Introduction
Osteomyelitis is a multifaceted disease characterized by inflammation of bone and marrow. While various etiologies of osteomyelitis have been documented, it is almost always secondary to infection. Osteomyelitis may occur through direct inoculation of bacteria into the bone, hematogenous spread from distant sites of infection, or the contiguous spread from nearby soft tissues, termed nonhematogenous infection. Common causative organisms of osteomyelitis include Staphylococcus aureus, Streptococcus spp., and Enterobacteriaceae. In patients with specific comorbidities, such as sickle cell disease, other etiologic infectious agents, such as Salmonella spp. and Escherichia coli, are more common.[1]
In the pediatric population, osteomyelitis typically affects the long bones and results from hematogenous spread. In adults, however, osteomyelitis is more commonly due to nonhematogenous contiguous spread from surgery, trauma, soft tissue infection, or prosthetic material. Patients with diabetes are at an increased risk of osteomyelitis, particularly if vascular function is compromised.[2]
Osteomyelitis may be acute, subacute, or chronic. Patients with acute osteomyelitis typically present within 2 weeks of disease onset with local symptoms of progressive erythema, edema, and warmth. Constitutional symptoms such as fever, chills, irritability, decreased appetite, lethargy, or malaise may also occur. Pediatric patients with acute osteomyelitis may present with localized symptoms but frequently present with a refusal to bear weight or limited motion of the affected extremity.
Patients with subacute osteomyelitis present after the initial 2 weeks of symptoms, often with mild pain and minimal fever. Septic arthritis can occur if the joint capsule is involved. Brodie abscess is a subacute form of osteomyelitis typically arising through hematogenous spread but may occur secondary to trauma. The classic presentation of Brodie abscess is a cavity in the metaphysis of a long bone, filled with suppurative or granulation material and surrounded by dense fibrous tissue and sclerotic bone.[3]
Chronic osteomyelitis develops when acute osteomyelitis is inadequately treated, or the infection does not respond to standard therapies. Symptoms of chronic osteomyelitis include edema, pain, and erythema at the site of infection; fever is less common. The defining characteristic of chronic osteomyelitis is the presence of necrotic bone, known as a sequestrum. Other typical features of chronic osteomyelitis include reactive bony encasement of the sequestrum, called an involucrum, and localized bone loss. In chronic osteomyelitis, there is potential for the development of sinus tracts if the infection extends through the infected cortical bone.[4]
Chronic recurrent multifocal osteomyelitis (CRMO) is not a subtype of chronic osteomyelitis but a unique inflammatory condition primarily affecting the pediatric population. CRMO is not an infectious process but an autoinflammatory disorder in which the immune system mistakenly targets the bone. The characteristic feature of CRMO is the presence of multiple bony lesions in various anatomical locations, typically long bones, clavicles, or vertebrae. Patients with CRMO experience recurrent episodes of bone pain, swelling, and tenderness. However, systemic symptoms like fever and weight loss are usually absent. Diagnosing CRMO can be challenging due to intermittent and nonspecific symptoms. Imaging modalities such as magnetic resonance imaging (MRI) are crucial in identifying the bone marrow edema and inflammatory patterns associated with CRMO. MRI also aids in distinguishing the bony abnormalities of CRMO from bony metastases.[5]
The adult counterpart of CRMO is SAPHO syndrome, defined as the combined occurrence of synovitis, acne, pustulosis, hyperostosis, and osteitis. Compared to patients with CRMO, patients with SAPHO syndrome have a significantly higher prevalence of skin lesions, particularly palmoplantar pustulosis.[6] The bony lesions of SAPHO syndrome are primarily seen in the chest wall and pelvis, while CRMO typically targets the long bones. This contrast is believed to be secondary to age-related metaphyseal development; open growth plates in children increase the likelihood of metaphyseal lesions. The involvement of the sternoclavicular and first sternocostal joint and ossification of the costoclavicular ligaments is frequently observed in SAPHO syndrome but not reported in CRMO.[7]
Diagnosing osteomyelitis relies on clinical evaluation, laboratory testing, and imaging studies. Imaging techniques, including x-rays, MRI, computed tomography (CT), and nuclear medicine studies such as bone scintigraphy, gallium scanning, and 18F-fluorodeoxyglucose positron emission tomography-CT (18F-FDG PET-CT), play a crucial role in identifying the early and chronic changes of osteomyelitis. Imaging findings may aid the diagnosis of osteomyelitis and play a role in determining disease complications and guiding treatment strategies.[8]
Osteomyelitis is a complicated and potentially devastating clinical condition. Advances in understanding its pathogenesis, antibiotic development, and improved imaging techniques have revolutionized the management of osteomyelitis. The early recognition of osteomyelitis promotes rapid intervention, minimizing morbidity and optimizing patient outcomes.
Anatomy
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy
Bone is a complex organ comprising cortical or compact bone and trabecular or spongy bone. Cortical bone forms the outer layer of the bone, providing strength and protection. Trabecular bone forms the inner matrix of the bone and consists of a network of interconnected trabeculae crucial in maintaining the integrity and function of the bone.[9]
Various components of bone play an integral role in the pathophysiology of acute osteomyelitis. The medullary cavity, located within the center of long bones, contains bone marrow and hematopoietic stem cells. In acute osteomyelitis, bacteria may infiltrate the medullary cavity, leading to infection and subsequent destruction of bone tissue.[10] Bones rely on a rich vascular network to supply nutrients and oxygen to the bone tissues. This vascular supply stems from arteries that penetrate the bone through nutrient foramina and anastomose within the bone itself. Osteomyelitis can disrupt the blood supply, leading to potential bone necrosis.[11]
Various soft tissues adjacent to bone are affected by osteomyelitis and can contribute to the pathophysiologic process. The periosteum, a fibrous membrane covering the outer surface of bones, can become inflamed and contribute to the spread of infection. The infectious process can also affect the surrounding muscles, tendons, and ligaments.[12]
A thorough understanding of the anatomical aspects of osteomyelitis allows healthcare professionals to make accurate diagnoses, plan appropriate interventions, and facilitate effective management of the condition.[13] Imaging modalities such as plain radiography, CT, and MRI can help visualize the bony structural changes, soft tissue involvement, and extent of infection in osteomyelitis. Surgical intervention, such as drainage and debridement, may be necessary to remove infected tissue and restore bone health. Antibiotics are typically prescribed to combat the bacterial infection and prevent further spread.
Plain Films
Plain radiography is typically the initial imaging modality employed in cases of suspected osteomyelitis due to its accessibility, cost-effectiveness, and ability to provide valuable information about bone integrity and gross osseous changes.
Early signs of osteomyelitis on plain radiographs can be observed in adjacent soft tissues as swelling, with or without displacement or obscuration of the soft tissue plane. Osseous changes become apparent 10 to 14 days after infection and may include decreased bone mineralization, periosteal reaction, focal resorption of the inner cortical layer, lytic lesions, or new bone formation (see Image. Acute Osteomyelitis, Right Hand, Plain Radiograph). Soft tissue gas may also indicate osteomyelitis.[14][15]
In chronic osteomyelitis, plain radiographs may reveal thickened and irregular bone with sclerosis and a nonaggressive periosteal reaction. If present, a sequestrum will appear as a focal sclerotic lesion with a surrounding radiolucent border, and the involucrum will appear as an irregular cortical thickening adjacent to the sequestrum. A cloaca is another possible finding of chronic osteomyelitis, appearing as a lucent gap in the cortical surface that allows clearance of pus or other material from the osseous structure into the nearby soft tissues (see Image. Chronic Osteomyelitis, Plain Radiography).[8]
A distinctive hallmark of subacute osteomyelitis is a Brodie abscess, typically occurring at a metaphysis, most commonly that of the tibia. When visualized on a plain radiograph, a Brodie abscess frequently manifests as an oval-shaped area of decreased density, forming a lucent lesion. This lesion aligns with the longitudinal axis of the bone and is encased by a dense rim of reactive sclerosis.[16]
Plain radiography is also helpful in ruling out stress fractures as the etiology of the patient's symptoms. Stress fractures may be difficult to visualize for several weeks; when seen early in the disease process, they appear as linear lucencies with some peripheral sclerosis.
The limited sensitivity of plain radiographs in diagnosing early osteomyelitis has led to the early utilization of other imaging modalities, such as MRI and bone scintigraphy; both offer greater accuracy and efficiency in promptly detecting osteomyelitis.[14]
Computed Tomography
Computed tomography (CT) can provide valuable information in evaluating osteomyelitis and complement findings revealed with other imaging modalities. CT offers excellent multiplanar reconstructions of axial images into coronal and sagittal images, enabling the detection of subtle bony changes. CT is particularly valuable in evaluating pathophysiologic and morphologic changes associated with chronic osteomyelitis.[17]
The superior bony resolution of CT compared to MRI is particularly effective in detecting intraosseous gas, sequestra, cloacae, and involucra in cases of chronic osteomyelitis (see Image. Chronic Osteomyelitis, Computed Tomography). Detecting sequestered areas of bone assists in determining appropriate treatment approaches. Moreover, CT is a valuable tool in guiding needle biopsies and joint aspirations, particularly in cases of vertebral osteomyelitis. Additionally, contrast-enhanced CT is useful for detecting sinus tracts in the soft tissues.[14]
However, CT demonstrates limitations in assessing soft tissue changes, such as bone marrow edema and soft tissue swelling, findings which are important early indicators of osteomyelitis. CT may not provide sufficient contrast resolution for identifying soft tissue changes accurately and is limited in revealing the muscle and other soft tissue involvement that can help make a definitive diagnosis. MRI is the imaging modality of choice in detecting early changes of osteomyelitis, particularly soft tissue changes such as bone marrow edema and fluid collections.[8]
The use of CT may also be limited, particularly in young children, due to concerns about exposure to ionizing radiation. Additionally, certain metals in or near the anatomical region affected by osteomyelitis can significantly reduce CT image resolution due to beam-hardening artifacts. Metal artifacts may also preclude the use of MRI.[8]
Magnetic Resonance
MRI permits detailed multiplanar imaging of the affected bone and its surrounding soft tissues in patients with osteomyelitis. The outstanding contrast resolution of MRI has provided significant advancements in diagnosing osteomyelitis over the last two decades.
The soft tissue contrast resolution of MRI allows the visualization of early inflammatory changes, edema, and abscess formation. MRI can accurately assess the extent of bone marrow involvement and identify associated soft tissue complications such as cellulitis or deep abscesses. MRI can allow rapid comparison of contralateral body parts without radiation cost.[18]
The earliest indication of acute osteomyelitis revealed by MRI is bone marrow edema, which can be observed as soon as 1 to 2 days following the onset of infection. Early identification of characteristic findings eliminates waiting for the traditional 10 to 14 days required to diagnose osteomyelitis using plain radiography. Bone marrow contains fat and normally results in high signal intensity on T1-weighted MR images. In acute osteomyelitis, the bone marrow becomes congested with fluid and pus, producing low T1-weighted signal intensity and high signal intensity on fluid-sensitive and post-contrast sequences such as short tau inversion recovery (STIR).[8] Imaging of the contralateral extremity may be helpful for comparison in cases of suspected osteomyelitis.[19]
MRI also plays a crucial role in evaluating chronic osteomyelitis. MRI assesses the spread of infection within the bone and surrounding soft tissues and may identify important features such as abscesses, sequestra, and sinus tracts. The necrotic bone fragments of sequestra appear as areas of low signal intensity on T1, T2, and STIR sequences and do not exhibit enhancement. Other characteristic MRI findings of chronic osteomyelitis include Brodie abscess, thickened periosteum, sequestra, and cloacae. Cancellous bone sequestra, although not enhancing, demonstrate relatively higher signal intensity than cortical sequestra on T1, T2, and STIR sequences. Granulation tissue, soft tissue inflammation, and sinus tracts exhibit T1 hypointensity, T2 and STIR hyperintensity, and enhancement after contrast administration.[8]
Intraosseous and subperiosteal abscesses exhibit a low signal intensity, while fluid-sensitive sequences show a high signal intensity surrounding the abscess. Hypervascular granulation tissue, represented by a thin intermediate signal rim on T1, can be observed around the abscess. The peripheral granulation tissue enhances upon administration of contrast, while the central pus-filled cavity maintains a low signal intensity (see Image. Acute Osteomyelitis, Magnetic Resonance Imaging). This distinct pattern of peripheral enhancement is called the penumbra sign and helps distinguish abscesses from phlegmon, which do not have surrounding walls. Phlegmons, characterized as solid inflammatory masses, typically demonstrate more heterogeneous enhancement than the discrete peripheral enhancement seen in abscesses. Unlike phlegmon, the diagnosis of an abscess necessitates surgical intervention.[8][20][21]
Both acute and chronic osteomyelitis can display a cloaca, a defect in the cortical bone enabling the drainage of pus from the medulla to the adjacent soft tissues. Fluid-sensitive sequences facilitate the identification of a cloaca; the pus contained within the cloaca will display a pronounced high signal intensity.[8]
In patients with suspected CRMO, MRI can be utilized to assess for marrow edema if plain radiographs are negative despite significant clinical symptoms. If clinical findings and the initial imaging evaluation point towards a diagnosis of CRMO, assessment with a comprehensive whole-body MRI is recommended to detect potentially asymptomatic lesions in this multifocal disease. Whole-body MRI is increasingly used to assess multifocal bone lesions instead of the more traditional technetium Tc 99m (99mTc) bone scintigraphy.[7]
While MRI offers numerous benefits in evaluating patients with osteomyelitis, there are situations where it may not be a feasible imaging modality. Absolute contraindications to MRI include the presence of a permanent cardiac pacemaker or intracranial aneurysm coils. In patients with metallic prostheses, the utility of MRI is limited due to susceptibility artifacts, although techniques to mitigate metallic artifacts are becoming more available. Sedation or general anesthesia may be necessary for pediatric patients requiring MRI. Additionally, the cost and limited accessibility of MRI remain significant considerations in many regions of the world. These limitations make it imperative for the radiologist to be aware of alternative imaging methods to evaluate for suspected osteomyelitis.[19]
Ultrasonography
Ultrasonography (US) is not commonly employed as the primary imaging modality for patients with osteomyelitis due to operator dependence and its limitations in assessing bony changes associated with osteomyelitis.[8] The significant difference in acoustic impedance between bone and soft tissue results in a large portion of the ultrasound wave reflecting at the bone-soft tissue interface. This reflection causes acoustic shadowing or attenuation of the ultrasound signal beyond the bone, making it challenging to visualize structures behind the bone using standard US techniques.[22] US is considered more sensitive for diagnosing acute osteomyelitis in children as the periosteal reaction is more pronounced in the immature skeleton, mainly in tubular bones, due to its relatively weak attachment to the underlying bone. The periosteum appears thicker in children than the barely visible hypoechoic band in adults.[23]
The initial signs of osteomyelitis revealed by US include juxtacortical soft tissue swelling, visualized as increased echogenicity in the subcutaneous fat with a lack of distinction between the fat and dermis, and increased vascular flow in affected tissues on color Doppler imaging. US may also reveal periosteal thickening during an earlier phase of osteomyelitis.[24] Findings such as periosteal elevation with underlying subperiosteal fluid can be observed as a collection near the echogenic cortex which should raise a strong suspicion of osteomyelitis. Such fluid collection can progress and develop into a subperiosteal abscess, typically seen 4 to 6 days after symptoms start.[25] US enables sequential measurements of the subperiosteal abscess, which can aid in guiding management, especially in children who show inadequate response to therapy.[26] US is useful for guiding percutaneous interventions such as aspiration or drainage.
US offers the advantages of real-time imaging, a lack of ionizing radiation, and portability, making it a valuable tool in specific clinical scenarios.[27] However, a normal ultrasonographic examination of the concerned area does not entirely rule out osteomyelitis; subsequent MRI is recommended.[8]
Nuclear Medicine
Bone scintigraphy has played a role in diagnosing osteomyelitis since 1975, as demonstrated by several seminal articles. The groundbreaking research by Duszynski et al revealed the ability of bone scans to identify osteomyelitis even before radiographic abnormalities became evident. Gilday et al further advanced the field by introducing the blood-pool image, a precursor to the current three-phase bone scan. Deysine et al proposed using gallium 67 for studying chronic and postoperative osteomyelitis.[17][28][29][30]
Nuclear imaging techniques add value to the evaluation of suspected osteomyelitis when MRI or CT is not possible due to metallic interference or contraindications. Various scintigraphic modalities are available to evaluate suspected osteomyelitis, including 18F-FDG PET-CT, single-photon emission CT (SPECT), and gamma cameras. Gamma cameras provide planar images; the other modalities offer cross-sectional image sets.[31]
These imaging methods rely on radiotracers, which can be used alone, as in the case of gallium 67, or combined with other molecules or cells that target areas of infection. Examples of such tracers include 99mTc, Indium 111 (111In), and F 18 [18F]. Tracers may be combined with leukocytes, such as [111In]-WBC, phosphonates, such as 99mTc methylene diphosphonate ([99mTc]-MDP), or a glucose analog, as in [18F] fludeoxyglucose ([18F]-FDG). SPECT and gamma cameras utilize the same isotopes; multiple techniques are often employed during the same examination.[32]
Nuclear imaging generally demonstrates high sensitivity in detecting inflammation and is more reliable when evaluating acute infections than chronic infections. However, a limitation of nuclear studies is the potential for confusion between radiographic evidence of bone turnover or inflammation due to noninfectious bone conditions and osteomyelitis.[33][34][35][36] Conditions such as recent trauma or surgery, recently healed osteomyelitis, septic arthritis, degenerative joint disease, bone tumors, and Paget disease of bone can mimic osteomyelitis on nuclear imaging.[37][38]
The typical nuclear medicine techniques used for the detection of foci of osteomyelitis are bone scintigraphy using [99mTc]-MDP or gallium 67 and [18F]-FDG PET-CT.
[99mTc]-MDP Bone Scintigraphy
Bone scintigraphy is commonly performed using [99mTc]-MDP as a tracer. [99mTc]-MDP is a radioactive substance that binds to hydroxyapatite crystals in the bone; its uptake depends on blood flow and the rate of new bone formation. When osteomyelitis is suspected, a 3-phase bone scan is typically conducted.
The 3-phase bone scan includes 3 stages: a dynamic imaging sequence known as the flow or perfusion phase, followed by static images of the region of interest during the blood pool or soft tissue phase. The third phase, the bone phase, involves acquiring images of the area of interest 2 to 4 hours after the injection. Focal hyperperfusion, focal hyperemia, and increased bony uptake are characteristic findings of osteomyelitis on a 3-phase bone scan.[39]
The 3-phase bone scan can help in distinguishing osteomyelitis and cellulitis. Cellulitis is typically associated with findings of increased perfusion and diffusely increased soft tissue activity on early images. These findings indicate heightened blood flow and inflammation within the soft tissues. However, there is no concurrent observable increase in bony activity on delayed images of patients with cellulitis. In contrast, findings consistent with osteomyelitis are increased activity on the flow and blood pool phases of imaging and osseous uptake during the delayed phase indicating active bone infection and inflammation.[40]
The 3-phase bone scan is sensitive and specific for diagnosing osteomyelitis in bones unaffected by underlying conditions. However, in preexisting conditions such as degenerative joint disease, fractures, or orthopedic hardware, the specificity is reduced due to overall new bone formation.[41]
The 3-phase scan images of a 74-year-old man with type 2 diabetes mellitus and a foot ulcer are provided. The initial blood flow image reveals diffusely increased activity in the mid and distal foot (Image. Three-phase Bone Scintigraphy; Flow Phase). The immediate blood pool image (Image. Three-phase Bone Scintigraphy; Blood Pool Phase) and bone phase image show increased activity involving the midfoot in the expected region of the 1st and 2nd metatarsals suggesting osteomyelitis (Image. Three-phase Bone Scintigraphy; Bone Phase).
Gallium 67 Bone Scintigraphy
Gallium scanning is a nuclear medicine technique in which radioactive gallium attaches to transferrin. In an inflammatory state, such as infection, malignancy, or sterile inflammation, transferrin extravasates from the bloodstream into inflamed areas. When gallium is attached to transferrin, the isotope demonstrates increased uptake in areas of active inflammation.
Scanning is typically performed 18 to 72 hours after a gallium injection and is frequently performed concurrently with [99mTc]-MDP bone scintigraphy. However, gallium scanning does not provide detailed visualization of bone structures and may not effectively distinguish between bony and soft tissue inflammation.[42] Gallium 67 emits gamma radiation and has a long half-life, resulting in a higher radiation burden than other radiopharmaceuticals used in bone imaging.[43]
In patients with active osteomyelitis, gallium scanning may reveal abnormal isotope accumulation in affected areas. This is in contrast to the decreased or normal activity in affected areas demonstrated with [99mTc]-MDP bone scintigraphy. Gallium accumulation may correlate more closely than technetium uptake with osteomyelitis inflammatory activity.[8][14]
18F-Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography
[18F]-FDG-PET employs the glucose analog [18F]-FDG, which accumulates in leukocytes and facilitates their accumulation at the site of infection. This imaging technique offers rapid results as images are obtained 30 to 60 minutes after tracer injection. Combining PET with CT ([18F]-FDG-PET-CT) provides high-resolution tomographic images and improved anatomical detail by superimposing the two image sets.[44]
The diagnostic utility of [18F]-FDG-PET is well-established for acute and chronic osteomyelitis. [18F]-FDG-PET has shown a high sensitivity and specificity in various studies, with reported values of 84% and 93%, respectively. One of the advantages of [18F]-FDG-PET is its ability to distinguish osteomyelitis from adjacent soft tissue infection due to its high spatial resolution. [45]
[18F]-FDG-PET has demonstrated utility in differentiating Charcot arthropathy from normal joints and osteomyelitis in patients with diabetes. [18F]-FDG-PET is superior to other imaging techniques, such as diffusion-weighted MRI and dynamic contrast-enhanced MRI (DCE-MRI), in distinguishing diabetic foot osteomyelitis from Charcot arthropathy.[46]
[18F]-FDG-PET has proven utility in assessing post-traumatic osteomyelitis, with a retrospective study suggesting high accuracy in diagnosing fracture-related infections. This imaging modality is also beneficial in diagnosing spondylodiscitis.[47]
Overall, [18F]-FDG-PET offers significant clinical benefits in evaluating osteomyelitis and related conditions, providing rapid imaging, accurate diagnosis, and the ability to differentiate between pathologies.[48][8]
Clinical Significance
Osteomyelitis is a condition with significant morbidity that is notoriously difficult to diagnose. However, imaging tools have improved our ability to identify this condition. Adopting a step-by-step diagnostic approach incorporating modern imaging machinery and techniques can facilitate early diagnosis and treatment.
When evaluating patients with suspected osteomyelitis, the initial imaging step is typically plain radiography. Plain radiography identifies bony abnormalities and may help exclude other diagnoses, such as stress fractures or bone tumors. Soft tissue changes, such as blurring of soft tissue planes and muscle swelling, can be early radiographic indicators of osteomyelitis. However, radiographic changes may not be visible until 10 to 14 days after the onset of infection. Further imaging is warranted if clinical suspicion of osteomyelitis remains high despite normal-appearing radiographs.[14]
MRI and bone scintigraphy are most valuable in clinical scenarios where osteomyelitis is suspected but not clearly demonstrated on plain radiographs. Bone scintigraphy using radiolabeled tracers can assist in detecting areas of increased bone turnover and inflammation and helps identify multifocal or diffuse osteomyelitis. Although bone scintigraphy can guide the selection of appropriate biopsy sites, it may not provide precise enough localizing information regarding the abnormality. Therefore, bone scintigraphy is more commonly used for screening purposes.[8]
MRI is highly sensitive and specific in detecting early bone, muscle, and other soft tissue involvement. MRI can reveal significant findings such as bone marrow edema, joint effusion, periosteal reaction, and abscesses. MRI provides detailed visualization of the spinal cord and surrounding soft tissues in cases of suspected vertebral osteomyelitis.[8] When MRI is unavailable or contraindicated, imaging with CT and US may be useful.
CT assesses for bony destruction, cortical continuity, and the presence of sequestra or gas. CT images are especially beneficial in evaluating chronic osteomyelitis or assessing complications such as abscess formation or sinus tracts.[8] US can be useful for evaluating soft tissue changes associated with osteomyelitis, such as abscess formation or cellulitis. US may help identify and assess fluid collections and guide aspirations or drainage procedures. US is of particular use in neonates before complete bone ossification.[24]
Interpreting radiological findings is crucial in the management of osteomyelitis. Key findings, including periosteal reaction, abscesses, or cloacae, can guide treatment decisions, such as the need for surgical intervention or targeted antibiotic therapy. Close collaboration between the ordering practitioner and radiologist is essential to ensure optimal patient care based on the imaging results. By following the appropriate imaging algorithm and understanding the significance of radiological findings, clinicians can make informed decisions and provide timely and effective management for patients with osteomyelitis.[8]
Media
(Click Image to Enlarge)

Three-phase Bone Scintigraphy: Flow Phase. This flow phase image from a 3-phase bone scan using [99mTc]-MDP reveals diffusely increased activity in the mid and distal foot. Contributed by D Dobaria, MD
(Click Image to Enlarge)
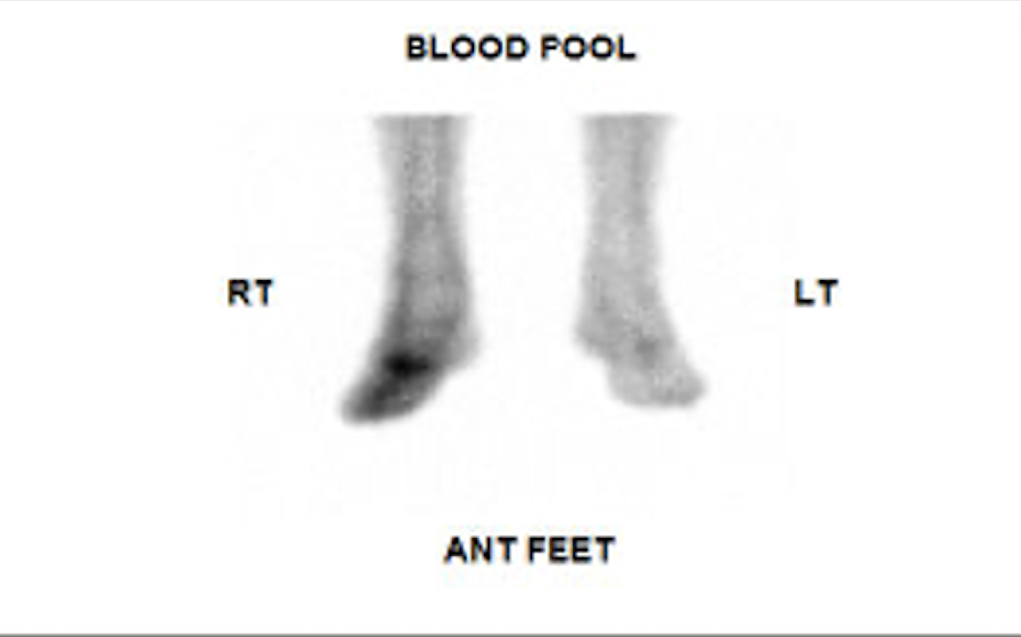
Three-phase Bone Scintigraphy: Blood Pool Phase. This blood pool phase image from a 3-phase bone scan using [99mTc]-MDP reveals increased activity involving the midfoot in the expected region of the 1st and 2nd metatarsals suggesting acute osteomyelitis. Contributed by D Dobaria, MD
(Click Image to Enlarge)
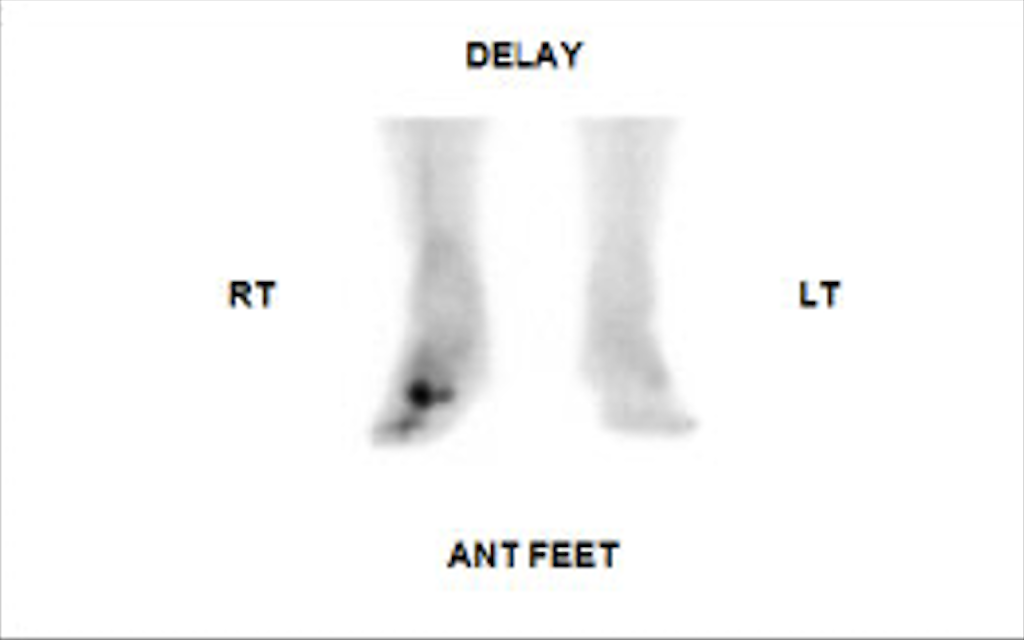
Three-phase Bone Scintigraphy: Bone Phase. This bone or delay phase image from a 3-phase bone scan using [99mTc]-MDP reveals increased activity involving the midfoot in the expected region of the 1st and 2nd metatarsals suggesting acute osteomyelitis. Contributed by D Dobaria, MD
(Click Image to Enlarge)
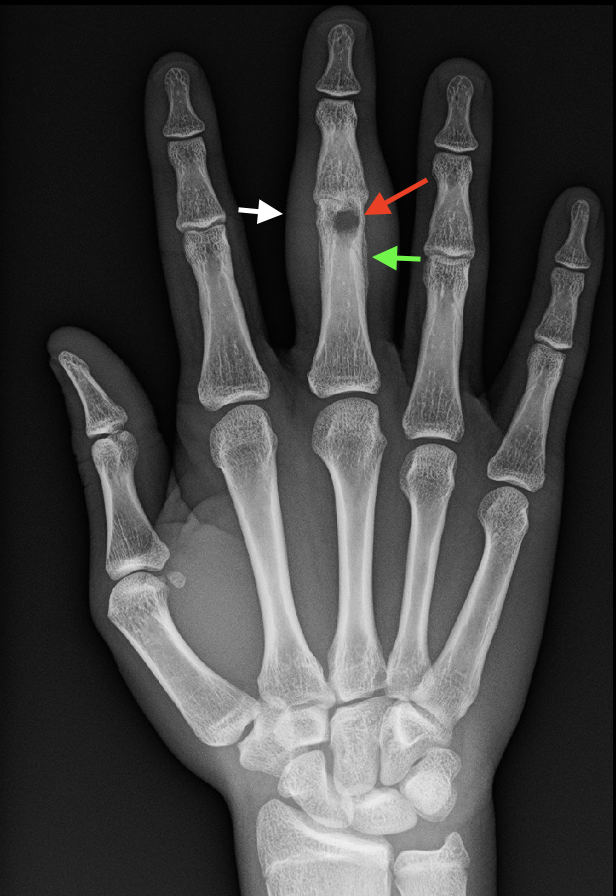
Acute Osteomyelitis, Plain Radiograph. This radiograph of the right hand of a patient with acute osteomyelitis in the third digit reveals soft tissue swelling (white arrow), periosteal reaction (green arrow), and a lytic lesion at the distal portion of the 3rd proximal phalanx (red arrow). These findings indicate inflammation, bone response, and bone destruction due to the infection. Contributed by D Dobaria, MD
(Click Image to Enlarge)

Chronic Osteomyelitis, Computed Tomography. This sagittal CT image with bone windows of a patient with chronic osteomyelitis depicts a sequestrum, a distinct sclerotic bone fragment, within the posterior proximal tibial metadiaphysis. The sequestrum is surrounded by an involucrum characterized by cortical thickening. Contributed by D Dobaria, MD
References
Lew DP, Waldvogel FA. Osteomyelitis. Lancet (London, England). 2004 Jul 24-30:364(9431):369-79 [PubMed PMID: 15276398]
Schmitt SK. Osteomyelitis. Infectious disease clinics of North America. 2017 Jun:31(2):325-338. doi: 10.1016/j.idc.2017.01.010. Epub [PubMed PMID: 28483044]
Salik M, Mir MH, Philip D, Verma S. Brodie's Abscess: A Diagnostic Conundrum. Cureus. 2021 Jul:13(7):e16426. doi: 10.7759/cureus.16426. Epub 2021 Jul 16 [PubMed PMID: 34422465]
Panteli M, Giannoudis PV. Chronic osteomyelitis: what the surgeon needs to know. EFORT open reviews. 2016 May:1(5):128-135. doi: 10.1302/2058-5241.1.000017. Epub 2017 Mar 13 [PubMed PMID: 28461939]
Hofmann SR, Kapplusch F, Girschick HJ, Morbach H, Pablik J, Ferguson PJ, Hedrich CM. Chronic Recurrent Multifocal Osteomyelitis (CRMO): Presentation, Pathogenesis, and Treatment. Current osteoporosis reports. 2017 Dec:15(6):542-554. doi: 10.1007/s11914-017-0405-9. Epub [PubMed PMID: 29080202]
Rukavina I. SAPHO syndrome: a review. Journal of children's orthopaedics. 2015 Feb:9(1):19-27. doi: 10.1007/s11832-014-0627-7. Epub 2015 Jan 14 [PubMed PMID: 25585872]
Khanna G, Sato TS, Ferguson P. Imaging of chronic recurrent multifocal osteomyelitis. Radiographics : a review publication of the Radiological Society of North America, Inc. 2009 Jul-Aug:29(4):1159-77. doi: 10.1148/rg.294085244. Epub [PubMed PMID: 19605663]
Lee YJ, Sadigh S, Mankad K, Kapse N, Rajeswaran G. The imaging of osteomyelitis. Quantitative imaging in medicine and surgery. 2016 Apr:6(2):184-98. doi: 10.21037/qims.2016.04.01. Epub [PubMed PMID: 27190771]
Clarke B. Normal bone anatomy and physiology. Clinical journal of the American Society of Nephrology : CJASN. 2008 Nov:3 Suppl 3(Suppl 3):S131-9. doi: 10.2215/CJN.04151206. Epub [PubMed PMID: 18988698]
Calhoun JH, Manring MM, Shirtliff M. Osteomyelitis of the long bones. Seminars in plastic surgery. 2009 May:23(2):59-72. doi: 10.1055/s-0029-1214158. Epub [PubMed PMID: 20567728]
Momodu II, Savaliya V. Osteomyelitis. StatPearls. 2023 Jan:(): [PubMed PMID: 30335283]
Nahian A, Chauhan PR. Histology, Periosteum And Endosteum. StatPearls. 2023 Jan:(): [PubMed PMID: 32491516]
Hofstee MI, Muthukrishnan G, Atkins GJ, Riool M, Thompson K, Morgenstern M, Stoddart MJ, Richards RG, Zaat SAJ, Moriarty TF. Current Concepts of Osteomyelitis: From Pathologic Mechanisms to Advanced Research Methods. The American journal of pathology. 2020 Jun:190(6):1151-1163. doi: 10.1016/j.ajpath.2020.02.007. Epub 2020 Mar 16 [PubMed PMID: 32194053]
Pineda C, Espinosa R, Pena A. Radiographic imaging in osteomyelitis: the role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Seminars in plastic surgery. 2009 May:23(2):80-9. doi: 10.1055/s-0029-1214160. Epub [PubMed PMID: 20567730]
Pineda C, Vargas A, Rodríguez AV. Imaging of osteomyelitis: current concepts. Infectious disease clinics of North America. 2006 Dec:20(4):789-825 [PubMed PMID: 17118291]
Desimpel J, Posadzy M, Vanhoenacker F. The Many Faces of Osteomyelitis: A Pictorial Review. Journal of the Belgian Society of Radiology. 2017 May 11:101(1):24. doi: 10.5334/jbr-btr.1300. Epub 2017 May 11 [PubMed PMID: 30039016]
van Schuppen J, van Doorn MM, van Rijn RR. Childhood osteomyelitis: imaging characteristics. Insights into imaging. 2012 Oct:3(5):519-33. doi: 10.1007/s13244-012-0186-8. Epub 2012 Aug 10 [PubMed PMID: 22875760]
Weaver JS, Omar IM, Mar WA, Klauser AS, Winegar BA, Mlady GW, McCurdy WE, Taljanovic MS. Magnetic resonance imaging of musculoskeletal infections. Polish journal of radiology. 2022:87():e141-e162. doi: 10.5114/pjr.2022.113825. Epub 2022 Mar 5 [PubMed PMID: 35505859]
Pugmire BS, Shailam R, Gee MS. Role of MRI in the diagnosis and treatment of osteomyelitis in pediatric patients. World journal of radiology. 2014 Aug 28:6(8):530-7. doi: 10.4329/wjr.v6.i8.530. Epub [PubMed PMID: 25170391]
Donovan A, Schweitzer ME. Use of MR imaging in diagnosing diabetes-related pedal osteomyelitis. Radiographics : a review publication of the Radiological Society of North America, Inc. 2010 May:30(3):723-36. doi: 10.1148/rg.303095111. Epub [PubMed PMID: 20462990]
Collins MS, Schaar MM, Wenger DE, Mandrekar JN. T1-weighted MRI characteristics of pedal osteomyelitis. AJR. American journal of roentgenology. 2005 Aug:185(2):386-93 [PubMed PMID: 16037509]
Bakhru RN, Schweickert WD. Intensive care ultrasound: I. Physics, equipment, and image quality. Annals of the American Thoracic Society. 2013 Oct:10(5):540-8. doi: 10.1513/AnnalsATS.201306-191OT. Epub [PubMed PMID: 24161064]
Level 2 (mid-level) evidenceCocco G, Ricci V, Villani M, Delli Pizzi A, Izzi J, Mastandrea M, Boccatonda A, Naňka O, Corvino A, Caulo M, Vecchiet J. Ultrasound imaging of bone fractures. Insights into imaging. 2022 Dec 13:13(1):189. doi: 10.1186/s13244-022-01335-z. Epub 2022 Dec 13 [PubMed PMID: 36512142]
Jaramillo D. Infection: musculoskeletal. Pediatric radiology. 2011 May:41 Suppl 1():S127-34. doi: 10.1007/s00247-011-2001-y. Epub 2011 Apr 27 [PubMed PMID: 21523583]
Cardinal E, Bureau NJ, Aubin B, Chhem RK. Role of ultrasound in musculoskeletal infections. Radiologic clinics of North America. 2001 Mar:39(2):191-201 [PubMed PMID: 11316354]
Jaramillo D, Dormans JP, Delgado J, Laor T, St Geme JW 3rd. Hematogenous Osteomyelitis in Infants and Children: Imaging of a Changing Disease. Radiology. 2017 Jun:283(3):629-643. doi: 10.1148/radiol.2017151929. Epub [PubMed PMID: 28514223]
Paliwal AK, Sahdev R, Deshwal A, Ram B. Role of ultrasound in the diagnosis of paediatric acute osteomyelitis. Journal of ultrasonography. 2021:21(84):34-40. doi: 10.15557/JoU.2021.0005. Epub 2021 Mar 8 [PubMed PMID: 33791114]
Duszynski DO, Kuhn JP, Afshani E, Riddlesberger MM Jr. Early radionuclide diagnosis of acute osteomyelitis. Radiology. 1975 Nov:117(2):337-40 [PubMed PMID: 1178861]
Level 3 (low-level) evidenceGilday DL, Paul DJ, Paterson J. Diagnosis of osteomyelitis in children by combined blood pool and bone imaging. Radiology. 1975 Nov:117(2):331-5 [PubMed PMID: 1178860]
Deysine M, Rafkin H, Teicher I, Silver L, Robinson R, Manly J, Aufses AH Jr. Diagnosis of chronic and postoperative osteomyelitis with gallium 67 citrate scans. American journal of surgery. 1975 Jun:129(6):632-5 [PubMed PMID: 1130608]
Level 3 (low-level) evidenceGholamrezanezhad A, Basques K, Batouli A, Matcuk G, Alavi A, Jadvar H. Clinical Nononcologic Applications of PET/CT and PET/MRI in Musculoskeletal, Orthopedic, and Rheumatologic Imaging. AJR. American journal of roentgenology. 2018 Jun:210(6):W245-W263. doi: 10.2214/AJR.17.18523. Epub [PubMed PMID: 29787313]
Jødal L, Afzelius P, Alstrup AKO, Jensen SB. Radiotracers for Bone Marrow Infection Imaging. Molecules (Basel, Switzerland). 2021 May 25:26(11):. doi: 10.3390/molecules26113159. Epub 2021 May 25 [PubMed PMID: 34070537]
Gross T, Kaim AH, Regazzoni P, Widmer AF. Current concepts in posttraumatic osteomyelitis: a diagnostic challenge with new imaging options. The Journal of trauma. 2002 Jun:52(6):1210-9 [PubMed PMID: 12045656]
Level 3 (low-level) evidenceAl-Sheikh W, Sfakianakis GN, Mnaymneh W, Hourani M, Heal A, Duncan RC, Burnett A, Ashkar FS, Serafini AN. Subacute and chronic bone infections: diagnosis using In-111, Ga-67 and Tc-99m MDP bone scintigraphy, and radiography. Radiology. 1985 May:155(2):501-6 [PubMed PMID: 3157204]
Kaim A, Maurer T, Ochsner P, Jundt G, Kirsch E, Mueller-Brand J. Chronic complicated osteomyelitis of the appendicular skeleton: diagnosis with technetium-99m labelled monoclonal antigranulocyte antibody-immunoscintigraphy. European journal of nuclear medicine. 1997 Jul:24(7):732-8 [PubMed PMID: 9211758]
Kolindou A, Liu Y, Ozker K, Krasnow AZ, Isitman AT, Hellman RS, Collier BD. In-111 WBC imaging of osteomyelitis in patients with underlying bone scan abnormalities. Clinical nuclear medicine. 1996 Mar:21(3):183-91 [PubMed PMID: 8846561]
Level 2 (mid-level) evidenceSchauwecker DS. The scintigraphic diagnosis of osteomyelitis. AJR. American journal of roentgenology. 1992 Jan:158(1):9-18 [PubMed PMID: 1727365]
Schauwecker DS. Osteomyelitis: diagnosis with In-111-labeled leukocytes. Radiology. 1989 Apr:171(1):141-6 [PubMed PMID: 2928518]
Level 2 (mid-level) evidenceAdams C, Banks KP. Bone Scan. StatPearls. 2023 Jan:(): [PubMed PMID: 30285381]
Dinh T, McWhorter N. Triple Phase Bone Scan. StatPearls. 2023 Jan:(): [PubMed PMID: 30571011]
Palestro CJ. Radionuclide Imaging of Musculoskeletal Infection: A Review. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2016 Sep:57(9):1406-12. doi: 10.2967/jnumed.115.157297. Epub 2016 Jul 7 [PubMed PMID: 27390160]
Dittrich RP, De Jesus O. Gallium Scan. StatPearls. 2024 Jan:(): [PubMed PMID: 33620825]
Bailey DL, Sabanathan D, Aslani A, Campbell DH, Walsh BJ, Lengkeek NA. RetroSPECT: Gallium-67 as a Long-Lived Imaging Agent for Theranostics. Asia Oceania journal of nuclear medicine & biology. 2021 Winter:9(1):1-8. doi: 10.22038/AOJNMB.2020.51714.1355. Epub [PubMed PMID: 33392343]
Ashraf MA, Goyal A. Fludeoxyglucose (18F). StatPearls. 2024 Jan:(): [PubMed PMID: 32491585]
Kung BT, Seraj SM, Zadeh MZ, Rojulpote C, Kothekar E, Ayubcha C, Ng KS, Ng KK, Au-Yong TK, Werner TJ, Zhuang H, Hunt SJ, Hess S, Alavi A. An update on the role of (18)F-FDG-PET/CT in major infectious and inflammatory diseases. American journal of nuclear medicine and molecular imaging. 2019:9(6):255-273 [PubMed PMID: 31976156]
Basu S, Chryssikos T, Houseni M, Scot Malay D, Shah J, Zhuang H, Alavi A. Potential role of FDG PET in the setting of diabetic neuro-osteoarthropathy: can it differentiate uncomplicated Charcot's neuroarthropathy from osteomyelitis and soft-tissue infection? Nuclear medicine communications. 2007 Jun:28(6):465-72 [PubMed PMID: 17460537]
Treglia G. Diagnostic Performance of (18)F-FDG PET/CT in Infectious and Inflammatory Diseases according to Published Meta-Analyses. Contrast media & molecular imaging. 2019:2019():3018349. doi: 10.1155/2019/3018349. Epub 2019 Jul 25 [PubMed PMID: 31427907]
Palestro CJ. FDG-PET in musculoskeletal infections. Seminars in nuclear medicine. 2013 Sep:43(5):367-76. doi: 10.1053/j.semnuclmed.2013.04.006. Epub [PubMed PMID: 23905618]