Introduction
Acute otitis media is defined as an infection of the middle ear space. It is a spectrum of diseases that includes acute otitis media (AOM), chronic suppurative otitis media (CSOM), and otitis media with effusion (OME). Acute otitis media is the second most common pediatric diagnosis in the emergency department, following upper respiratory infections. Although otitis media can occur at any age, it is most commonly seen between the ages of 6 to 24 months.[1]
Infection of the middle ear can be viral, bacterial, or coinfection. The most common bacterial organisms causing otitis media are Streptococcus pneumoniae, followed by non-typeable Haemophilus influenzae (NTHi) and Moraxella catarrhalis. Following the introduction of the conjugate pneumococcal vaccines, the pneumococcal organisms have evolved to non-vaccine serotypes. The most common viral pathogens of otitis media include the respiratory syncytial virus (RSV), coronaviruses, influenza viruses, adenoviruses, human metapneumovirus, and picornaviruses.[2][3][4]
Otitis media is diagnosed clinically via objective findings on physical exam (otoscopy) combined with the patient's history and presenting signs and symptoms. Several diagnostic tools are available such as a pneumatic otoscope, tympanometry, and acoustic reflectometry, to aid in the diagnosis of otitis media. Pneumatic otoscopy is the most reliable and has a higher sensitivity and specificity as compared to plain otoscopy, though tympanometry and other modalities can facilitate diagnosis if pneumatic otoscopy is unavailable.
Treatment of otitis media with antibiotics is controversial and directly related to the subtype of otitis media in question. Without proper treatment, suppurative fluid from the middle ear can extend to the adjacent anatomical locations and result in complications such as tympanic membrane (TM) perforation, mastoiditis, labyrinthitis, petrositis, meningitis, brain abscess, hearing loss, lateral and cavernous sinus thrombosis, and others.[5] This has led to the development of specific guidelines for the treatment of OM. In the United States, the mainstay of treatment for an established diagnosis of AOM is high-dose amoxicillin, and this has been found to be most effective in children under two years of age. Treatment in countries like the Netherlands is initially watchful waiting, and if unresolved, antibiotics are warranted[6]. However, the concept of watchful waiting has not gained full acceptance in the United States and other countries due to the risk of prolonged middle ear fluid and its effect on hearing and speech, as well as the risks of complications discussed earlier. Analgesics such as non-steroidal anti-inflammatory medications such as ibuprofen can be used alone or in combination to achieve effective pain control in patients with otitis media.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Otitis media is a multifactorial disease. Infectious, allergic, and environmental factors contribute to otitis media.[7][8][9][10][11][12]
These causes and risk factors include:
- Decreased immunity due to human immunodeficiency virus (HIV), diabetes, and other immuno-deficiencies
- Genetic predisposition
- Mucins that include abnormalities of this gene expression, especially upregulation of MUC5B
- Anatomic abnormalities of the palate and tensor veli palatini
- Ciliary dysfunction
- Cochlear implants
- Vitamin A deficiency
- Bacterial pathogens, Streptococcus pneumoniae, Haemophilus influenza, and Moraxella (Branhamella) catarrhalis are responsible for more than 95%
- Viral pathogens such as respiratory syncytial virus, influenza virus, parainfluenza virus, rhinovirus, and adenovirus
- Allergies
- Lack of breastfeeding
- Passive smoke exposure
- Daycare attendance
- Lower socioeconomic status
- Family history of recurrent AOM in parents or siblings
Epidemiology
Otitis media is a global problem and is found to be slightly more common in males than in females. The specific number of cases per year is difficult to determine due to the lack of reporting and different incidences across many different geographical regions. The peak incidence of otitis media occurs between six and twelve months of life and declines after age five. Approximately 80% of all children will experience a case of otitis media during their lifetime, and between 80% and 90% of all children will experience otitis media with an effusion before school age. Otitis media is less common in adults than in children, though it is more common in specific sub-populations such as those with a childhood history of recurrent OM, cleft palate, immunodeficiency or immunocompromised status, and others.[13][14]
Pathophysiology
Otitis media begins as an inflammatory process following a viral upper respiratory tract infection involving the mucosa of the nose, nasopharynx, middle ear mucosa, and Eustachian tubes. Due to the constricted anatomical space of the middle ear, the edema caused by the inflammatory process obstructs the narrowest part of the Eustachian tube leading to a decrease in ventilation. This leads to a cascade of events resulting in an increase in negative pressure in the middle ear, increasing exudate from the inflamed mucosa, and buildup of mucosal secretions, which allows for the colonization of bacterial and viral organisms in the middle ear. The growth of these microbes in the middle ear then leads to suppuration and, eventually, frank purulence in the middle ear space. This is demonstrated clinically by a bulging or erythematous tympanic membrane and purulent middle ear fluid. This must be differentiated from chronic serous otitis media (CSOM), which presents with thick, amber-colored fluid in the middle ear space and a retracted tympanic membrane on otoscopic examination. Both will yield decreased TM mobility on tympanometry or pneumatic otoscopy.
Several risk factors can predispose children to develop acute otitis media. The most common risk factor is a preceding upper respiratory tract infection. Other risk factors include male gender, adenoid hypertrophy (obstructing), allergy, daycare attendance, environmental smoke exposure, pacifier use, immunodeficiency, gastroesophageal reflux, parental history of recurrent childhood OM, and other genetic predispositions.[15][16][17]
Histopathology
Histopathology varies according to disease severity. Acute purulent otitis media (APOM) is characterized by edema and hyperemia of the subepithelial space, which is followed by the infiltration of polymorphonuclear (PMN) leukocytes. As the inflammatory process progresses, there is mucosal metaplasia and the formation of granulation tissue. After five days, the epithelium changes from flat cuboidal to pseudostratified columnar with the presence of goblet cells.
In serous acute otitis media (SAOM), inflammation of the middle ear and the eustachian tube has been identified as the major precipitating factor. Venous or lymphatic stasis in the nasopharynx or the eustachian tube plays a vital role in the pathogenesis of AOM. Inflammatory cytokines attract plasma cells, leukocytes, and macrophages to the site of inflammation. The epithelium changes to pseudostratified, columnar, or cuboidal. Hyperplasia of basal cells results in an increased number of goblet cells in the new epithelium.[18]
In practice, biopsy for histology is not performed for OM outside of research settings.
History and Physical
Although one of the best indicators for otitis media is otalgia, many children with otitis media can present with non-specific signs and symptoms, which can make the diagnosis challenging. These symptoms include pulling or tugging at the ears, irritability, headache, disturbed or restless sleep, poor feeding, anorexia, vomiting, or diarrhea. Approximately two-thirds of the patients present with fever, which is typically low-grade.
The diagnosis of otitis media is primarily based on clinical findings combined with supporting signs and symptoms as described above. No lab test or imaging is needed. According to guidelines set forth by the American Academy of Pediatrics, evidence of moderate to severe bulging of the tympanic membrane or new onset of otorrhea not caused by otitis externa or mild tympanic membrane (TM) bulging with recent onset of ear pain or erythema is required for the diagnosis of acute otitis media. These criteria are intended only to aid primary care clinicians in the diagnosis and proper clinical decision-making but not to replace clinical judgment.[19]
Otoscopic examination should be the first and most convenient way of examining the ear and will yield the diagnosis to the experienced eye. In AOM, the TM may be erythematous or normal, and there may be fluid in the middle ear space. In suppurative OM, there will be obvious purulent fluid visible and a bulging TM. The external ear canal (EAC) may be somewhat edematous, though significant edema should alert the clinician to suspect otitis externa (outer ear infection, AOE), which may be treated differently. In the presence of EAC edema, it is paramount to visualize the TM to ensure it is intact. If there is an intact TM and a painful, erythematous EAC, ototopical drops should be added to treat AOE. This can exist in conjunction with AOM or independent of it, so visualization of the middle ear is paramount. If there is a perforation of the TM, then the EAC edema can be assumed to be reactive, and ototopical medication should be used, but an agent approved for use in the middle ear, such as ofloxacin, must be used, as other agents can be ototoxic.[20][21][22]
Evaluation
The diagnosis of otitis media should always begin with a physical exam and the use of an otoscope, ideally a pneumatic otoscope.[23][24]
Laboratory Studies
Laboratory evaluation is rarely necessary. A full sepsis workup in infants younger than 12 weeks with fever and no obvious source other than associated acute otitis media may be necessary. Laboratory studies may be needed to confirm or exclude possible related systemic or congenital diseases.
Imaging Studies
Imaging studies are not indicated unless intra-temporal or intracranial complications are a concern.[25][26]
- When an otitis media complication is suspected, computed tomography of the temporal bones may identify mastoiditis, epidural abscess, sigmoid sinus thrombophlebitis, meningitis, brain abscess, subdural abscess, ossicular disease, and cholesteatoma.
- Magnetic resonance imaging may identify fluid collections, especially in the middle ear collections.
Tympanocentesis
Tympanocentesis may be used to determine the presence of middle ear fluid, followed by culture to identify pathogens.
Tympanocentesis can improve diagnostic accuracy and guide treatment decisions but is reserved for extreme or refractory cases.[27][28]
Other Tests
Tympanometry and acoustic reflectometry may also be used to evaluate for middle ear effusion.[29]
Treatment / Management
Once the diagnosis of acute otitis media is established, the goal of treatment is to control pain and treat the infectious process with antibiotics. Non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen can be used to achieve pain control. There are controversies about prescribing antibiotics in early otitis media, and the guidelines may vary by country, as discussed above. Watchful waiting is practiced in European countries with no reported increased incidence of complications. However, watchful waiting has not gained wide acceptance in the United States. If there is clinical evidence of suppurative AOM, however, oral antibiotics are indicated to treat this bacterial infection, and high-dose amoxicillin or a second-generation cephalosporin are first-line agents. If there is a TM perforation, treatment should proceed with ototopical antibiotics safe for middle-ear use, such as ofloxacin, rather than systemic antibiotics, as this delivers much higher concentrations of antibiotics without any systemic side effects.[23]
When a bacterial etiology is suspected, the antibiotic of choice is high-dose amoxicillin for ten days in both children and adult patients who are not allergic to penicillin. Amoxicillin has good efficacy in the treatment of otitis media due to its high concentration in the middle ear. In cases of penicillin allergy, the American Academy of Pediatrics (AAP) recommends azithromycin as a single dose of 10 mg/kg or clarithromycin (15 mg/kg per day in 2 divided doses). Other options for penicillin-allergic patients are cefdinir (14 mg/kg per day in 1 or 2 doses), cefpodoxime (10 mg/kg per day, once daily), or cefuroxime (30 mg/kg per day in 2 divided doses).
For those patients whose symptoms do not improve after treatment with high-dose amoxicillin, high-dose amoxicillin-clavulanate (90 mg/kg per day of amoxicillin component, with 6.4 mg/kg per day of clavulanate in 2 divided doses) should be given. In children who are vomiting or if there are situations in which oral antibiotics cannot be administered, ceftriaxone (50 mg/kg per day) for three consecutive days, either intravenously or intramuscularly, is an alternative option. Systemic steroids and antihistamines have not been shown to have any significant benefits.[30][31][19][32][33][34](A1)
Patients who have experienced four or more episodes of AOM in the past twelve months should be considered candidates for myringotomy with tube (grommet) placement, according to the American Academy of Pediatrics guidelines. Recurrent infections requiring antibiotics are clinical evidence of Eustachian tube dysfunction, and placement of the tympanostomy tube allows ventilation of the middle ear space and maintenance of normal hearing. Furthermore, should the patient acquire otitis media while a functioning tube is in place, they can be treated with ototopical antibiotic drops rather than systemic antibiotics.[35]
Differential Diagnosis
The following conditions come under the differential diagnosis of otitis media[36][37][38]
- Cholesteatoma
- Fever in the infant and toddler
- Fever without a focus
- Hearing impairment
- Pediatric nasal polyps
- Nasopharyngeal cancer
- Otitis externa
- Human parainfluenza viruses (HPIV) and other parainfluenza viruses
- Passive smoking and lung disease
- Pediatric allergic rhinitis
- Pediatric bacterial meningitis
- Pediatric gastroesophageal reflux
- Pediatric Haemophilus influenzae infection
- Pediatric HIV infection
- Pediatric mastoiditis
- Pediatric pneumococcal infections
- Primary ciliary dyskinesia
- Respiratory syncytial virus infection
- Rhinovirus (RV) infection (common cold)
- Teething
Prognosis
The prognosis for most of the patients with otitis media is excellent.[39] Mortality from AOM is a rare occurrence in modern times. Due to better access to healthcare in developed countries, early diagnosis and treatment have resulted in a better prognosis for this disease. Effective antibiotic therapy is the mainstay of treatment. Multiple prognostic factors affect the disease course. Children presenting with less than three episodes of AOM are three times more likely to have their symptoms resolved with a single course of antibiotics as compared to children who develop this condition in seasons apart from winter.[40]
Children who develop complications can be difficult to treat and tend to have high rates of recurrence. Intratemporal and intracranial complications, while very rare, have significant mortality rates.[41]
Children with a history of prelingual otitis media are at risk for mild-to-moderate conductive hearing loss. Children with otitis media in the first 24 months of life often have difficulty perceiving strident or high-frequency consonants, such as sibilants.
Complications
Due to the complex arrangement of structures in and around the middle ear, complications, once developed, are challenging to treat. Complications can be divided into intratemporal and intracranial complications.[41][42][43][42]
The following are the intratemporal complications;
- Hearing loss (conductive and sensorineural)
- TM perforation (acute and chronic)
- Chronic suppurative otitis media (with or without cholesteatoma)
- Cholesteatoma
- Tympanosclerosis
- Mastoiditis
- Petrositis
- Labyrinthitis
- Facial paralysis
- Cholesterol granuloma
- Infectious eczematoid dermatitis
Additionally, it is important to discuss the effect of OM on hearing, particularly in the 6-24 month age range, as this is an important time for language development, which is related to hearing. The conductive hearing loss resulting from chronic or recurrent OM can adversely affect language development and result in prolonged speech problems requiring speech therapy. This is one reason the American Academy of Pediatrics and the American Academy of Otolaryngology-Head & Neck Surgery recommend aggressive early treatment of recurrent AOM.
The following are the intracranial complications;
- Meningitis
- Subdural empyema
- Brain abscess
- Extradural abscess
- Lateral sinus thrombosis
- Otitic hydrocephalus
Consultations
Patients with uncomplicated AOM are usually treated by their primary care providers. However, primary care physicians may refer the patient to an otolaryngologist for surgical procedures, most likely tympanostomy tubes, in the case of recurrent AOM or CSOM. An audiologist is involved if children present with subjective evidence of hearing loss or failure to meet language development marks. Young children with CSOM may have speech and language delays owing to the hearing loss created by recurrent ear infections, which are managed by a speech therapist.[44]
Deterrence and Patient Education
Pneumococcal and influenza vaccines prevent upper respiratory tract infections (URTIs) in children. Apart from this, the avoidance of tobacco smoke can decrease the risk of URTI. Tobacco smoke is a respiratory stimulant that increases the risk of pneumonia in children. Infants with otitis media should be breastfed whenever possible, as breast milk contains immunoglobulins that protect infants from foreign pathogens in key phases of early extra-uterine life.[45]
Enhancing Healthcare Team Outcomes
Acute otitis media can often be managed in the outpatient/clinical setting. However, it can best be served via interprofessional management through an interprofessional team approach, including physicians, family, audiologists, nurses, pharmacists, and/or speech pathologists. Early diagnosis and prompt treatment decrease the risk of complications resulting in better patient outcomes. Nurses instruct the family about medication administration, supportive care, and analgesics. They review follow-up instructions. Pharmacists instruct patients about the potential adverse effects of medication and review for drug interactions.
Media
(Click Image to Enlarge)

Acute Otitis Media on Otoscopy. This otoscopic image shows tympanic membrane erythema and bulging, consistent with acute otitis media.
Contributed by Wikimedia Commons, B. Welleschik (CC by 2.0) https://creativecommons.org/licenses/by/2.0/
(Click Image to Enlarge)
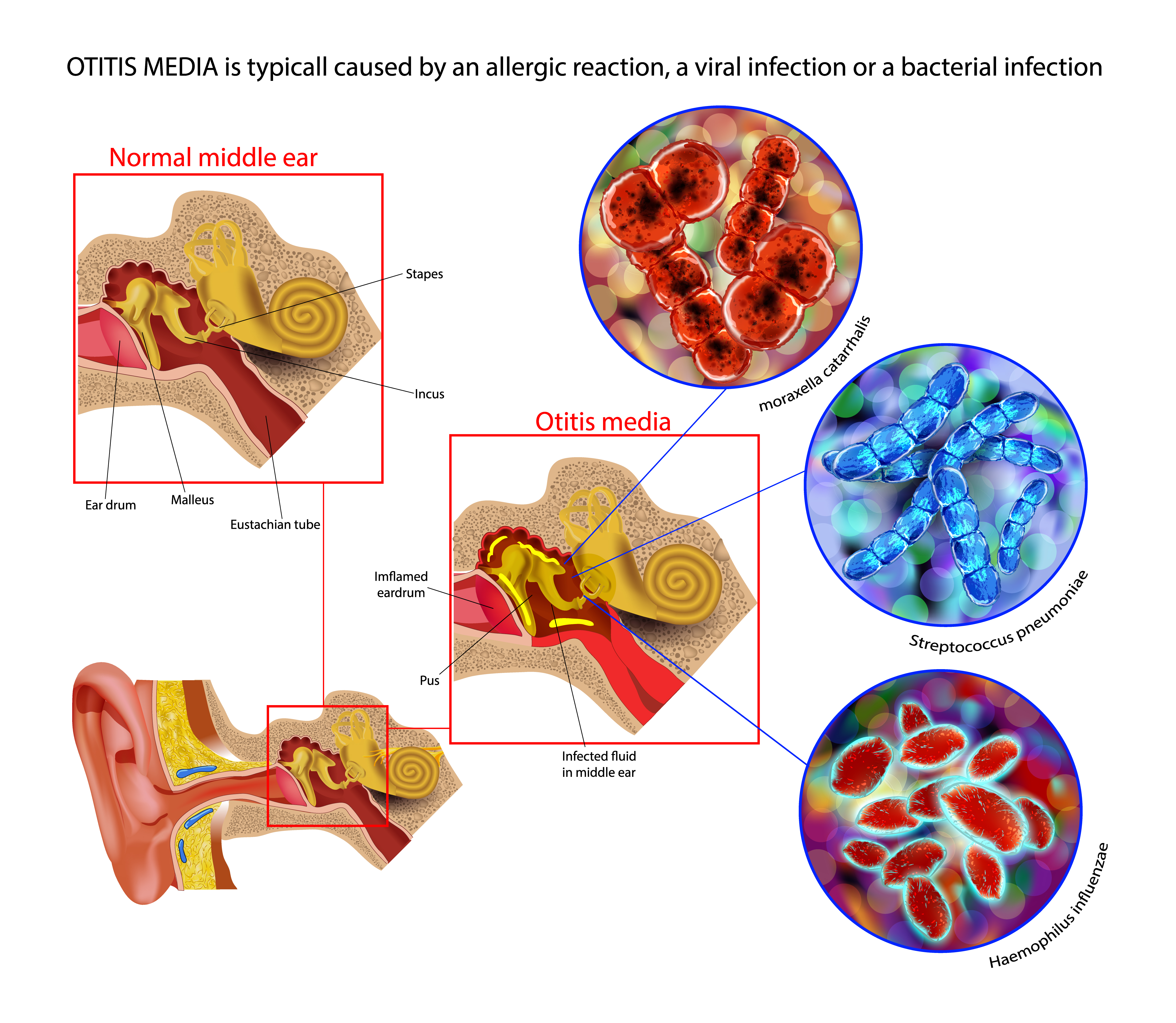
Acute Otitis Media Pathophysiology. This illustration shows the common etiologies and pathophysiology of acute otitis media.
Purchased from Shutterstock
References
Meherali S, Campbell A, Hartling L, Scott S. Understanding Parents' Experiences and Information Needs on Pediatric Acute Otitis Media: A Qualitative Study. Journal of patient experience. 2019 Mar:6(1):53-61. doi: 10.1177/2374373518771362. Epub 2018 Apr 24 [PubMed PMID: 31236452]
Level 2 (mid-level) evidenceUbukata K, Morozumi M, Sakuma M, Takata M, Mokuno E, Tajima T, Iwata S, AOM Surveillance Study Group. Etiology of Acute Otitis Media and Characterization of Pneumococcal Isolates After Introduction of 13-Valent Pneumococcal Conjugate Vaccine in Japanese Children. The Pediatric infectious disease journal. 2018 Jun:37(6):598-604. doi: 10.1097/INF.0000000000001956. Epub [PubMed PMID: 29474258]
Ubukata K, Morozumi M, Sakuma M, Adachi Y, Mokuno E, Tajima T, Iwata S, AOM Surveillance Study Group. Genetic characteristics and antibiotic resistance of Haemophilus influenzae isolates from pediatric patients with acute otitis media after introduction of 13-valent pneumococcal conjugate vaccine in Japan. Journal of infection and chemotherapy : official journal of the Japan Society of Chemotherapy. 2019 Sep:25(9):720-726. doi: 10.1016/j.jiac.2019.03.019. Epub 2019 Apr 12 [PubMed PMID: 30987951]
Protasova IN, Per'yanova OV, Podgrushnaya TS. [Acute otitis media in the children: etiology and the problems of antibacterial therapy]. Vestnik otorinolaringologii. 2017:82(2):84-89. doi: 10.17116/otorino201782284-89. Epub [PubMed PMID: 28514373]
García Carretero R. Cerebellar abscesses, infective endocarditis and bacteraemia due to a rare pathogen: Streptococcus constellatus. BMJ case reports. 2017 Sep 1:2017():. pii: bcr-2017-221374. doi: 10.1136/bcr-2017-221374. Epub 2017 Sep 1 [PubMed PMID: 28864559]
Level 3 (low-level) evidenceSchilder AG, Lok W, Rovers MM. International perspectives on management of acute otitis media: a qualitative review. International journal of pediatric otorhinolaryngology. 2004 Jan:68(1):29-36 [PubMed PMID: 14687684]
Level 2 (mid-level) evidenceMittal R, Robalino G, Gerring R, Chan B, Yan D, Grati M, Liu XZ. Immunity genes and susceptibility to otitis media: a comprehensive review. Journal of genetics and genomics = Yi chuan xue bao. 2014 Nov 20:41(11):567-81. doi: 10.1016/j.jgg.2014.10.003. Epub 2014 Oct 31 [PubMed PMID: 25434680]
Seppälä E, Sillanpää S, Nurminen N, Huhtala H, Toppari J, Ilonen J, Veijola R, Knip M, Sipilä M, Laranne J, Oikarinen S, Hyöty H. Human enterovirus and rhinovirus infections are associated with otitis media in a prospective birth cohort study. Journal of clinical virology : the official publication of the Pan American Society for Clinical Virology. 2016 Dec:85():1-6. doi: 10.1016/j.jcv.2016.10.010. Epub 2016 Oct 20 [PubMed PMID: 27780081]
Ardiç C, Yavuz E. Effect of breastfeeding on common pediatric infections: a 5-year prospective cohort study. Archivos argentinos de pediatria. 2018 Apr 1:116(2):126-132. doi: 10.5546/aap.2018.eng.126. Epub [PubMed PMID: 29557599]
Strachan DP, Cook DG. Health effects of passive smoking. 4. Parental smoking, middle ear disease and adenotonsillectomy in children. Thorax. 1998 Jan:53(1):50-6 [PubMed PMID: 9577522]
Level 2 (mid-level) evidenceJones LL, Hassanien A, Cook DG, Britton J, Leonardi-Bee J. Parental smoking and the risk of middle ear disease in children: a systematic review and meta-analysis. Archives of pediatrics & adolescent medicine. 2012 Jan:166(1):18-27. doi: 10.1001/archpediatrics.2011.158. Epub 2011 Sep 5 [PubMed PMID: 21893640]
Level 1 (high-level) evidenceVila PM, Ghogomu NT, Odom-John AR, Hullar TE, Hirose K. Infectious complications of pediatric cochlear implants are highly influenced by otitis media. International journal of pediatric otorhinolaryngology. 2017 Jun:97():76-82. doi: 10.1016/j.ijporl.2017.02.026. Epub 2017 Mar 12 [PubMed PMID: 28483256]
Usonis V, Jackowska T, Petraitiene S, Sapala A, Neculau A, Stryjewska I, Devadiga R, Tafalla M, Holl K. Incidence of acute otitis media in children below 6 years of age seen in medical practices in five East European countries. BMC pediatrics. 2016 Jul 26:16():108. doi: 10.1186/s12887-016-0638-2. Epub 2016 Jul 26 [PubMed PMID: 27457584]
Schilder AG, Chonmaitree T, Cripps AW, Rosenfeld RM, Casselbrant ML, Haggard MP, Venekamp RP. Otitis media. Nature reviews. Disease primers. 2016 Sep 8:2(1):16063. doi: 10.1038/nrdp.2016.63. Epub 2016 Sep 8 [PubMed PMID: 27604644]
Fireman P. Otitis media and eustachian tube dysfunction: connection to allergic rhinitis. The Journal of allergy and clinical immunology. 1997 Feb:99(2):S787-97 [PubMed PMID: 9042072]
Kraemer MJ, Richardson MA, Weiss NS, Furukawa CT, Shapiro GG, Pierson WE, Bierman CW. Risk factors for persistent middle-ear effusions. Otitis media, catarrh, cigarette smoke exposure, and atopy. JAMA. 1983 Feb 25:249(8):1022-5 [PubMed PMID: 6681641]
Fireman P. Eustachian tube obstruction and allergy: a role in otitis media with effusion? The Journal of allergy and clinical immunology. 1985 Aug:76(2 Pt 1):137-40 [PubMed PMID: 4019946]
Meyerhoff WL, Giebink GS. Panel discussion: pathogenesis of otitis media. Pathology and microbiology of otitis media. The Laryngoscope. 1982 Mar:92(3):273-7 [PubMed PMID: 6978445]
Level 3 (low-level) evidenceSiddiq S, Grainger J. The diagnosis and management of acute otitis media: American Academy of Pediatrics Guidelines 2013. Archives of disease in childhood. Education and practice edition. 2015 Aug:100(4):193-7. doi: 10.1136/archdischild-2013-305550. Epub 2014 Nov 12 [PubMed PMID: 25395494]
Marchisio P, Galli L, Bortone B, Ciarcià M, Motisi MA, Novelli A, Pinto L, Bottero S, Pignataro L, Piacentini G, Mattina R, Cutrera R, Varicchio A, Luigi Marseglia G, Villani A, Chiappini E, Italian Panel for the Management of Acute Otitis Media in Children. Updated Guidelines for the Management of Acute Otitis Media in Children by the Italian Society of Pediatrics: Treatment. The Pediatric infectious disease journal. 2019 Dec:38(12S Suppl):S10-S21. doi: 10.1097/INF.0000000000002452. Epub [PubMed PMID: 31876601]
Moazzami B, Mohayeji Nasrabadi MA, Abolhassani H, Olbrich P, Azizi G, Shirzadi R, Modaresi M, Sohani M, Delavari S, Shahkarami S, Yazdani R, Aghamohammadi A. Comprehensive assessment of respiratory complications in patients with common variable immunodeficiency. Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology. 2020 May:124(5):505-511.e3. doi: 10.1016/j.anai.2020.01.019. Epub 2020 Jan 30 [PubMed PMID: 32007567]
Kaur R, Czup K, Casey JR, Pichichero ME. Correlation of nasopharyngeal cultures prior to and at onset of acute otitis media with middle ear fluid cultures. BMC infectious diseases. 2014 Dec 5:14():640. doi: 10.1186/s12879-014-0640-y. Epub 2014 Dec 5 [PubMed PMID: 25475135]
Level 3 (low-level) evidenceChiappini E, Ciarcià M, Bortone B, Doria M, Becherucci P, Marseglia GL, Motisi MA, de Martino M, Galli L, Licari A, De Masi S, Lubrano R, Bettinelli M, Vicini C, Felisati G, Villani A, Marchisio P, Italian Panel for the Management of Acute Otitis Media in Children. Updated Guidelines for the Management of Acute Otitis Media in Children by the Italian Society of Pediatrics: Diagnosis. The Pediatric infectious disease journal. 2019 Dec:38(12S Suppl):S3-S9. doi: 10.1097/INF.0000000000002429. Epub [PubMed PMID: 31876600]
Homme JH. Acute Otitis Media and Group A Streptococcal Pharyngitis: A Review for the General Pediatric Practitioner. Pediatric annals. 2019 Sep 1:48(9):e343-e348. doi: 10.3928/19382359-20190813-01. Epub [PubMed PMID: 31505007]
Penido Nde O, Borin A, Iha LC, Suguri VM, Onishi E, Fukuda Y, Cruz OL. Intracranial complications of otitis media: 15 years of experience in 33 patients. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2005 Jan:132(1):37-42 [PubMed PMID: 15632907]
Level 2 (mid-level) evidenceMattos JL, Colman KL, Casselbrant ML, Chi DH. Intratemporal and intracranial complications of acute otitis media in a pediatric population. International journal of pediatric otorhinolaryngology. 2014 Dec:78(12):2161-4. doi: 10.1016/j.ijporl.2014.09.032. Epub 2014 Oct 6 [PubMed PMID: 25447953]
Level 2 (mid-level) evidenceVayalumkal J, Kellner JD. Tympanocentesis for the management of acute otitis media in children: a survey of Canadian pediatricians and family physicians. Archives of pediatrics & adolescent medicine. 2004 Oct:158(10):962-5 [PubMed PMID: 15466683]
Level 3 (low-level) evidenceSchaad UB. Predictive value of double tympanocentesis in acute otitis media. Pharmacotherapy. 2005 Dec:25(12 Pt 2):105S-10S [PubMed PMID: 16305279]
Lampe RM, Weir MR, Spier J, Rhodes MF. Acoustic reflectometry in the detection of middle ear effusion. Pediatrics. 1985 Jul:76(1):75-8 [PubMed PMID: 4040237]
Rettig E, Tunkel DE. Contemporary concepts in management of acute otitis media in children. Otolaryngologic clinics of North America. 2014 Oct:47(5):651-72. doi: 10.1016/j.otc.2014.06.006. Epub 2014 Aug 1 [PubMed PMID: 25213276]
Lieberthal AS, Carroll AE, Chonmaitree T, Ganiats TG, Hoberman A, Jackson MA, Joffe MD, Miller DT, Rosenfeld RM, Sevilla XD, Schwartz RH, Thomas PA, Tunkel DE. The diagnosis and management of acute otitis media. Pediatrics. 2013 Mar:131(3):e964-99. doi: 10.1542/peds.2012-3488. Epub 2013 Feb 25 [PubMed PMID: 23439909]
Level 1 (high-level) evidenceMarchisio P, Bortone B, Ciarcià M, Motisi MA, Torretta S, Castelli Gattinara G, Picca M, Di Mauro G, Bonino M, Mansi N, Varricchio A, Marseglia GL, Cardinale F, Villani A, Chiappini E. Updated Guidelines for the Management of Acute Otitis Media in Children by the Italian Society of Pediatrics: Prevention. The Pediatric infectious disease journal. 2019 Dec:38(12S Suppl):S22-S36. doi: 10.1097/INF.0000000000002430. Epub [PubMed PMID: 31876602]
Brinker DL Jr, MacGeorge EL, Hackman N. Diagnostic Accuracy, Prescription Behavior, and Watchful Waiting Efficacy for Pediatric Acute Otitis Media. Clinical pediatrics. 2019 Jan:58(1):60-65. doi: 10.1177/0009922818806312. Epub 2018 Oct 12 [PubMed PMID: 30311779]
Ahmed A, Kolo E, Aluko A, Abdullahi H, Ajiya A, Bello-Muhammad N, Raji H, Tsiga-Ahmed F. Diagnosis and management of otitis media with effusion in a tertiary hospital in Kano: a best practice implementation project. JBI database of systematic reviews and implementation reports. 2018 Oct:16(10):2050-2063. doi: 10.11124/JBISRIR-2017-003717. Epub [PubMed PMID: 30335043]
Level 1 (high-level) evidenceMarchica CL, Dahl JP, Raol N. What's New with Tubes, Tonsils, and Adenoids? Otolaryngologic clinics of North America. 2019 Oct:52(5):779-794. doi: 10.1016/j.otc.2019.05.002. Epub 2019 Jul 26 [PubMed PMID: 31353143]
Abdelaziz AA, Sadek AA, Talaat M. Differential Diagnosis of Post Auricular Swelling with Mastoid Bone Involvement. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2019 Nov:71(Suppl 2):1374-1376. doi: 10.1007/s12070-018-1432-2. Epub 2018 Jun 24 [PubMed PMID: 31750180]
Suri NA, Meehan CW, Melwani A. A Healthy Toddler With Fever and Lethargy. Pediatrics. 2019 May:143(5):. pii: e20180412. doi: 10.1542/peds.2018-0412. Epub 2019 Apr 5 [PubMed PMID: 30952780]
Dorner RA, Ryan E, Carter JM, Fajardo M, Marsden L, Fricchione M, Higgins A. Gradenigo Syndrome and Cavitary Lung Lesions in a 5-Year-Old With Recurrent Otitis Media. Journal of the Pediatric Infectious Diseases Society. 2017 Sep 1:6(3):305-308. doi: 10.1093/jpids/pix018. Epub [PubMed PMID: 28903516]
Paradise JL, Hoberman A, Rockette HE, Shaikh N. Treating acute otitis media in young children: what constitutes success? The Pediatric infectious disease journal. 2013 Jul:32(7):745-7. doi: 10.1097/INF.0b013e31828e1417. Epub [PubMed PMID: 23435311]
Level 1 (high-level) evidenceTähtinen PA, Laine MK, Ruohola A. Prognostic Factors for Treatment Failure in Acute Otitis Media. Pediatrics. 2017 Sep:140(3):. pii: e20170072. doi: 10.1542/peds.2017-0072. Epub 2017 Aug 8 [PubMed PMID: 28790141]
Wanna GB, Dharamsi LM, Moss JR, Bennett ML, Thompson RC, Haynes DS. Contemporary management of intracranial complications of otitis media. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2010 Jan:31(1):111-7. doi: 10.1097/MAO.0b013e3181c2a0a8. Epub [PubMed PMID: 19887978]
Level 2 (mid-level) evidenceZhang X, Chen M, Zhang J, Yang Y, Liu ZY. [Clinical features of occult mastoiditis complicated with periphlcbitis of sigmoid sinus in children]. Lin chuang er bi yan hou tou jing wai ke za zhi = Journal of clinical otorhinolaryngology head and neck surgery. 2019 Dec:33(12):1158-1162. doi: 10.13201/j.issn.1001-1781.2019.12.010. Epub [PubMed PMID: 31914264]
Kasemodel ALP, Costa LEM, Monsanto RDC, Tomaz A, Penido NO. Sensorineural hearing loss in the acute phase of a single episode of acute otitis media. Brazilian journal of otorhinolaryngology. 2020 Nov-Dec:86(6):767-773. doi: 10.1016/j.bjorl.2019.06.001. Epub 2019 Jul 2 [PubMed PMID: 31324458]
Voitl P, Meyer R, Woditschka A, Sebelefsky C, Böck A, Schneeberger V. Occurrence of patients compared in a pediatric practice and pediatric hospital outpatient clinic. Journal of child health care : for professionals working with children in the hospital and community. 2019 Dec:23(4):512-521. doi: 10.1177/1367493519853431. Epub 2019 May 26 [PubMed PMID: 31129994]
Shetty KR, Wang RY, Shetty A, Levi J, Aaronson NL. Quality of Patient Education Sections on Otitis Media Across Different Website Platforms. The Annals of otology, rhinology, and laryngology. 2020 Jun:129(6):591-598. doi: 10.1177/0003489420902183. Epub 2020 Jan 24 [PubMed PMID: 31975608]
Level 2 (mid-level) evidence