Introduction
Primary congenital glaucoma (PCG) is a category of glaucoma characterized by chronic and progressive visual neuropathies that result in irreversible blindness.[1] The classification pertains to childhood glaucoma cases, characterized by unique clinical features with an onset before 18 years of age. Genetic mutations leading to early-onset glaucoma are uncommon yet significant. Childhood glaucoma constitutes a notable category within early-onset glaucoma cases. Diagnosis is generally established through specific clinical criteria, including elevated intraocular pressure (IOP), optic nerve damage, corneal alterations, or visual field defects indicative of optic neuropathy.
PCG involves impairment of the normal drainage of aqueous fluid in the eye, predominantly arising from developmental abnormalities in the trabecular meshwork and anterior chamber angle, resulting in elevated IOP. This untreated pressure damages the optic nerve, resulting in subsequent vision loss. The disease's natural history frequently advances swiftly in the absence of intervention, exhibiting a marked tendency for bilateral involvement. Therefore, timely diagnosis and intervention are crucial for maintaining vision.
The trabecular meshwork of the eye is essential for regulating aqueous humor outflow. This route is either aberrant or obstructed in PCG, resulting in increased IOP.[2] The anterior chamber angle, comprising features such as the Schlemm canal and trabecular meshwork, is essential for proper fluid drainage. Irregularities in these structures in patients with PCG obstruct the correct passage of aqueous humor from the eye, leading to increased IOP, which damages the optic nerve and the retinal nerve fiber layer.[3] Comprehending the anatomical foundation of PCG is essential for clinical assessment and surgical intervention.
Hippocrates first described PCG when he noted abnormally enlarged eyes in infants. The pathogenesis of increased IOP and angle abnormalities were later correlated with this entity. PCG is also referred to as developmental glaucoma, as it might not always be present at birth. Subtypes of PCG correlate with the age of onset of the disease.[4]These subtypes are:
True congenital glaucoma: Also known as newborn glaucoma, this subtype accounts for approximately 25% of cases of PCG. In true congenital glaucoma, the child is either born with ocular enlargement or enlargement of the eyes is noticed within the 1st month of life. The elevation IOP likely occurs during fetal life.[5]
Infantile glaucoma: This subtype of PCG includes patients who manifest symptoms between ages 1 and 36 months and accounts for approximately 65% of patients with PCG.[6]
Juvenile glaucoma: This subtype accounts for approximately 10% of cases of PCG and includes patients with signs of elevated IOP that manifest between 3 years and adulthood.[7]
The Hoskin classification is another classification system for PCG.[8] This system is based on the area of dysgenesis and comprises 3 types. Hoskin type I is referred to as PCG; types II and III are considered secondary congenital glaucoma.
Type I, Trabeculodysgenesis: The defect lies in the development of trabecular meshwork.
Type II, Iridotrabeculodysgenesis: This includes hypoplasia or hyperplasia of the stroma, anomalous iris vessels, or structural defects in the form of coloboma or aniridia.
Type III, Corneotrabeculodysgenesis: This includes complex cases of congenital glaucoma like Axenfield, Rieger, or Peters anomaly.[8]
In conjunction with prominent ophthalmological organizations, the Childhood Glaucoma Research Network (CGRN) has established a consensus-driven classification system for childhood glaucoma.[9] This method classifies childhood glaucoma into primary and secondary glaucoma. Primary pediatric glaucoma encompasses PCG and juvenile open-angle glaucoma (JOAG). PCG, the predominant nonsyndromic variant in infancy, can be further categorized by the age of onset into neonatal or newborn onset (within 1 month of age), infantile (1 month to 2 years of age), or late-onset (older than 2 years of age) classifications.
PCG usually manifests in neonates or infants with symptoms such as buphthalmos (enlarged eyes) and Haab striae (corneal striae).[10] In contrast, JOAG is typically asymptomatic and frequently identified in older children or discovered incidentally during family screenings.[7] Conversely, secondary childhood glaucoma arises from nonacquired ocular defects, nonacquired systemic disorders, acquired conditions, or complications following cataract surgery. This classification facilitates the differentiation of glaucoma subtypes and guides treatment methods, acknowledging the impact of hereditary factors and systemic circumstances on disease progression.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Most cases of PCG are sporadic without a family history of the disease. The significant risk factors for PCG are consanguineous marriage, genetic predisposition, and first-degree relatives (including siblings) with the disease. Approximately 90% of cases belong to this category. PCG tends to be caused by genetic variants that follow a Mendelian inheritance pattern.[11] Another 10% of cases are familial, showing an autosomal recessive inheritance pattern with incomplete penetrance ranging from 40% to 100%. Mutations in the CYP1B1 (cytochrome P450 family 1 subfamily B member 1) gene are the predominant genetic anomalies linked to PCG.[12] This gene is essential for the formation of the trabecular meshwork and the anterior portion of the eye. Additional implicated genes, including LTBP2 (latent transforming growth factor beta binding protein 2), are located next to the GLC3C locus.[13][14] These genetic abnormalities cause a dysfunctional trabecular meshwork, obstructing proper drainage of aqueous fluid and increasing IOP. Several gene loci have been linked to PCG, which includes GLC3A, GLC3B, GLC3C, GLC3D, and GLC3E. Locus GLC3A has been linked to the CYP1B1 gene.[15]
Mutations in this gene are most commonly responsible for autosomal recessively inherited cases.[16] A recent systematic review reported that CYP1B1 was the most common gene mutation reported in the current literature and that the other gene variants related to childhood glaucoma included MYOC (myocilin), LTBP2, FOXC1 (forkhead box C1), PITX2 (paired-like homeodomain transcription factor 2), ANGPT1 (angiopoietin 1) and TEK (or receptor tyrosine kinase).[17]
Epidemiology
PCG is the most prevalent nonsyndromic glaucoma in infants. The incidence and prevalence varies geographically and ethnically.[18] Studies from Western countries have reported incidences ranging from 1/10,000 to 1/30,000 live births.[19] The incidence is reportedly as high as 1/2500 in countries like Saudi Arabia. Slovakian Roma have the greatest incidence at 1/1250.[20] The higher incidence in particular countries and ethnic groups is related to the higher prevalence of consanguineous marriages, particularly in those with frequent cousin-cousin marriages.
Approximately 65% to 80% of cases of PCG are bilateral.[21] A male-to-female ratio of 3:2 has been reported in studies from the United States and Europe.[22] A Japanese study quoted a male-to-female ratio of 6:5 in patients with CYP1BI mutation and 19:2 without the mutation.[23] Several studies have reported that glaucoma accounted for 7% to 18% of children registered in blind schools.[24][25] Asia, India, and Saudi Arabia have a mean presentation age of 3 to 4 months compared to 11 months in Western countries.[4] PCG appears earlier in high-incidence ethnicities.
Pathophysiology
The primary pathophysiologic process in PCG is the defect in the development of the trabecular meshwork and the anterior chamber angle. This hampers the aqueous outflow through the anterior chamber and increases IOP. Barkan proposed that the presence of an imperforate membrane at the angle of the anterior chamber impeded the aqueous outflow; this was later disproved.[26] The obstruction site is trabecular, as opposed to pretrabecular. The isolated maldevelopment of the trabecular meshwork, known as isolated trabeculodysgenesis, is the fundamental disease.[27]
The formation of an immature angle is believed to stem from the developmental arrest of tissues originating from neural crest cells during the third trimester of gestation. The degree of angle abnormalities is contingent upon the point at which angle development is halted.[28] The pathophysiology is believed to result from compacted thick trabecular sheets that merge and inhibit the posterior movement of the iris during the development of the anterior portion. The trabecular sheets position the iris more anteriorly, leading to the iris' characteristic "high" insertion in children with PCG.
The most accepted theory of the pathogenesis of PCG proposed by Anderson states that excessive collagen mesh within the trabecular meshwork prevents normal insertion of the ciliary body and iris. This results in an anteriorly inserted iris root, which in turn causes obstruction of the trabecular meshwork and elevated IOP.[29] Increased IOP leads to the typical symptoms of buphthalmos (enlargement of the eye) and Haab striae (breaks in the Descemet membrane).
Histopathology
Recently, histopathological and electron microscopic studies of PCG have demonstrated obstruction through the outflow pathway.[29] Frequently, the ciliary muscle is inserted high on the trabecular meshwork. Moreover, a detailed framework analysis has shown an excessive amount of collagen in the trabecular meshwork. Other studies have demonstrated fibrillary collagen fibers, elastin fibers, and ground substances in the intervening trabecular meshwork and the canal of Schlemm.[30] The microscopic observations explain the clinical manifestation of elevated IOP and optic nerve impairment.
History and Physical
A family history of glaucoma and a parental consanguineous marriage are essential elements to consider when considering a diagnosis of PCG.[31] The presentation of PCG may be unilateral or bilateral. Elevated IOP tends to be associated with the classic “triad” of symptoms (ie, epiphora, photophobia, and blepharospasm), which can occur because of rapid eye expansion, which can cause buphthalmos. Occasionally, parents report a bluish discoloration of the eyes, abnormally enlarged eyeballs, or sudden whitening of the cornea. The child may also demonstrate reduced visual acuity, myopia, astigmatism, anisometropia, and amblyopia.
The clinical examination must include:[32]
- Fixation of light: The patient’s ability to fixate and follow light should be tested with each eye separately. There may be exotropia due to poor fixation and nystagmus in long-standing cases.
- Sclera: The sclera(e) may appear bluish in color because of high myopia, scleral thinning, and exposure to underlying uveal tissue.[33]
- Cornea: Corneal examination might reveal signs of corneal enlargement or buphthalmos. Normal corneal size from birth to 6 months should be between 9.5 to 11.5 mm. A size of greater than 12 mm should raise the suspicion of glaucoma. A corneal diameter of more than 13 mm in any child older than 6 months indicates corneal enlargement. The slit-lamp examination may reveal horizontal or oblique tears and breaks in the Descemet membrane called Haab striae (see Image. Haab Striae). Another critical finding is corneal edema. This usually starts as epithelial edema and then gradually involves the deeper layers of the cornea, occasionally causing permanent opacities impairing vision profoundly (see Image. Chronic Primary Congenital Glaucoma).[34]
- Anterior chamber: The anterior chamber is usually deep.
- Iris: Iridodonesis, ectropion uvea, hypoplasia, or any atrophic patches may be present.[35]
- Pupil: The pupil may be oval, dilated, and ischemic.
- Lens: The clinician should evaluate for lenticular opacities or lens subluxation due to excessive stretching of zonules.[36]
- Optic disc: This typically demonstrates reversible cupping in the early stages. Later stages may present with an enlarged cup-to-disc ratio or even atrophy.[37][38]
- Intraocular pressure: IOP is usually elevated at presentation and can be measured using a pneumotonometer in the outpatient setting.[39]
Evaluation
The diagnosis of PCG necessitates a thorough and precise ophthalmologic assessment. Timely detection is essential for averting irreparable harm to ocular tissues and maintaining eyesight in children. Any suspicion of congenital glaucoma warrants a thorough and precise evaluation under anesthesia for detailed examination and planning of further management.[40] This evaluation should include an assessment of the following structures and performance of the following studies.
- Cornea: Corneal evaluation, namely for buphthalmos, corneal opacification, and Haab striae, is an essential diagnostic element.[41] The most common cause of buphthalmos is PCG or primary infantile glaucoma. Corneal clouding typically arises from epithelial edema due to increased IOP. In considerable edema, the slit-lamp examination may reveal posterior stromal involvement, signifying prolonged increased IOP. Assessing the horizontal corneal diameter is an essential component of PCG evaluation. The typical ocular diameter in neonates ranges from 9.5 to 10.5 mm, with an expansion >12 mm strongly indicative of PCG. Detailed corneal evaluation should be performed along with measuring corneal diameter with the help of calipers. In addition, a hand-held slit lamp can be used to evaluate the cornea and anterior segment details.
- Ophthalmoscopy: The evaluation of the optic nerve is essential for determining the degree of glaucomatous impairment.[42] Fundoscopy under anesthesia is frequently necessary in pediatric patients. The optic disc may exhibit reversible cupping in the initial phases of primary open-angle glaucoma.[43] However, if the condition advances untreated, the optic cup-to-disc ratio increases, potentially leading to irreversible optic nerve atrophy. Precise documentation of the optic nerve's appearance, preferably with images, is essential for monitoring disease development. Common alterations in the optic disc encompass increased cupping, pallor, and loss of the nerve fiber layer. Any abnormal vessels or other significant findings should be well documented.
- Intraocular pressure: Measuring IOP is fundamental to diagnosing glaucoma.[39] Specialized handheld instruments like the Perkins application, Schiotz tonometer, or Tonopen are frequently utilized in neonates.[44] The Schiotz tonometer, which assesses IOP by indentation principles, is similarly applicable but is less preferred due to its relative inaccuracy relative to applanation techniques. In healthy infants, IOP typically ranges from 10 to 20 mm Hg; in PCG, values can markedly surpass 30 to 40 mm Hg, signifying a substantially impaired aqueous humor outflow and increasing the risk of corneal epithelial edema. The effect of the chosen anesthetic agent on IOP should be kept in mind.
- Gonioscopy: This is a crucial diagnostic procedure used to assess the anterior chamber angle and verify the existence of trabeculodysgenesis.[45] The angle in PCG is frequently atypical, characterized by elevated iris insertion, a flattened or concave iris root, and an underdeveloped trabecular meshwork. This assessment necessitates the utilization of a Koeppe lens or Zeiss gonioprism and is generally conducted under anesthesia in younger children due to inadequate compliance. Gonioscopic findings are essential for distinguishing PCG from other forms of childhood glaucoma or anterior segment dysgenesis syndromes.[35]
- Pachymetry: Corneal thickness measurements can be increased in PCG due to corneal edema. Increased IOP causes stromal edema, resulting in a thicker than normal cornea. Pachymetry measurements might yield significant information, as a thicker cornea may result in inaccurately overestimated IOP readings. Monitoring corneal thickness is crucial throughout the postsurgical follow-up to evaluate edema resolution and better assess IOP measurements.
- Axial length: Ultrasound biometry can be used to ascertain the eye's axial length.[46] The axial length in neonates measures roughly 16 to 18 mm, growing to about 22 mm by age 2. In PCG, increased IOP results in axial elongation, which is associated with the increased severity and duration of pressure. Axial lengths greater than 20 mm at birth or during early infancy strongly indicate congenital glaucoma. Monitoring axial length is essential since excessive elongation may lead to axial myopia and additional visual deterioration.
- Cycloplegic retinoscopy: This procedure is essential for identifying refractive defects, especially myopia and astigmatism, prevalent in PCG due to axial elongation and corneal alterations.[47] Cycloplegic refraction aids in identifying anisometropia, a notable risk factor for the onset of amblyopia. An increased axial length might lead to axial myopia.
Perimetry can be tried to assess peripheral visual field loss in children older than 7 or 8 years who have reasonably good visual acuity, good fixation, and no nystagmus.[48] The SITA-FAST algorithm is preferred in these children. When the child becomes cooperative and eligible for slit lamp examination, optical coherence tomography can be attempted in these children to evaluate the retinal nerve and ganglion cell layer.[49] Handheld and spectral-domain optical coherence tomography [50] are upcoming modalities for assessing the anterior segment, retinal nerve fiber, and ganglion cell layer while evaluating anesthesia. Genetic screening, analysis, and pedigree chart evaluation can be considered in these cases.[51]
Treatment / Management
The management of PCG depends on the age and the severity of the disease at the time of diagnosis. The primary objective of treatment is to lower IOP and maintain optic nerve functionality; increased IOP may result in irreversible vision impairment if not addressed swiftly. Though the mainstay of treatment is surgical intervention, initial medical management may be required as dictated by the clinical presentation.[52]
The preferred treatment for PCG is angle surgery, either goniotomy or trabeculotomy, to alleviate IOP by enhancing aqueous outflow.[53] When angle surgery fails, trabeculectomy with mitomycin C or placement of a device such as the Ahmed® glaucoma valve or Baerveldt® glaucoma drainage device should be attempted.[54] In recalcitrant cases, cycloablation can be attempted using diode cyclophotocaogulation, Nd:YAG therapy, or cryoablation. Topical or oral antiglaucoma drugs are used for decreasing corneal edema, controlling IOP, and improving visualization when performing goniotomy.(B2)
Medical Treatment
This approach is often an initial treatment measure to lower the IOP to decrease corneal edema and improve angle visualization until any surgical procedure is planned or surgical clearance is obtained. Treatment with topical medications decreases aqueous production or increases the aqueous outflow.[55] Medications that decrease aqueous humor production include alpha-adrenergic agonists like brimonidine and apraclonidine, beta blockers like timolol, betaxolol, and levobetaxolol, or carbonic anhydrase inhibitors like brinzolamide. Certain aspects of topical therapy in newborns and children that should be considered include:
- Beta blockers: Beta blockers (eg, timolol, betaxolol) diminish aqueous humor production but should be used cautiously in newborns due to the potential for systemic adverse effects, including bronchospasm and bradycardia.
- Carbonic anhydrase inhibitors: Carbonic anhydrase inhibitors (eg, brinzolamide and acetazolamide) are utilized to reduce aqueous humor production. This class of topical drops is preferred due to their efficacy and safety.
- Prostaglandin analogs: Prostaglandin analogs (eg, latanoprost, travoprost) enhance uveoscleral outflow; nonetheless, their effectiveness in PCG is inconsistent, and they are generally not considered first-line treatments for newborns.
- Brimonidine: This alpha-adrenergic agonist is contraindicated for children younger than 2 years of age because of the potential for central nervous system depression. Brimonidine needs to be used with caution in children younger than 6 years, as it can cross the blood-brain barrier and may cause respiratory depression, apnea, and drowsiness.[56]
- Pilocarpine: Pilocarpine 1% or 2% can be used 2 to 3 times daily and is usually applied preoperatively to improve angle visualization during surgery. Occasionally, pilocarpine is administered postoperatively for a few weeks. (A1)
Surgical Treatment
Surgery is the mainstay of treatment for patients with PCG. The type of surgical procedure depends on the disease severity, cornea clarity, and surgeon's choice and experience. Surgical procedures for PCG can be broadly divided into the following:
Angle procedures
These procedures increase the aqueous outflow by decreasing the resistance in the aqueous pathway due to angle anomaly. The angle procedures are either of 2 types based on the following internal or external approaches:
- Internal approach: Barkan initially described an internal approach using goniotomy.[57] In this technique, a Barkan knife is passed through the limbus into the angle approximately between the root of the iris and Schwalbe ring under a gonioscopic view, which is then extended through 75 degrees. The prerequisite for this procedure is a relatively clear cornea, which enables clear visualization of angle structures. Success rates depend on cornea clarity, the severity of the disease, and the number of lobotomies performed. Studies have reported variable success rates from 70% to 90%.[58] (A1)
- External approach: Smith first described an external approach using trabeculectomy.[59] This is useful in cases of a hazy cornea due to corneal clouding or where goniotomy procedures have failed. This technique makes a conjunctival flap, followed by a partial thickness scleral flap. A scleral incision is made, and the Schlemm canal is exposed. The lower prong of a Harm trabeculotome is passed along the Schlemm canal on the inner side, and the upper prong visible outside serves as a guide. The trabeculotome is then rotated towards the anterior chamber to break the inner wall of the canal. A similar procedure is repeated on the other side through the 12 o'clock opening, thus opening 120 to 180 degrees of the trabeculum. A new modification using a prolene suture has been described as a modification procedure. This allows 360-degree trabeculotomy and the entire angle to be opened in a single sitting.[60] The studies have reported a reduction in IOP by 75% to 90% following trabeculotomy.[61] (B2)
Filtration procedures
The following filtration procedures may be utilized:
- Trabeculectomy: This was first described by Cairns.[62] Isolated trabeculectomy procedures are not often performed in PCG due to limited success rates and exaggerated healing responses experienced in children. Antifibrotic agents like mitomycin-C and 5-fluorouracil have shown promising results in improving success rates. Success rates from 52% to 82% have been reported following antimetabolite-assisted trabeculectomy procedures in PCG patients.[63] (B2)
- Deep sclerectomy: This procedure involves elevating a partial-thickness scleral flap and removing the external portion of the Schlemm canal and outer part of the trabecular meshwork, including juxtacanalicular tissue, without fully penetrating the eye, thus less risk of hypotony and endophthalmitis.[64]
- Glaucoma drainage devices (GDD): The role of GDD in PCG as a primary procedure is limited. GDD implantation in PCG is considered in cases where primary angle procedures have failed or in advanced refractory cases. Studies have shown a reduction of IOP by 28% to 49% following 1-year postsurgery.[65] These devices establish an artificial drainage pathway for the aqueous humor, redirecting it from the anterior chamber to an external reservoir (see Image. Glaucoma Drainage Device). Although GDDs effectively reduce IOP, they are linked to problems including tube migration, erosion, and infection. (B2)
Combined trabeculotomy and trabeculectomy
This procedure is attempted when the previous trabeculectomy has failed or cannulating the Schlemm canal is difficult.[66] In this, the trabeculectomy is added to the trabeculectomy.[67] A block of tissue is removed from the sclera aided by surgical peripheral iridectomy. Care is necessary when using mitomycin C.
Cyclodestructive procedures
This procedure is reserved for eyes with poor or nil visual prognosis. These approaches selectively abrogate the ciliary body to diminish aqueous fluid generation. Due to their aggressive character and the associated risks of consequences, including hypotony or retinal detachment, they are typically designated for advanced or refractory cases. The success rate in these cases is close to 30% only.[68] A newer modification in the form of a micropulse transscleral diode laser is a better and safer alternative.[69](B2)
Differential Diagnosis
The differential diagnoses of PCG can be remembered by the mnemonic STUMPED, which includes the following conditions:
- S: Sclerocornea, congenital hereditary stromal dystrophy.[70] This uncommon disorder is characterized by corneal opacification and may be mistaken for PCG. A flattened cornea with no concomitant elevation in IOP or optic nerve impairment defines Sclerocornea.
- T: Trauma, tears in Descemet membrane or endothelial (ie, from forceps).
- U: Ulcer [71] caused by various factors, including viral, fungal, bacterial, neurotrophic, and pythium [72][73]
- M: Metabolic disorders, eg, mucolipidoses, mucopolysaccharidosis, tyrisinosis
- P: Peters anomaly, an uncommon disorder characterized by central corneal opacity and adherence of the iris to the cornea, may manifest with glaucoma; the principal anomaly is the corneal-lenticular contact [74]
- E: Endothelial dystrophy, congenital hereditary endothelial dystrophy, posterior polymorphous dystrophy, Fuchs dystrophy [75]
- D: Dermoid. [76]
Other significant differentials which should be kept in mind include:
- Interstitial keratitis
- High myopia
- Megalocornea
- Corneal abrasion
- Messman dystrophy
- Reis-Buckler dystrophy
- Retinoblastoma
- Retinopathy of prematurity
- Persistent primary hyperplastic vitreous
- Traumatic glaucoma [77]
- Congenital rubella syndrome
- Sturge-Weber syndrome
- Aniridia
- Optic disc pit
- Optic atrophy [78]
- Coloboma
Prognosis
The overall prognosis in PCG depends on the time and severity of presentation, age of presentation, and corneal clarity. Early diagnosis and management are the keys to good visual potential in these cases. Corneal edema and optic nerve head changes are reversible if timely intervention is done. Children need to be screened for any associated refractive errors from axial elongation of the eyeball and appropriately managed for the same. IOPs and optic nerve heads need evaluation at regular intervals for life. Late presentations can lead to sight-threatening complications.
A study from the United States showed a lack of progression following adequate treatment in 90.3% at 1 year, 83.1% at 5 years, 70.8% at 10 years, and 58.3% at 34 years. Thus highlighting the importance of appropriate management and follow-ups for these patients.[79] Another study showed that angle procedures were 90% successful among patients presenting between 2 months and 1 year of age, compared to 50% among those presenting either in infantile or late-onset or late-recognized cases.[80]
Complications
Complications in PCG can be related to disease, surgery, or anesthesia. Patients having delayed presentations may develop significant visual impairment, glaucomatous optic atrophy, or visual field defects. Corneal and Haab striae development may later lead to permanent opacification of the cornea, thus significantly hampering vision. Stretching the eyeball due to elevated pressures may lead to axial myopia or astigmatism. Refractive correction should be provided with lifelong follow-up, as untreated cases can develop refractive amblyopia.[81] Further, these patients are at risk of lens dislocation or retinal complications.
Surgical Complications
Surgical complications include:
- Hyphema
- Shallow anterior chamber [82]
- Peripheral anterior synechiae
- Iridodialysis
- Cyclodialysis [83]
- Cataract [84][85]
- Epithelial ingrowth
- Choroidal detachment
- Retinal detachment
- Phthisis bulbi
Filtering Procedure-Related Complications
Adverse effects of filtering procedures include:
- Over or under-filtration
- Blebitis
- Vitreous loss
- Scleral collapse
- Scleral flap leak
- Tube lens touch
- Endothelial decompensation from tube cornea touch
- Tube erosion
- Implant migration
- Diplopia from implant-related restrictions
- Endophthalmitis
Cyclodestructive Procedure-Related Complications
Complications associated with cyclodestructive procedures include:
- Hypotony
- Retinal detachment [86]
- Phthisis
Anesthesia-Related Complications
Complications associated with anesthesia include:
- Oculocardiac reflex
- Anaphylaxis
- Malignant hyperthermia
- Cardiovascular collapse
- Hepatic porphyria
- Hypoxic brain injury
Postoperative and Rehabilitation Care
The children undergoing surgery should be started on topical steroids, either prednisolone 1% or dexamethasone 0.1% for 1 week each using an 8/7/6/5/4/3/2/1 tapering dosage. In addition, a topical antibiotic in the form of tobramycin 0.3% or 0.3% moxifloxacin or gatifloxacin 4 times per day for 20 days should be supplemented to prevent secondary infection. These patients will need close follow-ups postsurgery to look for signs of hypotony, inflammation, or infection. Moreover, the IOP needs to be recorded every 3 to 4 months for at least 2 years postsurgery.
Cycloplegic refraction will be needed every 6 months for these patients. Moreover, lifelong regular follow-up every 6 months is needed for IOP monitoring and early detection of any surgery-related complications. Cases of failing angle or filtration surgery should be counseled for the need for GDD and the risk of subsequent failure, amblyopia, blindness, and phthisis bulbs.
Consultations
Any child with clinical suspicion of PCG presenting to the outpatient department must be evaluated meticulously by an ophthalmologist. The general ophthalmologist should start the child on antiglaucoma medications and refer the child to a glaucoma specialist to confirm diagnosis and targeted treatment. The glaucoma specialist should decide for evaluation under anesthesia and surgical intervention of the child in the form of goniotomy or trabeculectomy.
Deterrence and Patient Education
PCG is a treatable disease, provided the condition is diagnosed early and timely intervention is done. Thus, educating the parents, general clinicians, and optometrists is very important to ensure early suspicion and timely referral to ophthalmologists. Any signs of enlarged eyes, watering, redness, or shying away from light should be reported to the healthcare team as soon as possible. Proper parental education about early signs and symptoms can prevent treatable blindness from PCG.
Management options should be explained to the parents, and a well-informed decision should be made. It is also essential to create awareness about the need for regular follow-ups and compliance with the treatment advised. The need for follow-up with optometrists for regular refraction should also be emphasized. In patients with low vision, appropriate mobilization for low-vision clinics should be ensured at an early age to help the child and parents understand the need for lifestyle and educational modifications.
Regular IOP and visual acuity assessment is essential, as glaucoma is a progressive condition that may reoccur despite successful surgical intervention. Parents must recognize that numerous procedures may be necessary to manage IOP throughout the child's life and that refractive defects, such as myopia or astigmatism, are prevalent in individuals with PCG, necessitating continuous use of corrective lenses and vision treatment to avert amblyopia.
Healthcare personnel must emphasize the significance of compliance with medical treatments, particularly recommended antiglaucoma drugs and postoperative care protocols. Should complications occur, including erythema, discomfort, or an abrupt deterioration in vision, parents must be instructed to pursue immediate medical attention, as these manifestations may signify surgical failure or the necessity for re-intervention. The significance of genetic counseling in high-risk families warrants discussion since comprehending inherited risk can guide future family planning and facilitate early screening for subsequent children.
Pearls and Other Issues
PCG is a vision-threatening ocular pathology in the pediatric age group. Children are highly vulnerable due to lack of communication, difficulty performing an examination, compliance with treatment, and regular follow-up. Any pediatric patient presenting to the outpatient department with lacrimation, photophobia, blepharospasm, buphthalmos, and corneal clouding should undergo a detailed clinical evaluation to diagnose the condition. While managing these children, all the other differentials must be carefully ruled out for targeted treatment and solving the eye with good visual outcomes. The parents should be counseled regarding the importance of genetic and family screening in these cases. Angle and filtration surgery are the treatment of choice for good anatomical and visual outcomes.
Regarding surgical outcomes, goniotomy and trabeculotomy are notably effective in managing IOP when executed promptly, particularly in newborns younger than 1 year. Surgical success rates diminish with advanced corneal clouding or substantial optic nerve cupping at presentation. Consequently, prompt referral to a glaucoma specialist is imperative. A significant concern is the chronic nature of PCG, necessitating continuous monitoring for disease recurrence and the care of possible consequences, including refractive errors and amblyopia.
Genetic counseling is essential, especially in populations with a high incidence of consanguineous marriages. A considerable percentage of PCG cases are transmitted in an autosomal recessive manner, involving mutations in genes like CYP1B1. Consequently, comprehending the genetic foundation of the condition is crucial for family planning, early identification in subsequent pregnancies, and providing prenatal diagnostic tests where feasible.
Acknowledging the significance of multidisciplinary care is a crucial insight for doctors. PCG management necessitates contributions from ophthalmologists, pediatricians, geneticists, and low-vision experts to guarantee optimal long-term patient outcomes. Low-vision rehabilitation and early participation in visual therapy programs can markedly improve the quality of life for children with remaining visual impairment posttreatment.
Enhancing Healthcare Team Outcomes
Early diagnosis and timely intervention are the key components for successfully managing patients with PCG. The entire healthcare team needs to be aware of their roles whenever they come in contact with these patients. A high level of suspicion by the optometrists, staff nurses, and general physicians in any patient with enlarged eyeballs or excessive watering, hazy corneas, abnormal congestion, photophobia, or high myopias in infancy or early childhood should be maintained. A strategic approach is crucial to optimize treatment plans, minimize adverse effects, and limit functional and anatomical glaucomatous damage.
A relatively lower threshold is maintained when referring these children to ophthalmologists for confirmation of diagnosis. Educating parents about the need for immediate referrals and that delay in treatment can lead to lifelong ocular comorbidities and visual compromise is also essential. Ophthalmologists play an important role in diagnosing and treating these cases. An evaluation under anesthesia should be planned for investigation, and any surgical intervention should be performed if needed. Close interprofessional communication for examination by pediatrician, anesthetist, and ophthalmologist with the help of staff nurses and the counselor will be required for successful outcomes in these patients.
Effective communication among all team members is crucial for enhancing patient outcomes. Interprofessional teamwork, encompassing regular case discussions, the exchange of patient information, and synchronized follow-up schedules, guarantees that no facet of the patient's treatment is neglected. This method aids in averting disease recurrence, managing surgical complications promptly, and delivering comprehensive treatment that considers the ocular dimensions of PCG and the child's developmental, educational, and emotional requirements.
Media
(Click Image to Enlarge)

Haab Striae. Slit lamp image of the child depicting megalocornea and horizontal oblique breaks in descemet membrane suggestive of Haab striae secondary to raised intraocular pressure and stretching of the cornea.
Contributed by K Kaur, MD
(Click Image to Enlarge)

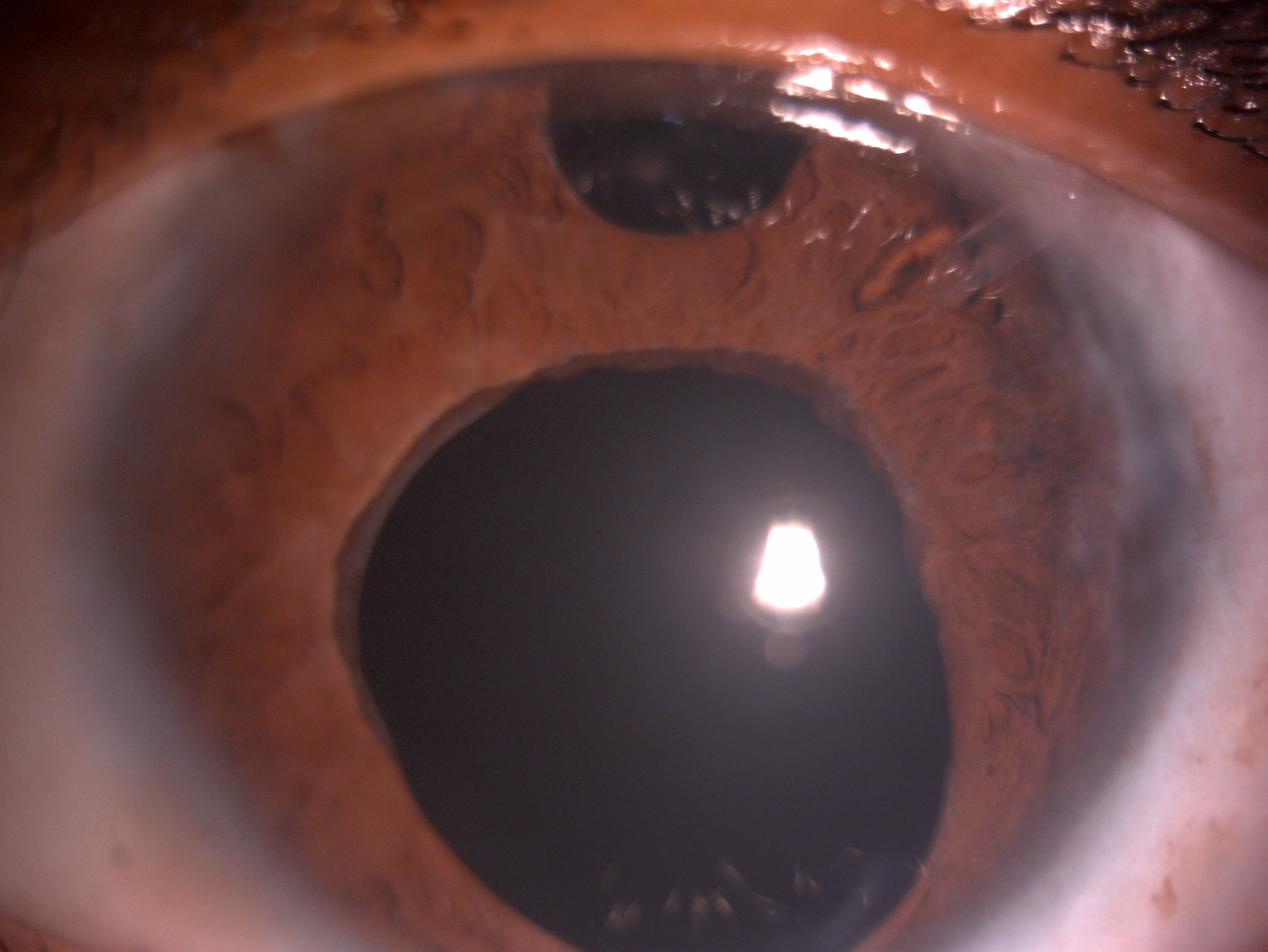
Chronic Primary Congenital Glaucoma. Slit lamp image of the child depicting mild conjunctival congestion, lower tarsal conjunctival hyperemia, megalocornea, near total corneal opacification with deep stromal vascularization suggestive of long-standing chronic primary congenital glaucoma.
Contributed by K Kaur, MD
(Click Image to Enlarge)
Glaucoma Drainage Device. Slit lamp image of the child depicting megalocornea, tube shunt in the anterior chamber, surgical peripheral iridectomy, dilated ischemic pupil, and aphakia post glaucoma drainage device for recalcitrant primary congenital glaucoma refractory to angle and filtration surgery.
Contributed by K Kaur, MD
References
Reis LM, Seese SE, Costakos D, Semina EV. Congenital anterior segment ocular disorders: Genotype-phenotype correlations and emerging novel mechanisms. Progress in retinal and eye research. 2024 Sep:102():101288. doi: 10.1016/j.preteyeres.2024.101288. Epub 2024 Aug 2 [PubMed PMID: 39097141]
Torné O, Oikawa K, Teixeira LBC, Kiland JA, McLellan GJ. Trabecular Meshwork Abnormalities in a Model of Congenital Glaucoma Due to LTBP2 Mutation. Investigative ophthalmology & visual science. 2024 Oct 1:65(12):28. doi: 10.1167/iovs.65.12.28. Epub [PubMed PMID: 39432401]
Gurpinar A, Niyaz L, Ariturk N. Long-term follow-up results and visual outcomes of childhood glaucoma in the black sea region of turkey. International ophthalmology. 2024 Aug 29:44(1):360. doi: 10.1007/s10792-024-03275-7. Epub 2024 Aug 29 [PubMed PMID: 39207647]
Badawi AH, Al-Muhaylib AA, Al Owaifeer AM, Al-Essa RS, Al-Shahwan SA. Primary congenital glaucoma: An updated review. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2019 Oct-Dec:33(4):382-388. doi: 10.1016/j.sjopt.2019.10.002. Epub 2019 Nov 7 [PubMed PMID: 31920449]
Kaushik S, Senthil S, Gupta V, Balekudaru S, Dubey S, Ali H, Mandal AK, Indian Childhood Glaucoma Study (ICGS) Group. Profile of Newly Diagnosed Childhood Glaucoma in India: Indian Childhood Glaucoma Study (ICGS) Group 1. Ophthalmology. Glaucoma. 2024 Jan-Feb:7(1):54-65. doi: 10.1016/j.ogla.2023.07.004. Epub 2023 Jul 15 [PubMed PMID: 37454975]
Choe S, Kim YK, Ha A. Nationwide incidence of and risk factors for undergoing incisional glaucoma surgery following infantile cataract surgery. Scientific reports. 2024 Jul 15:14(1):16286. doi: 10.1038/s41598-024-66559-z. Epub 2024 Jul 15 [PubMed PMID: 39009616]
Selvan H, Gupta S, Wiggs JL, Gupta V. Juvenile-onset open-angle glaucoma - A clinical and genetic update. Survey of ophthalmology. 2022 Jul-Aug:67(4):1099-1117. doi: 10.1016/j.survophthal.2021.09.001. Epub 2021 Sep 16 [PubMed PMID: 34536459]
Level 3 (low-level) evidenceHoskins HD Jr, Shaffer RN, Hetherington J. Anatomical classification of the developmental glaucomas. Archives of ophthalmology (Chicago, Ill. : 1960). 1984 Sep:102(9):1331-6 [PubMed PMID: 6477252]
Pan Y, Iwata T. Exploring the Genetic Landscape of Childhood Glaucoma. Children (Basel, Switzerland). 2024 Apr 9:11(4):. doi: 10.3390/children11040454. Epub 2024 Apr 9 [PubMed PMID: 38671671]
Mandal AK, Raghavachary C, Peguda HK. Haab's Striae. Ophthalmology. 2017 Jan:124(1):11. doi: 10.1016/j.ophtha.2016.07.002. Epub [PubMed PMID: 27993263]
Knight LSW, Ruddle JB, Taranath DA, Goldberg I, Smith JEH, Gole G, Chiang MY, Willett F, D'Mellow G, Breen J, Qassim A, Mullany S, Elder JE, Vincent AL, Staffieri SE, Kearns LS, Mackey DA, Luu S, Siggs OM, Souzeau E, Craig JE. Childhood and Early Onset Glaucoma Classification and Genetic Profile in a Large Australasian Disease Registry. Ophthalmology. 2021 Nov:128(11):1549-1560. doi: 10.1016/j.ophtha.2021.04.016. Epub 2021 Apr 20 [PubMed PMID: 33892047]
Haddad A, Ait Boujmia OK, El Maaloum L, Dehbi H. Meta-analysis of CYP1B1 gene mutations in primary congenital glaucoma patients. European journal of ophthalmology. 2021 Nov:31(6):2796-2807. doi: 10.1177/11206721211016308. Epub 2021 May 21 [PubMed PMID: 34020567]
Level 1 (high-level) evidenceAli M, McKibbin M, Booth A, Parry DA, Jain P, Riazuddin SA, Hejtmancik JF, Khan SN, Firasat S, Shires M, Gilmour DF, Towns K, Murphy AL, Azmanov D, Tournev I, Cherninkova S, Jafri H, Raashid Y, Toomes C, Craig J, Mackey DA, Kalaydjieva L, Riazuddin S, Inglehearn CF. Null mutations in LTBP2 cause primary congenital glaucoma. American journal of human genetics. 2009 May:84(5):664-71. doi: 10.1016/j.ajhg.2009.03.017. Epub 2009 Apr 9 [PubMed PMID: 19361779]
Suri F, Yazdani S, Elahi E. LTBP2 knockdown and oxidative stress affect glaucoma features including TGFβ pathways, ECM genes expression and apoptosis in trabecular meshwork cells. Gene. 2018 Oct 5:673():70-81. doi: 10.1016/j.gene.2018.06.038. Epub 2018 Jun 14 [PubMed PMID: 29908281]
Sarfarazi M, Akarsu AN, Hossain A, Turacli ME, Aktan SG, Barsoum-Homsy M, Chevrette L, Sayli BS. Assignment of a locus (GLC3A) for primary congenital glaucoma (Buphthalmos) to 2p21 and evidence for genetic heterogeneity. Genomics. 1995 Nov 20:30(2):171-7 [PubMed PMID: 8586416]
Level 3 (low-level) evidenceFan BJ, Wiggs JL. Glaucoma: genes, phenotypes, and new directions for therapy. The Journal of clinical investigation. 2010 Sep:120(9):3064-72. doi: 10.1172/JCI43085. Epub 2010 Sep 1 [PubMed PMID: 20811162]
Kumar A, Han Y, Oatts JT. Genetic changes and testing associated with childhood glaucoma: A systematic review. PloS one. 2024:19(2):e0298883. doi: 10.1371/journal.pone.0298883. Epub 2024 Feb 22 [PubMed PMID: 38386645]
Level 1 (high-level) evidenceLim SH, Tran-Viet KN, Yanovitch TL, Freedman SF, Klemm T, Call W, Powell C, Ravichandran A, Metlapally R, Nading EB, Rozen S, Young TL. CYP1B1, MYOC, and LTBP2 mutations in primary congenital glaucoma patients in the United States. American journal of ophthalmology. 2013 Mar:155(3):508-517.e5. doi: 10.1016/j.ajo.2012.09.012. Epub 2012 Dec 4 [PubMed PMID: 23218701]
Tamçelik N, Atalay E, Bolukbasi S, Çapar O, Ozkok A. Demographic features of subjects with congenital glaucoma. Indian journal of ophthalmology. 2014 May:62(5):565-9. doi: 10.4103/0301-4738.126988. Epub [PubMed PMID: 24881602]
Level 2 (mid-level) evidenceGenĉík A. Epidemiology and genetics of primary congenital glaucoma in Slovakia. Description of a form of primary congenital glaucoma in gypsies with autosomal-recessive inheritance and complete penetrance. Developments in ophthalmology. 1989:16():76-115 [PubMed PMID: 2676634]
Yu-Wai-Man C, Arno G, Brookes J, Garcia-Feijoo J, Khaw PT, Moosajee M. Primary congenital glaucoma including next-generation sequencing-based approaches: clinical utility gene card. European journal of human genetics : EJHG. 2018 Nov:26(11):1713-1718. doi: 10.1038/s41431-018-0227-y. Epub 2018 Aug 8 [PubMed PMID: 30089822]
deLuise VP, Anderson DR. Primary infantile glaucoma (congenital glaucoma). Survey of ophthalmology. 1983 Jul-Aug:28(1):1-19 [PubMed PMID: 6353647]
Level 3 (low-level) evidenceOhtake Y, Tanino T, Suzuki Y, Miyata H, Taomoto M, Azuma N, Tanihara H, Araie M, Mashima Y. Phenotype of cytochrome P4501B1 gene (CYP1B1) mutations in Japanese patients with primary congenital glaucoma. The British journal of ophthalmology. 2003 Mar:87(3):302-4 [PubMed PMID: 12598442]
Level 3 (low-level) evidenceAlabdulwahhab KM, Ahmad MS. Visual Impairment and Blindness in Saudi Arabia's School for the Blind: A Cross-Sectional Study. Clinical optometry. 2020:12():169-173. doi: 10.2147/OPTO.S265293. Epub 2020 Oct 7 [PubMed PMID: 33117027]
Level 2 (mid-level) evidenceSouma T, Tompson SW, Thomson BR, Siggs OM, Kizhatil K, Yamaguchi S, Feng L, Limviphuvadh V, Whisenhunt KN, Maurer-Stroh S, Yanovitch TL, Kalaydjieva L, Azmanov DN, Finzi S, Mauri L, Javadiyan S, Souzeau E, Zhou T, Hewitt AW, Kloss B, Burdon KP, Mackey DA, Allen KF, Ruddle JB, Lim SH, Rozen S, Tran-Viet KN, Liu X, John S, Wiggs JL, Pasutto F, Craig JE, Jin J, Quaggin SE, Young TL. Angiopoietin receptor TEK mutations underlie primary congenital glaucoma with variable expressivity. The Journal of clinical investigation. 2016 Jul 1:126(7):2575-87. doi: 10.1172/JCI85830. Epub 2016 Jun 6 [PubMed PMID: 27270174]
BARKAN O. Pathogenesis of congenital glaucoma: gonioscopic and anatomic observation of the angle of the anterior chamber in the normal eye and in congenital glaucoma. American journal of ophthalmology. 1955 Jul:40(1):1-11 [PubMed PMID: 14388087]
Mandal AK, Chakrabarti D. Update on congenital glaucoma. Indian journal of ophthalmology. 2011 Jan:59 Suppl(Suppl1):S148-57. doi: 10.4103/0301-4738.73683. Epub [PubMed PMID: 21150027]
Mandal AK, Chakrabarti D, Gothwal VK. Approach to primary congenital glaucoma: A perspective. Taiwan journal of ophthalmology. 2023 Oct-Dec:13(4):451-460. doi: 10.4103/tjo.TJO-D-23-00104. Epub 2023 Oct 19 [PubMed PMID: 38249492]
Level 3 (low-level) evidenceTawara A, Inomata H. Developmental immaturity of the trabecular meshwork in congenital glaucoma. American journal of ophthalmology. 1981 Oct:92(4):508-25 [PubMed PMID: 7294114]
Level 3 (low-level) evidenceGarcía-Antón MT, Salazar JJ, de Hoz R, Rojas B, Ramírez AI, Triviño A, Aroca-Aguilar JD, García-Feijoo J, Escribano J, Ramírez JM. Goniodysgenesis variability and activity of CYP1B1 genotypes in primary congenital glaucoma. PloS one. 2017:12(4):e0176386. doi: 10.1371/journal.pone.0176386. Epub 2017 Apr 27 [PubMed PMID: 28448622]
Papadopoulos M, Cable N, Rahi J, Khaw PT, BIG Eye Study Investigators. The British Infantile and Childhood Glaucoma (BIG) Eye Study. Investigative ophthalmology & visual science. 2007 Sep:48(9):4100-6 [PubMed PMID: 17724193]
Mandal AK. Acute Corneal Hydrops in Children with Primary Infantile Glaucoma: A Report of 31 Cases over 23 Years at the LVPEI. PloS one. 2016:11(6):e0156108. doi: 10.1371/journal.pone.0156108. Epub 2016 Jun 1 [PubMed PMID: 27249057]
Level 3 (low-level) evidenceDrechsler J, Lee A, Maripudi S, Kueny L, Levin MR, Saeedi OJ, Bazemore M, Karwoski B, Birdsong R, Martinez C, Jaafar MS, Yousaf S, Ahmed ZM, Madigan WP, Alexander JL. Corneal Structural Changes in Congenital Glaucoma. Eye & contact lens. 2022 Jan 1:48(1):27-32. doi: 10.1097/ICL.0000000000000844. Epub [PubMed PMID: 34608027]
Gupta S, Mahalingam K, Singh A, Selvan H, Somarajan BI, Gupta V. Posterior corneal morphological changes in primary congenital glaucoma. Indian journal of ophthalmology. 2022 Jul:70(7):2571-2577. doi: 10.4103/ijo.IJO_317_22. Epub [PubMed PMID: 35791159]
Sihota R, Mahalingam K, Maurya AK, Sharma A, Bukke AN, Dada T. Primary congenital glaucoma: An iridotrabeculodysgenesis? Indian journal of ophthalmology. 2024 Mar 1:72(3):328-334. doi: 10.4103/IJO.IJO_370_23. Epub 2023 Dec 15 [PubMed PMID: 38099353]
Walton DS. Chronic newborn primary congenital glaucoma with secondary lens subluxation. Journal of pediatric ophthalmology and strabismus. 2009 Jul-Aug:46(4):200, 231. doi: 10.3928/01913913-20090706-02. Epub [PubMed PMID: 19645394]
Snehi S, Singh AK, Kaushik S. Acquired Lens Zonular Loss with Bean Pot Optic Disc Cupping in Congenital Glaucoma. Ophthalmology. Glaucoma. 2023 Mar-Apr:6(2):159. doi: 10.1016/j.ogla.2023.01.001. Epub 2023 Jan 27 [PubMed PMID: 36710134]
Gupta V, James MK, Singh A, Kumar S, Gupta S, Sharma A, Sihota R, Kennedy DJ. Differences in Optic Disc Characteristics of Primary Congenital Glaucoma, Juvenile, and Adult Onset Open Angle Glaucoma Patients. Journal of glaucoma. 2016 Mar:25(3):239-43. doi: 10.1097/IJG.0000000000000154. Epub [PubMed PMID: 25265002]
Level 2 (mid-level) evidenceSihota R, Sidhu T, Agarwal R, Sharma A, Gupta A, Sethi A, Dada T, Pandey V. Evaluating target intraocular pressures in primary congenital glaucoma. Indian journal of ophthalmology. 2021 Aug:69(8):2082-2087. doi: 10.4103/ijo.IJO_3473_20. Epub [PubMed PMID: 34304183]
Beck AD. Diagnosis and management of pediatric glaucoma. Ophthalmology clinics of North America. 2001 Sep:14(3):501-12 [PubMed PMID: 11705150]
Ramyashri S, Senthil S. Effect of Haab's striae on corneal parameters in primary congenital glaucoma. Indian journal of ophthalmology. 2024 Nov 1:72(11):1679-1680. doi: 10.4103/IJO.IJO_2958_23. Epub 2024 Oct 26 [PubMed PMID: 39462935]
Sihota R, Sidhu T, Dada T. The role of clinical examination of the optic nerve head in glaucoma today. Current opinion in ophthalmology. 2021 Mar 1:32(2):83-91. doi: 10.1097/ICU.0000000000000734. Epub [PubMed PMID: 33470671]
Level 3 (low-level) evidenceEly AL, El-Dairi MA, Freedman SF. Cupping reversal in pediatric glaucoma--evaluation of the retinal nerve fiber layer and visual field. American journal of ophthalmology. 2014 Nov:158(5):905-15. doi: 10.1016/j.ajo.2014.07.030. Epub 2014 Jul 25 [PubMed PMID: 25068638]
Brusini P, Salvetat ML, Zeppieri M. How to Measure Intraocular Pressure: An Updated Review of Various Tonometers. Journal of clinical medicine. 2021 Aug 27:10(17):. doi: 10.3390/jcm10173860. Epub 2021 Aug 27 [PubMed PMID: 34501306]
Magan T, Tanner A, Fajardo-Sanchez J, Lim KS, Goyal S, Rodrigues I, Amaya L, Trikha S, Kulkarni A, Hammond C, Lascaratos G, Yu-Wai-Man C. Long-term outcomes in Primary congenital glaucoma, aniridia and anterior segment dysgenesis. European journal of ophthalmology. 2022 Sep:32(5):2920-2927. doi: 10.1177/11206721211073208. Epub 2022 Jan 10 [PubMed PMID: 35001688]
Janssens R, van Rijn LJ, Eggink CA, Jansonius NM, Janssen SF. Ultrasound biomicroscopy of the anterior segment in patients with primary congenital glaucoma: a review of the literature. Acta ophthalmologica. 2022 Sep:100(6):605-613. doi: 10.1111/aos.15082. Epub 2021 Dec 22 [PubMed PMID: 34939345]
Moore DB, Ben Zion I, Neely DE, Roberts GJ, Sprunger DT, Plager DA. Refractive outcomes with secondary intraocular lens implantation in children. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2009 Dec:13(6):551-4. doi: 10.1016/j.jaapos.2009.09.012. Epub [PubMed PMID: 20006814]
Sihota R, Selvan H, Sharma A, Gupta N, Shakrawal J, Angmo D, Dada T, Upadhyay A. Severity of visual field defects in primary congenital glaucoma and their risk factors. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2020 Jul:258(7):1483-1491. doi: 10.1007/s00417-020-04677-w. Epub 2020 Apr 15 [PubMed PMID: 32296990]
Naik A, Sihota R, Mahalingam K, Angmo D, Dada T, Kumar A, Kumar A, Gupta A. Evaluation of visual field changes with retinal nerve fiber layer thickness in primary congenital glaucoma. Indian journal of ophthalmology. 2022 Oct:70(10):3556-3561. doi: 10.4103/ijo.IJO_396_22. Epub [PubMed PMID: 36190046]
Abdeen W, Esmael AF, Gawdat G, El-Fayoumi D. Anterior chamber angle features in primary congenital glaucoma infants using hand-held anterior segment-oct. Eye (London, England). 2022 Jun:36(6):1238-1245. doi: 10.1038/s41433-021-01583-1. Epub 2021 Jun 11 [PubMed PMID: 34117386]
Makhoul NJ, Wehbi Z, El Hadi D, Noureddine B, Boustany RM, Al-Haddad C. Whole-exome screening for primary congenital glaucoma in Lebanon. Ophthalmic genetics. 2023 Jun:44(3):234-245. doi: 10.1080/13816810.2023.2189949. Epub 2023 Mar 30 [PubMed PMID: 36995002]
Gusson E, Chemello F, Longo R, Franzolin E, Vesentini R, Verlato G, Marchini G. Primary congenital glaucoma surgery: outcomes and visual function. International ophthalmology. 2021 Nov:41(11):3861-3867. doi: 10.1007/s10792-021-01957-0. Epub 2021 Jul 23 [PubMed PMID: 34297306]
Strzalkowska A, Strzalkowski P, Stingl JV, Pfeiffer N, Schuster AK, Hoffmann EM. Influence of different primary surgical techniques on long-term intraocular pressure and medication in glaucoma after congenital cataract surgery. PloS one. 2023:18(7):e0286318. doi: 10.1371/journal.pone.0286318. Epub 2023 Jul 5 [PubMed PMID: 37406023]
Geyer O, Segal A, Melamud A, Wolf A. Clinical Outcomes After Ahmed Glaucoma Valve Implantation for Pediatric Glaucoma After Congenital Cataract Surgery. Journal of glaucoma. 2021 Jan 1:30(1):78-82. doi: 10.1097/IJG.0000000000001689. Epub [PubMed PMID: 33003112]
Level 2 (mid-level) evidenceSamant M, Medsinge A, Nischal KK. Pediatric Glaucoma: Pharmacotherapeutic Options. Paediatric drugs. 2016 Jun:18(3):209-19. doi: 10.1007/s40272-016-0174-4. Epub [PubMed PMID: 27093864]
Lewis RA, Christie WC, Day DG, Craven ER, Walters T, Bejanian M, Lee SS, Goodkin ML, Zhang J, Whitcup SM, Robinson MR, Bimatoprost SR Study Group. Bimatoprost Sustained-Release Implants for Glaucoma Therapy: 6-Month Results From a Phase I/II Clinical Trial. American journal of ophthalmology. 2017 Mar:175():137-147. doi: 10.1016/j.ajo.2016.11.020. Epub 2016 Dec 22 [PubMed PMID: 28012819]
Level 1 (high-level) evidenceGhate D, Wang X. Surgical interventions for primary congenital glaucoma. The Cochrane database of systematic reviews. 2015 Jan 30:1():CD008213. doi: 10.1002/14651858.CD008213.pub2. Epub 2015 Jan 30 [PubMed PMID: 25636153]
Level 1 (high-level) evidenceBroughton WL, Parks MM. An analysis of treatment of congenital glaucoma by goniotomy. American journal of ophthalmology. 1981 May:91(5):566-72 [PubMed PMID: 7234937]
SMITH R. A new technique for opening the canal of Schlemm. Preliminary report. The British journal of ophthalmology. 1960 Jun:44(6):370-3 [PubMed PMID: 13832124]
Mendicino ME, Lynch MG, Drack A, Beck AD, Harbin T, Pollard Z, Vela MA, Lynn MJ. Long-term surgical and visual outcomes in primary congenital glaucoma: 360 degrees trabeculotomy versus goniotomy. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2000 Aug:4(4):205-10 [PubMed PMID: 10951295]
Level 2 (mid-level) evidenceMcPherson SD Jr, Berry DP. Goniotomy vs external trabeculotomy for developmental glaucoma. American journal of ophthalmology. 1983 Apr:95(4):427-31 [PubMed PMID: 6837685]
Cairns JE. Trabeculectomy. Preliminary report of a new method. American journal of ophthalmology. 1968 Oct:66(4):673-9 [PubMed PMID: 4891876]
Sidoti PA, Belmonte SJ, Liebmann JM, Ritch R. Trabeculectomy with mitomycin-C in the treatment of pediatric glaucomas. Ophthalmology. 2000 Mar:107(3):422-9 [PubMed PMID: 10711876]
Level 2 (mid-level) evidenceElhofi A, Helaly HA. Non-Penetrating Deep Sclerectomy versus Trabeculectomy in Primary Congenital Glaucoma. Clinical ophthalmology (Auckland, N.Z.). 2020:14():1277-1285. doi: 10.2147/OPTH.S253689. Epub 2020 May 12 [PubMed PMID: 32494118]
Razeghinejad MR, Kaffashan S, Nowroozzadeh MH. Results of Ahmed glaucoma valve implantation in primary congenital glaucoma. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2014 Dec:18(6):590-5. doi: 10.1016/j.jaapos.2014.08.008. Epub 2014 Nov 12 [PubMed PMID: 25459201]
Level 2 (mid-level) evidenceMalek I, Sayadi J, Choura R, Mekni M, Rayhane H, Khairallah M, Nacef L. Long-Term Results of Combined Trabeculotomy Trabeculectomy in Primary Congenital Glaucoma. Journal of glaucoma. 2023 Oct 1:32(10):848-853. doi: 10.1097/IJG.0000000000002229. Epub 2023 Apr 10 [PubMed PMID: 37079484]
Yazdani S, Pakravan M, Gerami E, Doozandeh A, Esfandiari H, Sharifipour F. Trabeculotomy Versus Combined Trabeculotomy-Trabeculectomy for Management of Primary Congenital Glaucoma. Journal of glaucoma. 2022 May 1:31(5):346-350. doi: 10.1097/IJG.0000000000001981. Epub 2022 Jan 10 [PubMed PMID: 34999664]
al Faran MF, Tomey KF, al Mutlaq FA. Cyclocryotherapy in selected cases of congenital glaucoma. Ophthalmic surgery. 1990 Nov:21(11):794-8 [PubMed PMID: 2270165]
Level 2 (mid-level) evidenceElhefney EM, Mokbel TH, Hagras SM, AlNagdy AA, Ellayeh AA, Mohsen TA, Gaafar WM. Micropulsed diode laser cyclophotocoagulation in recurrent pediatric glaucoma. European journal of ophthalmology. 2020 Sep:30(5):1149-1155. doi: 10.1177/1120672119858226. Epub 2019 Jul 1 [PubMed PMID: 31256680]
Gouider D, Choura R, Mekni M, Sayadi J, Malek I, Nacef L. Sclerocornea: A rare ocular condition. Journal francais d'ophtalmologie. 2021 Sep:44(7):1089-1091. doi: 10.1016/j.jfo.2021.05.001. Epub 2021 Jun 18 [PubMed PMID: 34148700]
Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian journal of ophthalmology. 2021 May:69(5):1095-1101. doi: 10.4103/ijo.IJO_1808_20. Epub [PubMed PMID: 33913840]
Level 2 (mid-level) evidenceGurnani B, Narayana S, Christy J, Rajkumar P, Kaur K, Gubert J. Successful management of pediatric pythium insidiosum keratitis with cyanoacrylate glue, linezolid, and azithromycin: Rare case report. European journal of ophthalmology. 2022 Sep:32(5):NP87-NP91. doi: 10.1177/11206721211006564. Epub 2021 Mar 28 [PubMed PMID: 33779337]
Level 3 (low-level) evidenceGurnani B, Kaur K. Pythium Keratitis. StatPearls. 2024 Jan:(): [PubMed PMID: 34424645]
Raven ML, Rodriguez ME, Potter HD. Corneal Leukoma with Features of Both Sclerocornea and Peter's Anomaly. Ophthalmology. 2016 Sep:123(9):1988. doi: 10.1016/j.ophtha.2016.05.011. Epub [PubMed PMID: 27549880]
Altamirano F, Ortiz-Morales G, O'Connor-Cordova MA, Sancén-Herrera JP, Zavala J, Valdez-Garcia JE. Fuchs endothelial corneal dystrophy: an updated review. International ophthalmology. 2024 Feb 12:44(1):61. doi: 10.1007/s10792-024-02994-1. Epub 2024 Feb 12 [PubMed PMID: 38345780]
Nusbaum L, Paul M, Maharshak I. [DEEP ORBITAL DERMOID CYSTS]. Harefuah. 2023 Feb:162(2):98-102 [PubMed PMID: 36916079]
Balamurugan S, Gurnani B, Kaur K, Gireesh P, Narayana S. Traumatic intralenticular abscess-What is so different? The Indian journal of radiology & imaging. 2020 Jan-Mar:30(1):92-94. doi: 10.4103/ijri.IJRI_369_19. Epub 2020 Mar 30 [PubMed PMID: 32476758]
Kaur K, Gurnani B, Devy N. Atypical optic neuritis - a case with a new surprise every visit. GMS ophthalmology cases. 2020:10():Doc11. doi: 10.3205/oc000138. Epub 2020 Feb 27 [PubMed PMID: 32269909]
Level 3 (low-level) evidencede Silva DJ, Khaw PT, Brookes JL. Long-term outcome of primary congenital glaucoma. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2011 Apr:15(2):148-52. doi: 10.1016/j.jaapos.2010.11.025. Epub [PubMed PMID: 21596293]
Shaffer RN. Prognosis of goniotomy in primary infantile glaucoma (trabeculodysgenesis). Transactions of the American Ophthalmological Society. 1982:80():321-5 [PubMed PMID: 7182965]
Kaur K, Kannusamy V, Mouttapa F, Gurnani B, Venkatesh R, Khadia A. To assess the accuracy of Plusoptix S12-C photoscreener in detecting amblyogenic risk factors in children aged 6 months to 6 years in remote areas of South India. Indian journal of ophthalmology. 2020 Oct:68(10):2186-2189. doi: 10.4103/ijo.IJO_2046_19. Epub [PubMed PMID: 32971637]
Christy J, Jain N, Gurnani B, Kaur K. Twinkling Eye -A Rare Presentation in Neovascular Glaucoma. Journal of glaucoma. 2019 May 23:():. doi: 10.1097/IJG.0000000000001287. Epub 2019 May 23 [PubMed PMID: 31135586]
Gurnani B, Kaur K, Sekaran S. First case of coloboma, lens neovascularization, traumatic cataract, and retinal detachment in a young Asian female. Clinical case reports. 2021 Sep:9(9):e04743. doi: 10.1002/ccr3.4743. Epub 2021 Aug 30 [PubMed PMID: 34484773]
Level 3 (low-level) evidenceGurnani B, Kaur K, Gireesh P. A rare presentation of anterior dislocation of calcified capsular bag in a spontaneously absorbed cataractous eye. Oman journal of ophthalmology. 2021 May-Aug:14(2):120-121. doi: 10.4103/ojo.OJO_65_2019. Epub 2021 Jun 28 [PubMed PMID: 34345149]
Gurnani B, Kaur K, Gireesh P. Rare Coexistence of Bilateral Congenital Sutural and Cortical Blue Dot Cataracts. Journal of pediatric ophthalmology and strabismus. 2020 Jan 1:57(1):68. doi: 10.3928/01913913-20191011-01. Epub [PubMed PMID: 31972045]
Kaur K, Gurnani B, Kannusamy V, Yadalla D. A tale of orbital cellulitis and retinopathy of prematurity in an infant: First case report. European journal of ophthalmology. 2022 Nov:32(6):NP20-NP23. doi: 10.1177/11206721211026098. Epub 2021 Jun 17 [PubMed PMID: 34137305]
Level 3 (low-level) evidence