Introduction
Acne keloidalis nuchae is a disease characterized by persistent folliculitis at the nape of the neck that forms keloid like scars and ultimately cicatricial alopecia. The disorder is most common in young African American males. The lesion occurs as a result of a folliculitis. [1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The exact etiology of acne keloidalis nuchae is unclear, but it might be triggered by chronic irritation or occlusion of the follicles due to hair cutting practices (e.g., close shaves), trauma, friction (e.g., rubbing from shirt collars or helmets), heat, or humidity as a predisposing or exacerbating factors. Also, It might be triggered by infection (Demodex or bacteria). Other potential contributory factors include autoimmunity, excess androgens or increased sensitivity to androgens, seborrhea, and medications (e.g., cyclosporine). [4][5]
Epidemiology
Individuals with darkly pigmented skin, especially African Americans, are more prone to developing acne keloidalis nuchae. It has been reported to affect young age group with a male-to-female ratio of approximately 20:1.
Pathophysiology
The repeated friction, trauma, and infection of the skin overlying the nape of the neck leads to acne keloidalis nuchae. Herzberg et al. proposed a series of ultrastructural events that are responsible for the formation of acne keloidalis nuchae:[6]
- Acute perifollicular inflammation followed by a weakening of the follicular wall at the level of the lower infundibulum, the isthmus, or both.
- Formation of acute and chronic granulomatous inflammation by the release of naked hair shaft which acts as a foreign body.
- The fibroblasts will produce new collagen and fibrosis.
- Distortion and occlusion of the follicular lumen by the fibrosis results in retention of the hair shaft in the follicle.
Histopathology
The histopathology of acne keloidalis nuchae depends on the timing of the biopsy. In general, there is an influx of neutrophils and lymphocytes distributed around the isthmus of the hair follicle and naked hair shafts in the dermis may also be visualized. As the condition progresses, one will see the destruction of the sebaceous glands. A chronic granulomatous inflammation reaction is common with evidence of collagen deposition and fibrosis. Sinus tracts may also be apparent when the fluid is discharged to the external skin. Ingrown hairs may be seen around the periphery of the papules.
History and Physical
Usually, physicians can diagnose acne keloidalis nuchae during the clinical presentation. It is easier to diagnose this condition by inspection and palpation, given its appearance and texture. History should also include trauma, hair-cutting routine, infection, and medications.
Acne keloidalis nuchae presents as a firm, dome-shaped, inflammatory papules and pustules over the nape of the neck. Over time, fibrosis ensues with coalescence of firm papules into keloidal scarring plaques. Scarring is typically present in the time patients present for medical evaluation. Scarring is manifested by variable sized keloidal papules, plaques, or nodules at the site of previously involved hair follicles.
Evaluation
The diagnosis of acne keloidalis nuchae is clinical, but laboratory studies are done to look for bacteria. If pathogenic microorganisms are isolated, then the appropriate antibiotics should be started. Rarely, a biopsy may be done to exclude psoriasis, cancer, or acne conglobata.
Treatment / Management
Management of acne keloidalis nuchae consists of measures directed at improving the clinical manifestations and symptoms of the disease.[1][7][8](B2)
Overall, the treatment of acne keloidalis nuchae is difficult and unsatisfactory. Over the years, many treatments have been used with varying degrees of success. There is no first-line therapy, and it all depends on the personal preference of the treating physician.
The first part of treatment is to educate the patient on preventing progression of the disease. This means avoiding close shaving and frequent haircuts. Secondly, the individual should be told to avoid shirts with tight collars and restrictive athletic neck gear. Any ornaments like chains worn around the neck should be discontinued.
The treatment should be initiated at the time of diagnosis to avoid cosmetic disfigurement. One may use topical antimicrobial agents such as benzoyl peroxide or chlorhexidine to prevent secondary bacterial infections.
- Mild keratolytic agents can help soften the coarse hairs.
- The patient should be told to avoid the use of all hair product greases that can interfere with hair growth.
- When the disease is in the early papular stage, it may respond to potent topical steroids with or without a retinoid.
- If folliculitis is present, one may need to use minocycline or doxycycline. Moderate dose isotretinoin (20 mg daily) has an anti-inflammatory effect on folliculitis but does not affect indurated lesions.
Once the acute disease is under control, one can use maintenance therapy with a topical steroid, benzyl peroxide washes, and a topical retinoid.
If the papules are hard, intralesional injection of triamcinolone can help reduce the size and also soften the lesion. The injections can be very painful, and pretreatment with topical lidocaine may help. Steroid injections may result in hypopigmentation and skin atrophy. Some dermatologists use cryotherapy with liquid nitrogen to create edema before the injection of steroids.
Cryotherapy has also been used as solo therapy, but it is often not well-tolerated because of pain. The treatment also causes hypopigmentation and often requires months of treatment.
Surgical excision may be performed, but mild recurrences are not rare. Cryosurgery also seems to be effective in acne keloidalis nuchae, while vaporization with the CO2 laser is less effective than surgery.
Various other types of lasers have been used to treat acne keloidalis nuchae with varying success. The most effective lasers are the 1064 nm Nd: YAG laser and 810 nm diode laser. Most patients require several laser sessions in combination with topical steroids or retinoids to improve the cosmesis. Pulsed Dye laser (595 nm) has also been used in acne keloidalis nuchae but is less effective than the other lasers. Phototherapy using targeted ultraviolet B light three times a week for 8 to 10 weeks has also been effective.
Radiation therapy should only be reserved for recalcitrant cases.
Differential Diagnosis
- Acne conglobata
- Acne vulgaris
- Acneiform eruptions
- Folliculitis decalvans
- Hidradenitis suppurativa
- Perifolliculitis capitis abscedens et suffodiens
Enhancing Healthcare Team Outcomes
The management of acne keloidalis is best done with an interprofessional team consisting of clinicians, nurses, and pharmacists. The disorder is not easy to treat and there is no one treatment that is suitable for all individuals. The nurse practitioner and primary care provider must educate the patient on removing the trigger factors.
Patient education is a critical step in improving active inflammation by avoiding potential exacerbating factors. Instruct the patient to avoid picking, rubbing, or scratching the affected area. Also, he needs to discontinue close shaving and trimming. Irritation by high-collared shirts should be avoided.
If acne keloidalis nuchae is diagnosed and treated early, the prognosis is good. However, once scarring has developed, the treatment is difficult, and most patients are left with a major cosmetic problem. The large plaques that occur also create poor body aesthetics and many males become withdrawn, shy, and depressed. Pruritus is common, and the constant scratching may lead to the breakdown of the papules and drainage. Finally, scarring alopecia results.[9]
Media
(Click Image to Enlarge)

Acne Keloidalis Nuchae, Follicular-based papules, Pustules Contributed by Daifallah M. Al Aboud, M.D.
(Click Image to Enlarge)
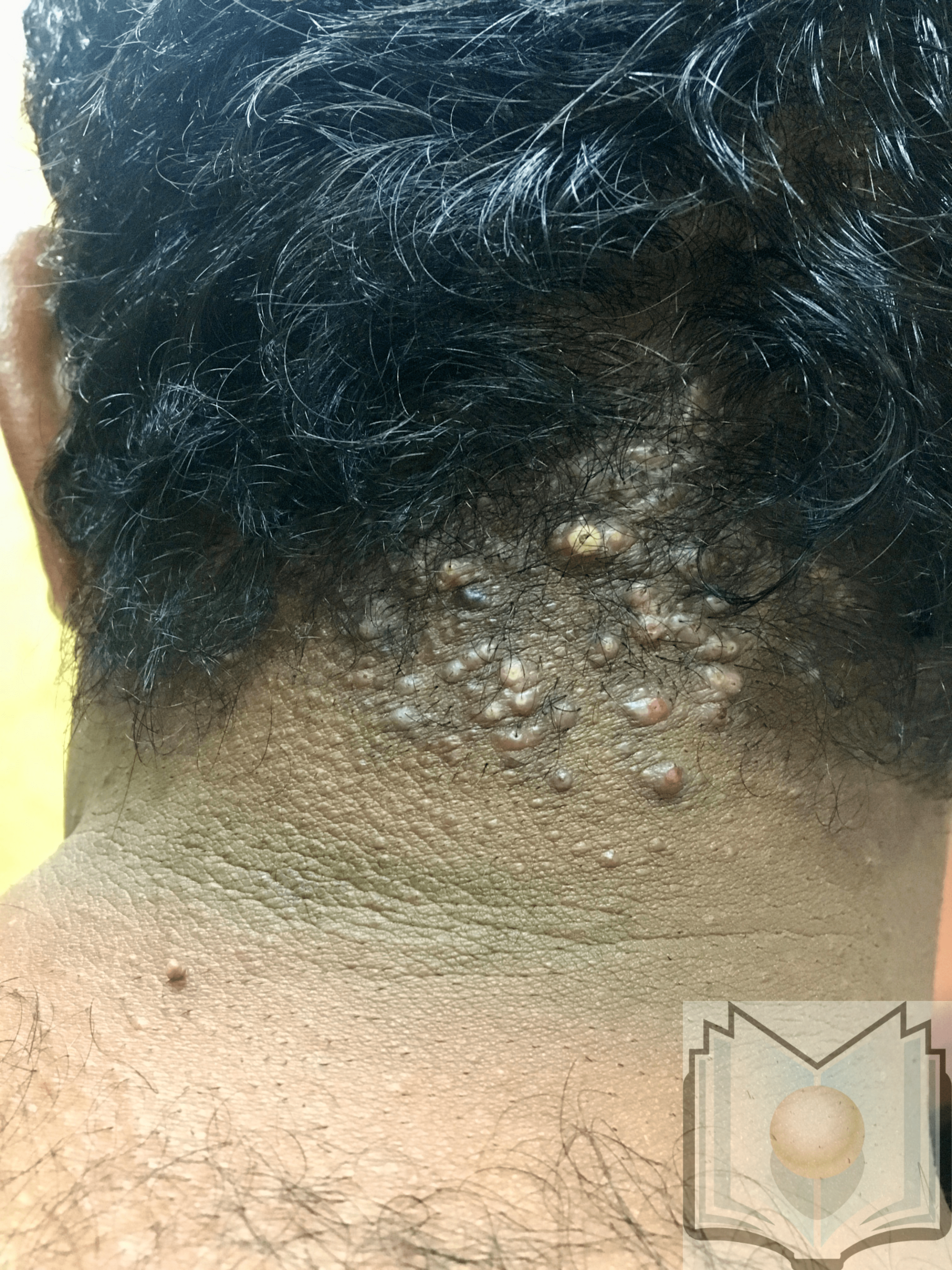
Acne keloidalis nuchae Contributed by Dr. Shyam Verma, MBBS, DVD, FRCP, FAAD, Vadodara, India
References
Gamil HD, Khater EM, Khattab FM, Khalil MA. Successful treatment of acne keloidalis nuchae with erbium:YAG laser: a comparative study. Journal of cosmetic and laser therapy : official publication of the European Society for Laser Dermatology. 2018 Nov-Dec:20(7-8):419-423. doi: 10.1080/14764172.2018.1455982. Epub 2018 May 14 [PubMed PMID: 29757041]
Level 2 (mid-level) evidenceNa K, Oh SH, Kim SK. Acne keloidalis nuchae in Asian: A single institutional experience. PloS one. 2017:12(12):e0189790. doi: 10.1371/journal.pone.0189790. Epub 2017 Dec 14 [PubMed PMID: 29240822]
Awosika O, Burgess CM, Grimes PE. Considerations When Treating Cosmetic Concerns in Men of Color. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2017 Nov:43 Suppl 2():S140-S150. doi: 10.1097/DSS.0000000000001376. Epub [PubMed PMID: 29064976]
Adotama P, Tinker D, Mitchell K, Glass DA 2nd, Allen P. Barber Knowledge and Recommendations Regarding Pseudofolliculitis Barbae and Acne Keloidalis Nuchae in an Urban Setting. JAMA dermatology. 2017 Dec 1:153(12):1325-1326. doi: 10.1001/jamadermatol.2017.3668. Epub [PubMed PMID: 29049485]
Loayza E, Vanegas E, Cherrez A, Cherrez Ojeda I. Acne keloidalis nuchae in Latin America: is there a different phenotype? International journal of dermatology. 2017 Dec:56(12):1469-1470. doi: 10.1111/ijd.13783. Epub 2017 Oct 3 [PubMed PMID: 28971477]
Herzberg AJ, Dinehart SM, Kerns BJ, Pollack SV. Acne keloidalis. Transverse microscopy, immunohistochemistry, and electron microscopy. The American Journal of dermatopathology. 1990 Apr:12(2):109-21 [PubMed PMID: 2331046]
Level 3 (low-level) evidenceTawfik A, Osman MA, Rashwan I. A Novel Treatment of Acne Keloidalis Nuchae by Long-Pulsed Alexandrite Laser. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2018 Mar:44(3):413-420. doi: 10.1097/DSS.0000000000001336. Epub [PubMed PMID: 29016541]
Ogunbiyi A. Acne keloidalis nuchae: prevalence, impact, and management challenges. Clinical, cosmetic and investigational dermatology. 2016:9():483-489. doi: 10.2147/CCID.S99225. Epub 2016 Dec 14 [PubMed PMID: 28008278]
Kundu RV, Patterson S. Dermatologic conditions in skin of color: part II. Disorders occurring predominately in skin of color. American family physician. 2013 Jun 15:87(12):859-65 [PubMed PMID: 23939568]