Introduction
The abdominal trunk is an area of special interest to plastic surgeons as it presents a large area of opportunity for body contouring. The trunk is a gross description of the area between the inferior aspect of the breasts and the beginning of the pelvis. The abdominoplasty, commonly referred to as a "tummy tuck," is a procedure to reduce the excess skin and fat around the abdomen and strengthen the abdominal wall musculature. The goal of this procedure is to develop an aesthetically pleasing abdomen, and can incorporate direct excisional techniques as well as liposuction. With the rise in bariatric surgery, the abdominoplasty has become a significant resource to help these patients with an excess abdominal tissue after their weight loss.[1]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The fat in the trunk is separated into distinct regions. It is divided by Scarpa's fascia into superficial and deep layers. The blood supply of the skin and fat of this area is supplied by perforating branches of the superior and inferior epigastric vessels. There are anchoring fascial areas, such as the anterior superior iliac spine (ASIS) and the umbilicus, which provide structural support for the abdominal skin. The inguinal and mons pubis zones of adherence are the most important because they maintain the structural integrity after abdominoplasty.
Indications
The reasons for undergoing abdominoplasty are numerous, including (1) men and women desiring aesthetic improvement of the abdomen, (2) women with significant skin and abdominal wall laxity following multiple pregnancies, or (3) bariatric patients who have excessive skin and/or pannus following significant weight loss. When selecting patients appropriate for surgery, it is vital to obtain a thorough history. Wound healing is of vital importance, and patients require good nutritional status, as well as optimal overall medical health. Bariatric patients present the plastic surgeon with specific challenges. The laxity of the skin after significant weight loss, as well as the potentially massive size of the skin apron, may require further dissection and may require additional adjunct procedures to lift the thigh, back, arm and flank areas to maintain overall symmetry of the body. Patients with lower BMI tend to have superior results, and patients with diabetes mellitus (DM) may be more prone to complications[2]. Patients with little to no fat and no abdominal wall laxity are optimal candidates for liposuction alone. Patients with minimal to moderate subcutaneous fat and minimal to moderate abdominal wall laxity which is located primarily in the infra-umbilical region are candidates for the "mini-abdominoplasty." Patients with excessive skin laxity, fat, and abdominal wall weakness are ideal candidates for full abdominoplasties[3].
Contraindications
Patients with poor health including advanced cardiopulmonary disease, cirrhosis, and uncontrolled diabetes are poor candidates for this procedure. Smoking is severely detrimental to the abdominoplasty, as the procedure requires an adequate blood supply. Many plastic surgeons consider current smoking a contraindication to the surgery. [4]
Equipment
No special equipment is needed for this procedure. If liposuction is to be added to the procedure, liposuction equipment should be available. Closed-suction should be readily available.
Personnel
Besides the surgeon, an assistant should be available to assist in retraction and can aid in closing the many layers associated with abdominoplasty.
Preparation
A patient's medical health should be optimized before surgery. Appropriate medical clearances should be obtained well in advance to identify any underlying illnesses that would preclude the patient from the procedure and should be tailored to each patient's medical history. Appropriate antibiotics should be given in the preoperative period to reduce skin flora contamination of the wound.
Technique or Treatment
The incision is extensive and is typically made from ASIS to ASIS through the natural suprapubic crease. This positions the final scar low enough on the trunk to be hidden in the bikini line. A flap between the fascia and fat is then created superiorly to the costal margin, following it until the xiphoid process is reached. The umbilicus is circumferentially dissected from the flap, leaving it attached to the abdomen by the umbilical stalk and fat. Special care is needed to leave enough of a fat pad circumferentially around the umbilicus to avoid ischemia and necrosis, as the plexus surrounding the umbilical stalk contains its blood supply. Once the flap is raised, the patient is flexed in the bed to re-drape the flap and determine its final position at the previous incision, and the excess skin is then marked. The fascia of the rectus muscle is then plicated with long-lasting absorbable suture such as polydioxanone (PDS) suture to reinforce the abdominal wall. Some surgeons prefer permanent sutures such as nylon or Prolene, though reports of local reactions and extrusion do exist.[5] After careful measurement, the marked excess skin and fat are excised and the superior flap is reapproximated to the lower incision in multiple suture layers to strengthen the closure and avoid tension on the skin layer, optimizing healing of the final scar. The umbilicus is then transplanted into the flap, and many techniques have been described for successful omphaloplasty with the choice left to the discretion of the individual surgeon and patient scenario[6].
Special Considerations
The abdominoplasty can be catered to each patient's body habitus by altering the procedure slightly. The use of liposuction can aid in the removal of excess fat in the lateral flanks and upper thighs to help smooth the contours of the abdominoplasty. A panniculectomy (essentially an abdominoplasty without the rectus muscle plication) can be of significant benefit in patients who have had extreme weight loss. The blood flow to the abdomen is better maintained in this procedure since it is not necessary to extend dissection to the xiphoid process. This ensures sufficient blood flow after significant weight loss and excessively flaccid skin aprons. A "mini-abdominoplasty" (wherein minimal skin and fat are excised but the rectus muscle is plicated and re-enforced) is ideal for patients who are not overweight and present with infra-umbilical abdominal wall laxity and minimal skin and fat excess. These patients are classically women at a healthy weight who have had one or two children but have maintained good skin laxity[7].
Postoperatively, it is important that the patient remains in a flexed (Semi-Fowler) position for 2 weeks. This positioning helps avoid excessive straining on the incision and reduce the risk of hypertrophic scar formation. A belt lipectomy can be considered in patients with significant flank, buttock, and thigh fat. This is a circumferential lipectomy which can add the benefits of a thigh and buttock lift to the abdominoplasty. Closed suction drains and oral antibiotics are used at the discretion of the surgeon but have shown only anecdotal benefits in preventing infection and other complications such as seroma and hematoma formation[8].
Complications
Seromas and hematomas are relatively common postoperative complications, occurring in up to 1/3 of cases[5]. If left untreated, these can result in necrosis of the flap from lack of blood supply or infections which can destroy the flap and are potentially life-threatening. Placement of closed-suction drainage systems can help decrease the incidence of accumulation of these fluids anecdotally, though high-quality data are not available to demonstrate efficacy[5]. Vascular compromise to the umbilicus is an important complication to avoid. Careful dissection of the umbilical stalk is directed at maintaining enough fat around the umbilicus to preserve adequate blood supply. Superficial wound complications remain the most common complications for this patient population. Infection and wound dehiscence can result when excessive tension is borne by the closure, particularly the subdermal and skin layers. Patients are usually placed in the "Semi-Fowler" position to minimize these complications, but even with ideal positioning the rate remains significant. [9][10]
Clinical Significance
When performed by experienced surgeons on properly selected patients, the majority of patients remain satisfied with the results after abdominoplasty. However, it is vital to educate patients on changes in lifestyle to prevent reaccumulation of fat around the waist area. This means participating in regular physical exercise, eating a healthy diet, discontinuing smoking, and refraining from excess alcohol.
Enhancing Healthcare Team Outcomes
Abdominoplasty is a major procedure and can be associated with serious complications. One significant complication is wound infection, which can prolong admission, worsen cosmesis and lead to an increase in healthcare costs. Thus it is imperative to identify risk factors and perform a thorough assessment of the patient prior to any surgery, and to refrain from such elective procedures until patients are at their medical optimum. [11] A team approach is an ideal way to minimize complications of this procedure. Prior to surgery, the following should be considered for each patient:
- Pulmonary and cardiology evaluation to optimize lung and heart function
- Instruction in incentive spirometer use, often with a nurse educator
- Evaluation by the anesthesiologist to ensure that the patient is fit for general anesthesia
- Psychological evaluation to ensure the patient has realistic expectations regarding surgical and aesthetic outcomes, particularly in post-weight loss patients
- Nutritionist consult to maintain healthy eating habits postoperatively
Evidence-based Approach
An interprofessional team that provides a holistic and integrated approach to postoperative care can help achieve the best possible outcomes. If a surgical wound infection occurs, the role of the diagnostic laboratory cannot be understated, allowing culture and antibiotic susceptibility to be accurately determined. If the patient is to be discharged home with a drain, consultation should be made with a social worker and community nurses who can monitor the patient as needed at home while the drain is in place, and educate them on the care of the drain before discharge.
Collaboration, shared decision making, and communication are key elements for good patient outcomes. The inter-disciplinary care provided to the patient must use an evidence-based approach to pre- and post-operative planning and evaluation.[12] The earlier signs and symptoms of a complication are identified, the better the prognosis and outcome.[9]
Media
(Click Image to Enlarge)
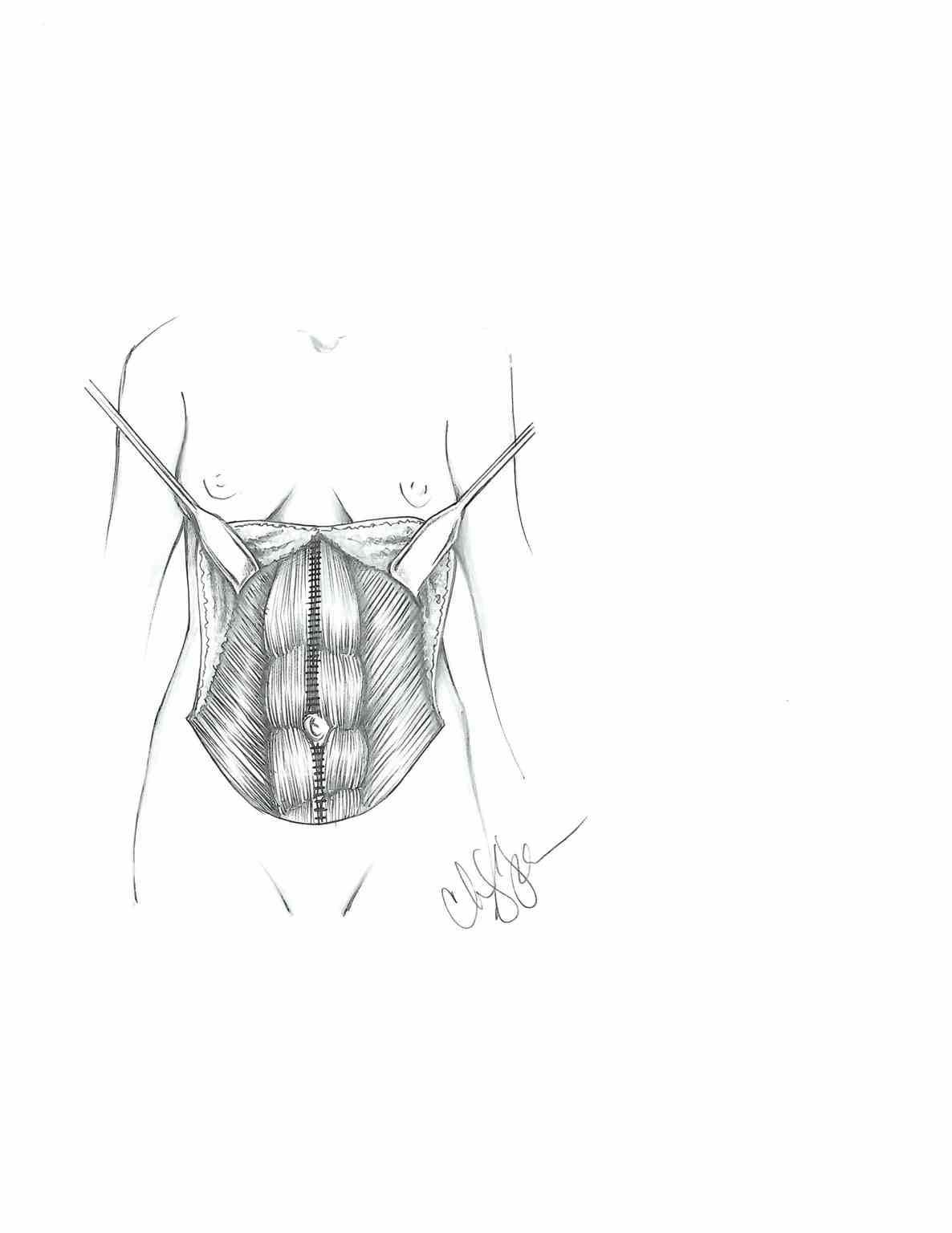
Abdominoplasty After Plication of the Rectus Muscle
Contributed Illustration by Christopher Palu
(Click Image to Enlarge)

Prune belly syndrome - A. At birth B. At nine years of age (surgical scars noted from a prior abdominoplasty procedure) Contributed by Senthilkumar Sankararaman, MD
References
Hafezi F, Nouhi A. Safe abdominoplasty with extensive liposuctioning. Annals of plastic surgery. 2006 Aug:57(2):149-53 [PubMed PMID: 16861993]
Hunecke P, Toll M, Mann O, Izbicki JR, Blessmann M, Grupp K. Clinical outcome of patients undergoing abdominoplasty after massive weight loss. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery. 2019 Aug:15(8):1362-1366. doi: 10.1016/j.soard.2019.06.001. Epub 2019 Jun 12 [PubMed PMID: 31296446]
Level 2 (mid-level) evidenceFrank K, Hamade H, Casabona G, Gotkin RH, Kaye KO, Tiryaki T, Freytag DL, Bialowas C, Koban KC, Cotofana S. Influences of Age, Gender, and Body Mass Index on the Thickness of the Abdominal Fatty Layers and its Relevance for Abdominal Liposuction and Abdominoplasty. Aesthetic surgery journal. 2019 Sep 13:39(10):1085-1093. doi: 10.1093/asj/sjz131. Epub [PubMed PMID: 31056694]
Gupta V, Winocour J, Rodriguez-Feo C, Bamba R, Shack RB, Grotting JC, Higdon KK. Safety of Aesthetic Surgery in the Overweight Patient: Analysis of 127,961 Patients. Aesthetic surgery journal. 2016 Jun:36(6):718-29. doi: 10.1093/asj/sjv268. Epub 2016 Feb 9 [PubMed PMID: 26895958]
Ho W, Jones CD, Pitt E, Hallam MJ. Meta-analysis on the comparative efficacy of drains, progressive tension sutures and subscarpal fat preservation in reducing complications of abdominoplasty. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2020 May:73(5):828-840. doi: 10.1016/j.bjps.2019.11.066. Epub 2020 Feb 1 [PubMed PMID: 32057746]
Level 2 (mid-level) evidenceVallim MG, Calderoni DR, Bueno MA, Motta MM, Basso RC, Kharmandayan P. Patient Versus Surgeon Preferences Between Traditional and Neo-omphaloplasty in Post-bariatric Abdominoplasty. Aesthetic plastic surgery. 2017 Feb:41(1):102-107. doi: 10.1007/s00266-016-0753-3. Epub 2016 Dec 28 [PubMed PMID: 28032175]
Hoyos AE, Perez ME, Castillo L. Dynamic definition mini-lipoabdominoplasty combining multilayer liposculpture, fat grafting, and muscular plication. Aesthetic surgery journal. 2013 May:33(4):545-60. doi: 10.1177/1090820X13484493. Epub [PubMed PMID: 23636628]
Level 2 (mid-level) evidenceAriyan S, Martin J, Lal A, Cheng D, Borah GL, Chung KC, Conly J, Havlik R, Lee WPA, McGrath MH, Pribaz J, Young VL. Antibiotic prophylaxis for preventing surgical-site infection in plastic surgery: an evidence-based consensus conference statement from the American Association of Plastic Surgeons. Plastic and reconstructive surgery. 2015 Jun:135(6):1723-1739. doi: 10.1097/PRS.0000000000001265. Epub [PubMed PMID: 25724064]
Level 1 (high-level) evidencePallara T, Del Buono R, Marangi GF, Langella M, Toto V, Persichetti P. Outcomes of traditional cosmetic abdominoplasty in a community setting: a retrospective analysis of 1008 patients. Plastic and reconstructive surgery. 2013 Nov:132(5):863e-864e. doi: 10.1097/PRS.0b013e3182a4c3e8. Epub [PubMed PMID: 24165640]
Level 3 (low-level) evidenceBertheuil N, Carloni R, Herlin C, Watier E, Chaput B. Abdominoplasty: Risk Factors, Complication Rates, and Safety of Combined Procedures. Plastic and reconstructive surgery. 2016 Jun:137(6):1051e-1052e. doi: 10.1097/PRS.0000000000002197. Epub [PubMed PMID: 26890513]
Massenburg BB, Sanati-Mehrizy P, Jablonka EM, Taub PJ. Risk Factors for Readmission and Adverse Outcomes in Abdominoplasty. Plastic and reconstructive surgery. 2015 Nov:136(5):968-977. doi: 10.1097/PRS.0000000000001680. Epub [PubMed PMID: 26505701]
Gutowski KA. Evidence-Based Medicine: Abdominoplasty. Plastic and reconstructive surgery. 2018 Feb:141(2):286e-299e. doi: 10.1097/PRS.0000000000004232. Epub [PubMed PMID: 29373443]