Introduction
Visual evoked potentials (VEP)s represent a valid electrophysiological tool in neurological pathologies. VEPs are the expression of the electrical activity of the visual pathways up to the optic nerve to the calcarine cortex.[1]
These potentials provide a non-invasive exploration method of the functionality of the human visual system through detecting neuronal pool activity responding to stimuli independently of the consciousness and attention state of the patient. The measurement of VEP is made possible by applying electrodes on the scalp in the occipital region and administering visual stimuli in a patient with open eyes.[1][2]
Depending on the characteristics of the stimulus, pattern visual evoked potentials can provide different information on the functionality of the various sectors of the visual field and the integrity of the optical pathways. This type of instrumental exploration has a clinical application in ophthalmological retinal pathology and neurological pathology related to the optic nerve and/or brain (inflammatory, atrophic, toxic, tumoral, and genetic disease). VEPs has been used as an alternative method to assess visual acuity in non-verbal infants and adults with low intellectual abilities or potential malingering.[3][4][5]
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
Technical Notions
The main type of VEPs used in studying neurological pathologies affecting the visual pathways is VEP structured with a stimulation model (pattern-VEP or P-VEP). Generally, it is a "reversal" pattern (reversal-P-VEP), in which the light and dark elements of the model are organized to form a chessboard or bars. The stimuli are reversed, allowing contrast variations with constant average luminance. Another type of VEP with an "onset-offset" pattern (onset-offset-P-VEP) is based on a visual stimulus that appears and disappears in a sequence always characterized by a constant average luminance.
VEPs that use a diffuse flash stimulus (flash-VEP or F-VEP) characterized by a variation in brightness, however, have a rather limited field of application in the field of neurological pathologies affecting the visual pathways considering that this testing method offers extremely variable responses in the normal individuals and are less sensitive than P-VEP. Furthermore, P-VEPs allow for the selection of characteristics for the most suitable stimulus in the clinical analysis of the different components of the visual system, which can be activated differently according to the spatial, temporal, chromatic, and contrast properties of the image.[6][7] (See Figures of instrumentation, testing, stimulator, and results of VEPs)
The spatial frequency (SF) of a pattern stimulus measures how many times the contrast of an image changes from the minimum to the maximum value in a degree of visual angle, which is then measured in cycles per degree (c / d), where 1 c / g corresponds to the complete alternation from a light element to a dark one in a degree of visual angle.
The size of the bar (w) can be calculated by the formula: w = 60/2f, where w is expressed in arc minutes and f is the SF expressed in c/d. If instead of bars, the model used is a chessboard, the dimensions of the chessboards are measured in arc minutes of the degree of visual angle. The different SFs permit the exploration of the different sectors of the visual field by stimulating the different neuronal systems of the visual pathway physiologically.[8]
The electrophysiological response obtained with a potential depends on the luminance of the stimulus, the contrast between the two stimuli (luminance difference), and the temporal frequency. P-VEP amplitude increases linearly with increasing contrast and disappears for contrasts equal to or less than 10% when the difference between light and dark elements is no longer recognizable. If VEPs are recorded according to an offset/onset stimulus, the background luminance of the offset stimulus must be identical to that of the structured stimulus (onset stimulus).
The contrast (C) between the elements of the pattern corresponds to the difference in luminance between the light and dark elements and is expressed in percentage values. The electrophysiological response obtained with a P-VEP depends on the temporal frequency, that is, on the speed with which the pattern appears or disappears (onset-off-set-P-VEP) or with which the elements of the model reverse their position (reversal-P-VEP). The variation of the temporal frequency with which the elements reverse each other at low frequencies (<4 Hz) is considered a "transient" type response, while at high frequencies (>4 Hz), the response type is defined as a "steady state."[9]
In the reversal-P-VEP, low stimulation FTs (between 1 Hz and 4 Hz) are currently used, allowing precise recording from the occipital cortex. This electrophysiological response is known as "transient" response. The "transient" potential of the reversal-P-VEP consists of three deflections of the electrical signal with an alternating polarity of reproducible latency and morphology, in which it is possible to recognize a positive main component with a latency of about 100 ms (potential P 100), preceded and followed by two negative components, with a latency of about 70 to 75 ms (potential N 75) and 130 to 145 ms (potential N 140) respectively. The positive component P100 represents the most stable and repeatable response of this P-potential, recordable on all scalp regions that correspond to the occipital cortex, with its maximum amplitude along the midline, at the inion.
Numerous studies have identified P100 as the electrical correlate of the activity of the primary visual cortex. For lesions of the optic pathways with cortical saving, it is still possible to record an intact P100. The other two negative components of the potential (N140 and N70) could instead have generators at the level of the striatal cortex (N70) and extra-striatal (N140), which tend not to be useful in clinical practice.[9][10][11] (See Figures of VEPs results)
Applications
In a routine clinical setting, the P-VEP stimulation pattern is obtained through the simultaneous stimulation of the two visual hemifields on the sides of the fixation center (whole-field stimulation) while the recording electrodes are positioned on the occipital scalp at Oz (International Electroencephalographic System 10-20) and on two symmetrical points placed laterally 5 to 7 cm away from the central one.
The potentials recorded by the laterally placed electrodes are generally variable and less represented; therefore, amplitude and latency parameters are regularly acquired considering the central electrode. The evaluations of the morphology, amplitude, and above all, the latency (retino-cortical conduction time) of the P100 potential represent the fundamental element for the electrophysiological study of the integrity of the optical pathways, especially at the pre-chiasmatic level.
The reduction of the sensitivity of the visual field due to damage to the retro-orbital nerve structures (optic nerve) determines alterations of the P-PEV that are reflected as a decrease in amplitude and/or in a lengthening of the latency time of the different components that make up the potential. The variations in amplitude and latency of PEVs represent precisely the electrophysiological correlate of different pathological phenomena that affect the optical pathways.
The topographic position, size, and degree of the campimetric deficit strictly condition any anomalies detected in the analysis of the P-PEV. Lesions of the optic nerve associated with relative scotomas in the macular area can cause significant alterations of the P-VEP recorded by the scalp, while an absolute scotoma, even if extensive but localized in the peripheral region of the visual field, can modify the P-VEP in a minimal or even null way.[12]
Clinical Significance
P-VEPs represent a sensitive indicator of abnormalities in the integrity of the entire visual system, which can be the subject of demyelinating or axonal pathologies. Depending on the type of pathogenetic mechanism, P-VEPs can signal the presence of demyelination phenomena, expressed by changes in latency and an increase in retinol-cortical conduction time, as well as indicating the existence of axonal damage evidenced by alterations in the amplitude and morphology of the acquired responses. According to these principles, P-VEPs are used to diagnose pre-chiasmatic, chiasmatic, and retrochiasmatic neurological pathologies.[13][14][15]
Neuropthalmological Field
VEPs are used in the field of neuro-ophthalmology for several clinical applications, which include: the quantification and monitoring of functional damage in optical neuropathies of different inflammatory, demyelinating, compressive, ischemic, traumatic, hereditary, degenerative, and/or toxic-metabolic origin; the differential diagnosis between optic nerve pathologies and retinal pathologies through the use of results associated with functional examinations of the retina; and, in the distinction between cortical blindness and malingering.[16][17][18]
Neurological Field
Multiple sclerosis is an inflammatory disease of the white matter characterized by a multifocal involvement of the brain's white matter. The clinical manifestations are very variable in relation to the localization and extent of demyelination outbreaks; however, the lesions seem to have a preferential distribution in some areas of the central nervous system. In more than 20% of cases, the symptom of the onset of the disease is optic neuritis, and over 50% of patients have a clinical episode of optic neuritis. Studies have sown that VEP latency and optical coherence tomography retinal nerve layer thickness measurements correlated with disability measurements and can be useful in the management of these patients.[19] The early clinical signs of MS could identify "benign" phenotypes, characterized by an almost complete recovery of vision and retinal sensibility loss in the acute phase.[20][21]
In demyelinating pathologies of the optic nerve, P-VEPs show a delay in the latency of responses, often in the absence of significant alterations of the amplitude related to the decrease in patients' visual acuity. The latency alterations of the P-VEP could persist for a long time, even after the full recovery of visual acuity. It is sometimes possible to observe the delay of the latency of the P-PEV also in the contralateral eye. This alteration type can reveal the presence of sub-clinical alterations of the conduction of the impulse along the optic nerve, even before clinical signs or symptoms of nerve involvement manifest.[22]
In the ischemic neuropathy of the optic nerve, anterior ischemic optic neuropathy or AION is due to infarction of the laminar or laminar portion of the optic nerve head caused by occlusion of the short ciliary posteriors arteries. The clinical onset of this alteration is generally unexpected, without pain, and the loss of vision can progress for many days. Studies have shown VEPs useful in the management of these patients.[23]
The campimetry deficit is typically altitudinal and may involve the central fixation area, which justifies the severe loss of visual acuity. Regarding VEP alterations, it is possible to observe a pre-dominant alteration that turns out to be the marked reduction in the amplitude of P100 associated with a poor modification of latency.[24]
The cause of optic nerve compression is frequent optic pathway gliomas of pediatric age. The clinical onset is characterized by a gradual loss of vision without orbital pain, which may even be asymptomatic for a long time. An early clinical diagnosis and an accurate follow-up of patients with compressive neuropathy of the optic nerve, especially in the presence of meningiomas or gliomas, is of fundamental importance to improve the therapeutic approach based on surgical resection and/or radiotherapy procedures.[25] In these cases, PEVs consistently exhibit a de-synchronized P100 of low amplitude with an evident latency delay.[26]
Concerning neurodegenerative diseases, the study VEPs do not typically have a diagnostic role. These testing methods, however, can offer the possibility of investigating the physio- and pathophysiological mechanisms and the involvement of the different neurotransmission systems involved in the pathogenesis of these morbid conditions in a refined and non-invasive way.
Leber optic neuropathy (LON) and Kjer-type dominant optic neuritis (DON) are the most common hereditary forms of primary retinal ganglion cell disease. LON typically presents a progressive loss of bilateral vision not associated with orbital tissue and is linked to mitochondrial mutations. In these cases, P-VEPs are markedly delayed, but relative maintenance of P100 morphology is possible in the initial stages of the disease.
Alterations in the P100 amplitude are related to the stage and clinical form of the disease. Alterations of P-PEVs are generally preceded by the reduction of the amplitude or even by the lack of reproducibility of the N95 potential.[27]
In Friedrich's Ataxia, PEVs are used to assess the evolution of visual function in this neurodegenerative disease, which tends to be abnormal in two-thirds of patients. The delayed latency and the increased amplitude of wave p100 is the most frequent electrophysiological alteration in this pathology.[28][29]
Other Issues
Surgical Intraoperative Monitoring
In the last few years, VEPs have been considered for intraoperative monitoring of visual function using several protocols; however, current literature and clinical evidence in this field are very limited. The use of total intravenous anesthesia, the introduction of light-emitting diode technology, electroretinography, and electroencephalography have increased the reliability of VEP neuromonitoring by enhancing the technique’s reproducibility and interpretability and working to make it more reliable and easier to integrate it into the operative workflow.
Recent studies have applied these tools in orbital and transsphenoidal surgery.[30][31][32] (See Figures of intraoperative surgical monitoring with VEPs)
Enhancing Healthcare Team Outcomes
VEP application requires an interprofessional team of healthcare professionals, including nurses, neurophysiopathology technicians, neurologists, and ophthalmologists. This team is fundamental for correctly applying this tool both in the clinical field and in intraoperative surgical monitoring. VEPs are regularly used in diagnosing pre-chiasmatic, chiasmatic, and retrochiasmatic neurological pathologies.[13] [Level 3]
In this scenario, the neurophysiopathology technician provides for the preparation and control of the instrumentation of the equipment it is equipped with and fully manages to collect and optimize the various diagnostic methods on which, upon request, it must draw up a descriptive report from the technical aspect. (level I)
Recent studies have applied VEPs in orbital and transsphenoidal surgery but without standardized protocols and homogeneous results.[30][31][32] [Level 3]
An interprofessional team that provides an integrated approach to patient care and comprehensive diagnostic management can help achieve the best possible outcomes. Collaboration, multidisciplinary shared decision-making, and open communication between team members are key elements for a proper diagnosis and a good outcome. The interprofessional care provided to the patient must use an integrated care pathway combined with an evidence-based approach to planning and evaluating all joint activities.[33] The earlier signs and symptoms of a complication are identified, the better the prognosis and outcome. [Level 3]
Media
(Click Image to Enlarge)
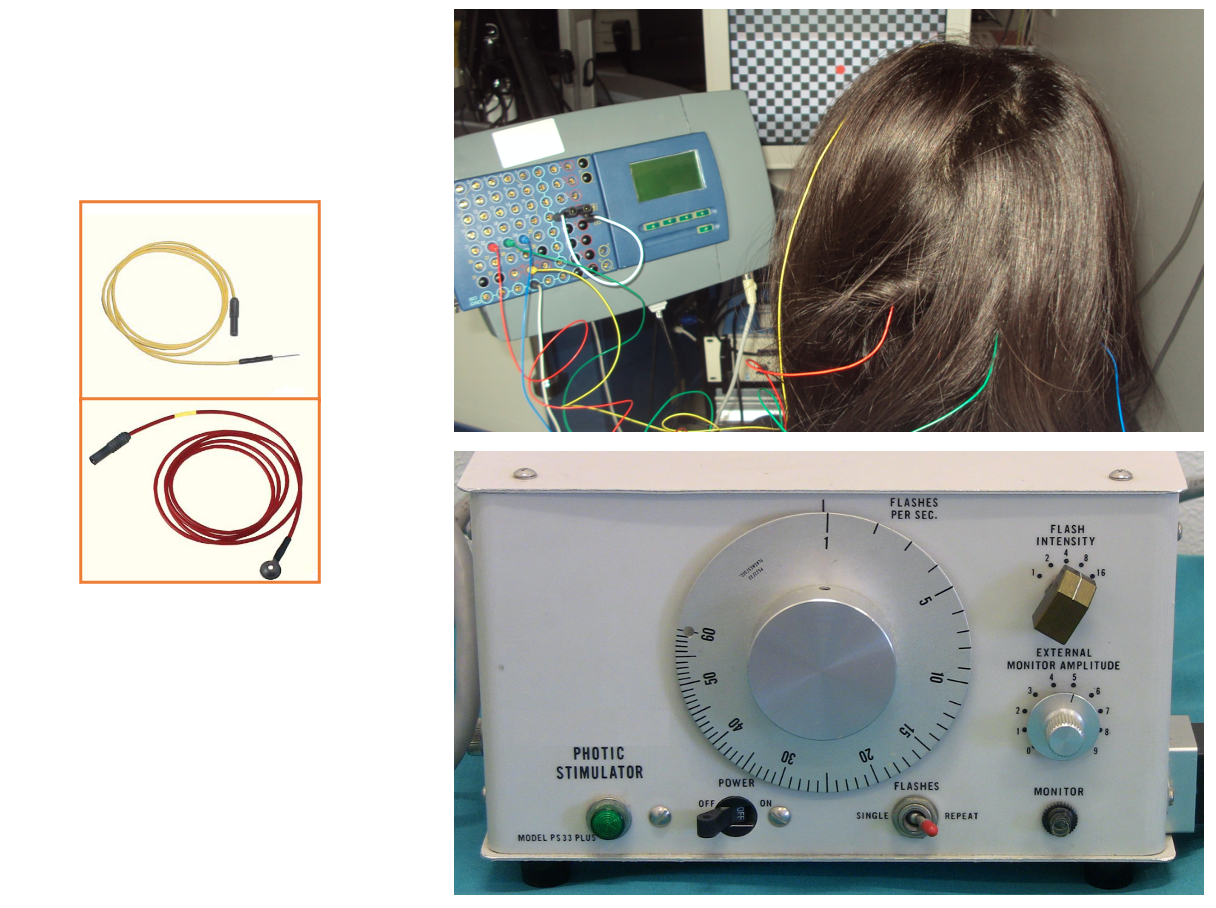
Visual evoked potentials (VEPs) using a chessboard stimulation. Different electrodes can be used, which are placed on the scalp. The instrument is equipped with a stimulator to regulate the frequency and intensity of the light stimuli. Contributed by Marco Zeppieri, MD, PhD. Images courtesy of Elisa Ecoretti and Giada Pauletto, MD.
(Click Image to Enlarge)
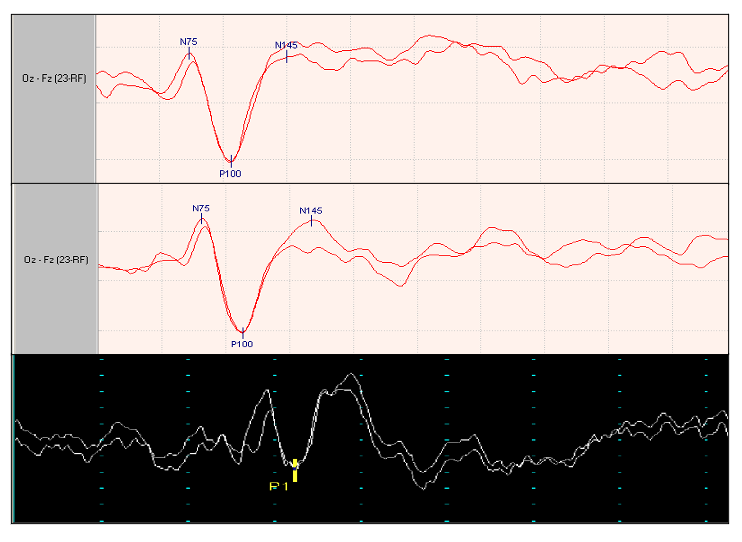
Pattern and flash visual evoked potentials (VEPs) results. Contributed by Marco Zeppieri, MD, PhD. Images courtesy of Elisa Ecoretti and Giada Pauletto, MD.
(Click Image to Enlarge)
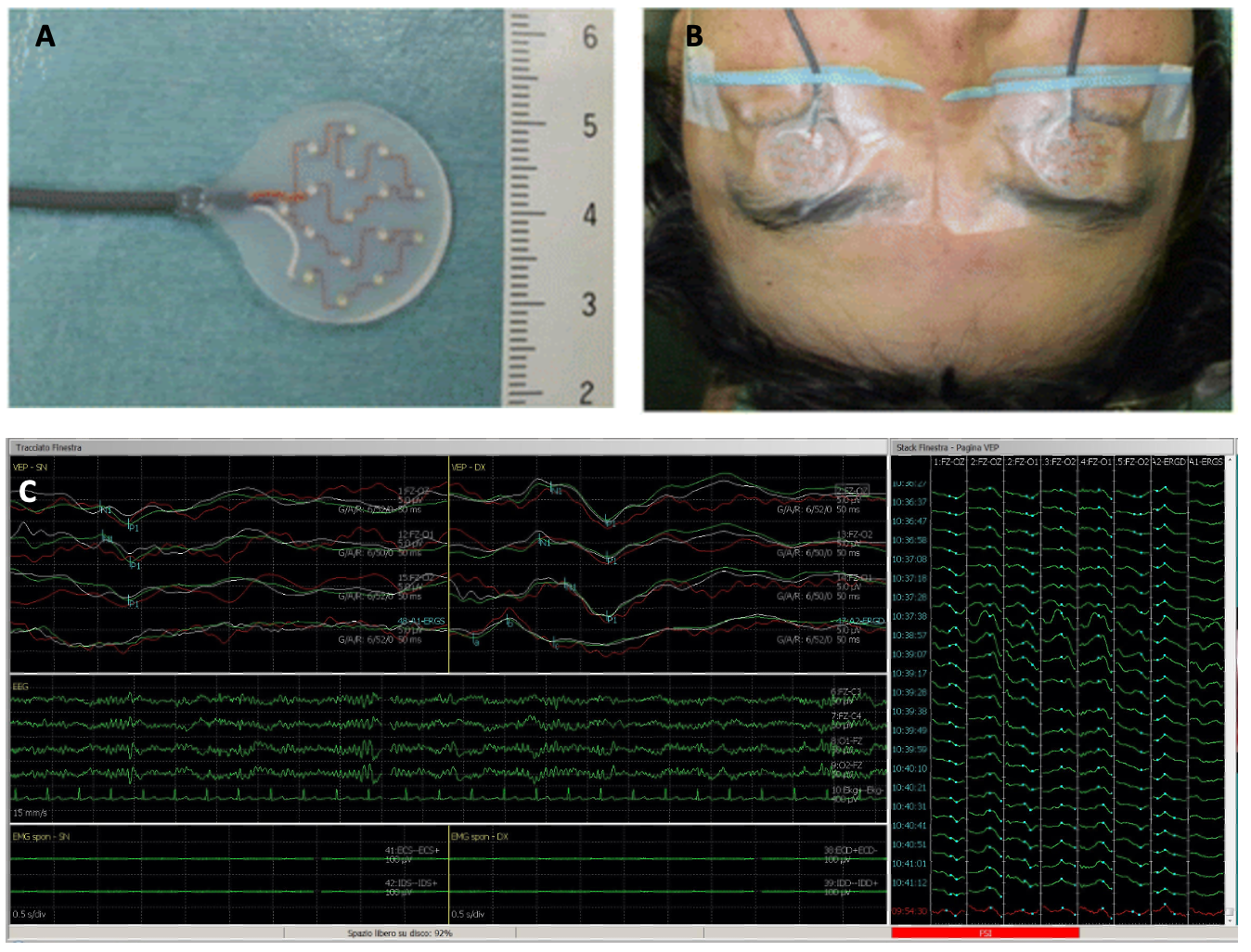
Flash stimulation pads used for surgical intraoperative monitoring. Intraoperative visual evoked potentials (VEPs) results. Contributed by Marco Zeppieri, MD, PhD. Images courtesy of Elisa Ecoretti and Giada Pauletto, MD.
References
Hoffmann MB, Brands J, Behrens-Baumann W, Bach M. VEP-based acuity assessment in low vision. Documenta ophthalmologica. Advances in ophthalmology. 2017 Dec:135(3):209-218. doi: 10.1007/s10633-017-9613-y. Epub 2017 Oct 4 [PubMed PMID: 28980154]
Level 3 (low-level) evidenceHamilton R, Bach M, Heinrich SP, Hoffmann MB, Odom JV, McCulloch DL, Thompson DA. VEP estimation of visual acuity: a systematic review. Documenta ophthalmologica. Advances in ophthalmology. 2021 Feb:142(1):25-74. doi: 10.1007/s10633-020-09770-3. Epub 2020 Jun 2 [PubMed PMID: 32488810]
Level 3 (low-level) evidencePatterson Gentile C, Joshi NR, Ciuffreda KJ, Arbogast KB, Master C, Aguirre GK. Developmental Effects on Pattern Visual Evoked Potentials Characterized by Principal Component Analysis. Translational vision science & technology. 2021 Apr 1:10(4):1. doi: 10.1167/tvst.10.4.1. Epub [PubMed PMID: 34003980]
Zheng X, Xu G, Zhang K, Liang R, Yan W, Tian P, Jia Y, Zhang S, Du C. Assessment of Human Visual Acuity Using Visual Evoked Potential: A Review. Sensors (Basel, Switzerland). 2020 Sep 28:20(19):. doi: 10.3390/s20195542. Epub 2020 Sep 28 [PubMed PMID: 32998208]
Soares TS, Sacai PY, Berezovsky A, Rocha DM, Watanabe SE, Salomão SR. Pattern-reversal visual evoked potentials as a diagnostic tool for ocular malingering. Arquivos brasileiros de oftalmologia. 2016 Sep-Oct:79(5):303-307. doi: 10.5935/0004-2749.20160087. Epub [PubMed PMID: 27982208]
Mahajan Y, Ching A, Watson T, Kim J, Davis C. Effect of sustained selective attention on steady-state visual evoked potentials. Experimental brain research. 2022 Jan:240(1):249-261. doi: 10.1007/s00221-021-06251-0. Epub 2021 Nov 2 [PubMed PMID: 34727219]
Hassankarimi H, Jafarzadehpur E, Mohammadi A, Noori SMR. Low-contrast Pattern-reversal Visual Evoked Potential in Different Spatial Frequencies. Journal of ophthalmic & vision research. 2020 Jul-Sep:15(3):362-371. doi: 10.18502/jovr.v15i3.7455. Epub 2020 Aug 6 [PubMed PMID: 32864067]
Montgomery DP, Hayden DJ, Chaloner FA, Cooke SF, Bear MF. Stimulus-Selective Response Plasticity in Primary Visual Cortex: Progress and Puzzles. Frontiers in neural circuits. 2021:15():815554. doi: 10.3389/fncir.2021.815554. Epub 2022 Jan 31 [PubMed PMID: 35173586]
Yang M, Jung TP, Han J, Xu M, Ming D. [A review of researches on decoding algorithms of steady-state visual evoked potentials]. Sheng wu yi xue gong cheng xue za zhi = Journal of biomedical engineering = Shengwu yixue gongchengxue zazhi. 2022 Apr 25:39(2):416-425. doi: 10.7507/1001-5515.202111066. Epub [PubMed PMID: 35523564]
Kothari R, Singh S, Singh R, Shukla AK, Bokariya P. Influence of visual angle on pattern reversal visual evoked potentials. Oman journal of ophthalmology. 2014 Sep:7(3):120-5. doi: 10.4103/0974-620X.142593. Epub [PubMed PMID: 25378875]
Dymond AM, Coger RW, Serafetinides EA. Data preprocessing applied to human average visual evoked potential P100-N140 amplitude, latency, and slope. Psychiatry research. 1980 Dec:3(3):315-22 [PubMed PMID: 6936725]
Yadav NK, Ludlam DP, Ciuffreda KJ. Effect of different stimulus configurations on the visual evoked potential (VEP). Documenta ophthalmologica. Advances in ophthalmology. 2012 Jun:124(3):177-96. doi: 10.1007/s10633-012-9319-0. Epub 2012 Mar 20 [PubMed PMID: 22426575]
Level 3 (low-level) evidencePark SH, Park CY, Shin YJ, Jeong KS, Kim NH. Low Contrast Visual Evoked Potentials for Early Detection of Optic Neuritis. Frontiers in neurology. 2022:13():804395. doi: 10.3389/fneur.2022.804395. Epub 2022 Apr 29 [PubMed PMID: 35572925]
Thirunavu VM, Mohammad LM, Kandula V, Beestrum M, Lam SK. Vision Outcomes for Pediatric Patients With Optic Pathway Gliomas Associated With Neurofibromatosis Type I: A Systematic Review of the Clinical Evidence. Journal of pediatric hematology/oncology. 2021 May 1:43(4):135-143. doi: 10.1097/MPH.0000000000002060. Epub [PubMed PMID: 33480655]
Level 1 (high-level) evidenceLeocani L, Guerrieri S, Comi G. Visual Evoked Potentials as a Biomarker in Multiple Sclerosis and Associated Optic Neuritis. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2018 Sep:38(3):350-357. doi: 10.1097/WNO.0000000000000704. Epub [PubMed PMID: 30106802]
Wang Y, Wu DZ, Wu LZ, Chen YZ. Visual field versus visual evoked potentials in maculopathies and optic neuropathies. Yan ke xue bao = Eye science. 1989 Jun:5(1-2):52-9 [PubMed PMID: 2485746]
Jurkute N, Robson AG. Electrophysiology in neuro-ophthalmology. Handbook of clinical neurology. 2021:178():79-96. doi: 10.1016/B978-0-12-821377-3.00019-2. Epub [PubMed PMID: 33832688]
Marcar VL, Battegay E, Schmidt D, Cheetham M. Parallel processing in human visual cortex revealed through the influence of their neural responses on the visual evoked potential. Vision research. 2022 Apr:193():107994. doi: 10.1016/j.visres.2021.107994. Epub 2021 Dec 31 [PubMed PMID: 34979298]
Eklund A, Huang-Link Y, Kovácsovics B, Dahle C, Vrethem M, Lind J. OCT and VEP correlate to disability in secondary progressive multiple sclerosis. Multiple sclerosis and related disorders. 2022 Dec:68():104255. doi: 10.1016/j.msard.2022.104255. Epub 2022 Oct 19 [PubMed PMID: 36544315]
Oh J, Vidal-Jordana A, Montalban X. Multiple sclerosis: clinical aspects. Current opinion in neurology. 2018 Dec:31(6):752-759. doi: 10.1097/WCO.0000000000000622. Epub [PubMed PMID: 30300239]
Level 3 (low-level) evidencede Seze J, Bigaut K. Multiple sclerosis diagnostic criteria: From poser to the 2017 revised McDonald criteria. Presse medicale (Paris, France : 1983). 2021 Jun:50(2):104089. doi: 10.1016/j.lpm.2021.104089. Epub 2021 Oct 28 [PubMed PMID: 34718114]
Backner Y, Petrou P, Glick-Shames H, Raz N, Zimmermann H, Jost R, Scheel M, Paul F, Karussis D, Levin N. Vision and Vision-Related Measures in Progressive Multiple Sclerosis. Frontiers in neurology. 2019:10():455. doi: 10.3389/fneur.2019.00455. Epub 2019 May 3 [PubMed PMID: 31130910]
Barbano L, Ziccardi L, Parisi V. Correlations between visual morphological, electrophysiological, and acuity changes in chronic non-arteritic ischemic optic neuropathy. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2021 May:259(5):1297-1308. doi: 10.1007/s00417-020-05023-w. Epub 2021 Jan 7 [PubMed PMID: 33415352]
Jayaraman M, Gandhi RA, Ravi P, Sen P. Multifocal visual evoked potential in optic neuritis, ischemic optic neuropathy and compressive optic neuropathy. Indian journal of ophthalmology. 2014 Mar:62(3):299-304. doi: 10.4103/0301-4738.118452. Epub [PubMed PMID: 24088641]
Level 2 (mid-level) evidenceDotto PF, Berezovsky A, Sacai PY, Rocha DM, Fernandes AG, Salomão SR. Visual function assessed by visually evoked potentials in adults with orbital and other primary intracranial tumors. European journal of ophthalmology. 2021 May:31(3):1351-1360. doi: 10.1177/1120672120925643. Epub 2020 May 29 [PubMed PMID: 32468859]
Bowman R, Walters B, Smith V, Prise KL, Handley SE, Green K, Mankad K, O'Hare P, Dahl C, Jorgensen M, Opocher E, Hargrave D, Thompson DA. Visual outcomes and predictors in optic pathway glioma: a single centre study. Eye (London, England). 2023 Apr:37(6):1178-1183. doi: 10.1038/s41433-022-02096-1. Epub 2022 May 13 [PubMed PMID: 35562551]
Tăbăcaru B, Stanca HT. Further advances in the diagnosis and treatment of Leber's Hereditary Optic Neuropathy - a review. Romanian journal of ophthalmology. 2022 Jan-Mar:66(1):13-16. doi: 10.22336/rjo.2022.4. Epub [PubMed PMID: 35531455]
Level 3 (low-level) evidenceZiccardi L, Cioffi E, Barbano L, Gioiosa V, Falsini B, Casali C, Parisi V. Macular Morpho-Functional and Visual Pathways Functional Assessment in Patients with Spinocerebellar Type 1 Ataxia with or without Neurological Signs. Journal of clinical medicine. 2021 Nov 12:10(22):. doi: 10.3390/jcm10225271. Epub 2021 Nov 12 [PubMed PMID: 34830553]
Rodríguez-Labrada R, Velázquez-Pérez L, Ortega-Sánchez R, Peña-Acosta A, Vázquez-Mojena Y, Canales-Ochoa N, Medrano-Montero J, Torres-Vega R, González-Zaldivar Y. Insights into cognitive decline in spinocerebellar Ataxia type 2: a P300 event-related brain potential study. Cerebellum & ataxias. 2019:6():3. doi: 10.1186/s40673-019-0097-2. Epub 2019 Mar 4 [PubMed PMID: 30873287]
MacDonald DB, Dong CC, Uribe A. Intraoperative evoked potential techniques. Handbook of clinical neurology. 2022:186():39-65. doi: 10.1016/B978-0-12-819826-1.00012-0. Epub [PubMed PMID: 35772897]
Zhu H, Qiao N, Yang X, Li C, Ma G, Kang J, Liu C, Cao L, Zhang Y, Gui S. The clinical application of intraoperative visual evoked potential in recurrent craniopharyngiomas resected by extended endoscopic endonasal surgery. Clinical neurology and neurosurgery. 2022 Mar:214():107149. doi: 10.1016/j.clineuro.2022.107149. Epub 2022 Jan 29 [PubMed PMID: 35151969]
Level 2 (mid-level) evidenceClauser LC, Tieghi R, Galie' M, Franco F, Carinci F. Surgical decompression in endocrine orbitopathy. Visual evoked potential evaluation and effect on the optic nerve. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2012 Oct:40(7):621-5. doi: 10.1016/j.jcms.2012.01.027. Epub 2012 Mar 17 [PubMed PMID: 22424910]
Level 2 (mid-level) evidenceGutowski KA. Evidence-Based Medicine: Abdominoplasty. Plastic and reconstructive surgery. 2018 Feb:141(2):286e-299e. doi: 10.1097/PRS.0000000000004232. Epub [PubMed PMID: 29373443]