Introduction
An accessory spleen, also called a supernumerary spleen, a splenule, or a splenunculus, is a benign and asymptomatic condition in which splenic tissue is found outside the normal spleen. Accessory spleens are a relatively common phenomenon with an estimated 10% to 30% of the population having one. Typically, an individual can have anywhere from one to six accessory splenic buds. Furthermore, the size of an accessory spleen can also vary. Most accessory spleens are approximately 1 centimeter, but it is not uncommon to find accessory spleens larger than a few centimeters. [1] Accessory spleens typically form due to developmental anomalies and are often confused with splenosis which is another form of ectopic splenic tissue. Splenosis arises from trauma which results in a portion of the spleen breaking off and embedding itself somewhere else in the peritoneal cavity. The newly embedded ectopic splenic tissue recruits local blood supply and becomes functional splenic tissue. An accessory spleen can be distinguished from splenosis since an accessory spleen is functionally and histologically similar to normal splenic tissue, but splenosis is missing key splenic characteristics such as a thick capsule, smooth muscle elements, and a blood supply arising from the splenic artery. [2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The normal spleen is a versatile organ responsible for a variety of functions including filtering blood and producing immunity. Each function is carried out by specialized tissues in the spleen called red pulp and white pulp. Red pulp is made of connective tissue helping to form cords and sinuses containing white blood cells (WBCs). The sinuses create empty spaces which allow blood to flow through and be exposed to WBCs. This filtration helps to remove old and damaged red blood cells and destroy foreign microbes such as viruses, bacteria, and fungi. The white pulp, on the other hand, is more intricately divided than the red pulp. The white pulp consists of three areas including the periarteriolar lymphoid sheaths, lymph follicles, and marginal zone. The periarteriolar lymphoid sheaths are filled with T lymphocytes and surround the arteriole blood supply. The lymph follicles, on the other hand, are filled with B lymphocytes and are located between the periarteriolar lymphoid sheaths and the marginal zone. The marginal zone is filled with antigen-presenting cells. The white pulp as a whole is responsible for the production and maturation of WBCs. [3] The accessory spleen is morphologically and physiologically similar to a normal spleen and is therefore composed of a comparable subset of structures which carry out similar functions.
Embryology
Accessory spleens arise due to the incomplete fusion of mesenchymal buds during development. Accessory splenic tissue can develop along the path from the midline that the spleen takes during development, or follow the path of gonad descent. Around the fifth week of development, a primitive spleen begins to form from the mesoderm of the dorsal mesogastrium. The dorsal mesogastrium initially is midline with the foregut but during early development rotates to the left side as the foregut begins to take a rounder shape. After the dorsal mesocardium rotates around the foregut, the mesenchymal tissue from the dorsal mesocardium which gives rise to the spleen migrates over to its predetermined location approximately between what will become the ninth and eleventh ribs. If mesenchymal buds moving away from the midline path do not fuse together, then accessory spleens can form. An accessory spleen, however, can also be formed by the descent of the gonads during development. The spleen initially forms near the urogenital ridge, the site of gonad development. Due to their proximity during development, the gonads can become fused to splenic tissue. The gonads, as they develop, descend through the abdomen. If the gonads fuse with the spleen, they can forcibly drag splenic tissue with them in their descent. This forcible descent of splenic tissue can create either a continuous or broken line of splenic tissue, resulting in a condition known as splenogonadal fusion which creates accessory splenic tissue located in the pelvis or groin. [4]
Blood Supply and Lymphatics
A normal spleen receives its blood from the splenic artery. The splenic artery divides into branches before it reaches the spleen, and each of the branches proceeds to vascularize a subset of the organ. This helps to form individual subsets of splenic tissue, each with a blood supply independent of the others but arising from the same origin, the splenic artery. Accessory spleens, like normal splenic tissue, receive their blood supply from the splenic artery. Since accessory spleens receive blood from a feeding artery off of the splenic artery, accessory spleens can function as active, functional splenic tissue even in the case of a total splenectomy. [2]
Physiologic Variants
An accessory spleen can be found in different locations with about 75% of all accessory spleens occurring in the splenic hilum, the site at which blood vessels enter the spleen. The next most likely location to find accessory splenic tissue is near the tail of the pancreas, with about 20% of all accessory pancreatic tissue appearing here. The final 5% of accessory splenic tissue can be found in the gastrosplenic ligaments, the lienorenal ligaments, the wall of the stomach, the wall of the intestines, the greater omentum, the mesentery, or even the pelvis or scrotum. [2]
Surgical Considerations
The most likely case necessitating surgical removal of an accessory spleen independent of the removal of the normal spleen is torsion of an accessory spleen. Symptoms for this condition can include flank pain and nausea. Pain from the torsion can arise from inflammation due to infarction or strangulation, venous congestions due to twisting of the vascular pedicle, or direct interference with adjacent organs. Hemorrhagic shock, peritonitis, and bowel obstruction are potential consequences of untreated torsion of an accessory spleen. [5]
Clinical Significance
Accessory spleens become important in two clinical scenarios: splenectomies and imaging studies. In a clinical case necessitating a therapeutic splenectomy, it is necessary to remove accessory splenic tissue as well to resolve symptoms. If the accessory splenic tissue is not removed, then symptoms will continue because an accessory spleen is functional splenic tissue. Conditions that tend to necessitate this sort of management are blood disorders such as hemolytic anemia and chronic idiopathic thrombocytopenic purpura. Accessory spleens are also relevant when evaluating the results of imaging studies. When viewing an imaging test, particularly CT scans, accessory spleens can appear similar to lymph nodes, neoplastic growth, or splenosis. Diagnosis of an accessory spleen via imaging requires the use of nuclear medicine, particularly scintigraphy. Scintigraphy with 99mTc-nanocolloid can confirm accessory splenic tissue because splenic tissue will accumulate 99mTc-nanocolloid remarkably well once administered, whereas lymph nodes and neoplastic growth will not demonstrate uptake to the extent that accessory splenic tissue will. [6] An accessory spleen can be distinguished from splenosis based on appearance; an accessory spleen has a thick capsule and smooth muscle elements which stain positive for smooth muscle actin and receives its blood supply from the splenic artery.
Media
(Click Image to Enlarge)
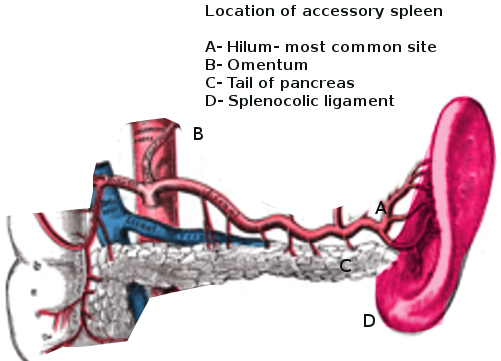
Accessory spleen Image courtesy S Bhimji MD
References
Mohammadi S, Hedjazi A, Sajjadian M, Ghrobi N, Moghadam MD, Mohammadi M. Accessory Spleen in the Splenic Hilum: a Cadaveric Study with Clinical Significance. Medical archives (Sarajevo, Bosnia and Herzegovina). 2016 Oct:70(5):389-391 [PubMed PMID: 27994303]
Yildiz AE, Ariyurek MO, Karcaaltincaba M. Splenic anomalies of shape, size, and location: pictorial essay. TheScientificWorldJournal. 2013:2013():321810. doi: 10.1155/2013/321810. Epub 2013 Apr 21 [PubMed PMID: 23710135]
MOORE RD, MUMAW VR, SCHOENBERG MD. THE STRUCTURE OF THE SPLEEN AND ITS FUNCTIONAL IMPLICATIONS. Experimental and molecular pathology. 1964 Feb:3():31-50 [PubMed PMID: 14117850]
Level 3 (low-level) evidenceVarga I, Galfiova P, Adamkov M, Danisovic L, Polak S, Kubikova E, Galbavy S. Congenital anomalies of the spleen from an embryological point of view. Medical science monitor : international medical journal of experimental and clinical research. 2009 Dec:15(12):RA269-76 [PubMed PMID: 19946246]
Ren C, Liu Y, Cao R, Zhao T, Chen D, Yao L, Pan Z. Colonic obstruction caused by accessory spleen torsion: A rare case report and literature review. Medicine. 2017 Sep:96(39):e8116. doi: 10.1097/MD.0000000000008116. Epub [PubMed PMID: 28953636]
Level 3 (low-level) evidenced'Amico A, Cofalik A, Przeorek C, Gawlik T, Olczyk T, Kalemba M, Modorowska A, Turska-d'Amico M, Bobek-Billewicz B, Jarzab B. Role of nuclear medicine imaging in differential diagnosis of accessory spleens in patients after splenectomy. Polish journal of radiology. 2012 Jan:77(1):68-71 [PubMed PMID: 22802870]
Level 3 (low-level) evidence