
Introduction
Vernal keratoconjunctivitis (VKC) is a recurrent, bilateral allergic inflammation of the conjunctiva.[1] The episodes are often periodic and have seasonal recurrences. Seasonal exacerbations characterize the condition in the initial stages with a peak incidence during spring and summer. Over time, the condition tends to become perennial. VKC is a subtype of allergic conjunctivitis. Vernal keratoconjunctivitis (VKC) is a type of allergic conjunctivitis.[2]
Additional types include perennial and seasonal rhinoconjunctivitis, atopic keratoconjunctivitis, and giant papillary conjunctivitis.VKC is classified based on the area of ocular involvement into palpebral, limbal, and mixed forms.[3]
Palpebral VKC
This involves the upper tarsal conjunctiva. There is a close association between the inflamed conjunctiva and the corneal epithelium, often leading to significant corneal disease.
Limbal VKC
This typically affects bulbar conjunctiva in the palpebral area and typically affects the Black and Asian populations.
Mixed VKC
This has features of both the palpebral and limbal forms.
Arlt was the first to describe peri-limbal swelling in 1846. Horner and Tranta explained the white elevations at the limbus, and these were named as Horner-Tranta dots. Gabrielides studied conjunctival secretions; he found that eosinophils are the main components of these secretions.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Vernal keratoconjunctivitis is a recurrent, bilateral disorder. VKC is more commonly present in males and is most commonly seen after five years. Most cases show remission over the years and are usually resolved by puberty. Few may develop atopic keratoconjunctivitis over the years. VKC is more commonly seen in warm and dry climates. There is also a seasonal variation in these patients, with peak incidence occurring in the spring and summer. These symptoms might become perennial over the years. Thus more chronic the disease, the higher are the chances of symptoms becoming persistent.[5]
There is often a history of atopy present in these patients. Family history of atopy might be positive in close to 49% of these cases. Thus, a genetic link has also been suggested. Apart from personal allergy history, other predisposing factors include male gender, close contact with animals, and increased exposure to dust and sunlight.[6]
Both IgE-mediated and cell-mediated immune mechanisms are thought to be responsible for these exacerbations. Activated eosinophils have also been implicated in the pathophysiology of VKC. Gabrielides also showed the consistent presence of eosinophils in the conjunctival scrapings of VKC patients. Additionally, the role of type 4 hypersensitivity mediated by CD4 T helper cells has also been highlighted through a few studies. Immunomodulators like interleukins 4, 5, 13, and fibroblast growth factors have also been implicated. There is also reported over-expression of cytokines and chemokines in the conjunctiva of these patients.[7]
Epidemiology
The prevalence of vernal keratoconjunctivitis varies from region to region. It is more commonly seen in tropical and sub-tropical countries and is more prevalent in warm and dry areas. The prevalence reported from cooler countries like the United States as 0.29/10000 population. A prevalence varying from 1.2 to 12.6 cases per 10000 have been reported from Europe. The disease is much more common in countries like Africa, with a reported prevalence varying from 2 to 37%.[6]
The prevalence of corneal complications, thus predisposing to blindness-related sequalae, also varies from region to region. The prevalence rates reported from Europe range from 0.30-2.26. While those reported from Italy vary from 0.4 to 4.8, and from Norway to as low as 0.1 to 1.0.[8]
VKC is more common in males. A study done in Ethiopia showed that males were 4.23 times more likely to get affected by VKC than females in their study.[6] Another study from Rwanda found odds of 1.7 for males getting affected compared to females. PMID: 21976577 Similar results with higher prevalence among males have also been reported from Italy.[9]
Pathophysiology
In vernal keratoconjunctivitis, multiple papillae are seen in the upper tarsal conjunctiva. The underlying pathological process involves hyperplasia of the conjunctival epithelium. These hyperplastic tissues send projections downwards into the subepithelial tissue. The adenoid layer shows marked cellular infiltration by eosinophils, plasma cells, lymphocytes, and histiocytes. The fibroblasts show proliferative changes, which later undergo hyaline changes. These factors are responsible for the inflammatory process and are involved in tissue remodeling, resulting in giant papillae seen in VKC.[7]
History and Physical
Vernal keratoconjunctivitis is a severe form of allergic disease characterized by marked itching. This is more commonly seen in young boys. The common symptoms include photophobia, burning, foreign body sensation, mucoid discharge, and tearing. Parents also complain about children rubbing their eyes frequently and increasing blinking. The clinical examination findings vary based on the type of disease, further dependent on the geographical location.[10]
Palpebral disease- In the early stages, there is conjunctival hyperemia and velvety papillary hypertrophy of the superior tarsal plate. In the intense disease, flat polygonal macropapillae, which are <1mm in size, are seen along with the whitish inflammatory disease. With further disease progression, these can form giant papillae that are>1mm in size and result from rupture of the dividing septa. Mucoid deposits can occur between giant papillae. The milder form of the pathology is characterized by minimal conjunctival congestion and decreased mucus production.[11]
The bulbar disease-The bulbar disease is also called limbal disease and is particularly more common and severe in tropical regions. This is characterized by congestion of the bulbar conjunctiva in the interpalpebral area. Gelatinous thickened papillae can form around the limbus and are associated with apically located whitish cellular collections known as Horner Tranta Spots.[12]
Corneal signs – Keratopathy is more commonly associated with palpebral disease and can present as superficial punctate epithelial erosions or epithelial macroerosions. The macroerosions usually result from epithelial toxicity from infiltration of inflammatory cytokines and secondary to direct traumatic mechanical effect from papillae. Severe forms can result in plaques and shield ulcers. These can significantly affect visual acuity. These shield ulcers are difficult to heal and can often result in subepithelial scars or keratinization. The scars can be central or peripheral, oval and grey in color, and affect the vision. Shield ulcers are more common in palpebral or mixed forms of the disease and result when the underlying Bowman's membrane is exposed and becomes coated with mucoid discharge and calcium phosphate, resulting in delayed healing and wetting. Shield ulcers should be aggressively treated to prevent secondary bacterial keratopathy.[13]
Pseudogerontoxon is characterized by a paralimbal band of superficial scarring adjacent to the inflamed limbus resulting from recurrent limbal disease. It usually mimics arcus senalis. VKC is also associated with corneal ectasias, particularly keratoconus, which results from persistent eye rubbing and occasionally superficial vascularization. Associated bilateral herpes simplex keratitis has also been reported.[14]
Lid signs - Blepharitis is often associated with patients with VKC. Some cases might be seen with eczema or maceration of the lid. Subconjunctival fibrosis and symblepharon can rarely develop due to the inflammatory sequelae.[15]
Evaluation
The diagnosis of vernal keratoconjunctivitis is based on clinical examination. The typical history and clinical signs lead to a straightforward diagnosis in most cases. Different staining techniques and associated scoring systems have been described to grade the severity of VKC. The fluorescein stain, lissamine green stain, and confocal microscopy are a few evaluation techniques that help score the severity and grade of involvement. Studies have proven that Oxford scores and Van Bijsterveld scores for evaluating epithelial damage are useful in patients with VKC. Further, the VKC-Collaborative Longitudinal Evaluation of Keratoconus Study (VKC-CLEK) was found to be useful in assessing both limbal and tarsal epithelial damage in VKC patients.[16]
Corneal topography is an additional investigation that should be considered in VKC patients. The use of videokeratography based on the Placido disc-based system has been proven useful in the early detection and prevention of severe forms of keratoconus. These investigations not only help detect subclinical keratoconus but also provide an opportunity for timely management of these cases and prevent further progression.[17] Occasionally additional lab tests in the form of conjunctival scrapings might be advised in patients with diagnostic dilemmas or not responding to the routine treatment. The conjunctival scraping will show the presence of eosinophils infiltrating the conjunctival epithelium. Additionally, determination of IgE levels, as well as skin tests to look for specific antigens, can be considered, but the usefulness of these tests is limited.
Treatment / Management
The treatment of vernal keratoconjunctivitis depends on the extent and severity of the disease at the time of presentation. The management may vary from conservative treatment to surgical interventions.
Conservative treatment – The foremost step in managing these patients shall be an attempt to remove any possible allergens in the patient’s surroundings. Cold compresses have a soothing effect.[10] Lid scrubs also form the first line of treatment. Dark goggles are helpful to prevent excess glare and photophobia and help prevent exposure to allergens in the surrounding environment. If the disease is recalcitrant, the patient might need to change from hot, windy areas to cold areas.
Medical treatment – In cases with moderate severity, topical mast cell stabilizers like sodium cromoglycate (2%), sodium nedocromil (2%), lodoxamide are helpful.[18] These can be used with topical antihistaminic eye drops, which act on H1 receptors like olopatadine and alcaftadinie.[19](A1)
Dual-action drops with H-1 blockers and mast cell stabilizers are preferred for moderate to severe diseases. These give the advantage of the immediate onset of action and have a long-term disease-modifying action. Topical nonsteroidal anti-inflammatory agents have also shown a beneficial effect in patients with VKC.[20]
Topical corticosteroids, especially low absorptions steroids like fluorometholone, loteprednol, remexolone, are safe alternatives. Severe cases might need more robust alternatives like dexamethasone or betamethasone. Topical steroids need a quick taper and close monitoring for intraocular pressure.
For patients with recurrent episodes, steroid-sparing agents are a better alternative. Topical immunomodulators like cyclosporin (0.05 to 2%) and tacrolimus (0.1%) are the most commonly used in this class.[2][4] These act by decreasing the inflammatory cytokines. Cyclosporine acts by blocking the T helper two cells, thus blocking lymphocyte proliferation.[21][22] It also works by inhibiting histamine release from mast cells and basophils and reducing the conjunctival fibroblast proliferation and interleukin 1b production.[23](A1)
Systemic treatment may be necessary for a few patients with VKC. These may be particularly useful in patients with a history of an associated atopic disease like atopic dermatitis or asthma. Drugs like montelukast, a leukotriene receptor inhibitor, which acts by inhibiting interleukin-10 helpful in treating asthma, have demonstrated benefits by reducing signs and symptoms among VKC patients.[24] Another monoclonal antibody, dupilumab, which acts by inhibiting interleukin-4 receptors, a drug used to treat atopic dermatitis, has also proven beneficial. Omalizumab, another anti-IgE monoclonal antibody, has been used off-label among recalcitrant cases of VKC.[25][26](B2)
Differential Diagnosis
The close differentials of vernal keratoconjunctivitis include all types of allergic conjunctivitis, including seasonal allergic conjunctivitis, perennial allergic conjunctivitis, atopic keratoconjunctivitis, giant papillary conjunctivitis. Most of these are IgE mediated responses except giant papillary conjunctivitis. None have gender predilection, except AKC and VKC, which are more prevalent among males. History and physical examination often help in distinguishing between these clinical entities.
The closest differential of VKC is AKC. The differentiating features include early age of onset in VKC in early teens compared to 20-50 years in AKC. AKC is more commonly associated with asthma, rhinitis, dermatitis. AKC is more chronic and often results in conjunctival cicatrization, whereas VKC episodes are usually self-limiting and do not result in severe vision-threatening sequelae.[19] VKC is associated with increased goblet cells compared to decrease goblet cells in AKC.
Toxicity and Adverse Effect Management
Close monitoring of intraocular pressures is essential in treating patients with topical corticosteroids. Steroid-induced glaucoma is common among patients on long-term treatment, so intraocular pressures should be assessed on regular follow-up visits.[27] Cataract, though rare, has also been reported as a side effect of steroids among VKC patients.
Prognosis
Vernal keratoconjunctivitis is generally a self-limiting disease. There occurs a spontaneous resolution of symptoms around puberty.[28][29] Usually, the course is benign with no vision-threatening sequelae. Rarely, complications in the form of keratoconus, shield ulcers, corneal scarring, and vascularisation may significantly affect visual acuity. Corneal ulcers are reported in close to 9.7% of patients.[30][31] Complications from unmonitored corticosteroids can result in cataracts, or glaucoma can lead to permanent visual impairment. Some cases may persist into adult age in as many as 12% of cases.
Complications
The ocular complications reported among vernal keratoconjunctivitis patients include steroid-induced cataract, steroid-induced glaucoma, irregular astigmatism, keratoconus, acute hydrops, shield ulcer, central corneal scars, and limbal tissue hyperplasia.
Postoperative and Rehabilitation Care
The treatment of vernal keratoconjunctivitis is mainly based on medical management. VKC episodes are known to be recurrent, with severe, often debilitating itching that prevents the patients from routine work. Thus, it is essential to educate the patients about the natural course of the disease. Steroids remain the mainstay for acute episodes and antihistaminic mast cell stabilizers or immunosuppressants for maintenance therapy. It is also essential to educate patients about the need to monitor intraocular pressures at regular intervals once started on topical steroids. Rarely, rehabilitation therapy in low vision aids might be needed in patients with severe vision-threatening sequelae.[32]
Consultations
Vernal keratoconjunctivitis patients might closely mimic AKC because of the close mimicking presentations between the two entities. Patients with non-resolving symptoms or those severe enough to need steroids must be referred to an ophthalmologist for detailed evaluation and proper management. Patients with a diagnostic dilemma or requiring higher management must be referred to a cornea and ocular surface specialist for expert opinion.[33]
Deterrence and Patient Education
Patients must be educated about the nature of the disease, recurrent episodes, and the self-limiting nature around puberty. They need to be educated to avoid the common allergens and precipitating factors like dust, sunlight, pets, etc.[34] Patients should be recommended to wear an eye cover whenever at risk of exposure to possible allergens in the environment. Additionally, they should be counseled about using their eye drops precisely as instructed. They should also be educated about the potential complications and explained the need for regular follow-ups.[35]
Pearls and Other Issues
Vernal keratoconjunctivitis is a ubiquitous clinical entity in tropical climates. Thus, all ophthalmologists and trained health workers must know this common entity's common presentations and management. Any patients suspected of VKC who are not responding well to antihistaminic or mast cell stabilizers should be referred to an ophthalmologist for consideration for starting a short course of steroids. Recurrent or recalcitrant cases should be considered for long-term use of immunosuppressants and advised regular follow-ups.[36]
Enhancing Healthcare Team Outcomes
Any patient presenting with signs and symptoms of vernal keratoconjunctivitis should be evaluated for the grade and severity of the presentation. A short course of steroids and antihistaminic eye drops can be sufficient in most cases. It is essential to monitor the intraocular pressures in these patients.[37] Patients presenting with recurrent episodes need evaluation and management under the care of an ophthalmologist. But, all physicians, nurses, and optometrists need to know the typical presentations in VKC.[38] The interprofessional healthcare team needs to diagnose these cases early and refer patients for proper management. Nurses, counselors, and pharmacists have a vital role as they need to explain to the patients about lifestyle modifications, the recurrent nature of the disease and ensure proper medications compliance and regular follow-ups with the patients.[39]
Media
(Click Image to Enlarge)
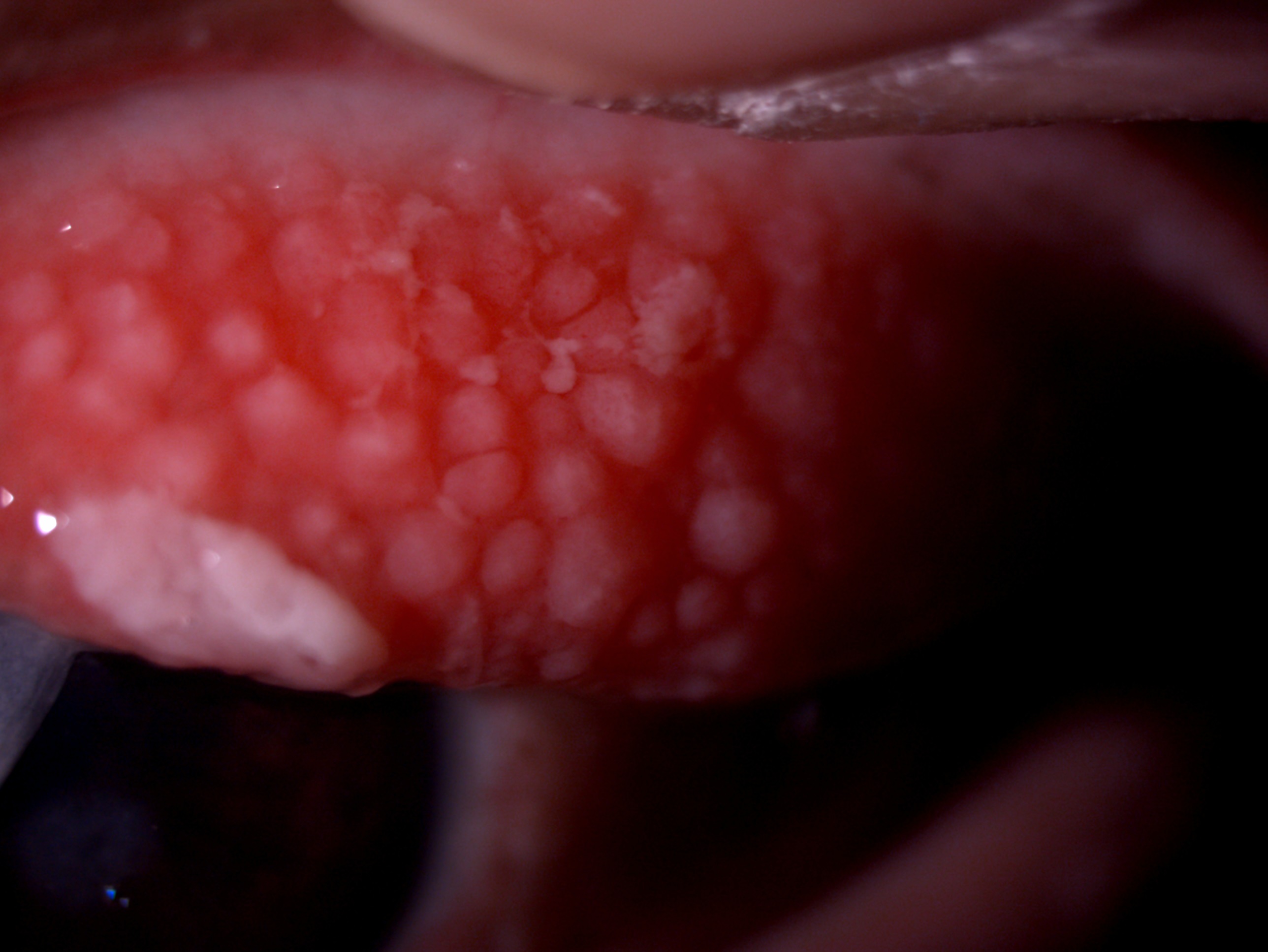
Slit lamp image of the patient depicting cobblestone giant papillae "Contributed by Dr Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS"
(Click Image to Enlarge)

Slit lamp image of the patient depicting macro-papillae in the upper tarsal conjunctiva Contributed by Dr Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS"
(Click Image to Enlarge)
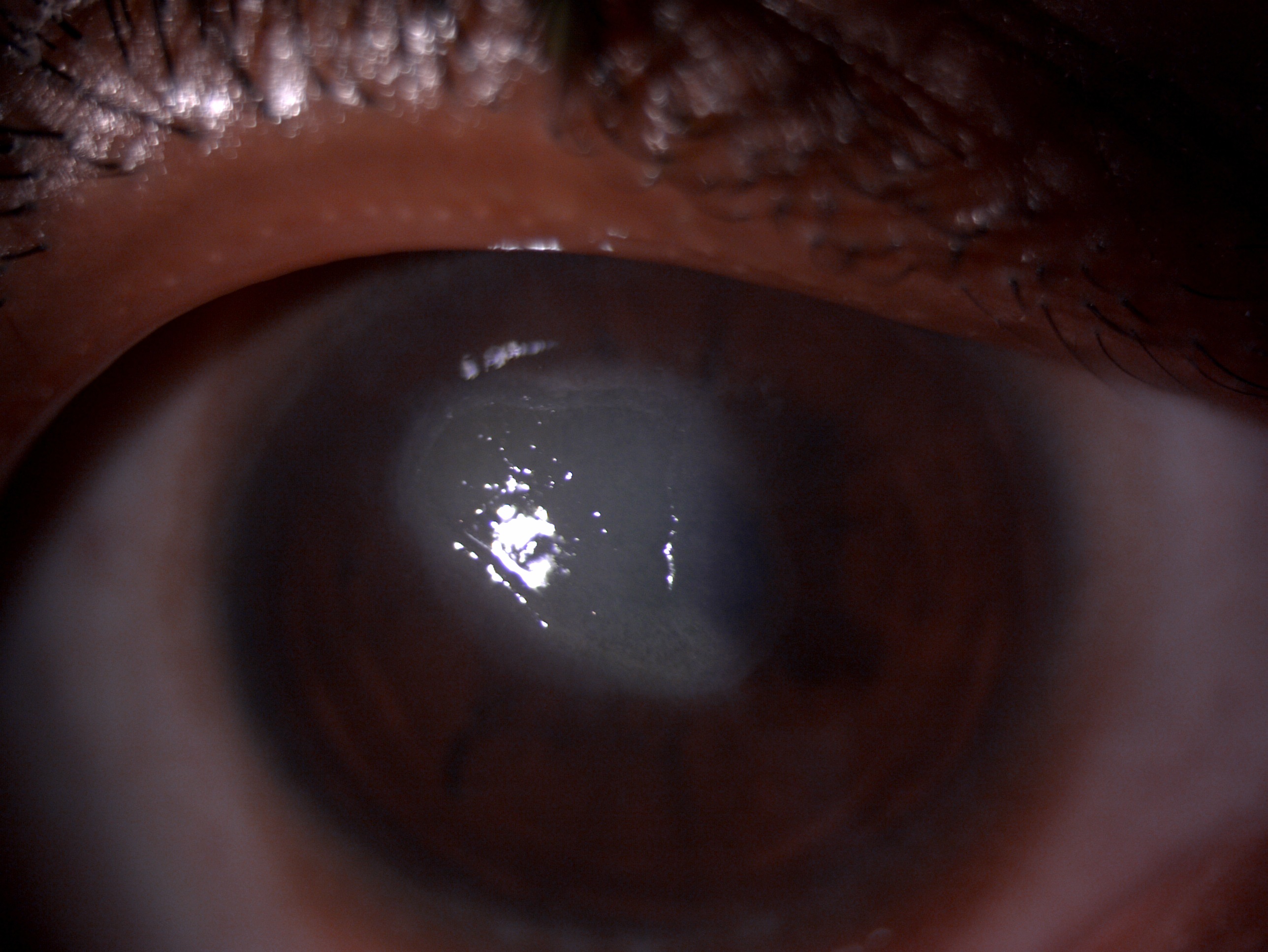
Slit lamp image of the patient depicting central corneal shield ulcer Contributed by Dr Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS"
References
Oray M,Toker E, Tear cytokine levels in vernal keratoconjunctivitis: the effect of topical 0.05% cyclosporine a therapy. Cornea. 2013 Aug; [PubMed PMID: 23676782]
Level 2 (mid-level) evidenceVichyanond P,Kosrirukvongs P, Use of cyclosporine A and tacrolimus in treatment of vernal keratoconjunctivitis. Current allergy and asthma reports. 2013 Jun; [PubMed PMID: 23625179]
Barot RK,Shitole SC,Bhagat N,Patil D,Sawant P,Patil K, Therapeutic effect of 0.1% Tacrolimus Eye Ointment in Allergic Ocular Diseases. Journal of clinical and diagnostic research : JCDR. 2016 Jun; [PubMed PMID: 27504320]
Wan Q,Tang J,Han Y,Wang D,Ye H, Therapeutic Effect of 0.1% Tacrolimus Eye Drops in the Tarsal Form of Vernal Keratoconjunctivitis. Ophthalmic research. 2018; [PubMed PMID: 28803239]
Leonardi A. Management of vernal keratoconjunctivitis. Ophthalmology and therapy. 2013 Dec:2(2):73-88. doi: 10.1007/s40123-013-0019-y. Epub 2013 Sep 7 [PubMed PMID: 25135808]
Alemayehu AM,Yibekal BT,Fekadu SA, Prevalence of vernal keratoconjunctivitis and its associated factors among children in Gambella town, southwest Ethiopia, June 2018. PloS one. 2019; [PubMed PMID: 30998721]
Leonardi A, Vernal keratoconjunctivitis: pathogenesis and treatment. Progress in retinal and eye research. 2002 May; [PubMed PMID: 12052387]
Bremond-Gignac D,Donadieu J,Leonardi A,Pouliquen P,Doan S,Chiambarretta F,Montan P,Milazzo S,Hoang-Xuan T,Baudouin C,Aymé S, Prevalence of vernal keratoconjunctivitis: a rare disease? The British journal of ophthalmology. 2008 Aug; [PubMed PMID: 18356259]
Level 2 (mid-level) evidenceNebbioso M,Zicari AM,Celani C,Lollobrigida V,Grenga R,Duse M, Pathogenesis of Vernal Keratoconjunctivitis and Associated Factors. Seminars in ophthalmology. 2015; [PubMed PMID: 24571721]
Brindisi G,Cinicola B,Anania C,De Castro G,Nebbioso M,Miraglia Del Giudice M,Licari A,Caffarelli C,De Filippo M,Cardinale F,Duse M,Zicari AM, Vernal keratoconjunctivitis: state of art and update on treatment. Acta bio-medica : Atenei Parmensis. 2021 Nov 29; [PubMed PMID: 34842588]
Lai B,Phan K,Lewis N,Shumack S, A rare case of vernal keratoconjunctivitis in a patient with atopic dermatitis treated with tralokinumab. Journal of the European Academy of Dermatology and Venereology : JEADV. 2021 Nov 22; [PubMed PMID: 34807480]
Level 3 (low-level) evidenceZengarini C,Roda M,Schiavi C,Bruni F,Bardazzi F,Bellusci C,Raone B, Successful treatment of severe recalcitrant vernal keratoconjunctivitis and atopic dermatitis associated with elevated IgE levels with omalizumab. Clinical and experimental dermatology. 2021 Nov 3; [PubMed PMID: 34731495]
Bonini S,Bonini S,Lambiase A,Marchi S,Pasqualetti P,Zuccaro O,Rama P,Magrini L,Juhas T,Bucci MG, Vernal keratoconjunctivitis revisited: a case series of 195 patients with long-term followup. Ophthalmology. 2000 Jun; [PubMed PMID: 10857837]
Level 2 (mid-level) evidenceJeng BH, Whitcher JP, Margolis TP. Pseudogerontoxon. Clinical & experimental ophthalmology. 2004 Aug:32(4):433-4 [PubMed PMID: 15281982]
Level 3 (low-level) evidenceTurgut B,Kurt J,Catak O,Demir T, Phthriasis palpebrarum mimicking lid eczema and blepharitis. Journal of ophthalmology. 2009; [PubMed PMID: 20339456]
Level 3 (low-level) evidenceLeonardi A,Lazzarini D,La Gloria Valerio A,Scalora T,Fregona I, Corneal staining patterns in vernal keratoconjunctivitis: the new VKC-CLEK scoring scale. The British journal of ophthalmology. 2018 Oct; [PubMed PMID: 29367201]
Umale RH,Khan MA,Moulick PS,Gupta S,Shankar S,Sati A, A clinical study to describe the corneal topographic pattern and estimation of the prevalence of keratoconus among diagnosed cases of vernal keratoconjunctivitis. Medical journal, Armed Forces India. 2019 Oct; [PubMed PMID: 31719737]
Level 3 (low-level) evidenceBonini S,Schiavone M,Bonini S,Magrini L,Lischetti P,Lambiase A,Bucci MG, Efficacy of lodoxamide eye drops on mast cells and eosinophils after allergen challenge in allergic conjunctivitis. Ophthalmology. 1997 May; [PubMed PMID: 9160033]
Level 1 (high-level) evidenceLa Rosa M,Lionetti E,Reibaldi M,Russo A,Longo A,Leonardi S,Tomarchio S,Avitabile T,Reibaldi A, Allergic conjunctivitis: a comprehensive review of the literature. Italian journal of pediatrics. 2013 Mar 14; [PubMed PMID: 23497516]
D'Angelo G,Lambiase A,Cortes M,Sgrulletta R,Pasqualetti R,Lamagna A,Bonini S, Preservative-free diclofenac sodium 0.1% for vernal keratoconjunctivitis. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2003 Mar; [PubMed PMID: 12644942]
Bielory L,Bonini S,Bonini S, Allergic eye disorders. Clinical allergy and immunology. 2002; [PubMed PMID: 11577546]
Pucci N,Novembre E,Cianferoni A,Lombardi E,Bernardini R,Caputo R,Campa L,Vierucci A, Efficacy and safety of cyclosporine eyedrops in vernal keratoconjunctivitis. Annals of allergy, asthma [PubMed PMID: 12269651]
Level 1 (high-level) evidenceLeonardi A,Borghesan F,DePaoli M,Plebani M,Secchi AG, Procollagens and inflammatory cytokine concentrations in tarsal and limbal vernal keratoconjunctivitis. Experimental eye research. 1998 Jul; [PubMed PMID: 9702183]
Lambiase A,Bonini S,Rasi G,Coassin M,Bruscolini A,Bonini S, Montelukast, a leukotriene receptor antagonist, in vernal keratoconjunctivitis associated with asthma. Archives of ophthalmology (Chicago, Ill. : 1960). 2003 May; [PubMed PMID: 12742837]
Level 3 (low-level) evidencede Klerk TA,Sharma V,Arkwright PD,Biswas S, Severe vernal keratoconjunctivitis successfully treated with subcutaneous omalizumab. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2013 Jun; [PubMed PMID: 23607979]
Level 3 (low-level) evidenceDoan S,Amat F,Gabison E,Saf S,Cochereau I,Just J, Omalizumab in Severe Refractory Vernal Keratoconjunctivitis in Children: Case Series and Review of the Literature. Ophthalmology and therapy. 2017 Jun; [PubMed PMID: 27909980]
Level 2 (mid-level) evidenceTabbara KF, Ocular complications of vernal keratoconjunctivitis. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 1999 Apr; [PubMed PMID: 10321319]
Kumar S, Vernal keratoconjunctivitis: a major review. Acta ophthalmologica. 2009 Mar; [PubMed PMID: 18786127]
De Smedt S,Wildner G,Kestelyn P, Vernal keratoconjunctivitis: an update. The British journal of ophthalmology. 2013 Jan; [PubMed PMID: 23038763]
NEUMANN E,GUTMANN MJ,BLUMENKRANTZ N,MICHAELSON IC, A review of four hundred cases of vernal conjunctivitis. American journal of ophthalmology. 1959 Feb; [PubMed PMID: 13617386]
Level 3 (low-level) evidenceCameron JA, Shield ulcers and plaques of the cornea in vernal keratoconjunctivitis. Ophthalmology. 1995 Jun; [PubMed PMID: 7777308]
Level 2 (mid-level) evidenceAlHarkan DH, Management of vernal keratoconjunctivitis in children in Saudi Arabia. Oman journal of ophthalmology. 2020 Jan-Apr; [PubMed PMID: 32174733]
Chatterjee A, Bandyopadhyay S, Kumar Bandyopadhyay S. Efficacy, Safety and Steroid-sparing Effect of Topical Cyclosporine A 0.05% for Vernal Keratoconjunctivitis in Indian Children. Journal of ophthalmic & vision research. 2019 Oct-Dec:14(4):412-418. doi: 10.18502/jovr.v14i4.5439. Epub 2019 Oct 24 [PubMed PMID: 31875095]
Sacchetti M, Plateroti R, Bruscolini A, Giustolisi R, Marenco M. Understanding Vernal Keratoconjunctivitis: Beyond Allergic Mechanisms. Life (Basel, Switzerland). 2021 Sep 26:11(10):. doi: 10.3390/life11101012. Epub 2021 Sep 26 [PubMed PMID: 34685384]
Level 3 (low-level) evidenceCarr W,Schaeffer J,Donnenfeld E, Treating allergic conjunctivitis: A once-daily medication that provides 24-hour symptom relief. Allergy [PubMed PMID: 27466061]
Tuft SJ,Cree IA,Woods M,Yorston D, Limbal vernal keratoconjunctivitis in the tropics. Ophthalmology. 1998 Aug; [PubMed PMID: 9709763]
Sen P,Jain S,Mohan A,Shah C,Sen A,Jain E, Pattern of steroid misuse in vernal keratoconjunctivitis resulting in steroid induced glaucoma and visual disability in Indian rural population: An important public health problem in pediatric age group. Indian journal of ophthalmology. 2019 Oct; [PubMed PMID: 31546501]
Riad SF,Dart JK,Cooling RJ, Primary care and ophthalmology in the United Kingdom. The British journal of ophthalmology. 2003 Apr; [PubMed PMID: 12642317]
Brown MT,Bussell JK, Medication adherence: WHO cares? Mayo Clinic proceedings. 2011 Apr; [PubMed PMID: 21389250]