
Introduction
The cisterna magna is a cerebrospinal fluid (CSF) filled space located in the posterior fossa dorsal to the medulla and caudal to the cerebellum. Mega cisterna magna refers to a cystic posterior fossa malformation characterized by an enlarged cisterna magna, absence of hydrocephalus, and an intact cerebellar vermis.[1][2]
The concept of mega cisterna magna was first introduced in the 1960s by Gonsette; its size was initially described on ventriculography as above 15 mm in anterior-posterior length, 5 mm height, and 20 mm width.[3] The size has more recently been proposed as a cisterna magna that is greater than 10 mm on mid-sagittal images.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Blake’s pouch is an inferior protrusion of the fourth ventricle, resulting from a finger-like expansion of the posterior membranous area.[5] During embryogenesis, Blake’s pouch is a transient structure that initially does not communicate with the surrounding subarachnoid space. It later becomes a permeable structure and constitutes the foramen of Magendie.[5]
The timing of when this permeabilization occurs has not yet been established with certainty. The mega cisterna magna is hypothesized to develop embryologically from the permeabilization of Blake’s pouch, allowing for the flow of CSF from the fourth ventricle inferiorly with the peri-medullary subarachnoid spaces and superiorly through the foramen of Magendie.[6]
Formation of the cisterna magna is completed within the leptomeninges at the end of the 7th gestational week. Anatomically, the cisterna magna occupies the vallecula cerebelli, a depression between the medial aspect of the cerebellar tonsils and the inferior surface of the vermis.[6]
The cisterna magna extends anteriorly to the foramen of Magendie and inferiorly to the first cervical level. The cisterna magna is limited posteriorly by an arachnoid membrane and inferiorly from the posteroinferior surface of the cerebellum at the level of the vermian pyramid to the upper cervical spinal cord. The posterior aspect of the cisterna magna is separated by the falx cerebelli.[6]
Epidemiology
The exact incidence and prevalence of mega cisterna magna are not well known as it is most commonly an asymptomatic radiographic finding on cranial imaging obtained for a different indication.
In a series of 19,301 consecutive computed tomography (CT) or magnetic resonance imaging (MRI) scans obtained for headache or mild head trauma, a total of 49 cases were identified for an estimated prevalence of 2.5 per 1000.[7] There is not a significant gender predilection.[8]
History and Physical
In the adult patient, history should include inquiry about developmental milestones in the pediatric patient and any potential neurologic, psychiatric, or cognitive manifestations. Physical examination during the perinatal period should include a search for additional neurologic and systemic malformations, including headache, nausea/vomiting, paresthesias, weakness, ataxia, etc.
The focus of the neurologic examination will vary based on the patient's age, including tests of attention, motor, sensory, coordination, reflexes, and brainstem reflexes, and in older patients should include a mental status examination.
Evaluation
Perinatal evaluation should include a search for the additional central nervous system (CNS) and extra-CNS malformations. Mega cisterna magna was initially evaluated by ventriculography which is rarely employed. Mega cisterna magna may now be evaluated with ultrasonography in the fetus or newborn before fontanelle closure.
Following fontanelle closure, the mega cisterna magna is best evaluated by computed tomography (CT) with magnetic resonance imaging (MRI) brain with and without contrast as the gold standard to rule out similar appearing pathologies. Radiographically, the mega cisterna magna appears as a prominent retrocerebellar CSF appearing space measuring greater than 10 mm on mid-sagittal images with a normal cerebellar vermis and ventricular caliber.[4]
It is critical to exclude ventriculomegaly and cerebellar hypoplasia before diagnosing mega cisterna magna. Additionally, there should be a lack of associated enhancement. Clinically, a neuropsychiatric evaluation could be considered if there is any clinical concern.
Treatment / Management
No specific treatment is necessary for patients with incidentally discovered mega cisterna magna. Medications may treat associated signs/symptoms that may or may not be directly related to the mega cisterna magna, including headache, seizure, or psychiatric illness.
There is a limited role in surgical intervention, which may include CSF diversion for the treatment of hydrocephalus. However, if hydrocephalus is present, the diagnosis of mega cisterna magna should be questioned. Other surgical interventions include suboccipital craniectomy, with the surgical exploration of 2 patients in an early study without relief of patient symptoms.[8]
There is no clear established follow-up timeline for patients with mega cisterna magna. It is probably reasonable to follow patients into adolescence and early adulthood as manifestations, if present, may not initially present in early childhood. There are no clear follow-up guidelines for adults with incidentally discovered mega cisterna magna.
It is likely reasonable in an asymptomatic adult with an incidentally discovered cisterna magna on a high-resolution image, such as an MRI of the brain, to follow up on an as-needed basis with repeat imaging obtained if new symptoms were to develop.
Differential Diagnosis
Posterior fossa arachnoid cyst: Arachnoid cysts are filled with cerebrospinal fluid (CSF) and do not communicate with the ventricular system or subarachnoid spaces. Posterior fossa arachnoid cysts may be difficult to distinguish from a mega cisterna magna and may appear anywhere within the posterior fossa.
Similar to mega cisterna magna, arachnoid cysts match the CSF signal density on computed tomography (CT) and signal intensity on magnetic resonance imaging (MRI) and typically do not enhance following administration of intravenous contrast. In contrast to mega cisterna magna, arachnoid cysts may be associated with a mass effect on the cerebellum, resulting in obstructive hydrocephalus. Posterior fossa arachnoid cysts may also result in scalloping of the occipital bone.[5]
Persistent Blake's pouch cyst: During embryogenesis, Blake's pouch is an inferior protrusion of the fourth ventricle. Blake's pouch results from a finger-like expansion of the posterior membranous area. It initially does not communicate with the subarachnoid space but later becomes a permeable structure and then constitutes the foramen of Magendia.[5]
Persistent Blake's pouch cyst results when there is failed permeabilization. Persistent Blake's pouch cyst radiographically may have a similar radiographic appearance to mega cisterna magna, appearing as a cystic posterior fossa mass that matches CSF density on CT imaging and CSF intensity on MRI imaging. In contrast to mega cisterna magna, persistent Blake's pouch is characteristically associated with hydrocephalus. Similar to mega cisterna magna, persistent Blake's pouch cyst is not associated with cerebellar hypoplasia. Persistent Blake's pouch cysts are not associated with other brain abnormalities.
Dandy-Walker variant: Dandy-Walker variant is usually an isolated malformation but can also occur in association with many other conditions, including Aicardi syndrome, Meckel-Gruber syndrome, Walker Warburg syndrome, and chromosomal abnormalities such as trisomy 9, 13, and 18, among others.
The key distinguishing feature of the Dandy-Walker variant radiographically is a hypoplasia of the cerebellar vermis, which rarely may be completely absent.[5] In contrast, hypoplasia of the cerebellar vermis is not characteristic of mega cisterna magna. Similar to in mega cisterna magna, hydrocephalus is not a common finding in the Dandy-Walker variant unless associated with an additional abnormality.
Epidermoid cyst: Epidermoid cysts are slow-growing congenital tumors that develop from remnants of epidermal elements during the closure of the neural tube and disjunction of the surface ectoderm with neural ectoderm.[9]
Posterior fossa epidermoid cysts usually arise in the lateral subarachnoid cisterns. Epidermoid cysts may be difficult to distinguish from mega cisterna magna on computed tomography (CT) and head ultrasound as they both match CSF signal density and echogenicity, respectively. Similarly, on MRI, mega cisterna magnas and epidermoid cysts will match CSF signal intensity.
In contrast to mega cisterna magna, epidermoid cysts on diffusion-weighted imaging (DWI) magnetic resonance imaging (MRI) sequence will appear hyperintense with correlated hypointensity on apparent diffusion coefficient (ADC). Mega cisterna magna, in contrast, do not restrict diffusion on diffusion-weighted imaging.
Pilocytic astrocytoma: Pilocytic astrocytomas account for approximately 15% of central nervous system (CNS) tumors and are the most common pediatric brain tumor.[10] Pilocytic astrocytomas may arise in the cerebral hemispheres, brainstem, spinal cord, and chiasmatic/hypothalamic region but tend to arise in the cerebellum.[11]
Pilocytic astrocytomas will have a cystic appearance similar to mega cisterna magna, but in contrast, pilocytic astrocytomas will typically additionally have an associated enhancing mural nodule. The cystic portion of pilocytic astrocytomas may or may not enhance following administration of intravenous contrast. Additionally, pilocytic astrocytomas, if large enough, can have an associated posterior fossa mass effect resulting in obstructive hydrocephalus, which is not seen in mega cisterna magna.
As with mega cisterna magna, unless there is significant mass effect or an additional associated abnormality present, there is no hypoplasia of the cerebellar vermis. Pilocytic astrocytomas do not typically restrict diffusion on diffusion-weighted imaging. Pilocytic astrocytomas may be associated with neurofibromatosis type 1.[12]
Prognosis
Overall, adults' cognitive functioning with isolated mega cisterna magna is within normal limits. However, patients with isolated mega cisterna magna in a small case series have been found to score inferior to controls on specific parameters, including those of memory, executive functioning, and verbal fluency.[7]
Studies on outcomes in patients with mega cisterna magna are limited and conflicting. In an older study identifying 14 cases of isolated mega cisterna magna out of 1,260 reviewed CT scans, long-standing neurologic dysfunction was reported in 57% of patients (8/14).[13]
The high frequency in this study may be due to the use of CT imaging, which has poor posterior fossa resolution and may have missed an associated malformation resulting in misdiagnosis. In a later study, 15 fetuses reviewed sonographically were found to have isolated mega cisterna magna.[14] In all 15 cases, the fetuses were found to be phenotypically normal without evidence of neurologic disorder. There was no reported evidence of neurologic disorder or developmental delay on available follow-up spanning up to 69 months for 8 of the patients.[14]
These results may also be of limited value as cognitive and behavioral disorders may be difficult to assess during childhood accurately and may become more apparent with age.
Complications
In a recent meta-analysis including 144 fetuses with mega cisterna magna, the rates of the additional central nervous system (CNS) and extra-CNS anomalies were 12.6% and 16.6%, respectively, without any identifiable chromosome abnormality.[15]
It has been postulated that the cerebellum is connected to various regions of the cerebral cortex by a cortico-cerebellar-thalamic-cortical circuit and that the cerebellum may serve a crucial role in this circuit by coordinating or modulating aspects of cortical activity.[16]
There have been reported psychiatric associations between mega cisterna magna, including mania, bipolar disorder, schizophrenia, and catatonia.[17][18][19]
Due to the limited reports and rarity of mega cisterna magna, it is difficult to state if there is any relationship between mega cisterna magna and psychiatric disorders or if these are purely incidental reports.
Deterrence and Patient Education
The exact incidence and prevalence of mega cisterna magna are unknown, but in available studies, it is rare, reported at less than 1%. Clinical manifestations are conflicting but appear more favorable in recent studies with a lower incidence of neurologic manifestations.[14]
Manifestations of mega cisterna magna may include specific cognitive parameters, including memory, executive function, verbal fluency, and psychiatric disorders.[17][18][19]
There is no specific treatment or surgical intervention that is usually needed or provides benefit in mega cisterna magna.
Enhancing Healthcare Team Outcomes
Healthcare professionals should be aware that in the vast majority of cases, the mega cisterna magna is an incidental radiographic finding with little if any clinical significance that does not require long-term follow-up. In most cases, it is considered a normal radiographic variant. It can, however, be associated with other neurologic or systemic anomalies, albeit rarely. All interprofessional team members, including clinicians (MDs, DOs, NPS, and PAs), and nursing staff, need to engage in open communication, collaborative action, and accurate record-keeping and information sharing to optimize patient outputs.
Appropriate evaluation, including magnetic resonance imaging (MRI) of the brain with and without contrast, should be obtained to rule out other etiologies. For mega cisterna magna, there is no indicated specific treatment or surgical intervention.
Media
(Click Image to Enlarge)
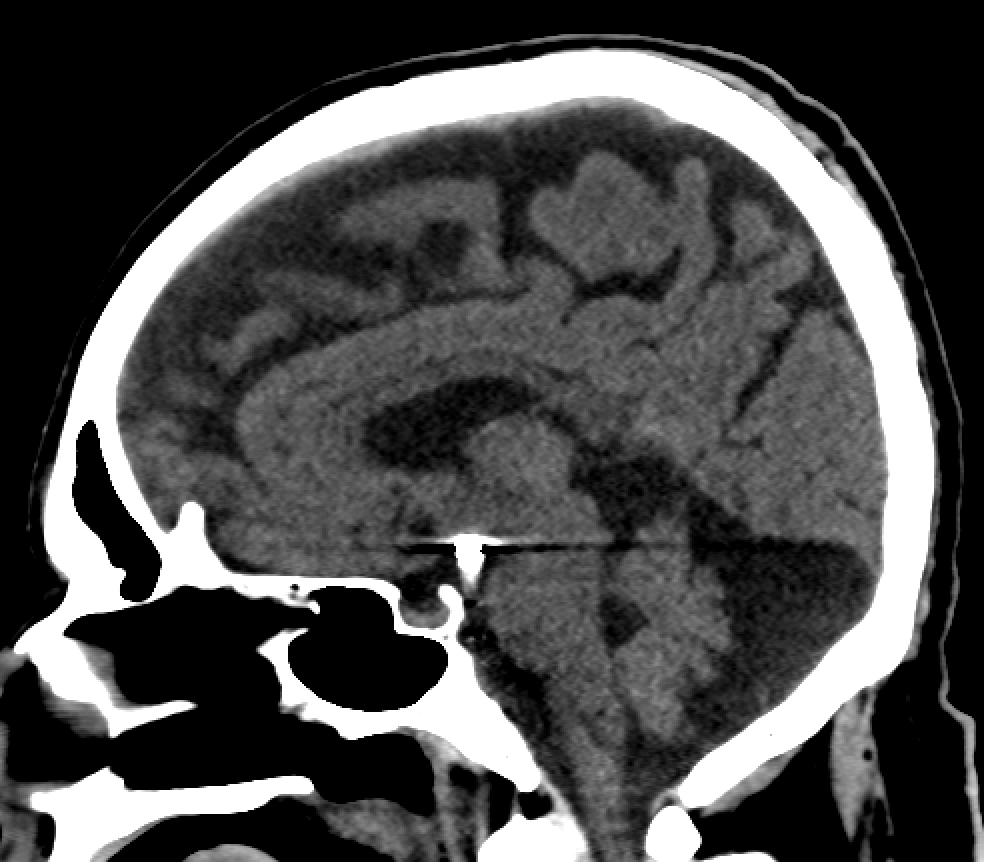
Mega cisterna magna Contributed by Steve Lange, MD
References
Altman NR, Naidich TP, Braffman BH. Posterior fossa malformations. AJNR. American journal of neuroradiology. 1992 Mar-Apr:13(2):691-724 [PubMed PMID: 1566724]
Tortori-Donati P, Fondelli MP, Rossi A, Carini S. Cystic malformations of the posterior cranial fossa originating from a defect of the posterior membranous area. Mega cisterna magna and persisting Blake's pouch: two separate entities. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 1996 Jun:12(6):303-8 [PubMed PMID: 8816293]
Gonsette R, Potvliege R, Andre-Balisaux G, Stenuit J. [Mega-cisterna magna: clinical, radiologic and anatomopathologic study]. Acta neurologica et psychiatrica Belgica. 1968 Aug:68(8):559-70 [PubMed PMID: 4976720]
Lerman-Sagie T, Prayer D, Stöcklein S, Malinger G. Fetal cerebellar disorders. Handbook of clinical neurology. 2018:155():3-23. doi: 10.1016/B978-0-444-64189-2.00001-9. Epub [PubMed PMID: 29891067]
Shekdar K. Posterior fossa malformations. Seminars in ultrasound, CT, and MR. 2011 Jun:32(3):228-41. doi: 10.1053/j.sult.2011.02.003. Epub [PubMed PMID: 21596278]
LILIEQUIST B. The anatomy of the subarachnoid cisterns. Acta radiologica. 1956 Jul-Aug:46(1-2):61-71 [PubMed PMID: 13361914]
Zimmer EZ,Lowenstein L,Bronshtein M,Goldsher D,Aharon-Peretz J, Clinical significance of isolated mega cisterna magna. Archives of gynecology and obstetrics. 2007 Nov; [PubMed PMID: 17453222]
Level 2 (mid-level) evidenceAdam R, Greenberg JO. The mega cisterna magna. Journal of neurosurgery. 1978 Feb:48(2):190-2 [PubMed PMID: 624967]
Berger MS, Wilson CB. Epidermoid cysts of the posterior fossa. Journal of neurosurgery. 1985 Feb:62(2):214-9 [PubMed PMID: 3968559]
Bornhorst M, Frappaz D, Packer RJ. Pilocytic astrocytomas. Handbook of clinical neurology. 2016:134():329-44. doi: 10.1016/B978-0-12-802997-8.00020-7. Epub [PubMed PMID: 26948364]
Sadighi Z, Slopis J. Pilocytic astrocytoma: a disease with evolving molecular heterogeneity. Journal of child neurology. 2013 May:28(5):625-32. doi: 10.1177/0883073813476141. Epub 2013 Feb 25 [PubMed PMID: 23439714]
Listernick R, Ferner RE, Liu GT, Gutmann DH. Optic pathway gliomas in neurofibromatosis-1: controversies and recommendations. Annals of neurology. 2007 Mar:61(3):189-98 [PubMed PMID: 17387725]
Bodensteiner JB, Gay CT, Marks WA, Hamza M, Schaefer GB. Macro cisterna magna: a marker for maldevelopment of the brain? Pediatric neurology. 1988 Sep-Oct:4(5):284-6 [PubMed PMID: 3242531]
Haimovici JA, Doubilet PM, Benson CB, Frates MC. Clinical significance of isolated enlargement of the cisterna magna (} 10 mm) on prenatal sonography. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 1997 Nov:16(11):731-4; quiz 735-6 [PubMed PMID: 9360236]
Level 2 (mid-level) evidenceD'Antonio F, Khalil A, Garel C, Pilu G, Rizzo G, Lerman-Sagie T, Bhide A, Thilaganathan B, Manzoli L, Papageorghiou AT. Systematic review and meta-analysis of isolated posterior fossa malformations on prenatal ultrasound imaging (part 1): nomenclature, diagnostic accuracy and associated anomalies. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2016 Jun:47(6):690-7. doi: 10.1002/uog.14900. Epub 2016 May 10 [PubMed PMID: 25970099]
Level 1 (high-level) evidenceAndreasen NC, Pierson R. The role of the cerebellum in schizophrenia. Biological psychiatry. 2008 Jul 15:64(2):81-8. doi: 10.1016/j.biopsych.2008.01.003. Epub 2008 Apr 8 [PubMed PMID: 18395701]
Pandurangi S, Pandurangi A, Matkar A, Shetty N, Patil P. Psychiatric manifestations associated with mega cisterna magna. The Journal of neuropsychiatry and clinical neurosciences. 2014 Apr 1:26(2):169-71. doi: 10.1176/appi.neuropsych.13040097. Epub [PubMed PMID: 24763763]
Level 3 (low-level) evidenceKumar S,Sur S,Singh A, Mega cisterna magna associated with recurrent catatonia: a case report. Biological psychiatry. 2011 Aug 15; [PubMed PMID: 21641583]
Level 3 (low-level) evidenceTuran T, Beşirli A, Asdemir A, Ozsoy S, Eşel E. Manic episode associated with mega cisterna magna. Psychiatry investigation. 2010 Dec:7(4):305-7. doi: 10.4306/pi.2010.7.4.305. Epub 2010 Nov 9 [PubMed PMID: 21253417]