Introduction
Therapeutic keratoplasty (TPK) is a surgical technique where a disease-host corneal tissue is replaced with a healthy donor cornea. A corneal graft is placed after terminating the infectious foci and improving the anatomical integrity of the cornea.[1] TPK is indicated in non-resolving infectious keratitis cases where the patient fails to respond or improve with conventional medical therapy. Hence, therapeutic keratoplasty is indicated when the corneal ulcer progresses despite maximal medical therapy for two weeks or when the integrity of the globe is compromised.[2]
Tectonic keratoplasty is performed in corneal perforation or corneal melt cases where the anterior chamber has collapsed, and aqueous humor has leaked.[3] TPK helps eliminate the infectious and exudates from the anterior chamber, reduces inflammation, reduces the microbial load, relieves pain, and saves the eye from multiple complications such as scleritis, scleral abscess, endophthalmitis, panophthalmitis, and secondary glaucoma. Visual rehabilitation is a secondary goal after TPK.[4]
In developing countries, there is a high load of non-healing microbial keratitis and perforated corneal ulcers, and TPK is commonly performed. TPK helps in cases of glue with bandage contact lens, tenoplasty, conjunctival Gundersen flap fails, or when the perforation is large.[5]
In the Singapore Corneal Transplant study, 13% of corneal transplants were therapeutic or tectonic, and in another study from Brazil, approximately 18% of corneal transplants were for corneal ulceration and perforation.[6] The medical management, graft survival rate, postoperative course, follow-up, and rehabilitation in TPK differ from that of conventional optical keratoplasty, as the surgery is done on an inflamed and infected eye.[7]
In TPK, anterior chamber exudates are removed after trephining the host disease cornea, angles are washed with normal saline, a peripheral surgical iridectomy is made, retro-iris exudates are washed, and retro-iris exudates are washed. Lens removal can also be performed based on the indication.[8] The goal should be to leave the posterior capsule intact to prevent transmission of infection from the anterior to the posterior chamber. Then the donor corneal button or graft is sutured to the host with 16 10-0 nylon sutures.
Additional sutures can be secured if there is an anterior chamber leak. The patient is started on antimicrobial therapy based on the pre-operative diagnosis, and topical steroids are initiated after a brief quiescence if there are no infectious foci or graft infections. The aim is to prevent complications of TPK and salvage the globe anatomically and functionally.[9]
Types of Therapeutic Keratoplasty
- Full-thickness therapeutic keratoplasty
Here the full-thickness corneal graft is placed over the host cornea after removing the diseased portion of the cornea with the primary aim of eliminating the infection.[10]
- Tectonic keratoplasty
Here the full-thickness corneal graft is placed over the host cornea to restore the tectonic integrity of the cornea.[11]
- Patch graft
Patch graft can be full thickness as well as lamellar patch graft depending on the extent of involvement of the corneal tissue.[12]
- Therapeutic deep anterior lamellar keratoplasty
In therapeutic DALK, the diseased corneal portion is usually the anterior stromal tissue; hence the deep anterior lamella is removed and replaced with a partial thickness graft.[13]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomy
The corneal tissue is composed of cellular and acellular components. The cellular components comprise epithelial cells, keratocytes, and endothelial cells. The acellular component is composed of collagenous protein and glycosaminoglycans.[14] The epithelial cells originate from the epidermal ectoderm, and the keratocyte and endothelial cells are derived from the neural crest. The cornea comprises five layers epithelium, bowman's, stroma, Descemet, and endothelium.[15]
Recently sixth layer has also been defined as Dua's layer, which is also labeled as the pre-descematic layer. In anterior lamellar keratoplasty, the area of focus is the anterior stroma, and in cases with posterior lamellar keratoplasty, the area of focus is Descemet and endothelium. Penetrating keratoplasty is a technique where the full thickness of the host cornea is trephine and replaced by a full-thickness donor button. All the cornea layers are transplanted. In cases with lamellar patch graft, the corneal tissue up to the anterior stroma is dissected, and the partial thickness donor button is sutured to the host rim.[16]
Physiology
Ocular Immune Privilege
Active
There is an increased expression of inhibitory cell surface molecules- FAS ligands, decay accelerating factor, CD46, and CD59. The presence of an immunosuppressive microenvironment also leads to the expression of transforming growth beta (TGF-B), Alpha melanocytic stimulating hormone (a- MSH), Vasoactive intestinal peptide (VIP), calcitonin gene-related peptide (CGRP), migration inhibitory factor (MIF) and free cortisol.[17]
Passive
Passive immunity contributes to the blood tissue barrier, deficient efferent lymphatics, and reduced MHC complex I and II expression.[18]
Indications
Infectious Keratitis
Fungal Keratitis
- Not improving (refractory) after maximal medical therapy; usually, the window period is 2 weeks. However, early keratoplasty is usually indicated in specific scenarios after 7 to 10 days.
- Corneal perforation
- Scleral involvement[19]
- Rapid corneal melt
- Non-compliance with medications or failed medical therapy
- Descemetocele[20]
Bacterial Keratitis
- Not improving (refractory) after maximal medical therapy; usually, the window period is 2 weeks. However, in specific scenarios, such as pseudomonas keratitis, early keratoplasty is indicated usually after 7-10 days.[21]
- Descemetocele
- Corneal perforation
- Limbus to limbus corneal involvement
- Corneoscleral abscess
- Non-compliance to medications
- Resistant to conventional therapy
- Mycobacterial keratitis
- Infectious crystalline keratopathy
Pythium Keratitis
- Descemetocele[22]
- Corneal perforation
- Early limbal spread
- Peripheral guttering
- Corneal melt[23]
- Not improving (refractory) after maximal medical therapy. The widow period is usually less than 7 to 10 days.[24]
- Graft reinfection[25]
- Nonresolving endoexudates[26]
Acanthamoeba Keratitis
- Descemetocele
- Corneal perforation
- Severe scleral involvement
- Non-resolving keratitis with maximal medical therapy[27]
Viral Keratitis
- Herpes simplex keratitis
- Herpes zoster keratitis
- Secondary bacterial infiltrate with corneal melt
- Corneal perforation[28]
Others
Equipment
- Side port 15-degree blade or MVR blade
- Screw speculum
- Corneoscleral fixation- Flieringa ring
- Ophthalmic Viscosurgical Device
- Normal saline or balanced salt solution
- Conjunctival forceps
- Conjunctival scissors
- Vannas scissors
- Trephine
- Lim's forceps
- Rhexis forceps
- 26 G needle cystitome
- Bimanual irrigation and aspiration Simcoe cannula
- Graft punch
- Cornisol solution
- Topical betadine
- Injection moxifloxacin
- Injection voriconazole
- Automated anterior vitrectomy
- Suture holding forceps
- McPherson forceps
- Suture-tying plane forceps
- 10-0 nylon monofilament suture
- 9-0 nylon monofilament suture
- Cotton bud
- Cotton swab
- Fluorescein dye
Personnel
The ophthalmic surgeon performs the preoperative medical management, surgical planning, keratoplasty, and postoperative management of these patients—the nursing staff in the outpatient department. The nursing staff in the operation theatre, counselor, and pharmacist play crucial roles in patient management.[31]
Preparation
Preoperative patient preparation is extremely critical while planning and attempting keratoplasty.
Ocular Examination
Torch Light Examination
Detailed torch light and slit lamp evaluation are mandatory in each case. Torchlight examination helps grossly assess ocular motility, the presence of any strabismus, and adnexal pathology.[32]
Anterior Segment Assessment
A detailed anterior segment examination is mandatory to assess the extent and depth of infiltrate, extent of corneal involvement, limbal involvement, anterior chamber depth, presence and absence of exudates, iris, pupil, and lens status if visible.[33] The corneal involvement should be documented photographically with dimensions of the corneal infiltrate, which help plan the trephination size intraoperatively. The corneal should be examined meticulously to assess any site of corneal perforation and iris prolapse. In doubtful cases, Seidel's test with topical fluorescein can also be performed on the slit lamp.[34] The anterior segment should also be assessed for anterior chamber inflammation, cells, flare, and exudates. It is also essential to rule out secondary glaucoma, scleral abscess, scleritis, endophthalmitis, and dry eyes.
Posterior Segment Assessment
Usually, the posterior segment assessment is masked by the corneal infiltrate, but a dilated fundus assessment can still be attempted.[35] Regarding B scan evaluation, there are two schools of thought. One is A and B scan should be done to rule out endophthalmitis when the fundus is not visualized in these cases.
Another school of thought is that B scan should be avoided preoperatively to avoid cross-transmission of infection and instruments becoming unsterilized. Postoperatively when the patient has undergone TPK, the retina will be better visualized, and a B scan can be attempted to assess the status of the retina. If retinal intervention is needed can be done as a staged procedure post-TPK. Endophthalmitis risk is higher in long-standing chronic infection, aphakia, and corneal perforation patients who have undergone cataract extraction previously.[36]
Preoperative Antimicrobial Therapy
All patients should be treated with preoperatively topical and systemic antimicrobial therapy in required cases. Targeted antimicrobial therapy is warranted when the etiology is known to reduce the virulence of microorganisms and the microbial load.[37]
Broad-spectrum antimicrobial therapy should be given in cases where etiology is doubtful and not labeled. Donnenfeld et al. proposed that topical ofloxacin (0.3%) should be used hourly for patients prepared for TPK to prevent the risk of secondary bacterial infection irrespective of the etiology. They also proposed that a tablet of ofloxacin 400 mg should be used 12 hours before admission, and intravenous vancomycin and tobramycin should be given after admission. As per significant studies, topical steroids should be avoided because it worsens the infectious process.[38]
In contrast, one of the studies recommended the use of topical and systemic steroids in cases with fungal keratitis. Besides antibiotics, antifungals such as natamycin, Itraconazole, and voriconazole are used in patients with established fungal etiology. The other adjuvant drugs needed are topical timolol and homatropine.[39]
Corneal Scraping
Gentle corneal scraping should be done in all cases when the patient first presents to the clinical outpatient setting. This helps in knowing the etiology and prescribing targeted antimicrobial therapy. Smear and culture analysis should be performed wherever possible. The culture report can be assessed after 48 to 72 hours. Preoperative culture reports give an idea regarding postoperative antimicrobial regimen and deciding on when to start steroids.[40]
Preoperative Intravenous Mannitol
Preoperative intravenous mannitol 50-100 ml should be given as a routine in all cases undergoing TPK to decompress the vitreous and reduce positive vitreous thrust while performing surgery.[41] The contraindications for intravenous mannitol, such as anuria, kidney disease, pulmonary congestion, pulmonary congestion, severe dehydration, active intracranial bleeding, progressive heart failure, and mannitol hypersensitivity, should be ruled out before injecting the drug. In cases where mannitol injection is not possible, oral glycerol of 20 to 30 ml can be given to the patient.[42]
Technique or Treatment
TPK is one of the most difficult ophthalmic surgeries as surgery is performed in an inflamed and open globe. TPK should be attempted by an experienced surgeon with good exposure to performing keratoplasties.[43] The surgery is usually performed with local anesthesia; general anesthesia is also required in selective cases. If the block is inadequate, it invites intraoperative complications. Depolarizing agents should be avoided as they can increase intraocular pressure in an open globe.[44]
Before the surgery, the donor tissue should be available, and the count and storage condition should be checked. The tissue is made available from the eye bank. The corneoscleral rim from the donor's eye should be stored in 4 C McCarey-Kaufman, Cornisol, or chondroitin sulfate-containing media having gentamicin.[45]
The criteria for TPK storage are not as strict as for a graft with optical penetrating keratoplasty quality. In case of tissue shortage, the cryopreserved or glycerin-preserved cornea and sclera have been suggested. A good quality donor tissue in TPK also helps in visual rehabilitation in TPK. The integrity of healthy corneal tissue has inherent advantages, such as the epithelium remaining intact and the risk of infection is minimized. A clear graft also helps to assess the anterior chamber reaction during the postoperative period.[46]
Lid Speculum or Sutures
A good self-retaining speculum of the lid or lid sutures helps prevent pressure on the globe.[47]
Scleral Fixation Ring
Scleral fixation rings like the Flieringa ring provide structural support and make the surgery easier. Killingsworth suggested that the scleral fixation ring should be avoided as it makes suturing difficult when the globe is hypotonus. The use Flieringa ring is variable and varies from surgeon to surgeon and center to center.[48]
Conjunctival Peritomy
In cases with large or eccentric grafts, conjunctival peritomy is recommended to avoid passing the suture through the conjunctiva. In my cases, practitioners rarely attempt a peritomy because if taken care of and the needle direction is kept right, the suture passes through the sclera. Peritomy becomes mandatory in cases with the scleral extension of the infectious foci to avoid cheeses wiring of the scleral tissue. Cautery can be done in cases where there is excess bleeding.[49]
Paracentesis
A small initial paracentesis in the accessible area is recommended. It has a few advantages. First, it reduces the intraocular pressure in cases with secondary glaucoma, second anterior chamber exudates can be drained through the paracentesis, and third viscoelastic can be put which helps push the iris lens diaphragm backward and helps in good trephination, which prevents injury to the iris.[50]
Host Trephination
Before trephination, the size of the infiltrate is measured with the help of calipers, and subsequently, the infiltrate with a 0.5 mm free margin of the cornea is marked with the use of ink. A central dot over the central portion of the cornea, followed by eight subsequent markings, is done in the peripheral cornea. Next, the sharp edge of the trephine is ink marked, and after aligning the trephine with the markings over the cornea, the recipient bed is trephined partial thickness.[51]
Care should be taken to avoid excess pressure over the recipient bed as it can damage the iris lens diaphragm and may lead to the extrusion of intraocular contents.[52] Trephination becomes problematic in cases with more extensive perforation as it is hypotony due to zero IOP, and pressure cannot be applied with the trephine over the recipient bed. In such scenarios, free hand dissection is attempted, or vacuum trephine is used. One of the previous studies suggested that in cases with central and peripheral larger corneal perforations, Hessberg Baron and Hanna suction trephines are easier to use than Franceschetti-type free blade trephines.[53]
The advantage of suction trephines is that lower incidence of shallowing of the anterior chamber and iris prolapse compared to free blade trephines. Suction trephines help to provide peripheral support and counter traction with the advancing blade, whereas the free blade trephines depend totally on the stability of the cornea, which is minimal in cases with perforation. As per the literature, the Hanna trephine is comparatively easier to use than the Hessberg Baron trephine as it provides a wide ring of peripheral suction, resulting in less central corneal distortion and holding the cornea in a more natural configuration. The trephines can be disposable as well as reusable. The disposable ones are readily available. Rao et al. suggested using cyanoacrylate glue or a patch graft in perforated eyes. They also suggested freehand dissection in cases with extensive perforation or entire corneal involvement.[54]
Graft Size
Graft size depends on the size of the infiltrate. Usually, the donor corneal button size is kept 0.5-1mm larger than the recipient trephined bed. Small grafts, eccentric grafts, and patch grafts have inherent disadvantages, such as sutures obscuring the visual axis and causing crowding of the anterior segment. Large grafts are more prone to graft rejection, failure, and post-keratoplasty glaucoma (peripheral anterior synechiae formation and synechial angle closure).
The size of the trephine usually varies from 7.00 mm to 12.00 mm. The important goal is removing the diseased host rim even if the graft size is larger. After trephination, the recipient should be divided into two parts and sent for microbiological and histopathological analysis. The material can be inoculated in blood agar, chocolate agar Sabouraud's dextrose agar, brain heart infusion broth, and non-nutrient agar with E.coli.[44]
Anterior Chamber Entry and Management
After marking the recipient bed with a trephine, anterior chamber entry is done with the help of a side port blade; subsequently, a 360-degree host cornea is excised. Once the diseased corneal portion is removed, the anterior chamber exudates, and purulent and fibrous membranes are removed with the help of forceps or can also be irrigated slowly. The iris is cleared of membranes, and occasionally the iris can bleed. Efforts should be made to minimize bleeding from the iris surface. Various authors have suggested using intracameral antifungals and antibiotics to irrigate the iris surface and reduce the infective foci.[55]
Peripheral Iridectomy
This is followed by peripheral iridectomy. Some authors perform one; some perform two iridectomies to prevent pupillary block glaucoma postoperatively. Care should be taken to avoid damage to the anterior lens capsule and the lens. There can be torrential bleeding sometimes after performing an iridectomy. The bleed can be controlled with gentle irrigation or minimal adrenaline.[8]
Lens Management
The recommendation is to preserve the lens in most cases as it acts as a barrier against migration of infection to the posterior segment and vitreous. Donnenfeld recommended 2% pilocarpine over the iris surface in phakic and pseudophakic patients to preserve the iris lens diaphragm and prevent spontaneous lens expulsion.[1]
The following case scenarios are based on the author's recommendations for lens management.
- In an elderly patient with a hard cataract and no retro iris exudates, lens removal can be attempted, and the posterior capsule should be preserved. This helps push the iris lens diaphragm backward, opens up the angle, and helps prevent synechial angle closure glaucoma postoperatively.
- In another case scenario, if there are retroiris exudates and the lens is cataract, lens removal should be performed to prevent the recurrence of infection, and it also helps in anterior chamber formation.[56]
- In cases with lens abscess, the lens should be removed.
- In pseudophakic patients with endophthalmitis, the IOL should be explanted. The lens should be preserved in patients younger than 50 with early cataracts and no retroiris exudates.[57] The lens acts as a barrier, and the accommodation and visual function is retained.[58]
Open Sky Vitrectomy
Automated anterior vitrectomy is recommended in cases with spontaneous lens expulsion and posterior capsular breach to remove the prolapsed vitreous. Intravitreal antimicrobials should be injected in these cases. The vitrectomy should be prompt and meticulous to prevent the risk of expulsive choroidal hemorrhage. A vitreous tap is also recommended in these cases for culture and sensitivity. If the microorganisms are unknown, intravitreal injection of vancomycin (1 mg in 0.1 mL) and ceftazidime (2.5 mg in 0.1 mL) should be given in aphakic patients and patients complicated by lens expulsion.[59]
Donor Button Preparation
Here again, there are two schools of thought. The question is whether to perform donor button excision before the host trephination or after host trephination.[60] Some surgeons perform donor button excision before trephination to prevent the risk of expulsive choroidal hemorrhage, as vitreous prolapse can occur, and the surgeon may not get adequate time to perform an anterior vitrectomy. Some believe that the excision of the donor button should always be performed after the host trephination as necrosed wound architecture may require additional trimming and may change the size of the graft. The donor button is punched endothelial side up and is kept 0.5 to 1 mm more than the host trephination size.[46]
Suturing the Donor Button
The donor button is sutured to the host rim with interrupted 10-0 monofilament nylon sutures. In cases with the cornea to limbal sutures, 9-0 monofilament nylon should be used. In cases of emergency when a particular suture type is unavailable, 10-0 or 9-0 can be used interchangeably.[61]
The suture depth should be 90% on the donor and host sides. The literature review also suggests 75% depth, but most surgeons attempt 90%. Complete thickness sutures should be avoided, as they form a suture tract from where aqueous can lead, and it also acts as a nidus for infection to pass from the cornea to the anterior chamber. Most surgeons prefer a 1:1 ratio of suture bites on the host and donor sides.[9]
However, some prefer larger bites on the host side to prevent cheese wiring of the host tissue through a potentially necrotic zone. All suture knots should be buried on the host side. Additional sutures can be attempted to prevent any subtle leak, and wound closure should be done meticulously. Pressure should be avoided over the globe throughout the surgery. Intracameral moxifloxacin should be given, and anterior chamber formation should be done.[62]
Check for Leakage
Before closing the case, fluorescein dye can be spread over the graft host junction and looked for any leaks. A cotton bud or a swab can also be used to look for leaks. In case of any suspected leakage, additional sutures should be placed.[63]
Pad and Bandage
After completion of the surgery, a pad and bandage are applied, preferably under a topical antibiotic or ointment cover. The pad and bandage can be opened after 4 to 6 hours, and appropriate postoperative drugs should be given.[64]
Postoperative Management
Postoperatively the patient should be started on antimicrobials for a brief initial period. Antibiotics should be started 6 to 8 times daily, along with adjuvant therapy in cases with bacterial keratitis as the etiology. Similarly, in patients with fungal etiology, antifungals should be started. The duration of antimicrobial therapy is governed by the severity of infection, microorganism load and virulence, and the pre-operative and postoperative culture results.[43]
After 3 or 4 weeks, the patient should be started on topical steroids if there are no signs of infection. The concept I follow is if the pre-operative and postoperative culture reports are negative and there are no clinical signs of infections, steroids can be started after two weeks post keratoplasty. If either of the culture reports is positive, it is better to wait three weeks before starting steroids; if both are positive, it is better to wait at least 4 weeks before starting steroids.
Fungal and Acanthamoeba keratitis cases usually require long-term postoperative antimicrobial therapy for several months. Cycloplegics are needed to relieve ciliary spasms, reduced uveitis, pain, pupillary block, posterior synechiae, and PAS formation. Antiglaucoma drugs are required to reduce the raised intraocular pressure in cases with trabeculitis, PAS, and uveitis after TPK.
Topical steroids should be started after a brief interval, as explained above. Topical steroids reduce inflammation and improve visual outcomes. Initiation of steroids should be under antimicrobial cover for approximately two weeks, and later patient can be given steroids alone. Topical steroids can be given from day 1 in viral keratitis cases under antiviral cover. Lubricating eye drops helps in reepithelization. In patients with neuroparalytic keratitis, dry eyes, and recurrent graft infection, lateral tarsorrhaphy with conjunctival flap should be considered.[65]
Postoperative Drug Regimes
Bacterial Keratitis
- Topical moxifloxacin or gatifloxacin or tobramycin, or amikacin 6-8 times per day to reduce the bacterial load (based on the etiology)
- Topical timolol or other adjuvant antiglaucoma medications two times per day. Miotics and prostaglandins should be avoided in an inflamed eye.
- Topical homatropine or atropine two times per day
- Topical lubricating hydroxypropyl methylcellulose or carboxymethylcellulose eye drops to regularize and smoothen the ocular surface. It also promotes re-epithelialization.
- Oral anti-inflammatory drugs such as diclofenac or paracetamol reduce pain and periorbital edema.[21]
Fungal Keratitis
Topical natamycin, voriconazole, or itraconazole 6-8 times daily to reduce the fungal load (based on the etiology). Rest adjuvant drugs remain the same. Oral ketoconazole may be required in cases with scleritis and endophthalmitis.[66]
Acanthamoeba Keratitis
Topical chlorhexidine or poly hexamethylene biguanides or neomycin, along with adjuvant drugs.[67]
Pythium Keratitis
Topical linezolid or azithromycin along with adjuvant drugs. Oral azithromycin may be required in cases with scleritis and endophthalmitis.[20]
Viral Keratitis
Topical antibiotics and steroids, along with adjuvant drugs.[28]
Steroid Regimen
Initially, steroids are started 3 or 4 times for the first seven days under antimicrobial cover as steroid initiation may invite infection. Once there are no signs of infection, I prefer to continue the steroid regimen 4/3/2/1 for 3 months each and later once for lifelong and antiglaucoma coverage. The patient should be regularly followed up to look for any signs of infection and loose suture removal intermittently, if any. All suture removal can be done in 12 months. If the graft in TPK fails after a period of time, then optical penetrating keratoplasty (OPK) can be attempted 12 months postoperatively once suture removal has been done. OPK can also be attempted in one-eyed patients at 6 to 8 months.[68]
Complications
The complications of therapeutic teratoplasty can be listed as follows:
Intraoperative
- Inadequate analgesia
- Inadequate akinesia
- Eccentric host trephination
- Irregular host rim
- Post irregular ledge at the host rim
- Iridodialysis
- Lens expulsion
- Posterior capsular rent
- Vitreous prolapse
- Expulsive choroidal hemorrhage
- Hyphema[44]
Postoperative
Early
- Wound gape
- Loose sutures
- Suture infiltrate
- Shallow or flat anterior chamber
- Anterior chamber leak
- Iris prolapse through graft host junction[69]
- Graft infiltrate
- Epithelial defect
- Anterior uveitis
- Peripheral anterior synechiae
- Secondary glaucoma
Late
- Choroidal effusion
- Peripheral anterior synechiae
- Hypotony
- Choroidal detachment
- Retinal detachment
- Cataract
- Graft failure
- Graft ectasia
- Secondary glaucoma
Secondary Glaucoma
There are various causes for secondary glaucoma
- Retained viscoelastic
- Pupillary block glaucoma
- Synechial angle closure
- Large graft occluding the angle
- Smaller graft with crowded anterior chamber angle
- Steroid-induced glaucoma as a late sequelae
- Malignant glaucoma
Clinical Significance
The clinical significance of TPK lies in eliminating the infection and providing good anatomical and functional outcomes to the patient. TPK is a boon for patients suffering from severe microbial keratitis and changes the quality of life of the patients. It is an essential surgical procedure in the surgeon's armamentarium for patients' ocular rehabilitation, especially in the developing world.
TPK plays a crucial role when globe integrity is compromised, and preoperative and postoperative antimicrobial therapy is crucial in these cases. A large-sized graft is mandatory in cases where the infiltrate size is larger. TPK with a suitable donor graft can restore visual function and may also obviate the need for second-stage optical keratoplasty.[7]
Enhancing Healthcare Team Outcomes
Managing a patient with a corneal ulcer is always a challenge. The decision of when to take the patient for TPK rest with the surgeon is based on his expertise and experience. The good outcome of TPK depends on the combined and coordinated effort of the nursing staff, mid-level ophthalmic personnel, Ophthalmic surgeons, assisting staff in the operating room, optometrist, technicians, pharmacist, and counselor. The surgeon's responsibility is good decision-making, counseling regarding regular use of medications, meticulous surgery, and regular follow-up of patients, which governs the good outcome of TPK.[70]
Nursing, Allied Health, and Interprofessional Team Interventions
The nursing and the allied health staff help take the patient to the operating room, arrange the equipment and instrument trolley, drape the patients, and assist in surgical intervention. They also help in patient examination preoperatively as well as postoperatively. Also, assist in regular monitoring, counseling, and follow-up of these patients. The mid-level ophthalmic personnel helps in patient recruitment, assistance in the outpatient department, corneal scraping, and explaining the procedure and time needed for the scraping results to arrive.[71]
Nursing, Allied Health, and Interprofessional Team Monitoring
The nursing, allied health professionals, and the rest of the interprofessional team help regularly monitor the patients, visual acuity, intraocular pressure, regular follow-up, application of topical drugs, intake of oral medications, and patient's ocular improvement.[72]
Media
(Click Image to Enlarge)
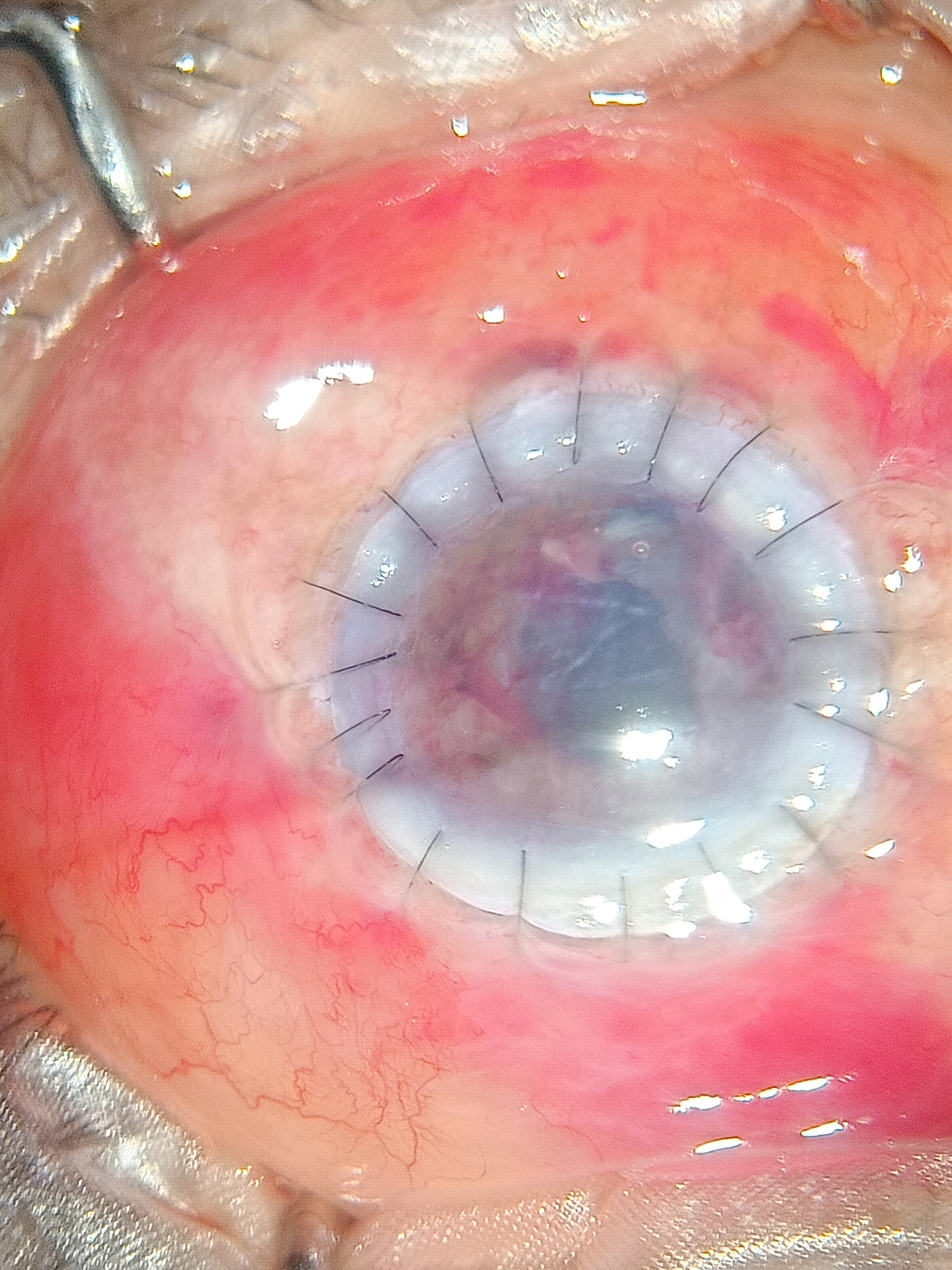
Digital image of the patient post tectonic keratoplasty depicting well opposed graft Contributed by Bharat Gurnani, MD
(Click Image to Enlarge)
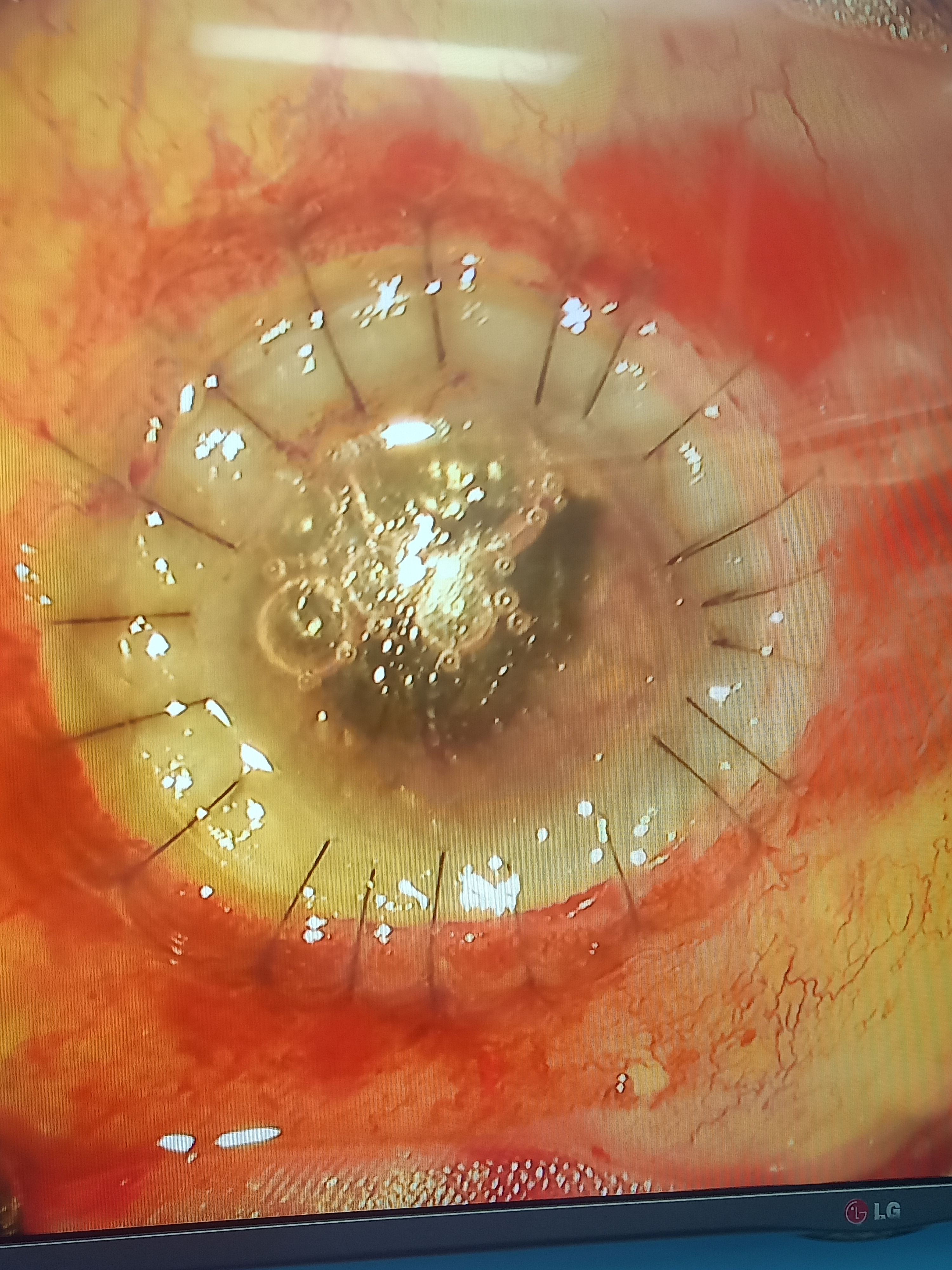
Digital image of the patient depicting well opposed graft in a case of perforate corneal ulcer post therapeutic keratoplasty Contributed by Bharat Gurnani, MD
References
Yao YF, Zhang YM, Zhou P, Zhang B, Qiu WY, Tseng SC. Therapeutic penetrating keratoplasty in severe fungal keratitis using cryopreserved donor corneas. The British journal of ophthalmology. 2003 May:87(5):543-7 [PubMed PMID: 12714387]
Level 2 (mid-level) evidenceSony P, Sharma N, Vajpayee RB, Ray M. Therapeutic keratoplasty for infectious keratitis: a review of the literature. The CLAO journal : official publication of the Contact Lens Association of Ophthalmologists, Inc. 2002 Jul:28(3):111-8 [PubMed PMID: 12144228]
Kato Y, Nagasato D, Nakakura S, Chikama T, Katakami C, Tabuchi H, Kiuchi Y. A Case of Paracentral Corneal Perforation Treated with One-Bite Mini-Keratoplasty. Turkish journal of ophthalmology. 2021 Feb 25:51(1):55-57. doi: 10.4274/tjo.galenos.2020.40111. Epub [PubMed PMID: 33631917]
Level 3 (low-level) evidenceCunningham MA, Alexander JK, Matoba AY, Jones DB, Wilhemus KR. Management and outcome of microbial anterior scleritis. Cornea. 2011 Sep:30(9):1020-3. doi: 10.1097/ICO.0b013e31820967bd. Epub [PubMed PMID: 21694595]
Level 3 (low-level) evidenceGurnani B, Christy J, Narayana S, Kaur K, Moutappa F. Corneal Perforation Secondary to Rosacea Keratitis Managed with Excellent Visual Outcome. Nepalese journal of ophthalmology : a biannual peer-reviewed academic journal of the Nepal Ophthalmic Society : NEPJOPH. 2022 Jan:14(27):162-167. doi: 10.3126/nepjoph.v14i1.36454. Epub [PubMed PMID: 35996914]
Tan DT, Janardhanan P, Zhou H, Chan YH, Htoon HM, Ang LP, Lim LS. Penetrating keratoplasty in Asian eyes: the Singapore Corneal Transplant Study. Ophthalmology. 2008 Jun:115(6):975-982.e1 [PubMed PMID: 18061267]
Raj A, Bahadur H, Dhasmana R. Outcome of therapeutic penetrating keratoplasty in advanced infectious keratitis. Journal of current ophthalmology. 2018 Dec:30(4):315-320. doi: 10.1016/j.joco.2018.04.001. Epub 2018 Apr 26 [PubMed PMID: 30555963]
Fang A, Wang P, He R, Qu J. Surgical peripheral iridectomy via a clear-cornea phacoemulsification incision for pupillary block following cataract surgery in acute angle closure. BMC ophthalmology. 2018 May 18:18(1):120. doi: 10.1186/s12886-018-0786-2. Epub 2018 May 18 [PubMed PMID: 29776352]
Pagano L, Shah H, Al Ibrahim O, Gadhvi KA, Coco G, Lee JW, Kaye SB, Levis HJ, Hamill KJ, Semeraro F, Romano V. Update on Suture Techniques in Corneal Transplantation: A Systematic Review. Journal of clinical medicine. 2022 Feb 18:11(4):. doi: 10.3390/jcm11041078. Epub 2022 Feb 18 [PubMed PMID: 35207352]
Level 1 (high-level) evidenceSingh R, Gupta N, Vanathi M, Tandon R. Corneal transplantation in the modern era. The Indian journal of medical research. 2019 Jul:150(1):7-22. doi: 10.4103/ijmr.IJMR_141_19. Epub [PubMed PMID: 31571625]
Doğan C, Arslan OŞ. Outcomes of Therapeutic and Tectonic Penetrating Keratoplasty in Eyes with Perforated Infectious Corneal Ulcer. Turkish journal of ophthalmology. 2019 Apr 30:49(2):55-60. doi: 10.4274/tjo.galenos.2018.06937. Epub [PubMed PMID: 31055888]
Chendran P, Meng Hsien Y, Wan Abdul Halim WH. Multifacet of Cornea Patch Graft in Anterior Segment Diseases. Case reports in ophthalmological medicine. 2019:2019():6862487. doi: 10.1155/2019/6862487. Epub 2019 Nov 11 [PubMed PMID: 31885979]
Level 3 (low-level) evidenceAl-Kharashi SA, Al-Obailan MM, Almohaimeed M, Al-Torbak AA. Deep anterior lamellar Keratoplasty. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2009 Oct:23(3-4):203-9. doi: 10.1016/j.sjopt.2009.10.004. Epub 2009 Oct 24 [PubMed PMID: 23960861]
Sridhar MS. Anatomy of cornea and ocular surface. Indian journal of ophthalmology. 2018 Feb:66(2):190-194. doi: 10.4103/ijo.IJO_646_17. Epub [PubMed PMID: 29380756]
Zavala J, López Jaime GR, Rodríguez Barrientos CA, Valdez-Garcia J. Corneal endothelium: developmental strategies for regeneration. Eye (London, England). 2013 May:27(5):579-88. doi: 10.1038/eye.2013.15. Epub 2013 Mar 8 [PubMed PMID: 23470788]
Dua HS, Freitas R, Mohammed I, Ting DSJ, Said DG. The pre-Descemet's layer (Dua's layer, also known as the Dua-Fine layer and the pre-posterior limiting lamina layer): Discovery, characterisation, clinical and surgical applications, and the controversy. Progress in retinal and eye research. 2023 Jan 13:():101161. doi: 10.1016/j.preteyeres.2022.101161. Epub 2023 Jan 13 [PubMed PMID: 36642673]
Niederkorn JY. Ocular immune privilege and ocular melanoma: parallel universes or immunological plagiarism? Frontiers in immunology. 2012:3():148. doi: 10.3389/fimmu.2012.00148. Epub 2012 Jun 13 [PubMed PMID: 22707951]
Liao S, von der Weid PY. Lymphatic system: an active pathway for immune protection. Seminars in cell & developmental biology. 2015 Feb:38():83-9. doi: 10.1016/j.semcdb.2014.11.012. Epub 2014 Dec 19 [PubMed PMID: 25534659]
Level 3 (low-level) evidenceGurnani B, Kaur K. Comment on: Sensitivity and specificity of potassium hydroxide and calcofluor white stain to differentiate between fungal and Pythium filaments in corneal scrapings from patients of Pythium keratitis. Indian journal of ophthalmology. 2022 Jun:70(6):2204. doi: 10.4103/ijo.IJO_345_22. Epub [PubMed PMID: 35648022]
Level 3 (low-level) evidenceGurnani B, Christy J, Kaur K, Moutappa F, Gubert J. Successful Management of Pythium insidiosum Keratitis Masquerading as Dematiaceous Fungal Keratitis in an Immunosuppressed Asian Male. Ocular immunology and inflammation. 2023 Feb 22:():1-4. doi: 10.1080/09273948.2023.2179495. Epub 2023 Feb 22 [PubMed PMID: 36812410]
Gurnani B, Kaur K. Bacterial Keratitis. StatPearls. 2023 Jan:(): [PubMed PMID: 34662023]
Gurnani B, Kaur K. Pythium Keratitis. StatPearls. 2023 Jan:(): [PubMed PMID: 34424645]
Gurnani B, Kaur K, Agarwal S, Lalgudi VG, Shekhawat NS, Venugopal A, Tripathy K, Srinivasan B, Iyer G, Gubert J. Pythium insidiosum Keratitis: Past, Present, and Future. Ophthalmology and therapy. 2022 Oct:11(5):1629-1653. doi: 10.1007/s40123-022-00542-7. Epub 2022 Jul 5 [PubMed PMID: 35788551]
Gurnani B, Narayana S, Christy J, Rajkumar P, Kaur K, Gubert J. Successful management of pediatric pythium insidiosum keratitis with cyanoacrylate glue, linezolid, and azithromycin: Rare case report. European journal of ophthalmology. 2022 Sep:32(5):NP87-NP91. doi: 10.1177/11206721211006564. Epub 2021 Mar 28 [PubMed PMID: 33779337]
Level 3 (low-level) evidenceGurnani B, Kaur K, Venugopal A, Srinivasan B, Bagga B, Iyer G, Christy J, Prajna L, Vanathi M, Garg P, Narayana S, Agarwal S, Sahu S. Pythium insidiosum keratitis - A review. Indian journal of ophthalmology. 2022 Apr:70(4):1107-1120. doi: 10.4103/ijo.IJO_1534_21. Epub [PubMed PMID: 35325996]
Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian journal of ophthalmology. 2021 May:69(5):1095-1101. doi: 10.4103/ijo.IJO_1808_20. Epub [PubMed PMID: 33913840]
Level 2 (mid-level) evidenceSzentmáry N, Daas L, Shi L, Laurik KL, Lepper S, Milioti G, Seitz B. Acanthamoeba keratitis - Clinical signs, differential diagnosis and treatment. Journal of current ophthalmology. 2019 Mar:31(1):16-23. doi: 10.1016/j.joco.2018.09.008. Epub 2018 Oct 19 [PubMed PMID: 30899841]
Koganti R, Yadavalli T, Naqvi RA, Shukla D, Naqvi AR. Pathobiology and treatment of viral keratitis. Experimental eye research. 2021 Apr:205():108483. doi: 10.1016/j.exer.2021.108483. Epub 2021 Feb 6 [PubMed PMID: 33556334]
Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clinical ophthalmology (Auckland, N.Z.). 2014:8():571-9. doi: 10.2147/OPTH.S45921. Epub 2014 Mar 19 [PubMed PMID: 24672223]
Umlauf PC. Neuroparalytic keratitis. Journal of the American Optometric Association. 1990 Mar:61(3):196-9 [PubMed PMID: 2335706]
Level 3 (low-level) evidenceKihira K. [The role of the pharmacist in the management of the operating room]. Masui. The Japanese journal of anesthesiology. 2012 Mar:61(3):267-75 [PubMed PMID: 22571121]
Yadav S, Tandon R. Comprehensive eye examination: what does it mean? Community eye health. 2019:32(107):S1-S4 [PubMed PMID: 32123482]
Agrawal RV, Murthy S, Sangwan V, Biswas J. Current approach in diagnosis and management of anterior uveitis. Indian journal of ophthalmology. 2010 Jan-Feb:58(1):11-9. doi: 10.4103/0301-4738.58468. Epub [PubMed PMID: 20029142]
Nowińska A, Chlasta-Twardzik E, Dembski M, Ulfik-Dembska K, Wylęgała E. Corneal Analysis with Swept Source Optical Coherence Tomography in Patients with Coexisting Cataract and Fuchs Endothelial Corneal Dystrophy. Diagnostics (Basel, Switzerland). 2021 Feb 2:11(2):. doi: 10.3390/diagnostics11020223. Epub 2021 Feb 2 [PubMed PMID: 33540847]
Martin R. Cornea and anterior eye assessment with slit lamp biomicroscopy, specular microscopy, confocal microscopy, and ultrasound biomicroscopy. Indian journal of ophthalmology. 2018 Feb:66(2):195-201. doi: 10.4103/ijo.IJO_649_17. Epub [PubMed PMID: 29380757]
Aironi VD, Gandage SG. Pictorial essay: B-scan ultrasonography in ocular abnormalities. The Indian journal of radiology & imaging. 2009 Apr-Jun:19(2):109-15. doi: 10.4103/0971-3026.50827. Epub [PubMed PMID: 19881064]
Leekha S, Terrell CL, Edson RS. General principles of antimicrobial therapy. Mayo Clinic proceedings. 2011 Feb:86(2):156-67. doi: 10.4065/mcp.2010.0639. Epub [PubMed PMID: 21282489]
Todd PA, Faulds D. Ofloxacin. A reappraisal of its antimicrobial activity, pharmacology and therapeutic use. Drugs. 1991 Nov:42(5):825-76 [PubMed PMID: 1723377]
Knutsson KA, Iovieno A, Matuska S, Fontana L, Rama P. Topical Corticosteroids and Fungal Keratitis: A Review of the Literature and Case Series. Journal of clinical medicine. 2021 Mar 11:10(6):. doi: 10.3390/jcm10061178. Epub 2021 Mar 11 [PubMed PMID: 33799843]
Level 2 (mid-level) evidenceLeck A. Taking a corneal scrape and making a diagnosis. Community eye health. 2009 Dec:22(71):42-3 [PubMed PMID: 20212927]
O'Keeffe M, Nabil M. The use of mannitol in intraocular surgery. Ophthalmic surgery. 1983 Jan:14(1):55-6 [PubMed PMID: 6402747]
Lin SY, Tang SC, Tsai LK, Yeh SJ, Shen LJ, Wu FL, Jeng JS. Incidence and Risk Factors for Acute Kidney Injury Following Mannitol Infusion in Patients With Acute Stroke: A Retrospective Cohort Study. Medicine. 2015 Nov:94(47):e2032. doi: 10.1097/MD.0000000000002032. Epub [PubMed PMID: 26632702]
Level 2 (mid-level) evidenceAustin A, Lietman T, Rose-Nussbaumer J. Update on the Management of Infectious Keratitis. Ophthalmology. 2017 Nov:124(11):1678-1689. doi: 10.1016/j.ophtha.2017.05.012. Epub 2017 Sep 21 [PubMed PMID: 28942073]
Krysik K, Wroblewska-Czajka E, Lyssek-Boron A, Wylegala EA, Dobrowolski D. Total Penetrating Keratoplasty: Indications, Therapeutic Approach, and Long-Term Follow-Up. Journal of ophthalmology. 2018:2018():9580292. doi: 10.1155/2018/9580292. Epub 2018 Apr 19 [PubMed PMID: 29850220]
Pels E, Beele H, Claerhout I. Eye bank issues: II. Preservation techniques: warm versus cold storage. International ophthalmology. 2008 Jun:28(3):155-63 [PubMed PMID: 17505780]
Gupta N, Dhasmana R, Maitreya A, Badahur H. Glycerol-preserved corneal tissue in emergency corneal transplantation: An alternative for fresh corneal tissue in COVID-19 crisis. Indian journal of ophthalmology. 2020 Jul:68(7):1412-1416. doi: 10.4103/ijo.IJO_1198_20. Epub [PubMed PMID: 32587179]
Jha RK, Kurumkattil R. Can lubrication of the eyelid speculum reduce overall pain perception associated with cataract surgery by phacoemulsification performed under topical anesthesia? Indian journal of ophthalmology. 2022 May:70(5):1606-1611. doi: 10.4103/ijo.IJO_2963_21. Epub [PubMed PMID: 35502036]
Olson RJ. The effect of scleral fixation ring placement and trephine tilting on keratoplasty wound size and donor shape. Ophthalmic surgery. 1981 Jan:12(1):23-6 [PubMed PMID: 7015211]
Sharma N, Sachdev R, Jhanji V, Titiyal JS, Vajpayee RB. Therapeutic keratoplasty for microbial keratitis. Current opinion in ophthalmology. 2010 Jul:21(4):293-300. doi: 10.1097/ICU.0b013e32833a8e23. Epub [PubMed PMID: 20531191]
Level 3 (low-level) evidenceIsayenkov S, Isner JC, Maathuis FJ. Membrane localisation diversity of TPK channels and their physiological role. Plant signaling & behavior. 2011 Aug:6(8):1201-4. doi: 10.4161/psb.6.8.15808. Epub 2011 Aug 1 [PubMed PMID: 21757998]
Tabatabaei SA, Soleimani M, Johari M. Corneal ring infiltration in contact lens wearers. Oman journal of ophthalmology. 2017 May-Aug:10(2):106-108. doi: 10.4103/0974-620X.209109. Epub [PubMed PMID: 28757697]
Lim DH, Shin DH, Han G, Chung ES, Chung TY. The Incidence and Risk Factors of Lens-iris Diaphragm Retropulsion Syndrome during Phacoemulsification. Korean journal of ophthalmology : KJO. 2017 Aug:31(4):313-319. doi: 10.3341/kjo.2016.0050. Epub 2017 Jun 26 [PubMed PMID: 28682016]
Prajna NV, Sangoi K. Commentary: Timing of therapeutic keratoplasty. Indian journal of ophthalmology. 2019 Oct:67(10):1606. doi: 10.4103/ijo.IJO_793_19. Epub [PubMed PMID: 31546489]
Level 3 (low-level) evidenceZhang Q, Zhao M, Xu M, Gu F, Liu Q, Chen Y, Zhang H, Kijlstra A. Outcomes of therapeutic keratoplasty for severe infectious keratitis in Chongqing, a 16-year experience. Infection and drug resistance. 2019:12():2487-2493. doi: 10.2147/IDR.S204025. Epub 2019 Aug 12 [PubMed PMID: 31496763]
Level 2 (mid-level) evidenceNanavaty MA, Vijjan KS, Yvon C. Deep anterior lamellar keratoplasty: A surgeon's guide. Journal of current ophthalmology. 2018 Dec:30(4):297-310. doi: 10.1016/j.joco.2018.06.004. Epub 2018 Jul 10 [PubMed PMID: 30555961]
Singh G, Farooqui JH, Acharya M, Gandhi A. Comment on the Article: Outcomes of Therapeutic Keratoplasty in Cases of Refractory Infectious Keratitis. Journal of current ophthalmology. 2021 Apr-Jun:33(2):215-216. doi: 10.4103/joco.joco_67_20. Epub 2021 Jul 5 [PubMed PMID: 34409237]
Level 3 (low-level) evidenceKaur K, Gurnani B. Lens Abscess. StatPearls. 2024 Jan:(): [PubMed PMID: 36512661]
Balamurugan S, Gurnani B, Kaur K, Gireesh P, Narayana S. Traumatic intralenticular abscess-What is so different? The Indian journal of radiology & imaging. 2020 Jan-Mar:30(1):92-94. doi: 10.4103/ijri.IJRI_369_19. Epub 2020 Mar 30 [PubMed PMID: 32476758]
Schepens CL. Clinical and research aspects of subtotal open-sky vitrectomy. XXXVII Edward Jackson Memorial Lecture. American journal of ophthalmology. 1981 Feb:91(2):143-71 [PubMed PMID: 6970523]
Level 3 (low-level) evidenceRoy A, Kamra D, Murthy SI, Mohamed A, Chaurasia S, Fernandes M, Das S, Sharma S. Intermediate outcomes of therapeutic penetrating keratoplasty for severe microbial keratitis using glycerol-preserved donor corneas during the COVID-19 pandemic. Indian journal of ophthalmology. 2021 Oct:69(10):2812-2817. doi: 10.4103/ijo.IJO_1183_21. Epub [PubMed PMID: 34571640]
Cowden JW. The clinical evaluation of 9-0 and 10-0 monofilament Polyglactin 910 absorbable suture for corneal surgery. Ophthalmic surgery. 1979 Jan:10(1):50-2 [PubMed PMID: 370706]
Drabble E, Spanopoulou S, Sioka E, Politaki E, Paraskeva I, Palla E, Stockley L, Zacharoulis D. How to tie dangerous surgical knots: easily. Can we avoid this? BMJ surgery, interventions, & health technologies. 2021:3(1):e000091. doi: 10.1136/bmjsit-2021-000091. Epub 2021 Jul 13 [PubMed PMID: 35047808]
Thanathanee O, Sripawadkul W, Anutarapongpan O, Luanratanakorn P, Suwan-Apichon O. Outcome of Therapeutic Penetrating Keratoplasty Using Glycerol-Preserved Donor Corneas in Infectious Keratitis. Cornea. 2016 Sep:35(9):1175-8. doi: 10.1097/ICO.0000000000000841. Epub [PubMed PMID: 27429078]
Stevens S. How to apply an eye pad, shield, and bandage. Community eye health. 2010 Dec:23(74):56 [PubMed PMID: 21311669]
Gokhale NS. Medical management approach to infectious keratitis. Indian journal of ophthalmology. 2008 May-Jun:56(3):215-20 [PubMed PMID: 18417822]
Ansari Z, Miller D, Galor A. Current Thoughts in Fungal Keratitis: Diagnosis and Treatment. Current fungal infection reports. 2013 Sep 1:7(3):209-218 [PubMed PMID: 24040467]
Gurnani B, Kaur K. Contact Lens–Related Complications. StatPearls. 2024 Jan:(): [PubMed PMID: 36512659]
Azevedo Magalhaes O, Shalaby Bardan A, Zarei-Ghanavati M, Liu C. Literature review and suggested protocol for prevention and treatment of corneal graft rejection. Eye (London, England). 2020 Mar:34(3):442-450. doi: 10.1038/s41433-019-0517-9. Epub 2019 Jul 22 [PubMed PMID: 31332293]
Gurnani B, Kaur K. Traumatic Iris Reconstruction. StatPearls. 2023 Jan:(): [PubMed PMID: 35201728]
Bajracharya L, Gurung R. Outcome of therapeutic penetrating keratoplasty in a tertiary eye care center in Nepal. Clinical ophthalmology (Auckland, N.Z.). 2015:9():2299-304. doi: 10.2147/OPTH.S92176. Epub 2015 Dec 7 [PubMed PMID: 26673279]
McCann VH, Philips CA, Quigley TR. Preoperative and postoperative management: the role of allied health professionals. The Orthopedic clinics of North America. 1975 Jul:6(3):881-906 [PubMed PMID: 1099512]
Nieuwlaat R, Wilczynski N, Navarro T, Hobson N, Jeffery R, Keepanasseril A, Agoritsas T, Mistry N, Iorio A, Jack S, Sivaramalingam B, Iserman E, Mustafa RA, Jedraszewski D, Cotoi C, Haynes RB. Interventions for enhancing medication adherence. The Cochrane database of systematic reviews. 2014 Nov 20:2014(11):CD000011. doi: 10.1002/14651858.CD000011.pub4. Epub 2014 Nov 20 [PubMed PMID: 25412402]
Level 1 (high-level) evidence