2017 Jun [PubMed PMID: 28638695]
Holmqvist M,Mantel Ä,Wållberg-Jonsson S,James S,Jernberg T,Askling J, Findings on Coronary Angiographies in Patients With Rheumatoid Arthritis and Ischemic Heart Disease: Are They Different From Patients Without Rheumatoid Arthritis? Arthritis care & research. 2021 May [PubMed PMID: 33285616]
Solomon DH,Goodson NJ,Katz JN,Weinblatt ME,Avorn J,Setoguchi S,Canning C,Schneeweiss S, Patterns of cardiovascular risk in rheumatoid arthritis. Annals of the rheumatic diseases. 2006 Dec; [PubMed PMID: 16793844]
Level 2 (mid-level) evidenceMartin-Trujillo A,van Rietschoten JG,Timmer TC,Rodríguez FM,Huizinga TW,Tak PP,Marsal S,Ibrahim SM,Dijkmans BA,van der Pouw Kraan TC,Verweij CL, Loss of imprinting of IGF2 characterises high IGF2 mRNA-expressing type of fibroblast-like synoviocytes in rheumatoid arthritis. Annals of the rheumatic diseases. 2010 Jun; [PubMed PMID: 19556211]
Atzeni F,Masala IF,di Franco M,Sarzi-Puttini P, Infections in rheumatoid arthritis. Current opinion in rheumatology. 2017 Jul; [PubMed PMID: 28422773]
Level 3 (low-level) evidenceCarbone F,Bonaventura A,Liberale L,Paolino S,Torre F,Dallegri F,Montecucco F,Cutolo M, Atherosclerosis in Rheumatoid Arthritis: Promoters and Opponents. Clinical reviews in allergy & immunology. 2020 Feb [PubMed PMID: 30259381]
Nicolau J,Lequerré T,Bacquet H,Vittecoq O, Rheumatoid arthritis, insulin resistance, and diabetes. Joint bone spine. 2017 Jul [PubMed PMID: 27777170]
Naranjo A,Sokka T,Descalzo MA,Calvo-Alén J,Hørslev-Petersen K,Luukkainen RK,Combe B,Burmester GR,Devlin J,Ferraccioli G,Morelli A,Hoekstra M,Majdan M,Sadkiewicz S,Belmonte M,Holmqvist AC,Choy E,Tunc R,Dimic A,Bergman M,Toloza S,Pincus T,QUEST-RA Group., Cardiovascular disease in patients with rheumatoid arthritis: results from the QUEST-RA study. Arthritis research & therapy. 2008 [PubMed PMID: 18325087]
Level 2 (mid-level) evidenceOzen G,Pedro S,Michaud K, The Risk of Cardiovascular Events Associated With Disease-modifying Antirheumatic Drugs in Rheumatoid Arthritis. The Journal of rheumatology. 2021 May; [PubMed PMID: 32801134]
Xie F,Chen L,Yun H,Levitan EB,Curtis JR, Benefits of Methotrexate Use on Cardiovascular Disease Risk Among Rheumatoid Arthritis Patients Initiating Biologic Disease-modifying Antirheumatic Drugs. The Journal of rheumatology. 2021 Jun [PubMed PMID: 33060309]
Klein A,Polliack A,Gafter-Gvili A, Rheumatoid arthritis and lymphoma: Incidence, pathogenesis, biology, and outcome. Hematological oncology. 2018 Dec; [PubMed PMID: 29862535]
Baecklund E,Iliadou A,Askling J,Ekbom A,Backlin C,Granath F,Catrina AI,Rosenquist R,Feltelius N,Sundström C,Klareskog L, Association of chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis and rheumatism. 2006 Mar [PubMed PMID: 16508929]
Level 2 (mid-level) evidenceHellgren K,Baecklund E,Backlin C,Sundstrom C,Smedby KE,Askling J, Rheumatoid Arthritis and Risk of Malignant Lymphoma: Is the Risk Still Increased? Arthritis [PubMed PMID: 27992692]
Jin S,Hsieh E,Peng L,Yu C,Wang Y,Wu C,Wang Q,Li M,Zeng X, Incidence of fractures among patients with rheumatoid arthritis: a systematic review and meta-analysis. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2018 Jun [PubMed PMID: 29546507]
Level 1 (high-level) evidenceKim SC,Schneeweiss S,Liu J,Solomon DH, Risk of venous thromboembolism in patients with rheumatoid arthritis. Arthritis care & research. 2013 Oct [PubMed PMID: 23666917]
Level 2 (mid-level) evidenceBacani AK,Gabriel SE,Crowson CS,Heit JA,Matteson EL, Noncardiac vascular disease in rheumatoid arthritis: increase in venous thromboembolic events? Arthritis and rheumatism. 2012 Jan [PubMed PMID: 21905005]
Level 2 (mid-level) evidenceLiang H,Danwada R,Guo D,Curtis JR,Kilpatrick RD,Hendrickson B,Islam SS, Incidence of inpatient venous thromboembolism in treated patients with rheumatoid arthritis and the association with switching biologic or targeted synthetic disease-modifying antirheumatic drugs (DMARDs) in the real-world setting. RMD open. 2019 [PubMed PMID: 31673413]
Matcham F,Rayner L,Steer S,Hotopf M, The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis. Rheumatology (Oxford, England). 2013 Dec [PubMed PMID: 24003249]
Level 2 (mid-level) evidenceMuñoz-Fernández S,Otón-Sánchez T,Carmona L,Calvo-Alén J,Escudero A,Narváez J,Rodríguez Heredia JM,Romero Yuste S,Vela P,Luján Valdés S,Royo García A,Baquero JL, Use of prognostic factors of rheumatoid arthritis in clinical practice and perception of their predictive capacity before and after exposure to evidence. Rheumatology international. 2018 Sep 24 [PubMed PMID: 30251128]
Solomon DH,Yu Z,Katz JN,Bitton A,Corrigan C,Fraenkel L,Harrold LR,Smolen JS,Losina E,Lu B, Adverse Events and Resource Use Before and After Treat-to-Target in Rheumatoid Arthritis: A Post Hoc Analysis of a Randomized Controlled Trial. Arthritis care & research. 2019 Sep [PubMed PMID: 30221841]
Level 1 (high-level) evidence