Introduction
Antibodies are naturally produced by plasma cells within the human body to mediate an adaptive immune response against invading pathogens. There are five predominant antibodies produced, each specialized to execute certain functions. Antibodies gain the ability to identify a diverse range of antigens by genetic recombination of different elements of its structure and while the affinity for a specific antigen derives from affinity maturation and somatic recombination processes. Antibodies have a plethora of clinical applications, the most important being their use in combating autoimmune conditions and cancer, conferring passive immunity, and their diagnostic applications.
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
Antibodies are produced primarily to mediate the immune response towards foreign pathogens, as part of the adaptive immune response. Pathogen recognition by B cells in secondary lymphoid organs allows differentiation into memory B cells and plasma cells. Memory cells remain to protect against subsequent attacks from the same pathogen while plasma cells produce antibodies specific for that pathogen. Vaccines rely on this concept, wherein a segment of the pathogen gets introduced to the individual such that an initial immune response is mounted and antibodies are more readily present when the real infection subsequently occurs. The five antibody classes produced by the body include IgG, IgM, IgA, IgD, and IgE. IgM is the first antibody produced and acts as a B-cell surface immunoglobulin(Ig). Complex signaling pathways then induce isotype switching to produce immunoglobulins more fit for fending off the particular pathogens.[1][2]
IgM is the first antibody produced, therefore it is the primary antibody response to pathogens. It is secreted form exists as a pentamer that allows strong binding of the Ig to the pathogen at the initial encounter. IgG is the most abundant antibody present in the serum. It functions to fix complement, neutralize toxins, and opsonizes bacteria. IgG is the only Ig that crosses the placenta and allows protection to the developing infant until levels decline substantially 6 months after birth. IgA mediates immune response in the mucosal membranes such as the gastrointestinal and respiratory lining. This antibody is also present in secretions such as tears and saliva as well as breast milk. IgE is used to mediate the type 1 hypersensitivity reaction in response to allergens with the use of inflammatory mediators such as bradykinins and histamines. IgE does this by binding on the surface of mast cells and basophils. The function of IgD is not entirely understood.[3]
Antibodies can persist in monomeric (IgG, IgE, IgD), dimeric (IgA) or pentameric (IgM) isotypes. A single antibody consists of four polypeptides, two of which are the heavy chains and two light chains. The heavy and light chains come together, forming a “Y” shaped structure, and different parts of the structure mediate different functions. The fragment antigen-binding (Fab) region determines the antibody’s idiotype and has an affinity for pathogenic antigens which allows the antibody to mediate its effect once bound to the antigen. The Fragment crystallizable (Fc) region of antibodies carries out other immune-related functions, such as complement binding, macrophage binding, and determining isotopes of that antibody.[4]
Antibodies recognize millions of different antigens due to the diversity generated during antibody synthesis. The heavy chain and light chains are subject to genetic recombination, in which different gene combinations occur to increase the diversity of the final gene product. Additionally, an enzyme called terminal deoxynucleotidyl inserts random nucleotides during the recombination process, increasing diversity.[5]
Once an antigen binds an antibody, isotype switching occurs in which the Ig most suited for eliminating that pathogen gets expressed on the surface of the B cell. Specificity increases by the concurrent processes of somatic hypermutation and affinity maturation. B cells continuously undergo mutations to increase the chance of producing a more specific antibody. B cell mutations with the highest affinity for the pathogen remain, while the ones with lower affinity get eliminated.[6]
Clinical Significance
Antibodies have been revolutionary in the field of medicine. They are often mandatory in an emergent response, such as in the case of Clostridium botulinum. Upon exposure, patients receive antibodies that confer immunity against the bacteria. Substantial harm can incur before the body naturally carries out an adaptive immune response; therefore, this intervention is essential; this is a form of passive immunity in which preformed Igs are given to the patient. In contrast, active immunity is one's body naturally producing antibodies in response to a pathogen, as seen in, for example, the seasonal influence virus. Patients with immunodeficient conditions such as Bruton agammaglobulinemia or selective IgA deficiency lack an innate ability to produce the entire set of antibodies required to maintain a healthy immune system. Again, the antibodies are passively introduced into the individual to sustain an immune system.[7][8]
Monoclonal antibodies are widely popular in treating autoimmune diseases such as rheumatoid arthritis or Crohn disease. Synthetically formed antibodies bind and prevent the functioning of inflammatory mediators such as TNF-alpha and limit the progression of the disease. Monoclonal antibodies have also been useful in cancer therapies where the Immunoglobulin is used to mount an immune response against the cancerous cell line.[9]
Another application is the use of antibodies to determine the presence of a previous infection. For example, the presence of certain antibodies against the hepatitis virus signifies whether the patient has had a previous infection or if they are currently combating the infection. The same principle is applied to determine immunity against certain diseases, with the presence of antibodies indicating previous infection and a currently immune patient. They can also be used to determine if an individual will be subject to a certain disease in the future. Coombs test is used to detect the potential for future hemolytic anemia by determining whether the antibody will bind the epitopes found on the red blood cell surface. This screening is important for blood transfusion reactions and to determine the likelihood of hemolytic disease of the newborn during pregnancy. It is also useful in home pregnancy tests as antibody binding to human chorionic gonadotropin (HCG) will elicit a response that can be displayed by the meter.[10][11]
A major medical application of antibodies is with immunodiagnostic tests, such as enzyme-linked immunofluorescent assay (ELISA), immunoelectrophoresis, and western blot. These, amongst many others techniques, rely on the principle that the antibody will bind the protein of interest and transmit a signal that can be detected and quantified, to determine the presence and quantity of certain proteins/protein complexes and often used for disease detection purposes.[11]
Media
(Click Image to Enlarge)
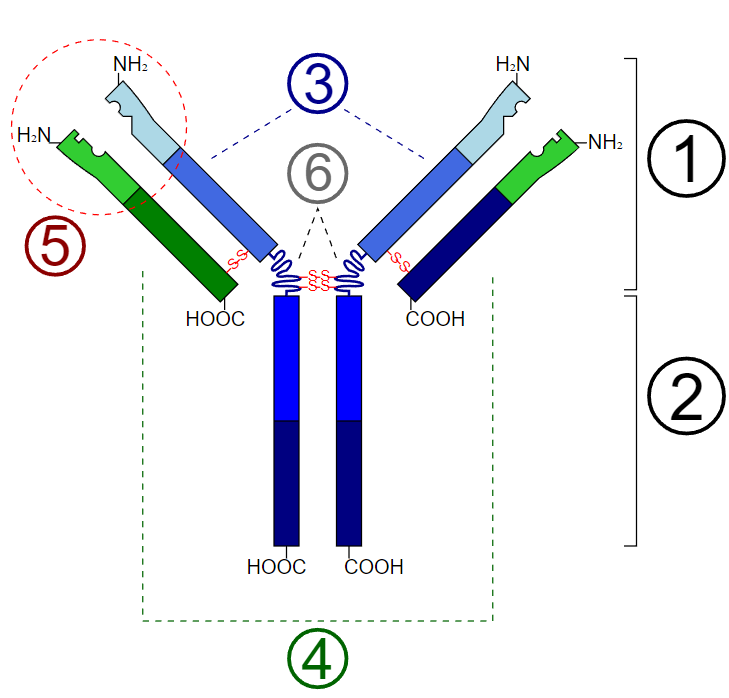
Basic Unit of Immunoglobulin (Antibody). 1. Fab region; 2. Fc region; 3. Heavy chains (consist of VH, CH1, hinge, CH2, and CH3 regions from the N-terminus); 4. Light chains (consist of VL and CL regions from the N-terminus); 5. Antigen binding site; 6. Hinge regions.
Y Tambe, Public Domain, via Wikimedia Commons
References
Forthal DN. Functions of Antibodies. Microbiology spectrum. 2014 Aug 15:2(4):1-17 [PubMed PMID: 25215264]
Amarasekera M. Immunoglobulin E in health and disease. Asia Pacific allergy. 2011 Apr:1(1):12-5. doi: 10.5415/apallergy.2011.1.1.12. Epub 2011 Apr 19 [PubMed PMID: 22053291]
Schroeder HW Jr, Cavacini L. Structure and function of immunoglobulins. The Journal of allergy and clinical immunology. 2010 Feb:125(2 Suppl 2):S41-52. doi: 10.1016/j.jaci.2009.09.046. Epub [PubMed PMID: 20176268]
Level 3 (low-level) evidenceCohen S, Antibody structure. Journal of clinical pathology. Supplement (Association of Clinical Pathologists). 1975; [PubMed PMID: 1078259]
Level 3 (low-level) evidenceBriney BS, Crowe JE Jr. Secondary mechanisms of diversification in the human antibody repertoire. Frontiers in immunology. 2013:4():42. doi: 10.3389/fimmu.2013.00042. Epub 2013 Mar 11 [PubMed PMID: 23483107]
Hwang JK, Alt FW, Yeap LS. Related Mechanisms of Antibody Somatic Hypermutation and Class Switch Recombination. Microbiology spectrum. 2015 Feb:3(1):MDNA3-0037-2014. doi: 10.1128/microbiolspec.MDNA3-0037-2014. Epub [PubMed PMID: 26104555]
Casadevall A. Passive antibody administration (immediate immunity) as a specific defense against biological weapons. Emerging infectious diseases. 2002 Aug:8(8):833-41 [PubMed PMID: 12141970]
Taneja A, Muco E, Chhabra A. Bruton Agammaglobulinemia. StatPearls. 2024 Jan:(): [PubMed PMID: 28846295]
Kotsovilis S, Andreakos E. Therapeutic human monoclonal antibodies in inflammatory diseases. Methods in molecular biology (Clifton, N.J.). 2014:1060():37-59. doi: 10.1007/978-1-62703-586-6_3. Epub [PubMed PMID: 24037835]
Level 3 (low-level) evidenceGilson R, Brook MG. Hepatitis A, B, and C. Sexually transmitted infections. 2006 Dec:82 Suppl 4(Suppl 4):iv35-9 [PubMed PMID: 17151052]
Siddiqui MZ. Monoclonal antibodies as diagnostics; an appraisal. Indian journal of pharmaceutical sciences. 2010 Jan:72(1):12-7. doi: 10.4103/0250-474X.62229. Epub [PubMed PMID: 20582184]