 Anatomy, Shoulder and Upper Limb, Pronator Teres
Anatomy, Shoulder and Upper Limb, Pronator Teres
Introduction
The word pronator originates from the Latin meaning “lying face downward,” and this appropriately describes the function of the pronator teres, which rotates the forearm so that the palm faces downwards. The pronator teres is a fusiform forearm muscle found in the superficial layer of the anterior compartment of the forearm. Its primary function is to pronate the forearm and assist in forearm flexion. This muscle, therefore, has essential involvement in sporting activities.[1]
The median nerve innervates the pronator teres as it travels through the pronator teres’ two heads originating from the humerus and the ulna. The median nerve is thus at risk for compression at this site in cases of pronator teres overuse or even hypertrophy. Clinically, median nerve compression at this site is known as pronator teres syndrome. Patients with this syndrome most commonly experience pain and numbness, but motor dysfunction may also be present in some cases.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The pronator teres has two heads, each named after its site of origin. The humeral head is the larger and more superficial head and originates on the medial supracondylar ridge of the humerus, just superior to the medial epicondyle. The ulnar head lies deep to the humeral head and originates from the coronoid process of the ulna. The two heads join and travel distally, deep to the brachioradialis in the superficial layer of the anterior compartment of the forearm, to insert on the pronator tuberosity of the radius.
The insertion site is a rough area found on the lateral surface of the midshaft of the radius located inferior to the supinator muscle. Occasionally, the pronator teres must be elevated off the radius at its insertion to allow for plate fixation of radial shaft fractures. The median nerve enters the forearm between the two heads of the pronator teres, and the ulnar head separates the median nerve from the ulnar artery.[1]
The pronator teres is part of an important landmark for the cubital fossa, which is the triangular area located on the anterior upper limb between the arm and forearm. The lateral end of the pronator teres forms the medial border of the cubital fossa.[2]
As its name suggests, the primary function of the pronator teres is to pronate the forearm. Acting synergistically with the pronator quadratus, the pronator teres pulls the radius medially, which causes the radial head to rotate around the proximal ulna. This pronation movement brings the hand from an upward palm position (supination) to a downward-facing palm (pronation). The pronator teres also plays a small role in flexion of the elbow.[3]
Embryology
The paraxial mesoderm germ layer gives rise to the myotome from which all limb muscles arise. Nearby, the lateral plate mesoderm gives rise to the bones, connective tissue, and vasculature of the limbs. Neural structures are derived from neural crest cells. Limb buds typically appear at four weeks gestational age, and the bones and muscles are established by eight weeks. Following the 8-week mark, the muscles increase in size.[4]
Blood Supply and Lymphatics
The blood supply for the pronator teres is from branches of the brachial, radial, and ulnar arteries. Branches from the ulnar artery include the common interosseus artery and the anterior ulnar recurrent artery. The radial recurrent artery is a branch off of the radial artery. The inferior ulnar collateral arteries are branches off of the ulnar artery. Each of these branches provides vascularization to the pronator teres.[5][6]
Nerves
The median nerve (C6, C7) innervates the pronator teres. The median nerve is a terminal branch of the brachial plexus originating from the medial and lateral cords. The median nerve also provides motor innervation of the forearm flexors and thenar eminence as well as sensation on the radial portion of the hand.[7]
Muscles
The pronator teres has a synergistic pronation effect with the pronator quadratus, a square-shaped muscle that originates on the anteromedial ulna and travels perpendicular to the direction of the forearm to insert on the anterolateral radius. The radius is pulled toward and over the ulna during contraction, causing the pronation movement.[3] The median nerve also innervates this muscle.[7] While the pronator teres is located on the proximal forearm, this muscle is located on the distal forearm.[3]
The primary muscles exerting flexion of the forearm at the elbow are the biceps brachii, brachioradialis, and brachialis. The pronator teres has a synergistic effect with these muscles as it also provides a small amount of assistance with forearm flexion.[8]
The primary antagonist is the supinator muscle which originates on parts of the humerus, ulna, radial collateral ligament, and annular ligament. It inserts on the proximal radial shaft and supinates the forearm. Another antagonist to pronation is the biceps brachii, which also supinates the forearm.[9]
Physiologic Variants
The literature has reported that the ulnar head of the pronator teres may be absent in some cases.[1] Nebot-Cegarra et al. found the ulnar head present in 78.3% of subjects in a study of 60 upper limbs.[10]
Surgical Considerations
Pronator teres syndrome is a compressive neuropathy of the median nerve as it travels between the two heads of the pronator teres. Its clinical manifestations include pain, paresthesias, and weakness.
Although most patients improve with conservative measures, surgical decompression may be an option in severe forms of this syndrome or for those who failed conservative treatment. Surgery aims to decompress the median nerve between the two heads of the pronator teres. The superficial facia of the pronator teres is first released. This can be followed by either partial or complete resection of tendon origin, depending on the extent of median nerve compression.[11]
Patients undergoing this surgery show good outcomes demonstrating improvement in the Disabilities of the Arm Shoulder and Hand (DASH) survey score and the Visual Analog Scale (VAS) pain score.[12] However, in one study, despite adequate decompression at the pronator teres, up to 25% of patients developed carpal tunnel syndrome.[12]
Medial epicondylitis, also known as golfer’s elbow, is a condition characterized by pain along the medial aspect of the elbow. The pain often has an insidious onset and is worsened by forearm pronation or wrist flexion. The pronator teres is often implicated as a source of pathology in this condition. The mainstay of treatment is conservative and thus includes stretching and strengthening exercises, but surgical interventions aimed at excising abnormal tissue, which may involve the pronator teres, can improve patients’ pain and functional status in recalcitrant cases.[13]
Clinical Significance
Pronator teres syndrome is a rare syndrome characterized by pain and numbness in the forearm and is caused by compression of the median nerve between the humeral head and ulnar head of the pronator teres. Patients with this syndrome often experience neuropathic symptoms and weakness of the muscles innervated by the anterior interosseous (AIN) branch of the median nerve. The muscles commonly involved are the flexor pollicis longus, flexor digitorum profundus of the second digit, and the pronator quadratus. The pain caused by this syndrome tends to be more concentrated at the wrist and is worsened by excessive pronation of the forearm.[1]
Patients may often find themselves dropping items and have a new sense of clumsiness. They also may discover previously simple tasks that involved these muscles challenging to perform, such as opening a prescription bottle with a lock.[1][7] This syndrome is rare and has a low incidence of only one to five percent of all median nerve neuropathies.[12] Therefore, this syndrome may be challenging to diagnose, and it is often confused clinically with carpal tunnel syndrome. Further diagnostic workup can better elucidate its distinct characteristics and guide treatment.[14]
Electromyography (EMG) and nerve conduction velocity (NCV) studies are typically not necessary for diagnosis but may be used. NCV will show a slowed conduction velocity of the median nerve in the proximal forearm. Magnetic resonance imaging (MRI) is not necessary for diagnosis, but it can be of utility and typically shows atrophy of the muscles innervated by the median nerve in the forearm and abnormally increased signal intensity in the pronator teres on T2-weighted image. Treatment for this condition often involves rest, NSAIDs, and physical therapy focused on stretching. However, a corticosteroid injection into the pronator teres should be considered if this approach fails. The last line of treatment involves surgical decompression.[12]
Strains of the pronator teres are rare, but they have been reported in some athletes. The mechanism of injury typically involves a bat or club striking the ground during a swing. This presents an eccentric force to an elbow in pronation. Due to its rarity, this condition may be confused with other injuries such as medial epicondylitis or injury to the ulnar medial collateral ligament. Patients can present with ecchymoses and tenderness to palpation over the pronator teres. MRI can often assist diagnosis of this injury. Conservative management with rest, NSAIDs, and physical therapy is the mainstay of treatment, and it often yields excellent results.[15][16]
Athletes engaging in forearm pronation as in tennis or golf may be at risk for pronator teres pathology. Insufficiency of the ulnar collateral ligament, flexor-pronator tendinosis, medial epicondylitis, and lateral epicondylitis can be accompanied by injury to the pronator teres.[17] Strengthening the pronator teres is useful in injury prevention and treatment of strains and can be done by using resistance bands. The pronator teres can be targeted by pulling a resistance band laterally with the elbow held in slight flexion, thus engaging the forearm in pronation.[16]
The two muscles responsible for pronation of the forearm (pronator teres and pronator quadratus) are both innervated by the median nerve. Therefore damage to this nerve can result in weakness or even loss of this movement. EMG and NCV can help clinicians pinpoint the exact location of this injury. Possible etiologies for this pathology include direct trauma to the nerve at the elbow or axilla or fracture of the supracondylar humerus.[7]
Media
(Click Image to Enlarge)
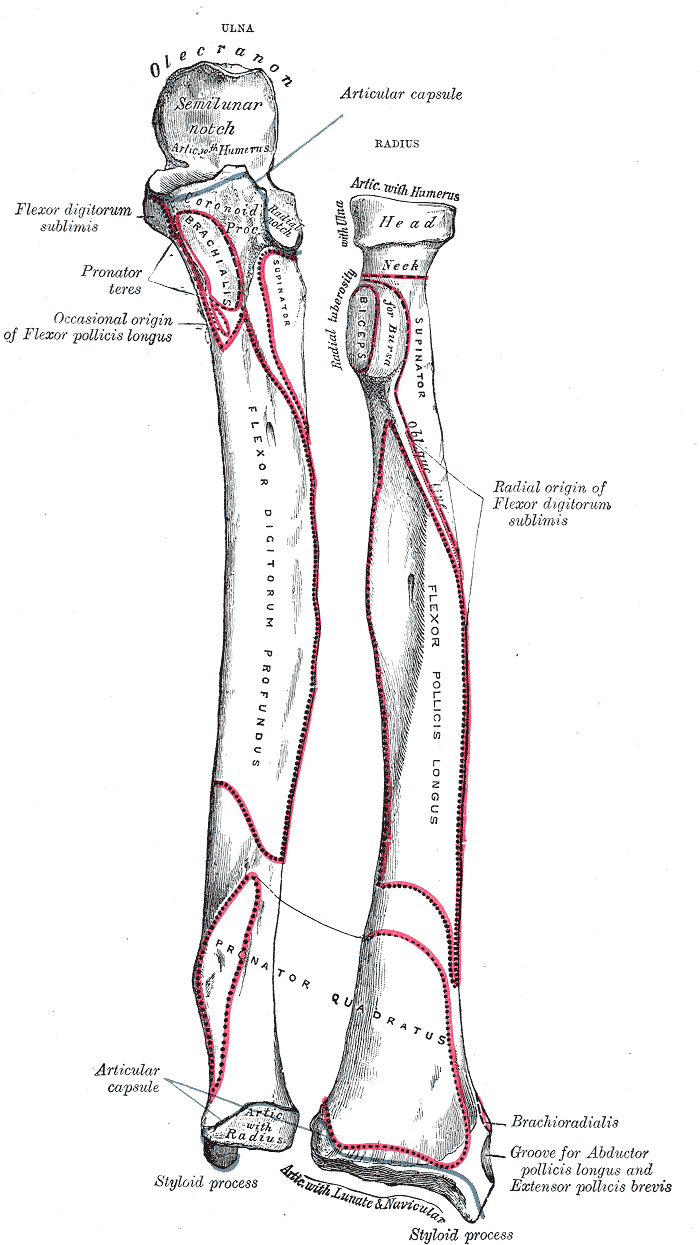
Forearm Bone Markings. Anatomy includes ulna, radius, forearm, articular capsule, olecranon, semilunar notch, flexor digitorum sublimis, flexor, digitorum, pronator teres, brachialis, flexor pollicis longus, pollicis longus, supinator, radial notch, radial tuberosity, biceps, oblique line, flexor digitorum profundus, flexor pollicis longus, radial origin, flexor digitorum sublimis, pronator quadratus, styloid process, brachioradialis, abductor, abductor pollicis longus, and extensor pollicis brevis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
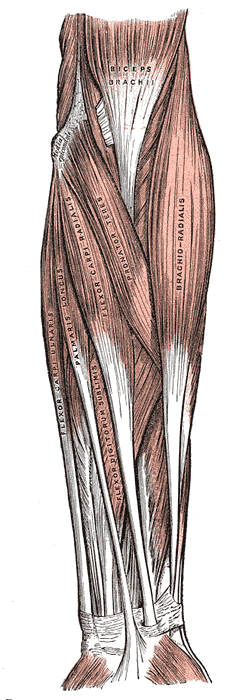
Forearm Muscles. This anterior view shows the biceps brachii, brachioradialis, pronator teres, flexor carpi radialis and ulnaris, palmaris longus, and flexor digitorum sublimis. Other structures in this illustration include the flexor retinaculum (not labeled) and medial epicondyle.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
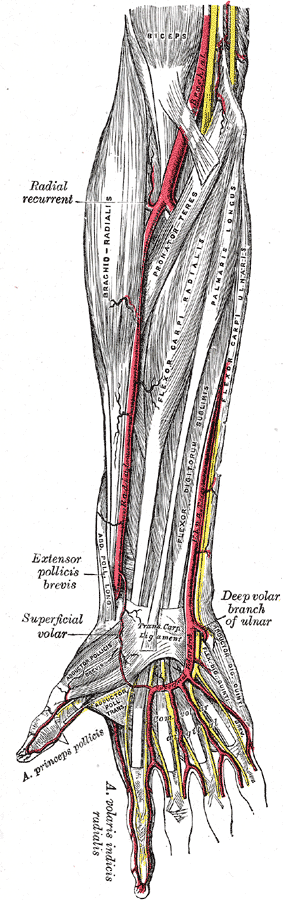
Muscles and Arteries of the right forearm and hand, Biceps, Brachial Artery, Racial recurrent, Brachioradialis, Pronator teres, Flexor carpi radialis, Palmaris longus, Flexor digitorum sublimis, Flexor carpis, Extensor pollicis brevis, Superficial volar, Abductor pollicis brevis, Adductor pollicis transversus, Abductor digiti quinti, Flexor digit quinti brevis, Yellow lines represent nerves.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Dididze M, Tafti D, Sherman AL. Pronator Teres Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 30252346]
Sheen JR, Khan YS. Anatomy, Shoulder and Upper Limb, Cubital Fossa. StatPearls. 2023 Jan:(): [PubMed PMID: 31869138]
Créteur V, Madani A, Brasseur JL. Pronator quadratus imaging. Diagnostic and interventional imaging. 2012 Jan:93(1):22-9. doi: 10.1016/j.diii.2011.10.006. Epub 2011 Dec 13 [PubMed PMID: 22277707]
Prummel KD, Nieuwenhuize S, Mosimann C. The lateral plate mesoderm. Development (Cambridge, England). 2020 Jun 19:147(12):. doi: 10.1242/dev.175059. Epub 2020 Jun 19 [PubMed PMID: 32561665]
Marques E, Bordoni B. Anatomy, Shoulder and Upper Limb, Ulnar Artery. StatPearls. 2023 Jan:(): [PubMed PMID: 31536226]
Marchese RM, Black AC, Geiger Z. Anatomy, Shoulder and Upper Limb, Forearm Radial Artery. StatPearls. 2023 Jan:(): [PubMed PMID: 31536233]
Dydyk AM, Negrete G, Sarwan G, Cascella M. Median Nerve Injury. StatPearls. 2023 Jan:(): [PubMed PMID: 31971749]
Tiwana MS, Charlick M, Varacallo M. Anatomy, Shoulder and Upper Limb, Biceps Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30137823]
Gilan İY, Gilan VB, Öztürk AH. Evaluation of the supinator muscle and deep branch of the radial nerve: impact on nerve compression. Surgical and radiologic anatomy : SRA. 2020 Aug:42(8):927-933. doi: 10.1007/s00276-020-02480-0. Epub 2020 May 4 [PubMed PMID: 32367465]
Nebot-Cegarra J, Perez-Berruezo J, Reina de la Torre F. Variations of the pronator teres muscle: predispositional role to median nerve entrapment. Archives d'anatomie, d'histologie et d'embryologie normales et experimentales. 1991-1992:74():35-45 [PubMed PMID: 1366347]
Lee HJ, Kim I, Hong JT, Kim MS. Early surgical treatment of pronator teres syndrome. Journal of Korean Neurosurgical Society. 2014 May:55(5):296-9. doi: 10.3340/jkns.2014.55.5.296. Epub 2014 May 31 [PubMed PMID: 25132940]
Level 3 (low-level) evidenceBinder H, Zadra A, Popp D, Komjati M, Tiefenboeck TM. Outcome of Surgical Treated Isolated Pronator Teres Syndromes-A Retrospective Cohort Study and Complete Review of the Literature. International journal of environmental research and public health. 2021 Dec 22:19(1):. doi: 10.3390/ijerph19010080. Epub 2021 Dec 22 [PubMed PMID: 35010338]
Level 2 (mid-level) evidenceCiccotti MG, Ramani MN. Medial epicondylitis. Techniques in hand & upper extremity surgery. 2003 Dec:7(4):190-6 [PubMed PMID: 16518220]
Hsiao CW, Shih JT, Hung ST. Concurrent carpal tunnel syndrome and pronator syndrome: A retrospective study of 21 cases. Orthopaedics & traumatology, surgery & research : OTSR. 2017 Feb:103(1):101-103. doi: 10.1016/j.otsr.2016.10.009. Epub 2016 Nov 25 [PubMed PMID: 27894853]
Level 2 (mid-level) evidenceQayyum U, Villacis D, Jobin CM. Pronator Teres Myotendinous Tear. American journal of orthopedics (Belle Mead, N.J.). 2017 Mar/Apr:46(2):E105-E107 [PubMed PMID: 28437501]
Farber AJ, Smith JS, Kvitne RS, Mohr KJ, Shin SS. Electromyographic analysis of forearm muscles in professional and amateur golfers. The American journal of sports medicine. 2009 Feb:37(2):396-401. doi: 10.1177/0363546508325154. Epub 2008 Nov 20 [PubMed PMID: 19022991]
Eygendaal D, Rahussen FT, Diercks RL. Biomechanics of the elbow joint in tennis players and relation to pathology. British journal of sports medicine. 2007 Nov:41(11):820-3 [PubMed PMID: 17638843]