 Transversus Thoracic Muscle Plane Block (TTMPB)
Transversus Thoracic Muscle Plane Block (TTMPB)
Introduction
The transversus thoracic muscle plane block (TTMPB) is a fascial plane nerve block that has become popular as of late.[1] It is most commonly performed following cardiothoracic surgeries (or any surgeries requiring sternotomy) to provide analgesia to the anterior chest wall.[2][3] The TTMPB, and thoracic fascial plane blocks, are increasingly being employed as part of enhanced recovery after surgery (ERAS) protocols for cardiothoracic procedures. They have been shown to significantly reduce both the time to extubation and the incidence of acute and chronic perioperative pain.[4][5]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The sternum is innervated by the intercostal nerves of the somatic nervous system, which arise from the anterior rami of spinal nerves of the thoracic spine. More specifically, the anterior branches of intercostal nerves of T2-T6 largely innervate much of the sternum.[2][6][7]
In terms of musculature, the anterior chest wall consists of the external, internal, and innermost intercostal muscles, the transversus thoracis muscles, and the subcostales muscles. The transversus thoracis is a thin muscle that lies in the same plane as the innermost intercostal and subcostal muscles.[7] These muscles separate the chest wall from the parietal pleura at this level. Medially, the transversus thoracis attaches to the lower posterior sternum down to the xiphoid process and spreads across the chest to attach to the thoracic ribcage, most often to ribs two through six.[8][9]
The TTMPB is intended to provide analgesic coverage to these same corresponding thoracic dermatomal levels. There is some variability in these attachments between individuals and even between the contralateral side of the same individual. The transversus thoracis functions to depress the ribs and aids in forced exhalation.[8] The internal thoracic artery, an important vessel often utilized during coronary artery bypass grafting (CABG) surgery, typically courses anteriorly to the muscle.[9]
Indications
The TTMPB is indicated in any surgical procedure where the sternum will be incised. This means that it has great utility in open heart procedures where a median sternotomy is typically performed. It was first described in 2015 by Ueshima et al.; since then, multiple studies reporting its benefit in cardiac surgeries have emerged.[1][10]
While it is arguably of best use for perioperative pain management for a sternotomy, any procedure where analgesia is needed in the anterior T2-T6 dermatomes would benefit from a TTMPB. This would include various thoracic surgeries, breast surgeries (when combined with a pectoralis (PECS) nerve block(s)), as well as other minor procedures such as subcutaneous implantable cardioverter-defibrillator (S-ICD) placement.[11][12][13][14] It may also be used in patients with sternal fractures and has been documented as a viable analgesic alternative for these situations.[15][16][17]
Contraindications
Contraindications to TTMPB are similar to those of other regional nerve blocks.[18][19] These include:
- Patient refusal
- Allergy to local anesthetics
- Infection at the site of injection
- Tumor at the site of injection
Additionally, caution should be taken in patients with liver dysfunction, given that local amide anesthetics are hepatically metabolized. Using a local amide anesthetic such as bupivacaine in these patients puts them at risk for local anesthetic systemic toxicity (LAST), which may manifest as neurologic symptoms (circumoral numbness, altered mental status, seizures) and, if severe enough, cardiac arrest and death.[20]
Pneumothorax is a serious potential complication of the TTMPB block. As such, care should be taken when performing a TTMPB for patients with compromised pulmonary function. The development of a pneumothorax could be catastrophic for such a patient.[1]
Lastly, while not a neuraxial technique, coagulopathy should be considered when performing a TTMPB, as some may consider it a deep nerve block in a non-compressible fascial space. If inadvertent vascular damage occurs, bleeding might be challenging to control.[3]
Equipment
The TTMPB is performed under ultrasound guidance, which minimizes the risk of complications. The basic equipment needed to perform the block includes:
- Ultrasound machine with a high-frequency linear transducer
- Sterile gloves
- Sterile ultrasound sleeve and gel
- Chlorhexidine or other antiseptic preparation
- Nerve block needle, typically 80 mm to 100 mm
- Two (if bilateral) 20 to 30 mL syringes containing local anesthetic +/- adjuncts
- Local anesthetic: long-acting agents such as bupivacaine or ropivacaine are typically used
- Physiologic monitors, including a pulse oximeter, blood pressure monitoring, and electrocardiography
Personnel
The TTMPB should be performed by an individual qualified in regional anesthesia who routinely performs peripheral nerve blocks in practice. This is most often an anesthesiologist. A second provider or nurse must perform the universal timeout or equivalent before proceeding with the block.
This additional provider would also assist the anesthesiologist during the block, holding the local anesthetic solution and injecting when the correct fascial plane is reached, as determined by the anesthesiologist guiding the needle via ultrasonography.
Preparation
Before performing any regional anesthetic technique, a review of the patient’s past medical and surgical history should be performed. The patient’s coagulation status should be ascertained, and knowledge about using any potential anticoagulants should be. A discussion should be had with the patient regarding the risks, benefits, and alternatives of the procedure. The patient should express understanding and consent to undergo the block.
The patient should have intravenous access and be hooked up to American Society of Anesthesiology standard monitors, including blood pressure, pulse oximetry, and electrocardiography. If done while the patient is awake, anxiolysis with midazolam or another agent may be needed, as well as a local anesthetic for skin and subcutaneous infiltration.
As mentioned previously, a universal protocol or time-out should be performed before beginning, where the patient’s name, date of birth, site, and laterality of the block and/or surgery are verified with the proceduralist, patient, and a nurse or second healthcare provider. Only when this is done, and all agree, should one proceed with the block.
Technique or Treatment
The TTMPB is most often described as being performed at the level of T4-T5.[4] The local anesthetic solution is drawn up, and the skin is prepped with an antiseptic solution of the provider’s choosing. After sterilely applying all personal protective equipment, a sterile ultrasound cover should be placed over a high-frequency linear transducer and placed approximately 1 cm lateral to the sternal border. The T4-T5 intercostal space is then identified under ultrasound guidance in a parasagittal view, and the nerve block needle is inserted in-plane into the probe. The needle is then guided to the transversus thoracis muscle plane between this muscle and the internal intercostal muscle. Here, the local anesthetic solution is deposited in a single-shot manner in small aliquots of volume, being mindful of aspirating before each injection to avoid intravascular and intrapleural administration. The ideal view needed to perform the block is demonstrated in Figure 1. As reported by Murata et al., confirmation of successful placement can be noted by the downward movement of the pleura.[21]
As this is a relatively novel block, there have been variations in where and how the TTMPB is performed. The T4-T5 intercostal space is most often targeted, as it was used by Ueshima et al., who first published their findings on the block. A cadaveric study has also corroborated the T4-T5 intercostal space as an ideal place for the TTMPB, showing the spread of local anesthetic from the manubrium of the sternum to the T5-T6 intercostal space.[22] However, the concept of a parasternal block that targets similar nerves and dermatomes as the TTMPB has been reported in the literature as early as 2005.[23]
Complications
Complications related specifically to the TTMPB occur quite rarely. In general, classic complications observed during or following regional anesthetic blocks include excessive bleeding at the puncture site, development of infection at the site of the block, neurovascular damage, and LAST.[19]
The TTMPB poses specific complication risks, given the surrounding anatomy. Given the proximity of the transversus thoracis muscle to the pleura, puncture of the pleural layer from an errant needle tip may lead to pneumothorax development. Similarly, the internal thoracic artery and pericardium are nearby structures that may also be damaged from poor needle placement and can lead to complications such as hemothorax and hemopericardium.[1] Utilizing the color wave doppler, Figure 2 provides a view of the internal thoracic artery, which lies in the same plane as the transversus thoracis muscle.
Clinical Significance
As the world's population continues to age, the amount of surgery being performed continues to rise. Cardiothoracic surgery is no exception. This increased surgical demand directly correlates to a need for continued advancement in pain management, as open cardiothoracic surgery is directly linked to poorly controlled postoperative pain and the development of chronic poststernotomy pain syndromes (PSPS).[3][24][25][26] Neuraxial techniques such as thoracic epidural analgesia and the paravertebral nerve block would be ideal for many open cardiothoracic procedures; however, the risk of epidural hematoma formation—especially when these patients are fully anticoagulated intraoperatively—makes these options unfavorable in most circumstances.[18][27] This is why fascial plane blocks such as the TTMPB have become more widespread, as they eliminate this risk and generally do not require patients to be off anticoagulation to perform.[3]
Poststernotomy pain syndromes are complex pain syndromes that can not only include sternal pain but encompass musculoskeletal pain of the trunk, head, neck, and upper extremities.[25] Inadequate pain management following cardiothoracic surgery can lead to significant cardiopulmonary complications, as there is an increased sympathetic surge resulting from the release of catecholamines.[4] This leads to increased blood pressure, heart rate, and respiratory rate that can cause sequelae such as increased postsurgical bleeding, myocardial demand, and ischemia. The pain experienced can also cause thoracic splinting and hypoventilation, leading to issues such as delayed extubation, extubation failure, and reintubation.[5]
In the past, it had been commonplace to liberally use opioids to treat such postsurgical pain and blunt the hemodynamic response that comes with it. However, this presents its problems, as the administration of excessive opioids may lead to delayed extubation and the development of pain syndromes such as opioid-induced hyperalgesia. This is ironic because inadequately treated pain may lead to the same complications, as previously mentioned.[2][3][5][25]
In general, the TTMPB and chest wall fascial plane blocks have been increasingly employed to mitigate these sequelae and have been utilized in ERAS protocols following cardiothoracic surgery. In addition, utilization of the TTMPB has allowed certain minimally invasive procedures to be performed with minimal-to-no sedation in patients who would otherwise poorly tolerate the hemodynamic swings that occur with general anesthesia.
There are several studies in which the TTPMB has been shown to decrease perioperative opioid use. Aydin et al. reported that in patients who underwent a median sternotomy and received a preoperative TTMPB with 0.25% bupivacaine, there was a significant reduction in postoperative opioid use 12 hours after surgery, as well as a significantly less incidence of postoperative nausea.[12] Shokri et al. also reported overall significantly reduced postoperative morphine consumption up to 24 hours after surgery, as well as significantly reduced postoperative pain scores and first analgesic requirements in patients who received a sternotomy and a TTMPB.[4] Hamed et al. reported similar findings, replacing morphine with fentanyl.[11]
Regarding postoperative ventilation, it has been reported that incorporating the TTMPB into cardiothoracic ERAS pathways bodes well regarding patient outcomes. In the study by Shokri et al., ventilation time and ICU stay were reported to be significantly shorter in the group that received a TTMPB.[4] Zhang et al. 2021. reported similar results for these same two variables.[13] The TTMPB's analgesic potential has been shown to be great, as it has been described to be able to completely relieve poststernotomy pain and prevent reintubation in at least one case report.[28]
Evidence of the TTMPB's efficacy in the pediatric population is also robust. In the pediatric population, multiple studies have reported significantly decreased ventilation time and significantly reduced pain scores and perioperative opioid consumption in pediatric patients undergoing cardiac surgery who received a TTPMB.[14][29][30][31]
Finally, the TTMPB reduces the incidence of chronic PSPS by decreasing the pain sensitization induced by open cardiothoracic surgery. It has also been used as a treatment for patients who have developed chronic pain from these surgical incisions.[2][32][33] Piracinni et al. described a case of a patient living with post-thoracotomy pain syndrome for ten months following surgery. The patient received a combination of a TTMPB and a parasternal block. The patient was treated with three weekly injections of a solution of ropivacaine and triamcinolone and immediately reported a complete resolution of pain that lasted for three months.[33]
The TTMPB shows great promise as an integral component of multimodal analgesia following cardiothoracic surgery, as it has been shown to facilitate faster extubation times, decrease and prevent acute and chronic pain, and is a variable alternative to neuraxial anesthesia when neuraxial approaches to pain management are contraindicated.
Enhancing Healthcare Team Outcomes
Major cardiothoracic surgery—the typical scenario in which a TTMPB is utilized—is an orchestrated production consisting of a multidisciplinary healthcare team for the patient's perioperative care, with pain management being a significant aspect of this care. The surgeons, the anesthesiologist, the perfusionists, the perioperative nursing staff, the cardiologists, the pharmacists, and the rest of the patient's hospital team – clear and compelling communication between all parties involved leads to better patient outcomes.[34]
Before performing any nerve block or procedure, a thorough review of the patient's medical record is required to select interventions that will provide maximal dermatomal coverage and analgesic benefit. A universal timeout should be performed before beginning the block to eliminate confusion, minimize errors, and answer questions regarding the procedure. The TTMPB should be performed by an anesthesiologist proficient in regional anesthesia to provide the most accurate needle placement and local anesthetic deposition possible.
After performing a TTMPB, the patient should be stationed in a unit that frequently monitors the patient's cardiopulmonary status, whether in the emergency department connected to ASA standard monitors or in the intensive care unit postoperatively. This is because complications following a TTMPB, while rare, could be severe and require prompt attention from interprofessional team members who recognize the warning signs.
Media
(Click Image to Enlarge)
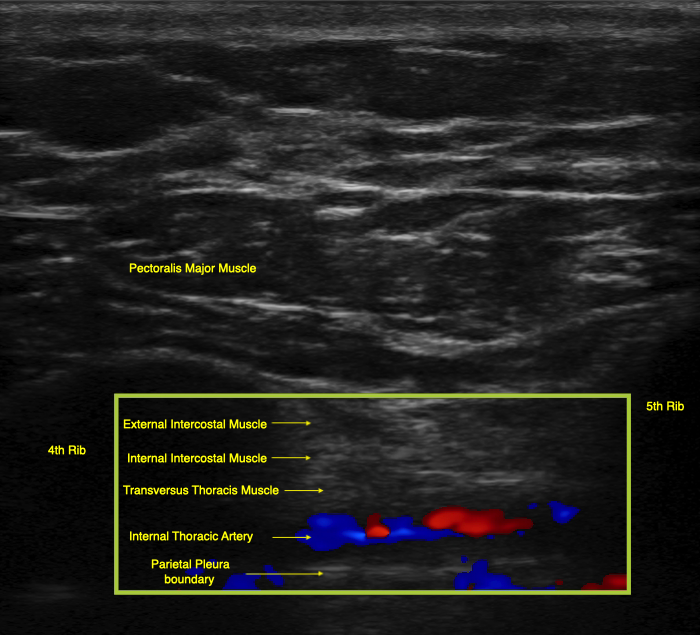
The internal thoracic artery lies in the same plane as the transversus thoracis muscle. Care should be taken to avoid injuring this vessel when performing a TTMPB. Contributed by Geoffrey Hayward, MD
(Click Image to Enlarge)
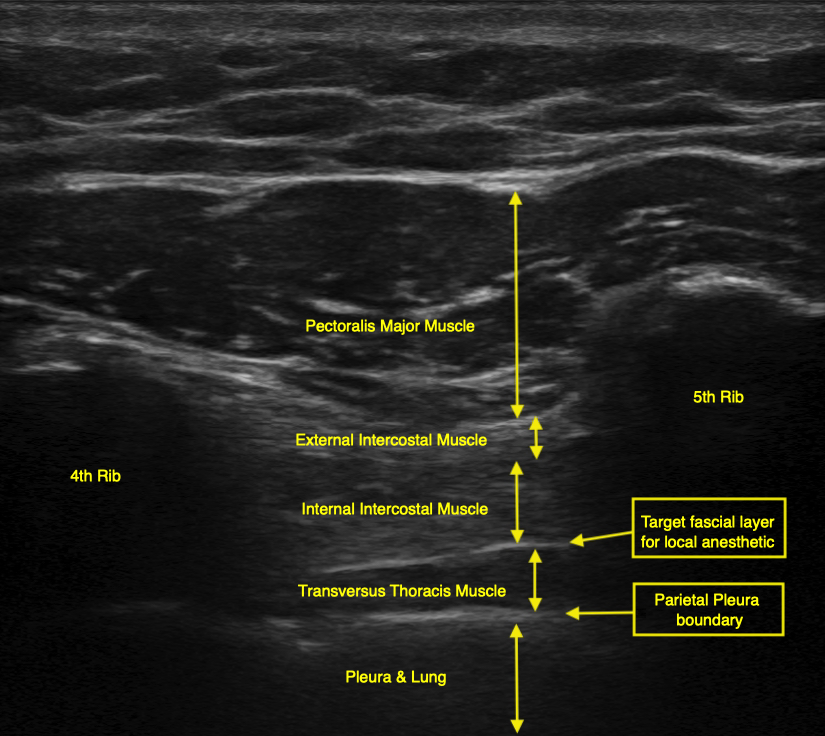
Proper sonographic view when performing a TTMPB. Local anesthetic should be deposited in the fascial layer between the transversus thoracis muscle and the internal intercostal muscle, as noted by the bright white fascial boundary between the two muscles. Contributed by Geoffrey Hayward, MD
References
Fujii S, Bairagi R, Roche M, Zhou JR. Transversus Thoracis Muscle Plane Block. BioMed research international. 2019:2019():1716365. doi: 10.1155/2019/1716365. Epub 2019 Jul 7 [PubMed PMID: 31360703]
Kelava M, Alfirevic A, Bustamante S, Hargrave J, Marciniak D. Regional Anesthesia in Cardiac Surgery: An Overview of Fascial Plane Chest Wall Blocks. Anesthesia and analgesia. 2020 Jul:131(1):127-135. doi: 10.1213/ANE.0000000000004682. Epub [PubMed PMID: 32032103]
Level 3 (low-level) evidenceJiang T, Ting A, Leclerc M, Calkins K, Huang J. Regional Anesthesia in Cardiac Surgery: A Review of the Literature. Cureus. 2021 Oct:13(10):e18808. doi: 10.7759/cureus.18808. Epub 2021 Oct 15 [PubMed PMID: 34804666]
Shokri H, Ali I, Kasem AA. Evaluation of the Analgesic Efficacy of Bilateral Ultrasound-Guided Transversus Thoracic Muscle Plane Block on Post-Sternotomy Pain: A Randomized Controlled Trial. Local and regional anesthesia. 2021:14():145-152. doi: 10.2147/LRA.S338685. Epub 2021 Nov 12 [PubMed PMID: 34803399]
Level 1 (high-level) evidenceHamilton C, Alfille P, Mountjoy J, Bao X. Regional anesthesia and acute perioperative pain management in thoracic surgery: a narrative review. Journal of thoracic disease. 2022 Jun:14(6):2276-2296. doi: 10.21037/jtd-21-1740. Epub [PubMed PMID: 35813725]
Level 3 (low-level) evidenceBall M, Falkson SR, Fakoya AO, Adigun OO. Anatomy, Angle of Louis. StatPearls. 2025 Jan:(): [PubMed PMID: 29083679]
Tang A, Bordoni B. Anatomy, Thorax, Muscles. StatPearls. 2022 Jan:(): [PubMed PMID: 30855905]
Donley ER, Holme MR, Loyd JW. Anatomy, Thorax, Wall Movements. StatPearls. 2023 Jan:(): [PubMed PMID: 30252279]
Jelev L, Hristov S, Ovtscharoff W. Variety of transversus thoracis muscle in relation to the internal thoracic artery: an autopsy study of 120 subjects. Journal of cardiothoracic surgery. 2011 Jan 27:6():11. doi: 10.1186/1749-8090-6-11. Epub 2011 Jan 27 [PubMed PMID: 21272314]
Level 2 (mid-level) evidenceUeshima H, Kitamura A. Clinical experiences of ultrasound-guided transversus thoracic muscle plane block: a clinical experience. Journal of clinical anesthesia. 2015 Aug:27(5):428-9. doi: 10.1016/j.jclinane.2015.03.040. Epub 2015 May 3 [PubMed PMID: 25944788]
Hamed MA, Boules ML, Sobhy MM, Abdelhady MA. The Analgesic Efficacy of Ultrasound-Guided Bilateral Transversus Thoracic Muscle Plane Block After Open-Heart Surgeries: A Randomized Controlled Study. Journal of pain research. 2022:15():675-682. doi: 10.2147/JPR.S355231. Epub 2022 Mar 5 [PubMed PMID: 35281480]
Level 1 (high-level) evidenceAydin ME, Ahiskalioglu A, Ates I, Tor IH, Borulu F, Erguney OD, Celik M, Dogan N. Efficacy of Ultrasound-Guided Transversus Thoracic Muscle Plane Block on Postoperative Opioid Consumption After Cardiac Surgery: A Prospective, Randomized, Double-Blind Study. Journal of cardiothoracic and vascular anesthesia. 2020 Nov:34(11):2996-3003. doi: 10.1053/j.jvca.2020.06.044. Epub 2020 Jun 18 [PubMed PMID: 32665179]
Level 1 (high-level) evidenceZhang Y, Li X, Chen S. Bilateral transversus thoracis muscle plane block provides effective analgesia and enhances recovery after open cardiac surgery. Journal of cardiac surgery. 2021 Aug:36(8):2818-2823. doi: 10.1111/jocs.15666. Epub 2021 May 28 [PubMed PMID: 34047403]
Zhang Y, Chen S, Gong H, Zhan B. Efficacy of Bilateral Transversus Thoracis Muscle Plane Block in Pediatric Patients Undergoing Open Cardiac Surgery. Journal of cardiothoracic and vascular anesthesia. 2020 Sep:34(9):2430-2434. doi: 10.1053/j.jvca.2020.02.005. Epub 2020 Feb 11 [PubMed PMID: 32151511]
Thomas KP, Sainudeen S, Jose S, Nadhari MY, Macaire PB. Ultrasound-Guided Parasternal Block Allows Optimal Pain Relief and Ventilation Improvement After a Sternal Fracture. Pain and therapy. 2016 Jun:5(1):115-22. doi: 10.1007/s40122-016-0050-5. Epub 2016 Mar 21 [PubMed PMID: 27001634]
Zhao Y, Jin W, Pan P, Feng S, Fu D, Yao J. Ultrasound-guided transversus thoracic muscle plane-pectoral nerve block for postoperative analgesia after modified radical mastectomy: a comparison with the thoracic paravertebral nerve block. Perioperative medicine (London, England). 2022 Jul 27:11(1):39. doi: 10.1186/s13741-022-00270-3. Epub 2022 Jul 27 [PubMed PMID: 35883207]
Bhatt HV, Hernandez N, Shariat A. Successful Use of Serratus and Transversus Thoracic Plane Blocks for Subcutaneous Implantable Cardioverter-Defibrillator Placement. Journal of cardiothoracic and vascular anesthesia. 2018 Feb:32(1):e22-e23. doi: 10.1053/j.jvca.2017.09.019. Epub 2017 Sep 15 [PubMed PMID: 29217249]
Ben Aziz M, Mukhdomi J. Thoracic Paravertebral Block. StatPearls. 2023 Jan:(): [PubMed PMID: 34033322]
Folino TB, Mahboobi SK. Regional Anesthetic Blocks. StatPearls. 2023 Jan:(): [PubMed PMID: 33085385]
Gitman M, Fettiplace MR, Weinberg GL, Neal JM, Barrington MJ. Local Anesthetic Systemic Toxicity: A Narrative Literature Review and Clinical Update on Prevention, Diagnosis, and Management. Plastic and reconstructive surgery. 2019 Sep:144(3):783-795. doi: 10.1097/PRS.0000000000005989. Epub [PubMed PMID: 31461049]
Murata H, Hida K, Hara T. Transverse Thoracic Muscle Plane Block: Tricks and Tips to Accomplish the Block. Regional anesthesia and pain medicine. 2016 May-Jun:41(3):411-2. doi: 10.1097/AAP.0000000000000374. Epub [PubMed PMID: 27093277]
Fujii S, Vissa D, Ganapathy S, Johnson M, Zhou J. Transversus Thoracic Muscle Plane Block on a Cadaver With History of Coronary Artery Bypass Grafting. Regional anesthesia and pain medicine. 2017 Jul/Aug:42(4):535-537. doi: 10.1097/AAP.0000000000000607. Epub [PubMed PMID: 28632672]
McDonald SB, Jacobsohn E, Kopacz DJ, Desphande S, Helman JD, Salinas F, Hall RA. Parasternal block and local anesthetic infiltration with levobupivacaine after cardiac surgery with desflurane: the effect on postoperative pain, pulmonary function, and tracheal extubation times. Anesthesia and analgesia. 2005 Jan:100(1):25-32. doi: 10.1213/01.ANE.0000139652.84897.BD. Epub [PubMed PMID: 15616047]
Level 1 (high-level) evidenceKleiman AM, Sanders DT, Nemergut EC, Huffmyer JL. Chronic Poststernotomy Pain: Incidence, Risk Factors, Treatment, Prevention, and the Anesthesiologist's Role. Regional anesthesia and pain medicine. 2017 Nov/Dec:42(6):698-708. doi: 10.1097/AAP.0000000000000663. Epub [PubMed PMID: 28937533]
van Leersum NJ, van Leersum RL, Verwey HF, Klautz RJ. Pain symptoms accompanying chronic poststernotomy pain: a pilot study. Pain medicine (Malden, Mass.). 2010 Nov:11(11):1628-34. doi: 10.1111/j.1526-4637.2010.00975.x. Epub [PubMed PMID: 21044253]
Level 3 (low-level) evidenceBordoni B, Marelli F, Morabito B, Sacconi B, Severino P. Post-sternotomy pain syndrome following cardiac surgery: case report. Journal of pain research. 2017:10():1163-1169. doi: 10.2147/JPR.S129394. Epub 2017 May 15 [PubMed PMID: 28553137]
Level 3 (low-level) evidenceBalan C, Bubenek-Turconi SI, Tomescu DR, Valeanu L. Ultrasound-Guided Regional Anesthesia-Current Strategies for Enhanced Recovery after Cardiac Surgery. Medicina (Kaunas, Lithuania). 2021 Mar 25:57(4):. doi: 10.3390/medicina57040312. Epub 2021 Mar 25 [PubMed PMID: 33806175]
de Haan JB, Yu D, Hernandez N, Sen S. Preventing intubation with the transverse thoracic muscle plane block. Annals of cardiac anaesthesia. 2020 Oct-Dec:23(4):540-541. doi: 10.4103/aca.ACA_12_19. Epub [PubMed PMID: 33109825]
Chaudhary V, Chauhan S, Choudhury M, Kiran U, Vasdev S, Talwar S. Parasternal intercostal block with ropivacaine for postoperative analgesia in pediatric patients undergoing cardiac surgery: a double-blind, randomized, controlled study. Journal of cardiothoracic and vascular anesthesia. 2012 Jun:26(3):439-42. doi: 10.1053/j.jvca.2011.10.012. Epub 2011 Dec 16 [PubMed PMID: 22176767]
Level 1 (high-level) evidenceCakmak M, Isik O. Transversus Thoracic Muscle Plane Block for Analgesia After Pediatric Cardiac Surgery. Journal of cardiothoracic and vascular anesthesia. 2021 Jan:35(1):130-136. doi: 10.1053/j.jvca.2020.07.053. Epub 2020 Jul 23 [PubMed PMID: 32798166]
Abdelbaser II, Mageed NA. Analgesic efficacy of ultrasound guided bilateral transversus thoracis muscle plane block in pediatric cardiac surgery: a randomized, double-blind, controlled study. Journal of clinical anesthesia. 2020 Dec:67():110002. doi: 10.1016/j.jclinane.2020.110002. Epub 2020 Jul 24 [PubMed PMID: 32717448]
Level 1 (high-level) evidenceRivat C, Bollag L, Richebé P. Mechanisms of regional anaesthesia protection against hyperalgesia and pain chronicization. Current opinion in anaesthesiology. 2013 Oct:26(5):621-5. doi: 10.1097/01.aco.0000432511.08070.de. Epub [PubMed PMID: 23995064]
Level 3 (low-level) evidencePiraccini E, Biondi G, Byrne H, Calli M, Bellantonio D, Musetti G, Maitan S. Ultrasound Guided Transversus Thoracic Plane block, Parasternal block and fascial planes hydrodissection for internal mammary post thoracotomy pain syndrome. European journal of pain (London, England). 2018 Oct:22(9):1673-1677. doi: 10.1002/ejp.1249. Epub 2018 May 31 [PubMed PMID: 29770535]
Engelman DT, Ben Ali W, Williams JB, Perrault LP, Reddy VS, Arora RC, Roselli EE, Khoynezhad A, Gerdisch M, Levy JH, Lobdell K, Fletcher N, Kirsch M, Nelson G, Engelman RM, Gregory AJ, Boyle EM. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery After Surgery Society Recommendations. JAMA surgery. 2019 Aug 1:154(8):755-766. doi: 10.1001/jamasurg.2019.1153. Epub [PubMed PMID: 31054241]
Level 1 (high-level) evidence