
Introduction
Astigmatism is a common refractive error, where refraction changes in different meridians of the eye.[1] The light rays passing through the eye cannot converge at a particular focal point but form focal lines.[2] In other words, astigmatism is a condition where parallel rays of light passing from the cornea do not converge to a point focus on the retina.[3]
Astigmatism can be regular or irregular. The etiology of astigmatism can be corneal, lenticular, or retinal. Regular astigmatism is divided into with the rule astigmatism, against the rule astigmatism, oblique, and bi-oblique astigmatism. The principle of Sturm's conoid defines the optics of regular astigmatism.
Astigmatism can also be divided into simple, compound, and mixed astigmatism.[4] The common symptoms of astigmatism can be asthenopia, discomfort, blurred and defective vision, elongation of objects, and accommodation problems. The signs include partial lid closure, head tilt, vertically oval or tilted optic disc, and different power in different meridians. The investigations needed include retinoscopy, slit lamp, examination, keratometry, Schiempflug imaging, astigmatic fan, and Jackson cross-cylinder evaluation.[5]
Astigmatism can be managed with spectacles, contact lenses, and surgical correction of astigmatism through refractive surgery, toric IOL implantation, and astigmatic relaxing incisions.[6]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Corneal Astigmatism
- Corneal astigmatism is the most common form of astigmatism and is secondary to abnormal corneal curvature.[7]
Lenticular Astigmatism
- Curvatural lenticular astigmatism is a secondary abnormal curvature of the lens as seen in lenticonus.[8]
- Positional astigmatism is due to tilting or displacement of the lens as in subluxation.[9]
- Index astigmatism is due to the variable refractive index of various meridians.[10]
Retinal Astigmatism
- Retinal astigmatism is due to oblique placement of macula.[11]
With the Rule Astigmatism
- In this, the two principal meridians are right-angled to each other, with the vertical meridian being steeper than the horizontal.[12] This type of astigmatism requires a concave cylinder at 180 ± 20 degrees or a convex cylinder at 90 ± 20. This is called a with the rule astigmatism. The vertical meridian is usually curved 0.25 D more than the horizontal due to the pressure of the eyelids.
Against the Rule Astigmatism
- In this, the horizontal meridian is more curved than the vertical meridian. This will require convex cylindrical correction at 180 ± 20 or a concave cylindrical lens at 90 ± 20.[12]
Oblique Astigmatism
- In this, the two principal meridians are right-angled to each other but not horizontal or vertical (For example, 45 degrees and 135 degrees).[13]
Bioblique Astigmatism
- In this type of astigmatism, the two principal meridians are not at right angles to each other (For example, 20 degrees and 110 degrees).[14]
Simple Astigmatism
- When light rays are focussed in front of the retina in one meridian, it is called simple myopic astigmatism. When they are focussed behind the retina, this is labeled simple hypermetropic astigmatism.[15]
Compound Astigmatism
- When the rays of light in both the meridian are focussed in front of the retina, this is labeled as compound myopic astigmatism, and when they are focussed behind the retina, this is labeled as compound hypermetropic astigmatism.[16]
Mixed Astigmatism
- In this scenario, the light rays in one meridian are focussed in front of the retina, and in other meridians, it is concentrated behind, so one meridian is myopic, and in another, it is hypermetropic; this is called mixed astigmatism.[17]
The most common and important causes of astigmatism are keratoconus, posterior keratoconus, corneal scar, keratoglobus, pellucid marginal degeneration, Dellen, LASIK, photorefractive keratectomy, pterygium, rheumatic ulcer, shield ulcer, Mooren ulcer, microbial keratitis, herpetic keratitis, band-shaped keratopathy, vortex keratopathy, corneal edema, basement membrane dystrophy, lattice dystrophy, contact lens wear, contact lens warpage, post keratoplasty astigmatism, suture induced astigmatism, ptosis, cataract wound-related, radial keratotomy, trabeculectomy, glaucoma shunt procedure, penetrating injury, foreign body, chalazion, tumor, and capillary haemangioma.[18]
Epidemiology
Astigmatism typically changes with age. In early childhood, from 0 to 4 years of age, the cornea is steep, there is a high degree of corneal astigmatism, and the most common axis is against the rule astigmatism. In the age group aged 4 to 18 years, the cornea flattens, astigmatism reduces, and small degrees of with the rule astigmatism is common. From 18 to 40 years, the cornea remains stable, and a small degree of with the rule astigmatism is common. From 40 years onwards, the cornea again steepens, and there is a shift in corneal astigmatism toward against the rule.[19]
Further, astigmatism varies amongst different ethnic groups. An increased prevalence of with the rule astigmatism has been noted among Native Americans.[20] Harvey, Dobson, and Miller reported astigmatism of 1.00D or more among 42% of school children.[21] Poor nutrition has been postulated as a cause of reduced corneal rigidity.[20]
As a result of this, the pressure from the upper eyelid steepens the vertical cornea and flattens the horizontal cornea. Increased rates of change in astigmatism have been reported among Asian subjects. The tightness of the Asian eyelids and narrow palpebral fissures have been suggested as causes of the greater rates of astigmatism change. Kleisnstein et al. reported the prevalence of one or more diopters among 33.6% of Asian and 36.9% of Hispanic children.
A study from Brazil reported the prevalence of myopia to be 2.7%, with a high prevalence of astigmatism of 16% (1 D astigmatism). They found a predominance of against the rule astigmatism.[22] In another study by Fuller et al., a high incidence of WTR astigmatism was seen in a small population subgroup of Bangladeshi children residing in East London.[23]
Pathophysiology
In regular astigmatism, the parallel light rays are not focused on a particular point, but rather two focal lines are formed. The configuration of rays refracted through the toric surface is labeled as Sturm's conoid, and the distance between the lines is called the focal interval of Sturm.[24] A higher degree of astigmatism is noted in infants and neonates. The astigmatism degree is even higher in preterm newborns, and an inverse co-relation is noted with postconceptional age and birth weight.[25]
Approximately 40 percent of newborns have approximately 1 D astigmatism since birth, and it is reduced to adult level by one year of age due to normal eye maturation and globe remodeling.[26] It has been proposed that high astigmatism in early life induces and stimulates accommodation. The magnitude and axis of astigmatism can vary during the day, and the variation can be due to eyelid pressure, extraocular muscle tension, change in pupil size, and accommodation.[27]
The palpebral fissure slant affects the corneal toricity, which in turn changes astigmatism. Patients with Down syndrome and Treacher Collins syndrome show oblique astigmatism due to upward or downward slant of the palpebral fissure. Corneal rigidity also affects astigmatism caused by eyelid pressure.[28]
Patients with nutritional deficiencies affect the horizontal meridian while steepening the vertical one. The pupil size also affects astigmatism. Larger pupil size is correlated with high cylindrical power and with the rule astigmatism.[29]
Larger pupil size is linked with higher-order aberrations like coma and may increase the cylindrical power in manifest refraction. Coma is linked with a higher amount of astigmatism. Tear film changes also affect the cornea and result in astigmatism.[30]
History and Physical
Patients with astigmatism usually present with asthenopic symptoms like headache, pain, heaviness in the eyes, frontal headache, difficulty focusing, transient blurring, drowsiness, and even nausea. The patient has also presented with blurred vision, diminution of vision, and elongation of objects with the degree of astigmatism.[31]
The patient also put objects close to the eyes while reading. History of trauma, surgical intervention, keratoconus, terrain marginal degeneration, pellucid marginal degeneration, pterygium, pinguecula, ocular surface squamous neoplasia, mass excision, limbal dermoid should be documented.[32]
Detailed torch light and slit-lamp examination should be performed to rule out lid closure, head tilt, keratoconus signs, corneal scar, lid mass, lid abnormality, dry eyes, or any other condition producing astigmatism.[32]
The lens should be carefully examined for nuclear sclerotic changes, subluxation, dislocation, microspherophakia, and traumatic cataracts. Dilated fundoscopy should be performed to rule out the oval or tilted optic disc and oblique placement of the macula.[33]
Evaluation
Visual Acuity
- Visual acuity should be evaluated with the help of Snellen's chart or E- chart, and uncorrected, best-corrected, and pinhole visual acuity should be documented.[34]
Retinoscopy and Refraction
- The retinoscopy evaluates the axis and magnitude of astigmatism, neutralization of refractive correction, and type of reflexes like a dull reflex, no reflex, or scissor reflex as in keratoconus. It also reveals different power on two different axes.[35]
Keratometry
- Keratometry and computerized topography will reveal different corneal curvatures on two different axes.[36]
Pachymetry
- This will help assess the cornea's thickness and help decide on refractive surgery.[37]
Astigmatic Fan Test and Jackson Cross Cylinder
- These tests help confirm the axis and power of the cylinder.[38]
Treatment / Management
Optical
In regular astigmatism, the regular treatment consists of prescribing spectacles with cylindrical lenses discovered after correct refraction. Hard contact lenses are another option for correcting astigmatism, which can correct up to 2-3 dioptre of astigmatism. For astigmatism higher than this, toric contact lenses are another option.[39]
Guidelines for Astigmatism Correction
Small Degree of Astigmatism
Minimal astigmatism up to 0.5 D should be corrected only if there are asthenopic symptoms or producing any symptoms. A low degree of astigmatism should be rectified with meticulous refraction, and care is crucial while prescribing the changes.[40]
High Degree of Astigmatism
The higher degree of astigmatism should be corrected fully to minimize asthenopic symptoms. The patients with a high cylindrical correction may not be happy with full cylindrical correction initially and may not accept it; hence the correction should be titrated till the patient is comfortable. These patients should have serial follow-ups, and serial adjustments should be made till full correction is accepted.[41]
Correction of Axis of Astigmatism
If the patient is not happy with cylindrical correction, the axis of astigmatism can be rechecked, considering the old axis of refraction. The patient with new correction should be told to wear new correction and walk for a few minutes till he is comfortable.[42]
New Astigmatic Correction
New correction should be avoided as it may result in intolerable symptoms, even if there is improvement in the best-corrected visual acuity. If there is a significant change, the patient should be ascertained that there is an improvement in visual acuity, and the new correction adjustment will take time.
Oblique Astigmatism, Mixed Astigmatism, and High Astigmatism are better treated with contact lenses than spectacles.[41]
Surgical Management of Astigmatism
Toric IOL Implantation
The corneal astigmatism present and cataractous changes in a patient can be managed with toric IOL implantation.[43]
Refractive Incisional Procedures
Astigmatic Keratotomy
Astigmatic Keratotomy (AK) is a technique of performing arcuate cuts or arcuate cuts in the mid-peripheral cornea, which is perpendicular to the steepest corneal meridian. The AK can be done alone for astigmatism correction or can be coupled with cataract surgery.[44]
Mechanism
In AK, the incised meridian flattens while the meridian 90 degrees away steepens by an equal amount. This technique can correct up to 4 to 6 D of astigmatism. The deeper, longer, and more central the incision is, the more the effect, but this may result in more irregular astigmatism, micro-perforations, and overcorrection.[45]
Technique
The incision length is usually 5 to 7 mm from the pupillary center. Nomograms are there to adjust for patient age and amount of astigmatism. AK can be done using transverse and arcuate incisions.[44]
Transverse Incisions
These incisions are fashioned in pairs in the steepest meridian and extend to 3 mm. The second pair of incisions are often required at the same meridian for a more significant effect. Transverse incisions are given tangential to the optic zone; hence, the flattening power decreases as the incision size increases.[46]
Arcuate Incision
The arcuate clear corneal incisions are at a particular distance from the center and are more effective than transverse cuts at a given optical zone size. The flattening effect increases with the length of the incision up to 90 degrees.[47](B3)
Limbal Relaxing Incision
Limbal relaxing incision (LRI) is an incision used to correct mild astigmatism (-1 D to -2D). The main advantage is that the procedure produces less glare and discomfort than AK. The incisions heal faster, and the corneal optical quality is preserved by making incisions at the limbus. The incisions are safe and can be easily coupled with cataract surgery.[48]
Laser Ablation Corneal Refractive Surgeries
Photoastigmatic Refractive Keratotomy
This technique uses a cylindrical ablation pattern in contrast to a spherical pattern. The axis of astigmatism should be marked while the patient is sitting because the position may shift as the patient lies down. In cases with compound myopic astigmatism, elliptical PRK should be performed, which may correct myopic and astigmatic correction.[49]
Astigmatic Epi-LASIK
Astigmatic LASIK is the preferred modality over PRK as it reduces pain and postoperative haze.[50]
Astigmatic LASIK
Like PRK, the LASIK procedure can be used to correct astigmatism. An astigmatic LASIK can correct up to 0.5-10 D of astigmatism.[51](B3)
C-LASIK
Wavefront-guided customized is presently the best modality to correct corneal astigmatism.[52]
Post-Keratoplasty Astigmatism Management
Suture Induced Astigmatism
Suture-induced astigmatism after keratoplasty can be managed by selective suture removal in steeper meridian and improved irregular and regular to a varying degree. Interrupted suture removal may be performed within three months, depending on the amount of astigmatism. Continuous suture removal should be attempted after one year of surgery. The selective suture removal can be guided by Scheimpflug imaging or keratoscopy.[53]
Relaxing Incision
Arcuate incisions along the steepest meridian in the donor area 0.5 mm central to the graft-host junction can correct astigmatism up to 3.5 to 8.5 D. The relaxing incisions are placed under topical anesthesia with the help of a razor blade or bearer blade, or a diamond knife. Two relaxing incisions up to 60-70% of the corneal depth are made up to 180 degrees apart, and the incision may extend up to 60-100 degrees.[54](A1)
Astigmatic LASIK
LASIK procedure can correct astigmatism up to 6-8 D. Wavefront-guided C-LASIK is the best technique to correct post keratoplasty astigmatism.[51](B3)
Relaxing Incisions and Compression Sutures
This technique can correct astigmatism up to 8.5 to 16 D astigmatism. After the relaxing incision, 2-3 10-0 nylon sutures are applied at the graft host junction, which is 90 degrees from the steepest meridian on each side.[54](A1)
Corneal Wedge Resection
This procedure can correct astigmatism up to 10 to 20 D before performing optical keratoplasty. Under peribulbar block, a corneal wedge of 1 to 1.5 mm wide base and 90 degrees is removed from the recipient cornea adjacent to the graft host junction in the flattest meridian. The defect created can be sutured with nylon sutures. The sutures are tightened enough to overcome one-third of existing astigmatism.[55]
Ruiz Procedure
This procedure can correct astigmatism up to 10 D astigmatism. A deep horizontal keratotomy incision is made with a guarded diamond blade in a step ladder fashion along with the steepest corneal meridian. The horizontal incisions are assisted by two adjacent radial incisional. The critical thing to be monitored is that the two incisions do not intersect as it may result in poor wound healing and gaping.[56](B2)
Repeat Optical Keratoplasty
Repeat optical keratoplasty is needed in a patient with more than 20 D of astigmatism.[57]
Differential Diagnosis
- Myopia
- Hypermetropia
- Presbyopia
Prognosis
The prognosis of cases with astigmatism is usually good if treated on time, as there are multiple options available to correct astigmatism. Untreated patients, especially during childhood, may result in a permanent reduction in visual acuity and amblyopia.[58]
Astigmatism is subject to change with time and will require new glasses and contact lenses. Refractive correction can often eliminate or reduce astigmatism in most cases. Patients with keratoconus can develop loss of visual acuity due to high astigmatism; hence timely and regular screening is mandated.[59]
Complications
- Defective vision
- Distorted vision
- Amblyopia
- Polyopia
- Strabismus
- Contact lens-induced infective keratitis[60]
Postoperative and Rehabilitation Care
Patients undergoing surgical correction for astigmatism should be prescribed postoperative eye drops as per the regimen.[61] In PRK, topical steroids and antibiotic combination (0.5% moxifloxacin and 0.25 loteprednol) are given 4/3/2/1 times for 15 days each, and topical lubricants like 0.5% Carboxymethylcellulose for three months.[62]
In LASIK, the same steroid and antibiotic regimen is offered four times weekly, and lubricants are continued for three months. Astigmatism management with cataract surgery is the same as post-cataract surgery topical drug regimen.[63]
Patients have been prescribed steroid and antibiotic combinations such as 0.5 % gatifloxacin and 0.1% dexamethasone in the dose of 6/5/4/3/2/1 for one week each and plain topical antibiotics such as 0.5% gatifloxacin or moxifloxacin for four times per day for 15 days. The patient should be counseled regarding the importance of using medications and regular follow-up.[64]
Consultations
The most crucial thing in the case of astigmatism is to pinpoint the etiology. The cases with corneal astigmatism should be referred to a cornea and external disease specialist for the best possible management. Patients requiring cataract surgery and astigmatism management should be directed to a surgeon who manages cataracts and IOL.[65]
Deterrence and Patient Education
The patient should be explained that astigmatism is a type of refractive error and should be managed promptly.[66] The patients must be educated that few basic investigations are required to pinpoint the etiology of astigmatism and, if not treated on time, may result in loss of visual acuity and amblyopia in children.[67]
The patient should also be educated regarding the importance of family screening in patients with astigmatism and keratoconus patients.[68] The patient should also be informed that in some cases, astigmatism management will require surgical intervention, and there can be residual astigmatism in very few cases.[65]
Pearls and Other Issues
Apart from the causes listed above for astigmatism, the exact cause of spontaneous astigmatism is not clearly understood. Recent research indicates that genetic factors play an essential role in the development of astigmatism.[69]
Other factors contributing to astigmatism include pressure from the lids, extraocular muscle tension, and visual feedback. The likely interaction between eyelid and cornea is a logical explanation for increased astigmatism between various groups. In children also, eyelid pressure influences the axis and degree of astigmatism. With the growing improvement of technology, the ability to measure and define ocular astigmatism has improved.[70]
Enhancing Healthcare Team Outcomes
Prompt diagnosis and meticulous management of astigmatism depend on interprofessional communication between the ophthalmologist, other clinicians, and the paramedical staff.[71] The etiology of astigmatism should be labeled, and family screening should be performed as a routine. The optometrists, nursing staff, allied health specialists, ophthalmologists, and paramedical staff have an essential role in determining the patients' final outcome. The patient's family clinician should also be kept informed regarding the underlying conditions that led to astigmatism, as well as any surgical interventions, as it may impact other care in some instances. This interprofessional communication is crucial to going optimal patient outcomes.[70]
Media
(Click Image to Enlarge)
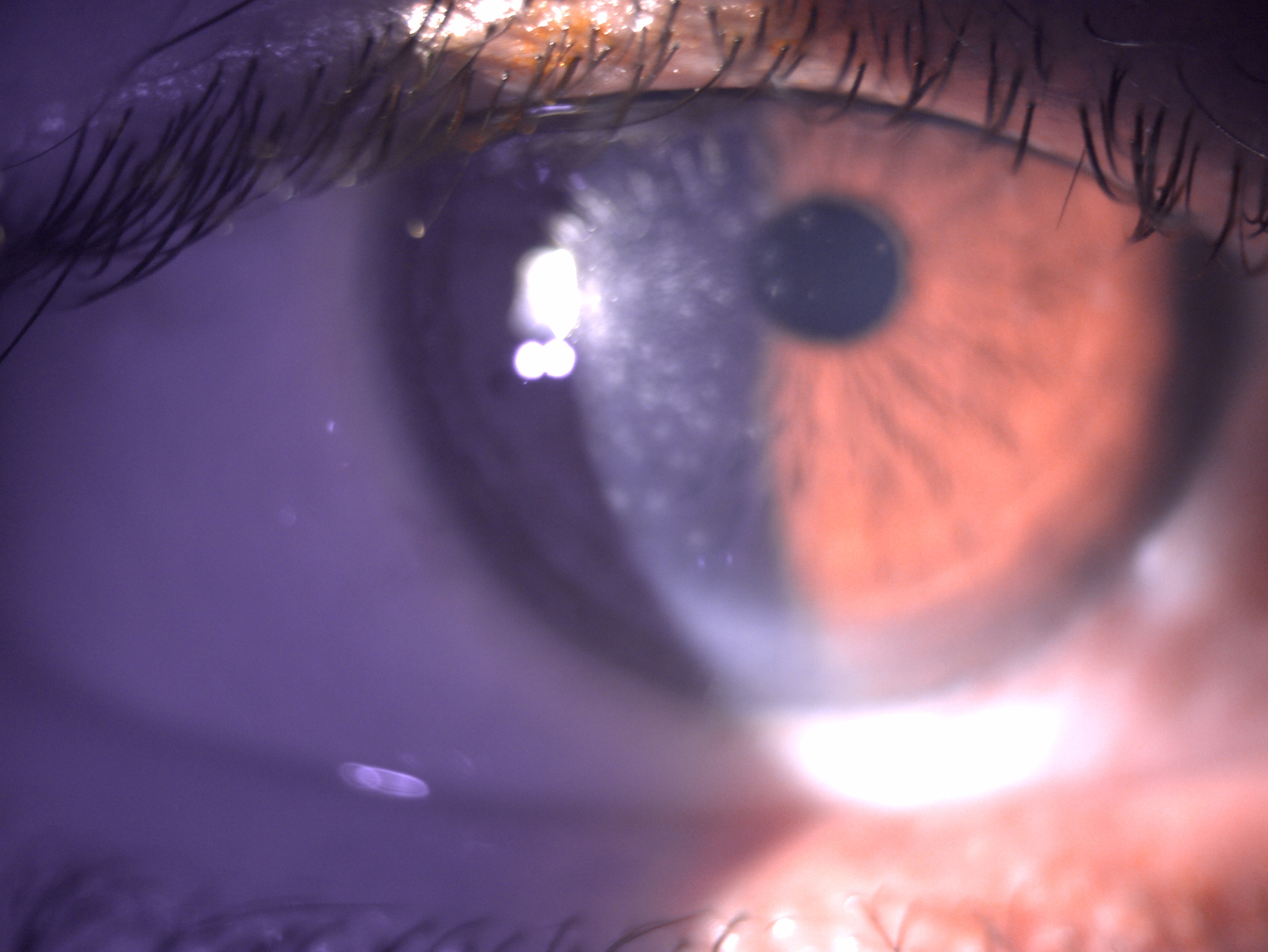
Digital image depicting multiple subepithelial scars post viral keratitis causing astigmatism Contributed by Dr Bharat Gurnani, MBBS, DNB, FCRS, FICO, MRCS Ed, MNAMS
References
Schiefer U, Kraus C, Baumbach P, Ungewiß J, Michels R. Refractive errors. Deutsches Arzteblatt international. 2016 Oct 14:113(41):693-702. doi: 10.3238/arztebl.2016.0693. Epub [PubMed PMID: 27839543]
Sutter E, Foster A, Francis V. Optics & refraction. Community eye health. 2000:13(33):8 [PubMed PMID: 17491945]
Wajuihian SO. Characteristics of astigmatism in Black South African high school children. African health sciences. 2017 Dec:17(4):1160-1171. doi: 10.4314/ahs.v17i4.25. Epub [PubMed PMID: 29937888]
Ueno Y, Nomura R, Hiraoka T, Kinoshita K, Ohara M, Oshika T. Comparison of corneal irregular astigmatism by the type of corneal regular astigmatism. Scientific reports. 2021 Aug 4:11(1):15769. doi: 10.1038/s41598-021-95358-z. Epub 2021 Aug 4 [PubMed PMID: 34349218]
Dhungel D, Shrestha GS. Visual symptoms associated with refractive errors among Thangka artists of Kathmandu valley. BMC ophthalmology. 2017 Dec 21:17(1):258. doi: 10.1186/s12886-017-0659-0. Epub 2017 Dec 21 [PubMed PMID: 29268725]
Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric Intraocular Lenses in the Correction of Astigmatism During Cataract Surgery: A Systematic Review and Meta-analysis. Ophthalmology. 2016 Feb:123(2):275-286. doi: 10.1016/j.ophtha.2015.10.002. Epub 2015 Nov 18 [PubMed PMID: 26601819]
Level 1 (high-level) evidenceMohammadi SF, Khorrami-Nejad M, Hamidirad M. Posterior corneal astigmatism: a review article. Clinical optometry. 2019:11():85-96. doi: 10.2147/OPTO.S210721. Epub 2019 Aug 12 [PubMed PMID: 31496856]
Bamotra RK, Meenakshi, Kesarwani PC, Qayum S. Simultaneous Bilateral Anterior and Posterior Lenticonus in Alport Syndrome. Journal of clinical and diagnostic research : JCDR. 2017 Aug:11(8):ND01-ND02. doi: 10.7860/JCDR/2017/25521.10369. Epub 2017 Aug 1 [PubMed PMID: 28969174]
Lakshminarayanan V, Enoch JM, Raasch T, Crawford B, Nygaard RW. Refractive changes induced by intraocular lens tilt and longitudinal displacement. Archives of ophthalmology (Chicago, Ill. : 1960). 1986 Jan:104(1):90-2 [PubMed PMID: 3484627]
Kaye SB. Objective evaluation of refractive data and astigmatism: quantification and analysis. Eye (London, England). 2014 Feb:28(2):154-61. doi: 10.1038/eye.2013.266. Epub 2013 Dec 13 [PubMed PMID: 24336294]
Davitt BV, Dobson V, Quinn GE, Hardy RJ, Tung B, Good WV, Early Treatment for Retinopathy of Prematurity Cooperative Group. Astigmatism in the Early Treatment for Retinopathy Of Prematurity Study: findings to 3 years of age. Ophthalmology. 2009 Feb:116(2):332-9. doi: 10.1016/j.ophtha.2008.09.035. Epub 2008 Dec 16 [PubMed PMID: 19091409]
Level 1 (high-level) evidenceRefai TA. Evaluation of the orientation of the steepest meridian of regular astigmatism among highly myopic Egyptian patients seeking non-ablative surgical correction of the refractive error. Electronic physician. 2015 Sep:7(5):1296-300. doi: 10.14661/1296. Epub 2015 Sep 16 [PubMed PMID: 26435831]
Shen J, Spors F, Egan D, Liu C. Peripheral refraction and image blur in four meridians in emmetropes and myopes. Clinical ophthalmology (Auckland, N.Z.). 2018:12():345-358. doi: 10.2147/OPTH.S151288. Epub 2018 Feb 19 [PubMed PMID: 29497275]
Remón L, Monsoriu JA, Furlan WD. Influence of different types of astigmatism on visual acuity. Journal of optometry. 2017 Jul-Sep:10(3):141-148. doi: 10.1016/j.optom.2016.07.003. Epub 2016 Sep 14 [PubMed PMID: 27639497]
Remón L, Tornel M, Furlan WD. Visual acuity in simple myopic astigmatism: influence of cylinder axis. Optometry and vision science : official publication of the American Academy of Optometry. 2006 May:83(5):311-5 [PubMed PMID: 16699444]
Parrey MUR, Elmorsy E. Prevalence and pattern of refractive errors among Saudi adults. Pakistan journal of medical sciences. 2019 Mar-Apr:35(2):394-398. doi: 10.12669/pjms.35.2.648. Epub [PubMed PMID: 31086521]
Xu G, Xu B, Zhou J. [A clinical report on mixed astigmatism]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 1996 Mar:32(2):126-9 [PubMed PMID: 9206230]
Grosvenor T, Etiology of astigmatism. American journal of optometry and physiological optics. 1978 Mar; [PubMed PMID: 677264]
Chen J, Jing Q, Tang Y, Qian D, Lu Y, Jiang Y. Age Differences in Axial Length, Corneal Curvature, and Corneal Astigmatism in Marfan Syndrome with Ectopia Lentis. Journal of ophthalmology. 2018:2018():1436834. doi: 10.1155/2018/1436834. Epub 2018 May 2 [PubMed PMID: 29854424]
Level 2 (mid-level) evidenceLyle WM, Grosvenor T, Dean KC. Corneal astigmatism in Amerind children. American journal of optometry and archives of American Academy of Optometry. 1972 Jun:49(6):517-24 [PubMed PMID: 4504449]
Harvey EM, Dobson V, Miller JM. Prevalence of high astigmatism, eyeglass wear, and poor visual acuity among Native American grade school children. Optometry and vision science : official publication of the American Academy of Optometry. 2006 Apr:83(4):206-12 [PubMed PMID: 16614575]
Level 2 (mid-level) evidenceThorn F, Cruz AA, Machado AJ, Carvalho RA. Refractive status of indigenous people in the northwestern Amazon region of Brazil. Optometry and vision science : official publication of the American Academy of Optometry. 2005 Apr:82(4):267-72 [PubMed PMID: 15829854]
Fuller JR, Baxter LA, Harun S, Levy IS. Astigmatism in Bangladeshi and white school entrants in East London: a prospective comparative study. Eye (London, England). 1995:9 ( Pt 6)():794-6 [PubMed PMID: 8849551]
Level 2 (mid-level) evidenceGlegg N. FOGGING FOR THE FOCAL INTERVAL OF STURM. The British journal of ophthalmology. 1934 May:18(5):264-6 [PubMed PMID: 18169199]
Varghese RM, Sreenivas V, Puliyel JM, Varughese S. Refractive status at birth: its relation to newborn physical parameters at birth and gestational age. PloS one. 2009:4(2):e4469. doi: 10.1371/journal.pone.0004469. Epub 2009 Feb 13 [PubMed PMID: 19214228]
Semeraro F, Forbice E, Nascimbeni G, Cillino S, Bonfiglio VME, Filippelli ME, Bartollino S, Costagliola C. Ocular Refraction at Birth and Its Development During the First Year of Life in a Large Cohort of Babies in a Single Center in Northern Italy. Frontiers in pediatrics. 2019:7():539. doi: 10.3389/fped.2019.00539. Epub 2020 Jan 29 [PubMed PMID: 32083036]
Chu CH, Kee CS. Effects of optically imposed astigmatism on early eye growth in chicks. PloS one. 2015:10(2):e0117729. doi: 10.1371/journal.pone.0117729. Epub 2015 Feb 12 [PubMed PMID: 25675443]
Level 3 (low-level) evidenceGarcia ML, Huang D, Crowe S, Traboulsi EI. Relationship between the axis and degree of high astigmatism and obliquity of palpebral fissure. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2003 Feb:7(1):14-22 [PubMed PMID: 12690364]
Level 2 (mid-level) evidenceWang LL, Wang W, Han XT, He MG. Influence of severity and types of astigmatism on visual acuity in school-aged children in southern China. International journal of ophthalmology. 2018:11(8):1377-1383. doi: 10.18240/ijo.2018.08.20. Epub 2018 Aug 18 [PubMed PMID: 30140644]
Wang Y, Zhao K, Jin Y, Niu Y, Zuo T. Changes of higher order aberration with various pupil sizes in the myopic eye. Journal of refractive surgery (Thorofare, N.J. : 1995). 2003 Mar-Apr:19(2 Suppl):S270-4 [PubMed PMID: 12699188]
Chen Z, Liu L, Pan C, Li X, Pan L, Lan W, Yang Z. Ocular residual and corneal astigmatism in a clinical population of high school students. PloS one. 2018:13(4):e0194513. doi: 10.1371/journal.pone.0194513. Epub 2018 Apr 9 [PubMed PMID: 29630629]
Morlet N, Minassian D, Dart J. Astigmatism and the analysis of its surgical correction. The British journal of ophthalmology. 2001 Sep:85(9):1127-38 [PubMed PMID: 11520769]
Amedo AO, Amoah K, Koomson NY, Ben Kumah D, Osae EA. Assessment of corneal astigmatism following frown and straight incision forms in sutureless manual small incision cataract surgery. Clinical optometry. 2016:8():47-52. doi: 10.2147/OPTO.S98920. Epub 2016 Apr 22 [PubMed PMID: 30214348]
Hennelly ML. How to detect myopia in the eye clinic. Community eye health. 2019:32(105):15-16 [PubMed PMID: 31409949]
Cordero I. Understanding and looking after a retinoscope and trial lens set. Community eye health. 2017:30(98):40-41 [PubMed PMID: 29070929]
Level 3 (low-level) evidenceTay E, Mengher L, Lin XY, Ferguson V. The impact of off the visual axis retinoscopy on objective central refractive measurement in adult clinical practice: a prospective, randomized clinical study. Eye (London, England). 2011 Jul:25(7):888-92. doi: 10.1038/eye.2011.79. Epub 2011 Apr 15 [PubMed PMID: 21494285]
Level 1 (high-level) evidenceKohnen T, Strenger A, Klaproth OK. Basic knowledge of refractive surgery: correction of refractive errors using modern surgical procedures. Deutsches Arzteblatt international. 2008 Feb:105(9):163-70; quiz 170-2. doi: 10.3238/arztebl.2008.0163. Epub 2008 Feb 29 [PubMed PMID: 19633786]
Del Priore LV, Guyton DL. The Jackson cross cylinder. A reappraisal. Ophthalmology. 1986 Nov:93(11):1461-5 [PubMed PMID: 3808608]
Mohammad-Rabei H, Mohammad-Rabei E, Espandar G, Javadi MA, Jafarinasab MR, Hashemian SJ, Feizi S. Three Methods for Correction of Astigmatism during Phacoemulsification. Journal of ophthalmic & vision research. 2016 Apr-Jun:11(2):162-7. doi: 10.4103/2008-322X.183924. Epub [PubMed PMID: 27413496]
Villegas EA, Alcón E, Artal P. Minimum amount of astigmatism that should be corrected. Journal of cataract and refractive surgery. 2014 Jan:40(1):13-9. doi: 10.1016/j.jcrs.2013.09.010. Epub [PubMed PMID: 24355718]
Sha J, Fedtke C, Tilia D, Yeotikar N, Jong M, Diec J, Thomas V, Bakaraju RC. Effect of cylinder power and axis changes on vision in astigmatic participants. Clinical optometry. 2019:11():27-38. doi: 10.2147/OPTO.S190120. Epub 2019 Mar 19 [PubMed PMID: 30936760]
Elliott DB, Black AA, Wood JM. Subjective Verticality Is Disrupted by Astigmatic Visual Distortion in Older People. Investigative ophthalmology & visual science. 2020 Apr 9:61(4):12. doi: 10.1167/iovs.61.4.12. Epub [PubMed PMID: 32293665]
Kaur M, Shaikh F, Falera R, Titiyal JS. Optimizing outcomes with toric intraocular lenses. Indian journal of ophthalmology. 2017 Dec:65(12):1301-1313. doi: 10.4103/ijo.IJO_810_17. Epub [PubMed PMID: 29208810]
Hiep NX, Khanh PTM, Quyet D, Thai TV, Nga VT, Dinh TC, Bac ND. Correcting Corneal Astigmatism with Corneal Arcuate Incisions during Femtosecond Laser Assisted Cataract Surgery. Open access Macedonian journal of medical sciences. 2019 Dec 30:7(24):4260-4265. doi: 10.3889/oamjms.2019.371. Epub 2019 Dec 20 [PubMed PMID: 32215074]
Monaco G, Scialdone A. Long-term outcomes of limbal relaxing incisions during cataract surgery: aberrometric analysis. Clinical ophthalmology (Auckland, N.Z.). 2015:9():1581-7. doi: 10.2147/OPTH.S89024. Epub 2015 Aug 31 [PubMed PMID: 26357459]
Song W, Chen X, Wang W. Effect of steep meridian clear corneal incisions in phacoemulsification. European journal of ophthalmology. 2015 Sep-Oct:25(5):422-5. doi: 10.5301/ejo.5000575. Epub 2015 Feb 6 [PubMed PMID: 25655599]
Thornton SP. Inverse arcuate incision: a new approach to the correction of astigmatism. Journal of refractive and corneal surgery. 1994 Jan-Feb:10(1):27-30 [PubMed PMID: 7517776]
Level 3 (low-level) evidenceAristeidou A, Taniguchi EV, Tsatsos M, Muller R, McAlinden C, Pineda R, Paschalis EI. The evolution of corneal and refractive surgery with the femtosecond laser. Eye and vision (London, England). 2015:2():12. doi: 10.1186/s40662-015-0022-6. Epub 2015 Jul 14 [PubMed PMID: 26605365]
Christiansen SM, Mifflin MD, Edmonds JN, Simpson RG, Moshirfar M. Astigmatism induced by conventional spherical ablation after PRK and LASIK in myopia with astigmatism { 1.00 D. Clinical ophthalmology (Auckland, N.Z.). 2012:6():2109-17. doi: 10.2147/OPTH.S37489. Epub 2012 Dec 20 [PubMed PMID: 23277735]
Pallikaris IG, Kalyvianaki MI, Katsanevaki VJ, Ginis HS. Epi-LASIK: preliminary clinical results of an alternative surface ablation procedure. Journal of cataract and refractive surgery. 2005 May:31(5):879-85 [PubMed PMID: 15975451]
Wu HK. Astigmatism and LASIK. Current opinion in ophthalmology. 2002 Aug:13(4):250-5 [PubMed PMID: 12165710]
Level 3 (low-level) evidenceSubbaram MV, MacRae S, Slade SG, Durrie DS. Customized LASIK treatment for myopia: relationship between preoperative higher order aberrations and refractive outcome. Journal of refractive surgery (Thorofare, N.J. : 1995). 2006 Oct:22(8):746-53 [PubMed PMID: 17061711]
Fares U, Mokashi AA, Elalfy MS, Dua HS. Sequential selective same-day suture removal in the management of post-keratoplasty astigmatism. Eye (London, England). 2013 Sep:27(9):1032-7. doi: 10.1038/eye.2013.126. Epub 2013 Jun 7 [PubMed PMID: 23743526]
Ho Wang Yin G, Hoffart L. Post-keratoplasty astigmatism management by relaxing incisions: a systematic review. Eye and vision (London, England). 2017:4():29. doi: 10.1186/s40662-017-0093-7. Epub 2017 Dec 6 [PubMed PMID: 29238735]
Level 1 (high-level) evidenceFeizi S, Zare M. Current approaches for management of postpenetrating keratoplasty astigmatism. Journal of ophthalmology. 2011:2011():708736. doi: 10.1155/2011/708736. Epub 2011 Jul 27 [PubMed PMID: 21811668]
Zuberbuhler B, Agrawal A, Gale R, Kipioti T, Gauba V, Noble B. Modified Ruiz procedure for reducing high astigmatism after penetrating keratoplasty. Cornea. 2007 Dec:26(10):1171-7 [PubMed PMID: 18043170]
Level 2 (mid-level) evidenceChaurasiya SK, Reddy JC, Vaddavalli PK, Rapuano CJ. Changes in post-keratoplasty astigmatism after suture removal: refraction vs tomography vs aberrometry. International journal of ophthalmology. 2021:14(11):1707-1713. doi: 10.18240/ijo.2021.11.09. Epub 2021 Nov 18 [PubMed PMID: 34804860]
de Zárate BR, Tejedor J. Current concepts in the management of amblyopia. Clinical ophthalmology (Auckland, N.Z.). 2007 Dec:1(4):403-14 [PubMed PMID: 19668517]
Harvey EM. Development and treatment of astigmatism-related amblyopia. Optometry and vision science : official publication of the American Academy of Optometry. 2009 Jun:86(6):634-9. doi: 10.1097/OPX.0b013e3181a6165f. Epub [PubMed PMID: 19430327]
Zimmerman AB, Nixon AD, Rueff EM. Contact lens associated microbial keratitis: practical considerations for the optometrist. Clinical optometry. 2016:8():1-12. doi: 10.2147/OPTO.S66424. Epub 2016 Jan 29 [PubMed PMID: 30214344]
Swampillai AJ, Khanan Kaabneh A, Habib NE, Hamer C, Buckhurst PJ. Efficacy of toric intraocular lens implantation with high corneal astigmatism within the United Kingdom's National Health Service. Eye (London, England). 2020 Jun:34(6):1142-1148. doi: 10.1038/s41433-019-0744-0. Epub 2019 Dec 16 [PubMed PMID: 31844167]
Karimian F, Faramarzi A, Fekri S, Mohammad-Rabie H, Najdi D, Doozandeh A, Delfaza-Baher S, Yaseri M. Comparison of Loteprednol with Fluorometholone after Myopic Photorefractive Keratectomy. Journal of ophthalmic & vision research. 2017 Jan-Mar:12(1):11-16. doi: 10.4103/2008-322X.200161. Epub [PubMed PMID: 28299001]
Campos M, Muccioli C, Malta JB, Gerade RA, LA Salame A, Belfort R. Efficacy and tolerability of a combined gatifloxacin plus prednisolone formulation for topical prophylaxis after LASIK. Clinical ophthalmology (Auckland, N.Z.). 2011:5():209-14. doi: 10.2147/OPTH.S17059. Epub 2011 Feb 15 [PubMed PMID: 21386913]
Solomon KD, Sandoval HP, Potvin R. Comparing Combination Drop Therapy to a Standard Drop Regimen After Routine Cataract Surgery. Clinical ophthalmology (Auckland, N.Z.). 2020:14():1959-1965. doi: 10.2147/OPTH.S260926. Epub 2020 Jul 10 [PubMed PMID: 32764861]
Núñez MX, Henriquez MA, Escaf LJ, Ventura BV, Srur M, Newball L, Espaillat A, Centurion VA. Consensus on the management of astigmatism in cataract surgery. Clinical ophthalmology (Auckland, N.Z.). 2019:13():311-324. doi: 10.2147/OPTH.S178277. Epub 2019 Feb 11 [PubMed PMID: 30809088]
Level 3 (low-level) evidenceHeus P, Verbeek JH, Tikka C. Optical correction of refractive error for preventing and treating eye symptoms in computer users. The Cochrane database of systematic reviews. 2018 Apr 10:4(4):CD009877. doi: 10.1002/14651858.CD009877.pub2. Epub 2018 Apr 10 [PubMed PMID: 29633784]
Level 1 (high-level) evidenceKaur K, Kannusamy V, Mouttapa F, Gurnani B, Venkatesh R, Khadia A. To assess the accuracy of Plusoptix S12-C photoscreener in detecting amblyogenic risk factors in children aged 6 months to 6 years in remote areas of South India. Indian journal of ophthalmology. 2020 Oct:68(10):2186-2189. doi: 10.4103/ijo.IJO_2046_19. Epub [PubMed PMID: 32971637]
Gurnani B, Kaur K. Comments on: Are we treating the effect and neglecting the cause of keratoconus? Indian journal of ophthalmology. 2021 Feb:69(2):462-463. doi: 10.4103/ijo.IJO_3280_20. Epub [PubMed PMID: 33463618]
Level 3 (low-level) evidenceLopes MC, Hysi PG, Verhoeven VJ, Macgregor S, Hewitt AW, Montgomery GW, Cumberland P, Vingerling JR, Young TL, van Duijn CM, Oostra B, Uitterlinden AG, Rahi JS, Mackey DA, Klaver CC, Andrew T, Hammond CJ. Identification of a candidate gene for astigmatism. Investigative ophthalmology & visual science. 2013 Feb 1:54(2):1260-7. doi: 10.1167/iovs.12-10463. Epub 2013 Feb 1 [PubMed PMID: 23322567]
Level 1 (high-level) evidenceRead SA,Collins MJ,Carney LG, A review of astigmatism and its possible genesis. Clinical [PubMed PMID: 17177660]
Level 3 (low-level) evidenceKeshav V, Henderson BA. Astigmatism Management with Intraocular Lens Surgery. Ophthalmology. 2021 Nov:128(11):e153-e163. doi: 10.1016/j.ophtha.2020.08.011. Epub 2020 Aug 13 [PubMed PMID: 32798525]