 Anatomy, Shoulder and Upper Limb, Hand Anatomical Snuff Box
Anatomy, Shoulder and Upper Limb, Hand Anatomical Snuff Box
Introduction
The anatomical snuffbox is a surface anatomy feature described as a triangular depression on the dorsum of the hand at the base of the thumb (see Image. Hand Anatomical Snuffbox). The anatomical snuffbox is prominently visible upon ulnar deviation of the wrist and extension and abduction of the thumb. Its name was derived from using the depression as a means of placement for the inhalation of powdered tobacco, otherwise known as dry snuff. It was first described in the medical literature in 1850.[1] However, the anatomical snuffbox was not introduced into anatomy textbooks until the early 1900s when it was described by Germain Cloquet and Marie Francois Bichat.[2]
Anatomically, the anatomical snuffbox is bordered medially by the tendons of the extensor pollicis longus and laterally by the tendons of the muscles named the extensor pollicis brevis and the abductor pollicis longus. The floor of the anatomical snuffbox is formed by the scaphoid bone and trapezium bone of the wrist, as well as the tendons of the muscle named the extensor carpi radialis longus and the muscle named the extensor carpi radialis brevis. Within the anatomical snuffbox, the base of the first metacarpal bone can be palpated distally, and the styloid process of the radius can be palpated proximally. Contained within the anatomical snuffbox are the radial artery, the superficial branches of the radial nerve, and the cephalic vein.[3]
Clinically, the anatomical snuffbox is important because the scaphoid bone can be palpated on its floor (see Image. Scaphoid Bone). Therefore, it is an easily examinable place to assess for signs of scaphoid fracture following trauma, which, if missed, can lead to long-term pain and functional disability.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The anatomical snuffbox is a broadly triangular superficial depression in the skin that emerges when the thumb is held in abduction and the wrist in ulnar deviation. The triangle's base lies parallel to the lateral border of the radial head, while the apex point to the first metacarpophalangeal joint.
When viewing the dorsum of the hand from above, the medial (ulnar) edge of the anatomical snuffbox is formed by the tendon of the extensor pollicus longus muscle, while the lateral (radial) edge is formed by the tendons of extensor pollicus brevis and abductor pollicus longus which run closely in parallel (see Image. Anatomical Snuff Box and Ulnar Styloid Process).
The extensor pollicus longus originates from approximately halfway up the ulna and inserts into the base of the distal phalanx of the thumb, allowing it to be the key extensor of the terminal phalanx. It is innervated by the posterior interosseous nerve.[4] The extensor pollicus brevis (EPB) and abductor pollicus longus (APL) both originate from the posterior aspect of the radius and ulna, although the former muscle is more closely related to the radius and interosseous membrane.[5] The APL inserts as two tendon slips: one at the base of the first metacarpal and the second at the trapezium. The EBP, in contrast, inserts as a thin tendon at the base of the proximal phalanx of the thumb. Both the APL and EBL are innervated by the posterior interosseous nerve, and indeed both act to extend the thumb at the carpometacarpal joint, and the EBP can additionally extend the thumb at the metacarpophalangeal joint.
The base of the anatomical snuffbox contains various bony landmarks. From proximal to distal, these are the radial styloid, the scaphoid bone, the trapezium, and the base of the thumb metacarpal, all of which are palpable on examination with the hand in ulnar deviation with the thumb extended.[6]
The anatomical snuffbox is merely a surface anatomy characteristic and functions in context with other anatomical structures. However, y knowing the boundaries and contents of the anatomical snuff box, a healthcare provider can generate a differential diagnosis when a patient complains of pain in the area. For example, tenderness to palpation in the anatomical snuffbox after a fall on an outstretched hand indicates a scaphoid fracture and would require further testing, including radiologic X-rays, to accurately make the definitive diagnosis. Knowledge of the contents of the anatomical snuffbox will also aid the healthcare provider in those patients with difficult vascular access because both the radial artery and the cephalic vein lie within this area.[7][3]
Blood Supply and Lymphatics
Although the anatomical snuffbox does not have its own blood supply, several vessels course through the boundaries of this surface anatomy feature. Both the cephalic vein and radial artery lie within the anatomical snuffbox. However, the radial artery branches are the most discussed in the practice of medicine due to their supply of the scaphoid bone. Direct branches from the radial artery supply 80% of the proximal scaphoid through intraosseous retrograde flow through the articular foramina, while the remainder is supplied via the volar scaphoid branches of the radial artery that enter at the distal pole. Avascular necrosis of the scaphoid bone commonly occurs due to the unique flow found in the anatomical snuffbox to the scaphoid bone.[8]
Nerves
The superficial nerve branches of the radial nerve that reside within the anatomical snuffbox can be rolled over the tendon of the muscle named the extensor pollicis longus. The tendon of this muscle serves as the medial border of the anatomical snuffbox.[9] The superficial branch of the radial nerve is the terminal branch of the radial nerve, which originates from the posterior cord of the brachial plexus (from nerve roots C5-C8 and T1). The course of this nerve involves passing down through the upper limb, traversing between the long and medial head of the triceps before taking a spiral-like course around the back of the humerus and piercing the intermuscular septum approximately one-third of the distance down the forearm. It gives off the clinically important posterior interosseous nerve (C7, C8), which is the last motor branch of the radial nerve before it terminates as the slender superficial radial nerve, running within the anatomical snuffbox to supply the skin of the two and a half digits from the radial aspect of the hand, and an area over the dorsum of the hand also.[10] See Image. Cutaneous Innervation of the Right Upper Extremity.
Muscles
The anatomical snuffbox is bordered medially by the tendons of the extensor pollicis longus and laterally by the tendons of the extensor pollicis brevis and the abductor pollicis longus. As described earlier, the extensor pollicus brevis and abductor pollicus longus act to extend the thumb, moving it in the lateral horizontal plane.[11][12] This action occurs mainly at the carpometacarpal joint for the abductor pollicus longus, whereas the extensor pollicus brevis acts both at this joint and the metacarpophalangeal joint. The floor of the anatomical snuffbox is partially formed by the tendons of the muscle named the extensor carpi radialis longus and the muscle named the extensor carpi radialis brevis.[13]
Physiologic Variants
Through anatomical research, multiple variations of the tendons of the anatomical snuffbox have been discovered. Both the extensor pollicis longus and the abductor pollicis longus have been shown to have numerous tendon slips and different areas of insertion. This is clinically significant because it may predispose an individual patient to the development of tendinopathy of either of these two muscles. Surgical management, if needed, would also be affected because of these numerous variations in tendon location.[14][13]
Through similar cadaveric research, multiple variations have been noted in the location of the cephalic vein and the radial artery. Clinically this is important because intravenous access can be obtained in the anatomical snuffbox, and inadvertent arterial puncture may cause a pseudo-aneurysm, arterial occlusion, or hematoma.[15]
Surgical Considerations
The superficial branch of the radial nerve is the third most common peripheral nerve injury and will cause an area of paresthesia over the dorsum of the first web space on the hand. Surgeons should be aware of their variable location within the anatomical snuffbox to avoid injury.[9]
The anatomical snuffbox can be used as a point of access for percutaneous arterial access for coronary intervention.[16][17] This approach has several advantages over the more commonly used radial artery approach; most importantly that if the angiography catheter occludes the artery completely, adequate collateral perfusion is strongly available from the radial artery still, and this will avoid ischemic injury of the hand. Furthermore, complications such as bleeding or spreading subcutaneous hematoma generally are managed locally within the anatomical snuffbox; that is, compression of the entire wrist is not necessary, in contrast to similar complications occurring following radial artery puncture, and this preserves movement of the wrist for the patient.[6]
Finally, if the arterial access is not accessible in the anatomical snuffbox, or if, following successful cannulation, there is a procedural complication such as vasospasm or bleeding, the commonly used radial arterial access option remains available as a backup. Disadvantages of this approach include the fact that the caliber of the radial artery is relatively small in the anatomical snuffbox, but a cohort study demonstrated successful cannulation here with a 6 Fr catheter in 132 out of 150 patients, and the authors concluded that this approach is feasible and safe for both coronary angiography and percutaneous coronary intervention.[18]
Clinical Significance
The anatomical snuffbox is clinically significant when there is pain with palpation within its boundaries. Scaphoid fractures account for two-thirds of all carpal bone fractures and are commonly misdiagnosed. The most common form of injury is when a patient falls onto an outstretched hand when it is pronated and deviated in the ulnar plane. The hallmark of anatomic snuffbox tenderness is highly sensitive for scaphoid fractures but lacks specificity. Due to the lack of specificity, those with snuffbox tenderness should undergo radiographic studies of the wrist. Those with initial negative imaging can be managed with either a thumb spica short-armed splint or advanced imaging by MRI or CT to determine if a fracture exists. Given the unique blood flow to the scaphoid, fracture location is important in determining treatment options to prevent avascular necrosis of the bone.[19]
The importance of correctly identifying scaphoid fractures is underlined by the fact that up to 32% of these fractures lead to non-union of the bone, which develops into osteoarthritis.[20] The effect of missing this clinically important fracture on the subsequent quality of life of the patient if non-union develops is potentially highly significant and detrimental. For patients who have a non-displaced or only minimally-displaced fracture of the scaphoid, systematic review and meta-analysis of relevant studies have suggested that there is no difference in long-term pain and disability outcomes between treating these with surgical or non-surgical methods.[21]
De Quervain tenosynovitis is a second clinically significant diagnosis relative to the anatomical snuffbox. De Quervain tenosynovitis is a stenosing tendinopathy that affects the first dorsal compartment, including the abductor pollicis longus and the muscle named the extensor pollicis brevis, both of which are lateral borders of the anatomical snuffbox. Diagnosis can be made based on a thorough history and physical examination. History may include repetitive hand motions in which repeated radio-ulnar deviation occurs. Patients will typically present with pain or swelling over the dorsal aspect of the wrist with associated aggravation of symptoms with the forced resistance of the thumb. Treatment typically includes conservative therapy with NSAIDs, corticosteroids, physical therapy, or splinting in a thumb spica splint. Surgery is reserved for refractory symptomology.[22]
Media
(Click Image to Enlarge)
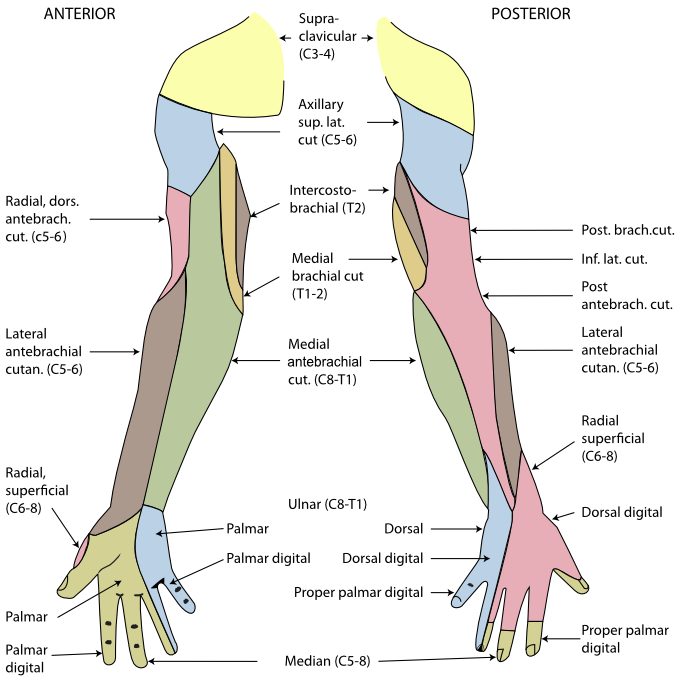
Cutaneous Innervation of the Right Upper Extremity. The areas innervated by the radial nerve are colored pink.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
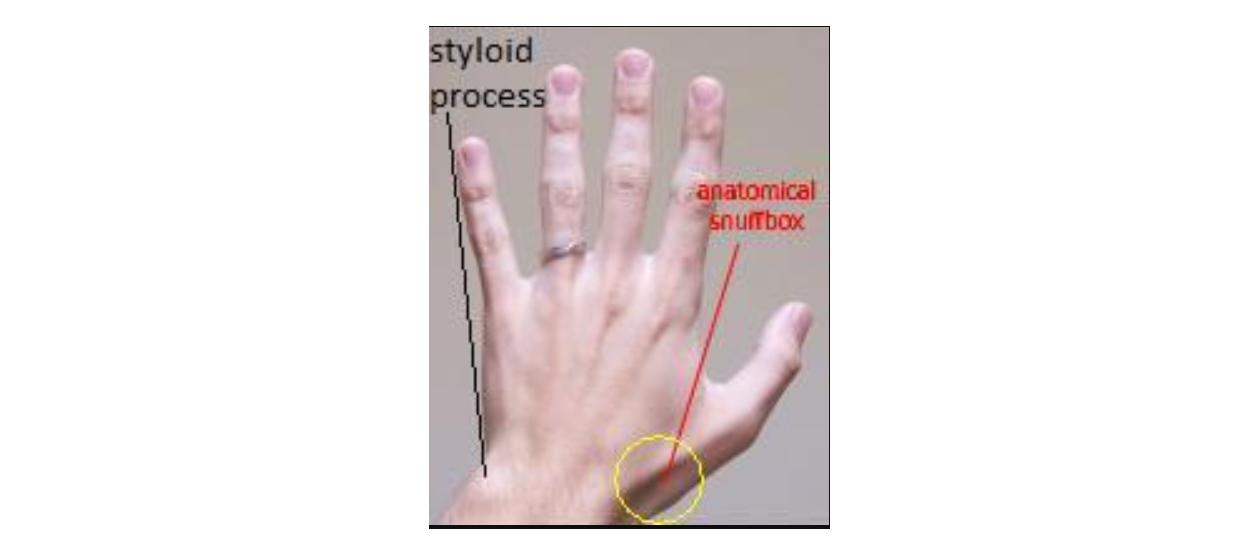
Anatomical Snuff Box and Ulnar Styloid Process. The anatomical snuff box and ulnar styloid process are shown in the image. The boundaries of the anatomical snuff box are the tendons of the abductor pollicis longus and extensor pollicis brevis laterally and the extensor pollicis longus medially.
Mcstrother, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
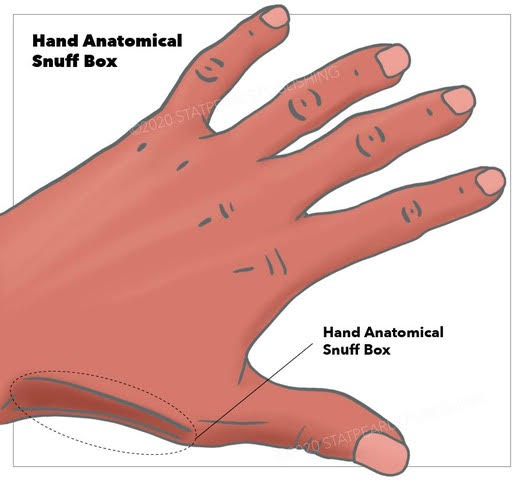
Hand Anatomical Snuffbox
StatPearls Publishing
(Click Image to Enlarge)

Scaphoid Bone
Contributed by S Munakomi, MD
References
Sapundzhiev N, Werner JA. Nasal snuff: historical review and health related aspects. The Journal of laryngology and otology. 2003 Sep:117(9):686-91 [PubMed PMID: 14561353]
Seidenberg AB, Halperin EC, Goldstein AO. It's time to snuff out the "anatomical snuff box". Academic medicine : journal of the Association of American Medical Colleges. 2015 Aug:90(8):1003-4. doi: 10.1097/ACM.0000000000000784. Epub [PubMed PMID: 26218360]
Berger RA. The anatomy of the scaphoid. Hand clinics. 2001 Nov:17(4):525-32 [PubMed PMID: 11775465]
Strauch RJ,Strauch CB, Extensor pollicis brevis tendon can hyperextend thumb interphalangeal joint in absence of extensor pollicis longus: Case report and review of the literature. World journal of orthopedics. 2016 Jul 18 [PubMed PMID: 27458556]
Level 3 (low-level) evidenceShigematsu S, Shimizu H, Beppu M, Hirata K. Anatomy of the extensor pollicis brevis associated with an extension mechanism of the thumb metacarpophalangeal joint. Hand surgery : an international journal devoted to hand and upper limb surgery and related research : journal of the Asia-Pacific Federation of Societies for Surgery of the Hand. 2014:19(2):171-9. doi: 10.1142/S0218810414500166. Epub [PubMed PMID: 24875499]
Roh JH, Lee JH. Distal Radial Approach through the Anatomical Snuff Box for Coronary Angiography and Percutaneous Coronary Intervention. Korean circulation journal. 2018 Dec:48(12):1131-1134. doi: 10.4070/kcj.2018.0293. Epub [PubMed PMID: 30403016]
Sendher R, Ladd AL. The scaphoid. The Orthopedic clinics of North America. 2013 Jan:44(1):107-20. doi: 10.1016/j.ocl.2012.09.003. Epub [PubMed PMID: 23174330]
The vascularity of the scaphoid bone., Gelberman RH,Menon J,, The Journal of hand surgery, 1980 Sep [PubMed PMID: 7430591]
Robson AJ, See MS, Ellis H. Applied anatomy of the superficial branch of the radial nerve. Clinical anatomy (New York, N.Y.). 2008 Jan:21(1):38-45 [PubMed PMID: 18092362]
Gurses IA, Coskun O, Gayretli O, Kale A, Ozturk A. The relationship of the superficial radial nerve and its branch to the thumb to the first extensor compartment. The Journal of hand surgery. 2014 Mar:39(3):480-3. doi: 10.1016/j.jhsa.2013.12.004. Epub 2014 Feb 1 [PubMed PMID: 24495622]
Öztürk K, Dursun A, Kastamoni Y, Albay S. Anatomical variations of the extensor tendons of the fetal thumb. Surgical and radiologic anatomy : SRA. 2021 May:43(5):755-762. doi: 10.1007/s00276-020-02611-7. Epub 2020 Nov 10 [PubMed PMID: 33170332]
Sugiura S,Matsuura Y,Suzuki T,Nishikawa S,Mori C,Kuniyoshi K, Variant course of extensor pollicis brevis tendon in the third extensor compartment. Surgical and radiologic anatomy : SRA. 2018 Mar; [PubMed PMID: 29138875]
Adams JE, Habbu R. Tendinopathies of the Hand and Wrist. The Journal of the American Academy of Orthopaedic Surgeons. 2015 Dec:23(12):741-50. doi: 10.5435/JAAOS-D-14-00216. Epub 2015 Oct 28 [PubMed PMID: 26510626]
Thwin SS, Fazlin F, Than M. Multiple variations of the tendons of the anatomical snuffbox. Singapore medical journal. 2014 Jan:55(1):37-40 [PubMed PMID: 24452976]
Lirk P, Keller C, Colvin J, Colvin H, Rieder J, Maurer H, Moriggl B. Unintentional arterial puncture during cephalic vein cannulation: case report and anatomical study. British journal of anaesthesia. 2004 May:92(5):740-2 [PubMed PMID: 15003983]
Level 3 (low-level) evidencePua U,Quek LHH, "Snuffbox" Distal Radial Access. Journal of vascular and interventional radiology : JVIR. 2018 Jan [PubMed PMID: 29258662]
Kiemeneij F. Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI). EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology. 2017 Sep 20:13(7):851-857. doi: 10.4244/EIJ-D-17-00079. Epub [PubMed PMID: 28506941]
Kim Y, Ahn Y, Kim I, Lee DH, Kim MC, Sim DS, Hong YJ, Kim JH, Jeong MH. Feasibility of Coronary Angiography and Percutaneous Coronary Intervention via Left Snuffbox Approach. Korean circulation journal. 2018 Dec:48(12):1120-1130. doi: 10.4070/kcj.2018.0181. Epub 2018 Aug 6 [PubMed PMID: 30088362]
Level 2 (mid-level) evidenceKo JH, Pet MA, Khouri JS, Hammert WC. Management of Scaphoid Fractures. Plastic and reconstructive surgery. 2017 Aug:140(2):333e-346e. doi: 10.1097/PRS.0000000000003558. Epub [PubMed PMID: 28746289]
Cohen A,Reijman M,Kraan GA,Mathijssen NMC,Koopmanschap MA,Verhaar JAN,Mol S,Colaris JW,SUSPECT study group, Clinically SUspected ScaPhoid fracturE: treatment with supportive bandage or CasT? 'Study protocol of a multicenter randomized controlled trial' (SUSPECT study). BMJ open. 2020 Sep 29 [PubMed PMID: 32994236]
Level 1 (high-level) evidenceLi H, Guo W, Guo S, Zhao S, Li R. Surgical versus nonsurgical treatment for scaphoid waist fracture with slight or no displacement: A meta-analysis and systematic review. Medicine. 2018 Nov:97(48):e13266. doi: 10.1097/MD.0000000000013266. Epub [PubMed PMID: 30508914]
Level 1 (high-level) evidenceAshurst JV, Turco DA, Lieb BE. Tenosynovitis caused by texting: an emerging disease. The Journal of the American Osteopathic Association. 2010 May:110(5):294-6 [PubMed PMID: 20538752]
Level 3 (low-level) evidence