Introduction
Macular edema is a retinal condition characterized by fluid buildup in the central part of the retina responsible for sharp, central vision, and accompanies various retinal diseases such as diabetic retinopathy, retinal vascular occlusions, and uveitis.[1][2] This condition causes decreased visual acuity and, when persistent, can lead to severe vision loss.[3] Fluid accumulates due to a mismatch between retinal fluid entry and exit mechanisms.[4] Dysfunction of the blood-retinal barrier allows the entry of proteins and solutes into retinal tissue, which underlies its pathogenesis.[5]
The distinctive anatomical characteristics of the macula, including its abundant photoreceptor count, elevated metabolic activity, and limited extracellular fluid resorption due to a central avascular zone, along with its specialized cellular and molecular composition containing specific glial cells like Müller cells, suggest a propensity for fluid accumulation. Furthermore, the intriguing arrangement of the Henle fiber layer and the potential presence of a "glymphatic system" further indicate the macula's role as a reservoir for fluid retention.[4][6][7]
Patients affected by macular edema commonly experience symptoms such as metamorphopsia, micropsia, blurred vision, central scotoma, and reduced contrast or color sensitivity. Clinicians frequently utilize fundus fluorescein angiography (FFA) and optical coherence tomography (OCT) for diagnostic purposes, as diagnosing macular edema clinically can be challenging in patients with mild disease or when adequate visualization of the fundus is impossible. The visual impairment can be variable and reversed with appropriate therapy. Treatment options for macular edema vary depending on the underlying pathology and may encompass anti–vascular endothelial growth factor therapy (VEGF), corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), or surgical intervention. These treatments target vasoactive and inflammatory mediators that disrupt the blood-retinal barrier.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The primary underlying causes of macular edema are increased leakage from damaged retinal blood vessels, the growth of abnormal blood vessels in the deep retina, and the breakdown of the blood-retinal barrier. New blood vessels lacking normal tight junctions lead to abnormal serum leakage from the bloodstream into the retina. Other significant causes of macular edema include diabetes, branch and central retinal vein occlusion (RVO), choroidal neovascularization, posterior uveitis, postoperative inflammation, and central serous chorioretinopathy (see Image. Macular Edema Associated With Diabetes).
Additional causes of macular edema include Coats disease, retinal artery macroaneurysms, radiation retinopathy, hypertensive retinopathy, inflammatory disorders, medications, choroidal tumors, retinitis pigmentosa, nonarteritic anterior ischemic optic neuropathy (NAION), and Irvine-Gass syndrome.
Common causes of subfoveal fluid without intraretinal fluid include acute central serous chorioretinopathy, polypoidal choroidal vasculopathy, and uveitis, including Vogt-Koyanagi-Harada syndrome, sympathetic ophthalmia, posterior scleritis, and choroidal granuloma.[8][9][10][11][12] In addition, foveoschisis with or without subretinal fluid characterizes optic disc pit maculopathy.
Epidemiology
Among the global working population, macular edema is the primary cause of vision loss in patients with diabetic retinopathy.[13] Its occurrence in population-based investigations ranges from 4.2% to 7.9% for individuals with type 1 diabetes and 1.4% to 12.8% for those with type 2 diabetes.[14] Notably, 27% of patients affected by type 1 diabetes develop diabetic macular edema within 9 years of onset.
RVO presents with varying prevalence rates of macular edema. Central RVO (CRVO) impacts approximately 0.1% to 0.2% of the population, whereas branch RVO (BRVO) affects nearly 0.5% to 2% of individuals.[15][16] In a Canadian cohort, the annual incidence of visual impairment, defined as visual acuity worse than 20/40 due to macular edema associated with BRVO, is 0.056%, and due to CRVO is 0.021%.[17]
Prevalence rates for age-related macular degeneration increase with age. The annual incidence of age-related macular degeneration ranges from 0.3 per 1000 in people 55 to 59 to 36.7 per 1000 in individuals aged 55 to 59 to 36.7 per 1000 individuals in those aged 90 or older. Uveitis may lead to macular edema, with prevalence rates varying based on the underlying uveitic condition. The incidence of uveitis itself ranges from 10.5 to 52 per 100,000 person-years.[18]
The incidence of clinical Irvine-Gass syndrome, also known as pseudophakic cystoid macular edema, which manifests following uneventful cataract surgery, varies from 0.1% to 2.35%.[19] However, patients assessed with FFA and OCT reveal a notably higher incidence of 30% after extracapsular cataract surgery and 4% to 11% after phacoemulsification.[20][21] Risk factors for its development include systemic conditions such as diabetes and hypertension, preexisting ocular conditions such as diabetic retinopathy and RVO, as well as intraoperative complications such as posterior capsule rupture, surgical trauma, vitreous loss, use of high phacoemulsification energy, and prolonged surgical duration.[22]
In a study involving 25 eyes with NAION, OCT revealed subretinal fluid around the optic disc in 64% of eyes, with involvement extending to the fovea in 16% of cases.[23] However, this prevalence may be underestimated since not all patients with NAION undergo OCT routinely.[24] Macular edema may occur in 10% to 50% of patients with retinitis pigmentosa.[25]
Pathophysiology
General Pathophysiology
Intra- or subretinal fluid accumulation is due to a combination of dysregulation of the blood-retinal barrier, which permits proteins and other solutes that are usually retained in the blood to infiltrate the retinal tissue, increased leakage from damaged retinal blood vessels, and the growth of abnormal blood vessels in the deep retina. This fluid can accumulate diffusely in the central retina or within cysts.
Blood-Retinal Barrier
To promote optimal light transmission, the retinal interstitial spaces maintain a dry state through collaborative mechanisms that regulate fluid movement in and out. The relatively rigid macular framework provides resistance, limiting fluid influx from the vitreous cavity driven by intraocular pressure (IOP). Additionally, osmotic and hydrostatic forces within the retinal tissue and capillaries counterbalance each other. Choroidal osmotic pressure efficiently draws fluid out of the subretinal space, while active transport mechanisms in the retinal pigment epithelium pumps actively transport fluid from the subretinal space to the choroid.[5]
The crucial element in maintaining this delicate equilibrium is the blood-retinal barrier.[26] This barrier prevents large molecules, such as proteins, from entering the retinal tissue. Any disruption of the blood-retinal barrier that allows proteins and other solutes, typically confined to the bloodstream, to infiltrate the retinal tissue can result in macular edema. Tight junctions form the inner blood-retinal barrier, or zonulae occludentes, among retinal capillary endothelial cells.
In contrast, the outer blood-retinal barrier comprises tight junctions between retinal pigment epithelial cells, adherens junctions, and desmosomes or maculae adherens. Although adherens junctions between photoreceptors and the external limiting membrane are not entirely impermeable to proteins, they restrict free protein movement. Pathological conditions that disrupt the blood-retinal barrier lead to macular edema by allowing proteins to enter the retinal tissue, initiating fluid accumulation through osmosis.[6]
Microvascular Changes
Vascular leakage involves various mechanisms, with inflammation of vessel walls playing a central role. A myriad of inflammatory mediators initiate a complex cascade of reactions. These mediators include VEGF, angiopoietin-2 (Ang-2), placental growth factor (PlGF), angiotensin II, prostaglandins, cytokines, chemokines, interleukins, matrix metalloproteinases, intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1), P-selectin, E-selectin, as well as inflammatory cells such as macrophages and neutrophils.[27][28]
The inflamed vessel wall activates the renin-angiotensin pathway, leading to the generation of angiotensin. Angiotensin II contributes to the breakdown of the blood-retinal barrier through various mechanisms, including leukocyte infiltration, heightened vascular permeability, and extracellular matrix remodeling. Ischemia in the retina, combined with angiotensin II, inflammation, and other growth factors, triggers the secretion of VEGF. This cascade results in the breakdown of the blood-retinal barrier by initiating leukocyte infiltration, prompting structural alterations, and dissolving tight junctions among endothelial cells through processes such as phosphorylation of occludin protein, activation of protein kinase C, and induction of fenestrations. Similarly, prostaglandin E1 induces blood-retinal barrier breakdown by facilitating the opening of tight junctions.[29]
The subretinal fluid typically results from a combination of inner blood-retinal barrier breakdown and damage to the retinal pigment epithelium pump. Conditions such as exudative age-related macular degeneration, choroidal neovascularization, choroidal neovascular membrane, polypoidal choroidal vasculopathy, and retinal angiomatosis proliferation involve active exudation within the subretinal space due to abnormal choroidal vessels. Consequently, subretinal fluid accumulation is more pronounced in these diseases compared to those that primarily affect the blood-retinal barrier.[6][7]
Disease Specific Pathophysiology
Macular edema in diabetes: Diabetic macular edema arises from microvascular alterations in the retina, characterized by basement membrane thickening and pericyte reduction. These changes increase retinal vascular permeability, causing leakage of plasma constituents into the surrounding retina and edema. Hypoxia resulting from this process can further stimulate VEGF production.[6][7]
Retinal vein occlusions: Ischemia, raised hydrostatic pressure in the perifoveal capillaries, and turbulent blood flow disrupt the outer blood-retinal barrier.[5]
Macular neovascularization: The most common cause of macular neovascularization is wet age-related macular degeneration.[30] Choroidal neovascularization results in macular edema, as the newly formed blood vessels leak into the retina, causing fluid accumulation in the macula.[31]
Vitreomacular interface disorders: Vitreomacular interface disorders, including epiretinal membrane and vitreomacular traction due to incomplete posterior vitreous detachment, can cause macular edema through several effects. Researchers believe the traction causes increased local VEGF secretion and inflammation, causing blood-retinal barrier breakdown, vascular leakage, and macular edema. In addition, direct distortion of surrounding intraretinal vessels likely contributes to leakage, amplifies local VEGF secretion, and triggers the release of inflammatory factors such as basic fibroblast growth factor, further inducing local inflammation.[30]
Coats disease: Coats disease is an idiopathic ocular condition characterized by retinal telangiectasia, aneurysms, and exudation. Damage to the endothelium of the retinal vasculature and abnormal pericytes disrupt the inner blood-retinal barrier.[32] These abnormalities lead to multiple telangiectasias, aneurysmal dilation of vessels, and retinal ischemia.[33]
Retinal artery macroaneurysms: Retinal artery macroaneurysms are typically caused by chronic hypertension, arteriosclerosis, and focal ischemia of blood vessel walls. These factors lead to the weakening of the blood vessel wall and subsequent aneurysmal dilatation, resulting in macular exudation and hemorrhage.[34][35]
Radiation retinopathy: Macular edema is one of the earliest features of radiation retinopathy.[36] Initially, vascular damage occurs in capillaries due to free radicals, resulting in capillary nonperfusion and leakage.[37] Subsequently, retinal ischemia ultimately leads to macular edema, neovascularization, vitreous hemorrhage, and tractional retinal detachment.[36] Tissue tolerance doses (TD) are the total radiation doses that lead to complication rates of 5% (TD5/5) and 50% (TD50/5), respectively, at 5 years.[38][39] The TD5/5 and TD50/5 for the retina are 45 and 65 Gy, respectively.[38][40][41]
Hypertensive retinopathy: Hypertensive retinopathy is characterized by ischemic hypoperfusion of the choroid, disrupting the outer blood-retinal barrier and damaging the retinal pigment epithelium.[7]
Irvine-Gass syndrome: Irvine-Gass syndrome is typically triggered by surgical trauma during intraocular surgeries, which induces the breakdown of the blood-aqueous barrier through various mechanisms, including prostaglandin release.[42] The subsequent diffusion of inflammatory mediators into the vitreous cavity disrupts the blood-retinal barrier, leading to increased permeability of the perifoveal capillaries.[43]
Inflammatory disorders: Inflammatory disorders are characterized by the infiltration of inflammatory cells, such as lymphocytes and macrophages, within the retinal layers. Additionally, various factors, including prostaglandins, initiate inflammatory cascades that contribute to tissue damage and exacerbate the breakdown of the blood-retinal barrier.[22] Patients with inflammatory conditions like intermediate uveitis, anterior uveitis, birdshot retinochoroiditis, retinal vasculitis, and post-fever retinitis may exhibit cystoid macular edema (see Image. Cystoid Macular Edema, Uveitis).[44][45][46][47][48]
Panretinal photocoagulation: Macular edema following panretinal photocoagulation occurs as a secondary effect of the inflammation induced during the procedure, coupled with increases in macular blood flow secondary to the laser.[1][2][6]
Drug-induced macular edema: Drug-induced macular edema can be triggered by various medications. For instance, topical epinephrine has been associated with the breakdown of the blood-retinal barrier and subsequent macular edema.[49] Prolonged systemic use of tamoxifen can also lead to reversible macular edema.[50] In addition, systemic nicotinic acid disrupts the blood-retinal barrier through prostaglandin release and Müller cell toxicity.[51][52] Topical latanoprost may cause a blood-aqueous barrier disruption in early postoperative eyes.[53]
Choroidal tumors: Choroidal tumors such as choroidal hemangioma can be linked to cystoid macular edema and subretinal fluid due to abnormal leaking vessels. In rare cases, choroidal melanoma may also lead to these conditions secondary to the infiltration of chronic inflammatory cells within the choroid adjacent to the tumor.[54][55]
Retinitis pigmentosa and other inherited retinal diseases: Macular edema associated with inherited retinal diseases may occur through several mechanisms. These include the breakdown of the blood-retinal barrier caused by toxic products released from degenerating retinal cells, particularly the retinal pigment epithelial cells. Additionally, failure of the retinal pigment epithelial pumping mechanism and Müller cell dysfunction can contribute to its development.[25] Macular edema may be present in conditions such as gyrate atrophy of the retina and choroid, even without leakage on FFA.[56][57][58][59]
Juvenile X-linked retinoschisis, resulting due to mutations in the retinoschisin 1 (RS1) gene, encoding retinoschisin—a protein crucial for intercellular adhesion and likely retinal cellular organization—is a significant cause of juvenile macular degeneration in males. This condition typically manifests in the first decade of life (see Image. Juvenile X-Linked Retinoschisis).
Nonarteritic anterior ischemic optic neuropathy: Macular edema is an uncommon finding associated with NAION.[60] Researchers speculate that fluid from the peripapillary choroid can percolate into the subretinal or intraretinal spaces.[24] Notably, subretinal fluid extending to the fovea or involving the fovea alone may be noted in other disorders causing optic disc edema, including neuroretinitis.[61]
Histopathology
Histopathological studies underscore the critical role of blood-retinal barrier breakdown in the pathogenesis of macular edema. Macular edema frequently manifests with vascular changes, including capillary dilation, microaneurysm formation, and endothelial cell hyperplasia.[62] In addition, structural changes, including the presence of cystoid spaces within the inner nuclear layer and disruption of the external limiting membrane, are common findings.[63] These morphological changes correspond with the clinical manifestation of cystoid macular edema observed in imaging studies.
An additional characteristic histopathological feature is the presence of lipid-laden exudates within the macular region, particularly evident in cases associated with vascular abnormalities such as macular edema associated with diabetes.[64] These exudates contribute to the disruption of retinal architecture and further compromise visual function. Moreover, chronic macular edema often exhibits histological alterations in the extracellular matrix, including collagen deposition and fibrous tissue proliferation. These changes may signify the advancement of macular edema to a more advanced and irreversible stage.[65]
History and Physical
Macular edema can sometimes be asymptomatic, but typical symptoms include metamorphopsia, where objects—specifically straight lines—appear warped, distorted, or bent, and micropsia, where patients perceive the external world as smaller than its actual size. Additional symptoms include blurred vision, central scotoma, and reduced contrast or color sensitivity. Visual impairment can range from mild to severe. In cases of central serous chorioretinopathy, patients commonly report experiencing central round or oval relative scotomas.
Retinal Vein Occlusion
Common symptoms of RVO include scotoma or visual field deficits, along with blurred or gray vision. Pain is typically absent as the retina lacks trigeminal innervation. In BRVO, patients may not exhibit symptoms or experience peripheral visual field defects. Blurred central vision arises if macular involvement or edema occurs. CRVO presents with an acute onset of broad, unilateral, painless, blurred vision, whereas patients with hemiretinal vein occlusion typically report blurred central vision.
Coats Disease
Coats disease, primarily impacting males aged 18 or younger and middle-aged men, commonly presents with diminished visual acuity, strabismus, and leukocoria. The condition can sometimes develop as a secondary response to a previous vascular event. Symptoms usually manifest unilaterally, and clinical examination often reveals subretinal lipid accumulation alongside abnormal telangiectatic vessels. Please see StatPearls' companion resource, "Exudative Retinitis (Coats Disease)," for further information.
Retinal Artery Macroaneurysms
Individuals with retinal artery macroaneurysms commonly experience a sudden onset of painless vision loss in an eye. The patient may remain asymptomatic if the central macula is spared or the aneurysm occurs without exudation or hemorrhage. See StatPearls' companion resource, "Retinal Macroaneurysm," for further information regarding the presentation and physical examination findings associated with retinal artery macroaneurysms.
Radiation Retinopathy
Radiation retinopathy is often asymptomatic and is typically discovered incidentally during fundoscopic examination. Clinical observations may include cotton-wool spots, hard exudates, retinal edema, telangiectasia, and perivascular sheathing. When symptomatic, symptoms of painless vision loss may manifest months to years after radiation therapy. Dilated funduscopic examination often reveals macular edema, exudates, microaneurysms, and vessel telangiectasias.
Irvine-Gass Syndrome
Decreased or blurry vision following cataract surgery is a common presentation of Irvine-Gass syndrome, often accompanied by optic disc edema as a characteristic funduscopic finding.
Nonarteritic Anterior Ischemic Optic Neuropathy
Affected patients typically present with monocular vision loss that occurs over hours to days. Common findings from the examination include reduced visual acuity, diminished color vision, an afferent pupillary defect, optic disc edema, peripapillary splinter hemorrhage, and a small optic cup in the unaffected eye. The optic disc is usually hyperemic.
Evaluation
Historically, methods for evaluating macular edema included contact and non-contact slit lamp biomicroscopy, indirect ophthalmoscopy, FFA, fundus stereo photography, and OCT. Currently, OCT and FFA are the predominant investigative tools. Notably, measuring visual acuity in all patients is imperative, as while it may not directly aid in diagnosing macular edema, it serves as a crucial parameter for monitoring disease progression.
Slit-Lamp Biomicroscopy
The initial step in evaluating macular edema involves slit-lamp biomicroscopy, typically conducted using a 90D or 78D lens. The biomicroscopic examination method reveals the presence and location of macular thickening, exudates, and cystoid changes.[66] A distinctive stellate or radially oriented pattern of perifoveal cysts attributed to the oblique arrangement of the Henle fiber layer characterizes cystoid macular edema. Beyond the macular area, edema presents a honeycomb appearance due to the perpendicular alignment of the outer plexiform layer. A central cyst associated with cystoid macular edema may resemble a full-thickness macular hole; however, conducting the Watzke-Allen test during slit lamp biomicroscopy with a 90D lens reveals an intact vertical line without a central break.[67] Additionally, macular edema tends to reduce choroidal visibility compared to unaffected areas. Stereoscopic examination, facilitated by a 90D or macular contact lens, provides a 3-dimensional perspective, aiding in the identification of retinal elevation.
Fundus Fluorescein Angiography
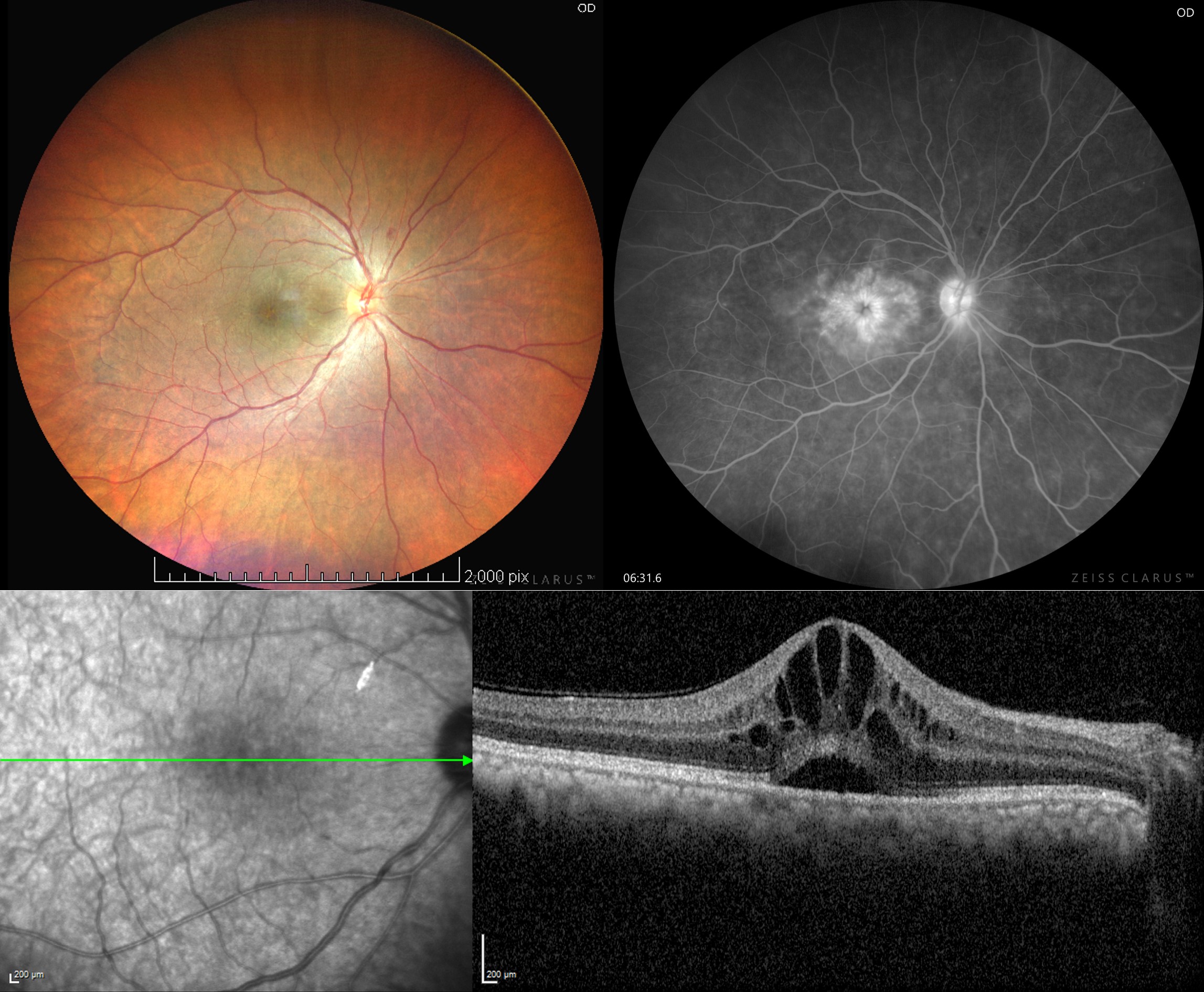
FFA can delineate regions of retinal capillary leakage. The Early Treatment Diabetic Retinopathy Study (ETDRS) categorizes diabetic macular edema into diffuse and focal types based on the degree of fluorescein leakage associated with microaneurysms. According to the ETDRS criteria, focal diabetic macular edema exhibits 67% or more leakage associated with microaneurysms, intermediate demonstrates 33% to 66% leakage, and diffuse showcases less than 33% leakage associated with microaneurysms.[68] Larssen et al define diffuse diabetic macular edema as retinal thickening affecting 2 or more disk areas with involvement of the macular center. Focal diabetic macular edema, on the other hand, presents retinal thickening of less than 2 disk areas without affecting the macular center.[69] In FFA, focal macular edema is identified by fluorescein leakage from specific capillary regions. Ischemic diabetic macular edema appears as hypofluorescent areas within the macula (see Image. Multimodal Imaging of Diabetic Macular Edema).
Early-phase choroidal fluorescence can become partially obstructed in the presence of a considerable amount of edema, whether cystoid or non-cystoid, particularly if turbid due to lipid-laden macrophages. Dilation of the fine capillary network or telangiectatic retinal vessels around the fovea may be observed in the arteriovenous phase. Late-phase imaging reveals hyperfluorescence caused by dye accumulation leaking from retinal vessels, the extent of which depends on the dysfunctional retinal vascular endothelium. Hyperfluorescence may manifest as cystic or diffuse irregular staining, filling cystoid spaces rapidly in the presence of pronounced leakage or appearing late if not significant. Additionally, large retinal vessels may leak, termed perivascular staining, due to inflammation, traction, or occlusion. Cystoid macular edema typically presents as a petaloid leak at the macula during the late phase of FFA.[70]
Conditions in which an FFA leak is not evident despite the presence of macular edema include retinitis pigmentosa, gyrate atrophy of the retina and the choroid with foveoschisis, juvenile X-linked retinoschisis, Goldmann-Favre disease, phototoxicity, toxicity from antimicrotubule agents such as paclitaxel and docetaxel, and toxicity from nicotinic acid.[51][52][71] Foveoschisis and leaking cystoid macular edema can be distinguished through FFA, as foveoschisis does not exhibit leakage or induce the characteristic petaloid leak of cystoid macular edema.
Optical Coherence Tomography
Clinicians use OCT to evaluate macular edema caused by diseases such as age-related macular degeneration, diabetic retinopathy, hereditary retinal degeneration, RVO after cataract surgery, epiretinal membrane, and uveitis. Owing to its excellent reproducibility, OCT has become the preferred diagnostic modality for diagnosing and monitoring cystoid macular edema. OCT enables clinicians to identify, localize, and quantify fluid collections, facilitating precise assessment and long-term monitoring. Additionally, OCT's capacity to classify various diseases supports prognostication, aiding in disease management, predicting patient outcomes, and treatment planning.
Diabetic macular edema: Different patterns of fluid accumulation appear on OCT in patients with diabetic macular edema:
- Diffuse retinal thickening: Characterized by retinal thickness greater than 200 μm in height and more than 200 μm in width with areas of lower reflectivity, especially in the outer retinal layers.
- Cystoid macular edema: Manifests as intraretinal fluid accumulation within well-defined spaces of low reflectivity, typically originating around the outer plexiform layer but potentially involving the photoreceptor and inner retinal layers.
- Posterior hyaloid traction or taut posterior hyaloid membrane: Identified by the presence of a highly reflective membrane on the inner retinal surface, causing tractional retinal elevation.
- Subretinal fluid: Identified as a dome-shaped dark region located between the neurosensory retina and the retinal pigment epithelium.
- Tractional retinal detachment: Characterized by a peak-shaped retinal detachment resulting from traction exerted by proliferative membranes over the retinal surface or within the vitreous.[41] This condition presents as a low signal area underlying the highly reflective border of the detached retina.
Radiation retinopathy: OCT enables clinicians to grade radiation retinopathy using a 5-point grading system, which correlates with visual acuity.
- Grade 1: Foveola-sparing non-cystoid macular edema
- Grade 2: Foveola-sparing cystoid macular edema
- Grade 3: Foveola-involving non-cystoid macular edema
- Grade 4: Mild-to-moderate foveola-involving cystoid macular edema
Juvenile X-linked retinoschisis: OCT findings can classify juvenile X-linked retinoschisis into distinct types, as mentioned below.
- Type 1 or foveal: Absence of both lamellar schisis on OCT and peripheral schisis on the ophthalmoscopy.
- Type 2 or foveolamellar: Presence of lamellar schisis on OCT without peripheral schisis on the ophthalmoscopy.
- Type 3 or complex: Lamellar schisis on OCT and peripheral schisis on the ophthalmoscopy.
- Type 4 or foveoperipheral: Presence of peripheral schisis on ophthalmoscopy without lamellar schisis on OCT.[72][73]
The hallmark finding of juvenile X-linked retinoschisis is the presence of a spoke-wheel pattern in the macula, particularly observable in high-magnification ophthalmoscopy in patients aged 30 or younger. Currently, spectral domain OCT serves as the primary diagnostic modality for this condition, allowing for the visualization of marked retinoschisis in various retinal layers. Clinicians may observe dilation of the fine capillary network or telangiectatic retinal vessels around the fovea.
On OCT, patients with uveitis typically exhibit diffuse macular edema, cystoid macular edema, and subretinal detachment. Clinicians may observe intraretinal fluid, accumulation of subretinal fluid, and pigment epithelial detachments in patients with choroidal neovascularization, as seen in wet age-related macular degeneration. Subretinal detachment is also evident in OCT scans of patients with BRVO. Vitreomacular traction manifests as foveal cavitation, while the posterior hyaloid often appears hyper-reflective and thickened on OCT. OCT angiography is a valuable tool for evaluating the vascular status of the posterior pole.
Treatment / Management
A stepwise therapeutic approach is essential for managing macular edema, typically involving systemic and ocular pharmaceutical agents. Surgical intervention may also be required to address specific needs in certain cases.
Systemic Therapy
Given that many patients develop macular edema as a secondary manifestation of systemic health conditions such as diabetes, hypertension, dyslipidemia, or inflammatory conditions, addressing these underlying systemic issues is paramount. Research indicates that strict glycemic control can effectively delay the onset and progression of diabetic retinopathy in both type 1 and type 2 diabetes.[74][75] Additionally, managing associated disorders such as nephropathy and ischemic heart disease yields significant benefits.[76][77](A1)
Intravitreal Anti-Vascular Endothelial Growth Factor
Intravitreal injections of anti-VEGF agents represent the primary treatment approach for macular edema across various pathologies. Pegaptanib, the initial medication approved for human use, is a 40-kDa aptamer and mRNA polyethylene glycol-linked molecule designed to specifically target VEGF165. However, it is no longer utilized for treatment.[78] (B3)
Currently, clinicians commonly administer 3 formulations of intravitreal anti-VEGF therapies:
- Bevacizumab, available at 1.25 mg/0.05 mL, is a 148-kDa humanized full-size monoclonal IgG1 antibody targeting all VEGF-A subtypes.
- Ranibizumab, available at 0.3 mg/0.05 mL and 0.5 mg/0.05 mL, is a 48-kDa humanized monoclonal antibody fragment also targeting all VEGF-A subtypes.
- Aflibercept, available at 2 mg/0.05 mL, is a 115-kDa fusion protein targeting VEGF-A, VEGF-B, and placental growth factors.
Diabetic macular edema: Findings from the Diabetic Retinopathy Clinical Research (DRCR) Retina Network Protocol H indicate that intravitreal bevacizumab may mitigate diabetic macular edema in select cases.[79] Similarly, the bevacizumab or laser therapy (BOLT) study demonstrates the favorable impact of intravitreal bevacizumab on center-involving clinically significant macular edema in eyes without advanced macular ischemia. The ETDRS defines clinically significant macular edema as retinal thickening within 500 μm of the macular center, hard exudates within 500 μm of the macular center with associated adjacent retinal thickening, or retinal thickening measuring 1 or more disc areas, a part of which lies within 1 disc diameter of the macular center.[80] (A1)
Results indicate that eyes receiving intravitreal bevacizumab experience a median increase of 8 letters on the ETDRS visual acuity chart. In comparison, those treated with laser therapy experience a median decrease of 0.5 letters after 1 year. The likelihood of gaining 10 or more letters on the ETDRS visual acuity chart is 5.1 times higher in the intravitreal bevacizumab cohort.[81] Notably, the use of intravitreal bevacizumab in this capacity is off-label. (A1)
The Ranibizumab Monotherapy or Combined with Laser versus Laser Monotherapy for Diabetic Macular Edema (RESTORE) trial demonstrates that intravitreal ranibizumab 0.5 mg, either as monotherapy or combined with laser, yields greater visual improvement compared to standard laser alone.[82] Additionally, 2 parallel phase III trials indicate that intravitreal ranibizumab at both 0.3 and 0.5 mg doses outperforms sham injections in terms of visual improvement and reduction in central retinal thickness.[83] (A1)
The DRCR Retina Network Protocol I shows that 0.5 mg of intravitreal ranibizumab with prompt or deferred laser produces superior visual gain compared to 4 mg of intravitreal triamcinolone acetonide with laser and laser alone. Visual outcomes produced by intravitreal ranibizumab plus deferred laser are better than those from intravitreal ranibizumab plus prompt laser. Subgroup analysis reveals that intravitreal triamcinolone acetonide plus laser yields similar results to intravitreal ranibizumab plus laser in eyes with pseudophakic macular edema.[84](A1)
The diabetic macular edema and vascular endothelial growth factor trap-eye: Investigation of Clinical Impact (DA VINCI) study demonstrates that intravitreal aflibercept achieves superior anatomical and functional improvement compared to laser therapy.[85] In addition, 2 parallel phase III trials reveal that eyes treated with aflibercept exhibit significantly greater mean visual gain and edema resolution after 1 year compared to laser therapy.[86](A1)
All 3 medications demonstrate comparable efficacy when visual acuity exceeds 20/50. However, when the baseline visual acuity is 20/50 or worse, aflibercept exhibits superior improvement compared to ranibizumab and bevacizumab. The median number of injections and occurrence of adverse events remain consistent across all 3 medications.[87][88] (A1)
The DRCR Retina Network Protocol V shows no significant difference in visual loss at the end of 2 years among eyes with center-involving diabetic macular edema and a best corrected visual acuity of 20/25 or better, irrespective of the treatment. Consistent with current practice, the study proposes clinicians observe patients with good visual acuity and treat them with aflibercept only if the visual acuity worsens.[89](A1)
Retinal vein occlusion: In the Branch Retinal Vein Occlusion (BRAVO) trial, eyes with BRVO receiving 6 monthly intravitreal ranibizumab 0.3 or 0.5 mg injections show superior visual improvement compared to sham injections. Visual acuity at 1 year remains well-maintained even after shifting to as-needed dosing for the subsequent 6 months.[90] The Central Retinal Vein Occlusion (CRUISE) trial yields similar outcomes.[91](A1)
Studies demonstrate that administering 6 monthly aflibercept injections followed by bi-monthly injections results in superior visual benefit and reduced edema compared to macular grid laser in eyes with BRVO-related macular edema at 24 and 52 weeks.[92] Additionally, 2 other studies reveal that 6 monthly aflibercept injections followed by as-needed dosing help achieve more significant visual benefit and edema reduction than macular grid laser in eyes with ventral RVO-related macular edema.[93][94] Brolicizumab (6 mg/0.05 mL) and faricimab (6 mg/0.05 mL) are among the additional available anti-VEGF medications.[95][96] (A1)
Ocular Topical Medications
Nonsteroidal anti-inflammatory drugs: NSAIDs reduce the production of prostaglandins by inhibiting the enzyme cyclooxygenase. Most studies reveal that NSAIDs have a beneficial role in managing pseudophakic cystoid macular edema. However, further well-designed randomized control trials are necessary to establish their efficacy conclusively.[43][97] Bromfenac 0.09%, nepafenac 0.1%, diclofenac 0.1%, ketorolac 0.5%, flurbiprofen 0.03%, and indomethacin 1% have demonstrated efficacy in reducing postoperative inflammation following cataract surgery in randomized controlled clinical trials. Evidence suggests that combining topical NSAIDs with topical corticosteroids in patients with pseudophakic cystoid macular edema provides a synergistic effect (see Image. Pseudophakic Cystoid Macular Edema).
Recent studies indicate improved central subfield thickness in patients with diabetic macular edema who maintain good glycemic control. Patients treated with NSAIDs show more stable intraocular pressure compared to those receiving topical corticosteroids, suggesting a potential advantage. However, further research is needed to confirm these findings. The DRCR Retina Network Protocol R findings suggest that topical nepafenac 0.1% does not significantly affect OCT-measured retinal thickness in eyes with non-center involving diabetic macular edema after 1 year.[98] (A1)
Topical carbonic anhydrase inhibitors: Carbonic anhydrase inhibitors (CAI) inhibit the enzymes carbonic anhydrase and γ-glutamyl transferase, increasing fluid transport from the sub-retinal space toward the choroid. These medications are particularly effective in disorders with diseased retinal pigment epithelium, such as retinal pigment-related macular edema.
Ocular Laser
Ocular lasers can treat macular edema secondary to various diseases.
Diabetic macular edema: Laser therapy is recommended for patients with inadequate response to anti-VEGF therapy. Healthcare providers typically utilize double diode or YAG photocoagulation lasers to treat diabetic macular edema. The ETDRS reveals that laser reduces the risk of moderate visual loss, or a loss of 15 letters on the EDTRS visual chart or a doubling of the visual angle, at 36 months. After 6 weeks, clinicians can treat any untreated initial lesions. Repeat treatment should be scheduled at least 4 months after the initial session if no initial lesions remain.[99]
Diabetic macular edema treatment techniques: The various techniques to manage diabetic macular edema are listed below.
- Focal laser: Focal laser treatment involves addressing lesions situated within 500 to 3000 µm from the macular center using moderate-intensity burns sized 50 to 100 µm for durations of 50 to 100 ms. These lesions typically include microaneurysms, intraretinal microvascular abnormalities, and leaking short capillary segments observed on FFA. Treatment success is indicated by whitening or darkening of the focal lesions, serving as the end point.[100]
- Grid laser: Grid laser treatment targets regions displaying diffuse capillary leakage or nonperfusion observed on FFA within 500 to 3000 µm from the macular center. Clinicians apply burns sized 50 to 200 µm for durations of 50 to 500 ms, placing 2 burn widths apart. The end point of treatment is signified by mild retinal pigment epithelium whitening. Focal leaks within this region have also been addressed. The possible mechanisms of action include improved oxygen supply to the inner retina due to laser-induced damage to oxygen-consuming photoreceptors and retinal pigment epithelium, reduced autoregulatory vasoconstriction, and restoration of the retinal pigment epithelium barrier and pump.[100]
- Modified grid laser: This laser treatment ensures burns are not intense enough to alter the color of microaneurysms. Achieving mild gray-white burns beneath all microaneurysms is considered adequate for effective treatment.[100]
- Mild macular laser photocoagulation: This involves applying light burns that are barely visible or appear as light gray over the macula, including both thickened and normal retina. Microaneurysms are not directly treated during this procedure.[101] (A1)
The DRCR Retina Network Protocol A reports that while the mild macular photocoagulation laser protocol may be less effective in reducing retinal thickness compared to the modified grid laser protocol, both protocols yield similar visual outcomes.[101] Protocol B demonstrates that the modified grid laser protocol is more effective and associated with fewer adverse effects than intravitreal triamcinolone injections over a 2-year period.[102](A1)
Branch retinal vein occlusion: The Branch Retinal Vein Occlusion, Associated Macular Edema study reports that nearly one-third of cases improve spontaneously within the first 3 months. Eyes with persistent macular edema, visual acuity of 20/40 or worse, and an absence of macular ischemia on FFA have better visual outcomes at 3 years when treated with macular grid laser than observation. Clinicians place the grid laser spots in the area of capillary leak located outside the edge of the foveal avascular zone and inside the significant vascular arcades.[103](B3)
Central retinal vein occlusion: The CRUISE trial demonstrates that macular grid laser treatment reduces angiographic evidence of macular edema in central retinal vein occlusion. However, it does not show any significant visual benefit.[104](A1)
Retinal artery macroaneurysm: Clinicians have several options for treating leaking retinal microaneurysms, including direct or indirect laser therapy, or a combination of both. Clinicians perform direct laser by applying 200 to 500 µm size, 200 to 500 ms duration burns over the microaneurysm to seal the aneurysm. However, this can weaken the already thin and distended wall of the aneurysm, potentially leading to complications such as aneurysm rupture, vitreous and preretinal hemorrhage, and arterial occlusion. Clinicians perform indirect laser treatment by applying 100 to 200 ms confluent burns around the lesion. This treatment may reduce the oxygen demand of the surrounding tissue, which subsequently may reduce the blood flow and pressure inside the aneurysm.
Intravitreal Steroids
Fluocinolone acetate: A non-biodegradable intravitreal implant containing fluocinolone acetonide (0.59 mg; Retisert; Bausch and Lomb) is available. Studies reveal that implanting this device achieves better visual and anatomic outcomes than laser in eyes for diabetic macular edema. The rates of cataract progression and IOP elevation to 30 mm Hg or more are 91% and 61.4%, respectively.[105] An additional non-biodegradable, sustained-release device containing fluocinolone acetonide (0.19 mg; Iluvien; Alimera Sciences, Inc) is also available.(A1)
A phase III trial reveals that implantable devices containing either 0.2 or 0.5 μg/d produce superior visual improvement compared to sham injections for up to 3 years. Patients with chronic diabetic macular edema have superior outcomes. Almost all patients with phakic macular edema develop cataracts, but visual improvement is equivalent to pseudophakic macular edema following cataract surgery. The associated incidence of glaucoma is low at 7.6% in high-dose or 0.5 μg/d and 3.7% in the low-dose or 0.2 μg/d groups.[106](A1)
Intravitreal triamcinolone acetonide: The Standard Care Versus Corticosteroid for Retinal Vein Occlusion (SCORE) trial reveals that intravitreal triamcinolone acetonide at doses of 1 mg or 4 mg does not offer significant benefits compared to macular grid laser for macular edema related to BRVO, in terms of visual acuity or foveal thickness. Intravitreal triamcinolone acetonide treatment results in notable adverse effects such as cataracts and elevated IOP. Conversely, intravitreal triamcinolone acetonide demonstrates superiority over observation for macular edema associated with central RVO. Moreover, the safety profile of the 1 mg dose is preferable to the 4 mg dose.[107](A1)
Clinicians may use posterior subtenon triamcinolone injections to address various disorders leading to macular edema.[108] High-dose systemic steroids, including intravenous methylprednisolone, may aid in managing subfoveal fluid in acute Vogt-Koyanagi-Harada disease and sympathetic ophthalmia.[109](B3)
Dexamethasone: Implantable dexamethasone is available in a biodegradable 0.35 or 0.7 mg sustained-release device (Ozurdex; Allergan, Inc.). Studies reveal that the implant meets the primary efficacy end point for visual improvement without monthly injections. However, studies indicate that 67.9% of eyes in the 0.7 mg group develop cataracts, and 27.7% experience a 10-mm Hg or more elevation in IOP.[110] A study demonstrates superior anatomical and similar visual outcomes of the steroid implant compared to bevacizumab for diabetic macular edema with fewer injections.[111] Further research highlights its effectiveness in both BRVO and central RVO compared to sham treatment, with peak visual and anatomical improvement observed after 60 days before subsequent deterioration in vision.[112](A1)
The DRCR Retina Network Protocol U reveals that adding a dexamethasone implant to continued intravitreal ranibizumab therapy is not likely to improve visual acuity at 24 weeks compared to using intravitreal ranibizumab therapy alone in eyes with persistent diabetic macular edema. However, combining these treatments is expected to reduce retinal thickness while potentially increasing IOP.[113](A1)
Further studies comparing anti-VEGF therapy with dexamethasone implants have shown superior results with anti-VEGF injections compared to dexamethasone implants in treating macular edema due to diabetes and RVO. Although implants reduce injection frequency, they carry higher risks of cataracts and steroid-induced glaucoma. Therefore, dexamethasone or any implantable steroid is typically considered second-line therapy. Combination therapy with anti-VEGF medications is not likely superior to anti-VEGF injections alone.
Differential Diagnosis
The differential diagnoses of macular edema include the following conditions:
- Vitreomacular traction and epiretinal membrane
- Autosomal dominant cystoid macular edema due to Müller cell dysfunction
- Juvenile X-linked retinoschisis [72][73]
- Foveoschisis
- Hypotony macular edema due to abnormal retinal capillary permeability secondary to reduced IOP [1][2]
- Congenital cavitary disc maculopathy, including optic nerve head pit or optic disc pit, morning glory anomaly, optic nerve coloboma, and extra-papillary cavitation [114]
- Chronic central serous chorioretinopathy [114][115]
- Microcystic macular edema in advanced glaucoma and optic neuropathy [116]
- Berlin edema or commotio retinae (see Image. Commotio Retinae With Foveal Involvement)[117]
- Macular telangiectasia or idiopathic juxtafoveal telangiectasia [118]
- Central retinal arterial occlusion [119]
Prognosis
The prognosis of macular edema typically varies based on its underlying cause. Approximately 33% to 35% of individuals with diabetic macular edema experience spontaneous resolution within 6 months. With the advent of newer pharmacological agents for intravitreal injection, the prognosis of most retinal disorders has improved.
Several OCT biomarkers can aid in determining the prognosis of macular edema, as mentioned below.
Disorganization of the inner retinal layers: This is characterized by the inability to distinguish boundaries between any 2 of the following—ganglion cell–inner plexiform layer complex, inner nuclear layer, or the outer plexiform layer in more than 50% of the foveal 1-mm zone defines disorganization of the inner retinal layers. A poor visual prognosis is anticipated when disorganization of the inner retinal layers affects 50% or more of the central foveal 1 mm.[120]
Hyperreflective retinal foci: These indicate subclinical lipoproteins or other materials that extravasate following the breakdown of the inner blood-retinal barrier. Their presence indicates a high chance of subfoveal hard exudate deposition after the resolution of macular edema.[121]
Intraretinal cystoid spaces: These serve as indicators of Müller cell malfunction, and their prognostic significance depends on their size. Small cysts measure less than 100 µm, whereas large ones range from 101 to 200 µm, and giant cysts exceed 200 µm. Additionally, their location and association with hyperreflective material, composed of fibrin and inflammatory by-products, further determine their prognostic significance, signifying severe blood-retinal barrier disruption. The hyperreflective material observed on OCT angiography manifests as an extravascular signal attributed to particulate Brownian motion, termed suspended scattering particles in motion. Typically located at the vascular-avascular junction, these signals often resolve with the formation of hard exudates.[122][123] Large cysts are usually associated with macular ischemia, whereas giant cysts tend to inflict damage on the outer nuclear layer and ellipsoid zone, resulting in poorer visual outcomes.
Photoreceptor outer segment: This refers to the length between the junction of the inner and outer segments of the photoreceptor and the retinal pigment epithelium. Shorter lengths are often associated with poorer visual acuity.[124]
The integrity of the external limiting membrane and ellipsoid zone: The integrity of outer retinal layers indicates the health of photoreceptors and retinal pigment epithelium.[125]
Complications
If left untreated, macular edema can lead to irreversible vision loss.[126] Additional complications may include damage to the central retinal tissue, foveal atrophy, epiretinal membrane, macular ischemia, lamellar macular hole, and macular fibrosis. However, the various treatment modalities may also carry risks of additional complications. For instance, laser photocoagulation may lead to accidental foveal burns, subretinal fibrosis, scarring, and choroidal neovascular membranes. Intravitreal injections pose the risk of severe complications such as endophthalmitis, as well as vitreous hemorrhage, central retinal artery occlusion, and retinal tears.[127] Risks specific to anti-VEGF medications include cerebrovascular accidents, vasculitis with occlusion, and retinal occlusion, while corticosteroids may cause cataracts and steroid-induced glaucoma.
Deterrence and Patient Education
Macular edema, characterized by fluid accumulation in the macula of the eye, can result in vision loss if left untreated. Early detection and treatment are vital for individuals at risk to prevent irreversible damage to vision. The American Academy of Ophthalmology recommends ophthalmic screening for patients with type 1 diabetes within 5 years of diagnosis and those with type 2 diabetes at the time of diagnosis.[128] Regular eye examinations are crucial, especially for individuals with diabetes or a history of RVO, as these conditions heighten the risk of developing macular edema. Patients should be vigilant for symptoms such as blurred or distorted vision, central blind spots, or difficulty reading the fine print and promptly report any changes to their eye care professional
Maintaining strict control of blood sugar, blood pressure, and cholesterol levels and quitting smoking can mitigate the risk of developing macular edema or slow its progression. Additionally, patients must be aware of available treatment options, including anti-VEGF injections, corticosteroid injections, or laser therapy, and the importance of adhering to their treatment plan to preserve their vision. Through proactive engagement and staying well-informed about their eye health, patients can effectively manage their condition and mitigate the impact of macular edema on their overall quality of life.
Enhancing Healthcare Team Outcomes
Macular edema, characterized by fluid accumulation in the macula of the eye, is a prevalent and potentially vision-threatening condition that demands vigilant recognition and management by clinicians. This condition occurs secondary to underlying pathologies, including diabetes, RVO, uveitis, and other retinal diseases. Clinicians should be aware of recognizing typical symptoms, including blurred or distorted vision, central blind spots, and difficulty reading fine print. Diagnosis involves a comprehensive eye examination, including OCT and FFA. Depending on the underlying cause and severity of the edema, treatment options may include intravitreal injections of anti-VEGF agents, corticosteroids, or laser therapy.
Healthcare professionals, encompassing physicians, advanced care practitioners, nurses, pharmacists, and dieticians, should leverage their clinical expertise for diagnosing and developing personalized treatment plans for individual patients. Vigilant monitoring by a multidisciplinary healthcare team is essential to enable timely intervention, avert irreversible vision loss, monitor for potential adverse treatment effects, and optimize patient outcomes. Effective interprofessional communication is crucial for comprehensive care planning, collaborative problem-solving, and informed decision-making, fostering a cohesive approach to management. Through coordinated efforts across disciplines, the healthcare team can minimize delays, avoid redundant services, and enhance the overall efficiency and effectiveness of care delivery. Ultimately, by leveraging their collective skills, strategy, interprofessional communication, and care coordination, healthcare professionals can deliver holistic, patient-centered care that maximizes outcomes, ensures patient safety, and enhances team performance in addressing macular edema.
Media
(Click Image to Enlarge)
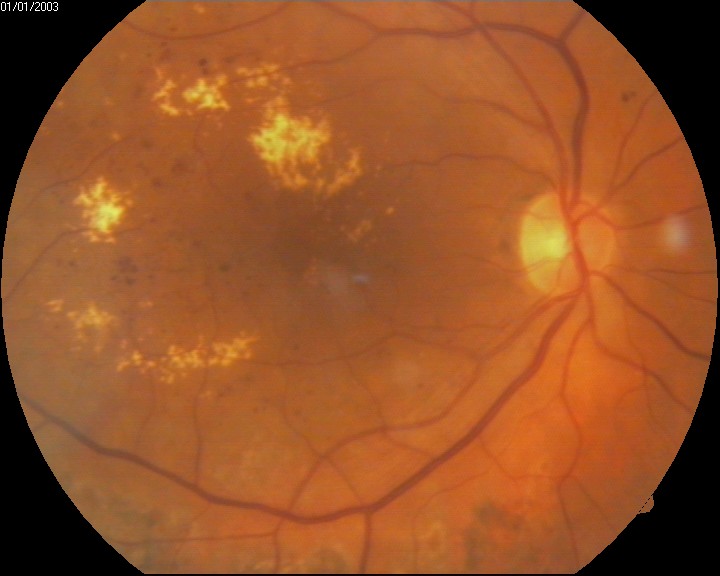
Macular Edema Associated With Diabetes.
Contributed by U Shukla, MS, DNB, FVRS, PhD
(Click Image to Enlarge)

Cystoid Macular Edema, Uveitis. This optical coherence tomography image shows cystoid macular edema in a patient with uveitis.
Contributed by BCK Patel, MD
(Click Image to Enlarge)
Commotio Retinae With Foveal Involvement. This image displays the commotio retinae of a patient with foveal involvement, also known as Berlin edema.
Contributed by K Tripathy, MD
(Click Image to Enlarge)

Multimodal Imaging of Diabetic Macular Edema. This image set showcases fundus photography, fundus fluorescein angiography, and optical coherence tomography scans, providing a comprehensive view of diabetic macular edema and its manifestations across different imaging modalities.
Aravind Eye Hospital, Madurai
(Click Image to Enlarge)
Pseudophakic Cystoid Macular Edema. Optical coherence tomography reveals cystoid macular edema with accompanying subretinal fluid in a patient with pseudophakic cystoid macular edema.
Aravind Eye Hospital, Madurai
(Click Image to Enlarge)

Juvenile X-Linked Retinoschisis. The fundus autofluorescence images exhibit a spoke-wheel pattern centered at the fovea. Additionally, optical coherence tomography reveals vertical tissue bridges connecting the inner and outer retina, characteristic of juvenile X-linked retinoschisis.
Aravind Eye Hospital, Madurai
References
Tranos PG, Wickremasinghe SS, Stangos NT, Topouzis F, Tsinopoulos I, Pavesio CE. Macular edema. Survey of ophthalmology. 2004 Sep-Oct:49(5):470-90 [PubMed PMID: 15325193]
Level 3 (low-level) evidenceRotsos TG, Moschos MM. Cystoid macular edema. Clinical ophthalmology (Auckland, N.Z.). 2008 Dec:2(4):919-30 [PubMed PMID: 19668445]
Coscas G, Cunha-Vaz J, Soubrane G. Macular edema: definition and basic concepts. Developments in ophthalmology. 2010:47():1-9. doi: 10.1159/000320070. Epub 2010 Aug 10 [PubMed PMID: 20703040]
Daruich A, Matet A, Moulin A, Kowalczuk L, Nicolas M, Sellam A, Rothschild PR, Omri S, Gélizé E, Jonet L, Delaunay K, De Kozak Y, Berdugo M, Zhao M, Crisanti P, Behar-Cohen F. Mechanisms of macular edema: Beyond the surface. Progress in retinal and eye research. 2018 Mar:63():20-68. doi: 10.1016/j.preteyeres.2017.10.006. Epub 2017 Nov 7 [PubMed PMID: 29126927]
Haydinger CD, Ferreira LB, Williams KA, Smith JR. Mechanisms of macular edema. Frontiers in medicine. 2023:10():1128811. doi: 10.3389/fmed.2023.1128811. Epub 2023 Mar 7 [PubMed PMID: 36960343]
Scholl S, Kirchhof J, Augustin AJ. Pathophysiology of macular edema. Ophthalmologica. Journal international d'ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 2010:224 Suppl 1():8-15. doi: 10.1159/000315155. Epub 2010 Aug 18 [PubMed PMID: 20714176]
Cunha-Vaz J. Mechanisms of Retinal Fluid Accumulation and Blood-Retinal Barrier Breakdown. Developments in ophthalmology. 2017:58():11-20. doi: 10.1159/000455265. Epub 2017 Mar 28 [PubMed PMID: 28351041]
Gupta A, Tripathy K. Central Serous Chorioretinopathy. StatPearls. 2024 Jan:(): [PubMed PMID: 32644399]
Venkatesh P, Chawla R, Tripathy K, Singh HI, Bypareddy R. Scleral resection in chronic central serous chorioretinopathy complicated by exudative retinal detachment. Eye and vision (London, England). 2016:3(1):23. doi: 10.1186/s40662-016-0055-5. Epub 2016 Sep 9 [PubMed PMID: 27617266]
Paulbuddhe V, Addya S, Gurnani B, Singh D, Tripathy K, Chawla R. Sympathetic Ophthalmia: Where Do We Currently Stand on Treatment Strategies? Clinical ophthalmology (Auckland, N.Z.). 2021:15():4201-4218. doi: 10.2147/OPTH.S289688. Epub 2021 Oct 20 [PubMed PMID: 34707340]
Tripathy K, Mittal K, Chawla R. Sympathetic ophthalmia following a conjunctival flap procedure for corneal perforation. BMJ case reports. 2016 Mar 14:2016():. doi: 10.1136/bcr-2016-214344. Epub 2016 Mar 14 [PubMed PMID: 26976837]
Level 3 (low-level) evidenceChawla R, Kapoor M, Mehta A, Tripathy K, Vohra R, Venkatesh P. Sympathetic Ophthalmia: Experience from a Tertiary Care Center in Northern India. Journal of ophthalmic & vision research. 2018 Oct-Dec:13(4):439-446. doi: 10.4103/jovr.jovr_86_17. Epub [PubMed PMID: 30479714]
Shukla UV, Tripathy K. Diabetic Retinopathy. StatPearls. 2024 Jan:(): [PubMed PMID: 32809640]
Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye and vision (London, England). 2015:2():17. doi: 10.1186/s40662-015-0026-2. Epub 2015 Sep 30 [PubMed PMID: 26605370]
Rogers S, McIntosh RL, Cheung N, Lim L, Wang JJ, Mitchell P, Kowalski JW, Nguyen H, Wong TY, International Eye Disease Consortium. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology. 2010 Feb:117(2):313-9.e1. doi: 10.1016/j.ophtha.2009.07.017. Epub [PubMed PMID: 20022117]
Level 1 (high-level) evidenceLaouri M, Chen E, Looman M, Gallagher M. The burden of disease of retinal vein occlusion: review of the literature. Eye (London, England). 2011 Aug:25(8):981-8. doi: 10.1038/eye.2011.92. Epub 2011 May 6 [PubMed PMID: 21546916]
Petrella RJ, Blouin J, Davies B, Barbeau M. Incidence and Characteristics of Patients with Visual Impairment due to Macular Edema Secondary to Retinal Vein Occlusion in a Representative Canadian Cohort. Journal of ophthalmology. 2012:2012():723169. doi: 10.1155/2012/723169. Epub 2012 Oct 14 [PubMed PMID: 23097691]
El Jammal T, Loria O, Jamilloux Y, Gerfaud-Valentin M, Kodjikian L, Sève P. Uveitis as an Open Window to Systemic Inflammatory Diseases. Journal of clinical medicine. 2021 Jan 14:10(2):. doi: 10.3390/jcm10020281. Epub 2021 Jan 14 [PubMed PMID: 33466638]
Henderson BA, Kim JY, Ament CS, Ferrufino-Ponce ZK, Grabowska A, Cremers SL. Clinical pseudophakic cystoid macular edema. Risk factors for development and duration after treatment. Journal of cataract and refractive surgery. 2007 Sep:33(9):1550-8 [PubMed PMID: 17720069]
Flach AJ. The incidence, pathogenesis and treatment of cystoid macular edema following cataract surgery. Transactions of the American Ophthalmological Society. 1998:96():557-634 [PubMed PMID: 10360304]
Perente I, Utine CA, Ozturker C, Cakir M, Kaya V, Eren H, Kapran Z, Yilmaz OF. Evaluation of macular changes after uncomplicated phacoemulsification surgery by optical coherence tomography. Current eye research. 2007 Mar:32(3):241-7 [PubMed PMID: 17453944]
Koronis S, Stavrakas P, Balidis M, Kozeis N, Tranos PG. Update in treatment of uveitic macular edema. Drug design, development and therapy. 2019:13():667-680. doi: 10.2147/DDDT.S166092. Epub 2019 Feb 19 [PubMed PMID: 30858697]
Molaie AM, Pramil V, Hedges TR 3rd, Tomb LC, Vuong LN. Vitreoretinal Findings in Nonarteritic Ischemic Optic Neuropathy. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2022 Mar 1:42(1):e124-e129. doi: 10.1097/WNO.0000000000001264. Epub 2021 Apr 26 [PubMed PMID: 34001734]
Hedges TR 3rd, Vuong LN, Gonzalez-Garcia AO, Mendoza-Santiesteban CE, Amaro-Quierza ML. Subretinal fluid from anterior ischemic optic neuropathy demonstrated by optical coherence tomography. Archives of ophthalmology (Chicago, Ill. : 1960). 2008 Jun:126(6):812-5. doi: 10.1001/archopht.126.6.812. Epub [PubMed PMID: 18541844]
Strong S, Liew G, Michaelides M. Retinitis pigmentosa-associated cystoid macular oedema: pathogenesis and avenues of intervention. The British journal of ophthalmology. 2017 Jan:101(1):31-37. doi: 10.1136/bjophthalmol-2016-309376. Epub 2016 Dec 2 [PubMed PMID: 27913439]
Cunha-Vaz J, Bernardes R, Lobo C. Blood-retinal barrier. European journal of ophthalmology. 2011:21 Suppl 6():S3-9. doi: 10.5301/EJO.2010.6049. Epub [PubMed PMID: 23264323]
Owen LA, Hartnett ME. Soluble mediators of diabetic macular edema: the diagnostic role of aqueous VEGF and cytokine levels in diabetic macular edema. Current diabetes reports. 2013 Aug:13(4):476-80. doi: 10.1007/s11892-013-0382-z. Epub [PubMed PMID: 23649946]
Ascaso FJ, Huerva V, Grzybowski A. The role of inflammation in the pathogenesis of macular edema secondary to retinal vascular diseases. Mediators of inflammation. 2014:2014():432685. doi: 10.1155/2014/432685. Epub 2014 Jul 22 [PubMed PMID: 25152567]
Toklu Y, Sarac O, Berk S, Simsek S. Angioedema after intravitreal bevacizumab injection. Cutaneous and ocular toxicology. 2012 Mar:31(1):85-6. doi: 10.3109/15569527.2011.609207. Epub [PubMed PMID: 22309281]
Level 3 (low-level) evidenceSpaide RF, Jaffe GJ, Sarraf D, Freund KB, Sadda SR, Staurenghi G, Waheed NK, Chakravarthy U, Rosenfeld PJ, Holz FG, Souied EH, Cohen SY, Querques G, Ohno-Matsui K, Boyer D, Gaudric A, Blodi B, Baumal CR, Li X, Coscas GJ, Brucker A, Singerman L, Luthert P, Schmitz-Valckenberg S, Schmidt-Erfurth U, Grossniklaus HE, Wilson DJ, Guymer R, Yannuzzi LA, Chew EY, Csaky K, Monés JM, Pauleikhoff D, Tadayoni R, Fujimoto J. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology. 2020 May:127(5):616-636. doi: 10.1016/j.ophtha.2019.11.004. Epub 2019 Nov 14 [PubMed PMID: 31864668]
Level 3 (low-level) evidenceYeo NJY, Chan EJJ, Cheung C. Choroidal Neovascularization: Mechanisms of Endothelial Dysfunction. Frontiers in pharmacology. 2019:10():1363. doi: 10.3389/fphar.2019.01363. Epub 2019 Nov 29 [PubMed PMID: 31849644]
Gupta A, Paulbuddhe VS, Shukla UV, Tripathy K. Exudative Retinitis (Coats Disease). StatPearls. 2024 Jan:(): [PubMed PMID: 32809517]
Sen M, Shields CL, Honavar SG, Shields JA. Coats disease: An overview of classification, management and outcomes. Indian journal of ophthalmology. 2019 Jun:67(6):763-771. doi: 10.4103/ijo.IJO_841_19. Epub [PubMed PMID: 31124484]
Level 3 (low-level) evidencePitkänen L, Tommila P, Kaarniranta K, Jääskeläinen JE, Kinnunen K. Retinal arterial macroaneurysms. Acta ophthalmologica. 2014 Mar:92(2):101-4. doi: 10.1111/aos.12210. Epub 2013 Jun 25 [PubMed PMID: 23800325]
Singh D, Tripathy K. Retinal Macroaneurysm. StatPearls. 2024 Jan:(): [PubMed PMID: 35015432]
García-O'Farrill N, Pugazhendhi S, Karth PA, Hunter AA. Radiation retinopathy intricacies and advances in management. Seminars in ophthalmology. 2022 May 19:37(4):417-435. doi: 10.1080/08820538.2021.2000623. Epub 2021 Dec 7 [PubMed PMID: 34874814]
Level 3 (low-level) evidenceSahoo NK, Ranjan R, Tyagi M, Agrawal H, Reddy S. Radiation Retinopathy: Detection and Management Strategies. Clinical ophthalmology (Auckland, N.Z.). 2021:15():3797-3809. doi: 10.2147/OPTH.S219268. Epub 2021 Sep 8 [PubMed PMID: 34526764]
Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, Shank B, Solin LJ, Wesson M. Tolerance of normal tissue to therapeutic irradiation. International journal of radiation oncology, biology, physics. 1991 May 15:21(1):109-22 [PubMed PMID: 2032882]
Lambrecht M, Eekers DBP, Alapetite C, Burnet NG, Calugaru V, Coremans IEM, Fossati P, Høyer M, Langendijk JA, Méndez Romero A, Paulsen F, Perpar A, Renard L, de Ruysscher D, Timmermann B, Vitek P, Weber DC, van der Weide HL, Whitfield GA, Wiggenraad R, Roelofs E, Nyström PW, Troost EGC, work package 1 of the taskforce “European Particle Therapy Network” of ESTRO. Radiation dose constraints for organs at risk in neuro-oncology; the European Particle Therapy Network consensus. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2018 Jul:128(1):26-36. doi: 10.1016/j.radonc.2018.05.001. Epub 2018 May 17 [PubMed PMID: 29779919]
Level 3 (low-level) evidenceBrown GC, Shields JA, Sanborn G, Augsburger JJ, Savino PJ, Schatz NJ. Radiation retinopathy. Ophthalmology. 1982 Dec:89(12):1494-501 [PubMed PMID: 7162794]
Horgan N, Shields CL, Mashayekhi A, Shields JA. Classification and treatment of radiation maculopathy. Current opinion in ophthalmology. 2010 May:21(3):233-8. doi: 10.1097/ICU.0b013e3283386687. Epub [PubMed PMID: 20393294]
Level 3 (low-level) evidenceCimolai N. Comment on "Insights into the pathogenesis of cystoid macular edema: leukostasis and related cytokines". International journal of ophthalmology. 2020:13(8):1343-1344. doi: 10.18240/ijo.2020.08.25. Epub 2020 Aug 18 [PubMed PMID: 32821693]
Level 3 (low-level) evidenceGrzybowski A, Sikorski BL, Ascaso FJ, Huerva V. Pseudophakic cystoid macular edema: update 2016. Clinical interventions in aging. 2016:11():1221-1229 [PubMed PMID: 27672316]
Mahendradas P, Kawali A, Luthra S, Srinivasan S, Curi AL, Maheswari S, Ksiaa I, Khairallah M. Post-fever retinitis - Newer concepts. Indian journal of ophthalmology. 2020 Sep:68(9):1775-1786. doi: 10.4103/ijo.IJO_1352_20. Epub [PubMed PMID: 32823394]
Chauhan K, Tripathy K. Pars Planitis. StatPearls. 2024 Jan:(): [PubMed PMID: 28613790]
Tripathy K. Cystoid Macular Edema in Retinitis Pigmentosa with Intermediate Uveitis Responded Well to Oral and Posterior Subtenon Steroid. Seminars in ophthalmology. 2018:33(4):492-493. doi: 10.1080/08820538.2017.1303521. Epub 2017 Mar 29 [PubMed PMID: 28353369]
Tripathy K, Chawla R, Venkatesh P, Vohra R, Sharma YR, Gogia V, Jain S, Behera A. Ultra-wide Field Fluorescein Angiography in Retinitis Pigmentosa with Intermediate Uveitis. Journal of ophthalmic & vision research. 2016 Apr-Jun:11(2):237-9. doi: 10.4103/2008-322X.183929. Epub [PubMed PMID: 27413510]
Geetha R, Tripathy K. Chorioretinitis. StatPearls. 2024 Jan:(): [PubMed PMID: 31869169]
Mackool RJ, Muldoon T, Fortier A, Nelson D. Epinephrine-induced cystoid macular edema in aphakic eyes. Archives of ophthalmology (Chicago, Ill. : 1960). 1977 May:95(5):791-3 [PubMed PMID: 860942]
Drenser K, Sarraf D, Jain A, Small KW. Crystalline retinopathies. Survey of ophthalmology. 2006 Nov-Dec:51(6):535-49 [PubMed PMID: 17134644]
Level 3 (low-level) evidenceMillay RH, Klein ML, Illingworth DR. Niacin maculopathy. Ophthalmology. 1988 Jul:95(7):930-6 [PubMed PMID: 3174043]
Level 3 (low-level) evidenceDomanico D, Verboschi F, Altimari S, Zompatori L, Vingolo EM. Ocular Effects of Niacin: A Review of the Literature. Medical hypothesis, discovery & innovation ophthalmology journal. 2015 Summer:4(2):64-71 [PubMed PMID: 26060832]
Tripathy K, Patel P, Geetha R. Latanoprost. StatPearls. 2024 Jan:(): [PubMed PMID: 31082022]
Chawla R, Tripathy K, Sharma A, Vohra R. Swept source optical coherence tomography-angiography of choroid in choroidal hemangioma before and after laser photocoagulation. Indian journal of ophthalmology. 2017 Aug:65(8):751-754. doi: 10.4103/ijo.IJO_974_16. Epub [PubMed PMID: 28820167]
Garoon RB, Shields CL, Kaliki S, Shields JA. Cystoid macular edema as the initial manifestation of choroidal melanoma. Oman journal of ophthalmology. 2012 Sep:5(3):187-8. doi: 10.4103/0974-620X.106104. Epub [PubMed PMID: 23440248]
Elnahry AG, Tripathy K. Gyrate Atrophy of the Choroid and Retina. StatPearls. 2024 Jan:(): [PubMed PMID: 32491691]
Mansour AM, Elnahry AG, Tripathy K, Foster RE, Mehanna CJ, Vishal R, Çavdarlı C, Arrigo A, Parodi MB. Analysis of optical coherence angiography in cystoid macular oedema associated with gyrate atrophy. Eye (London, England). 2021 Jun:35(6):1766-1774. doi: 10.1038/s41433-020-01166-6. Epub 2020 Sep 1 [PubMed PMID: 32873946]
Tripathy K, Chawla R, Sharma YR, Gogia V. Ultrawide field fluorescein angiogram in a family with gyrate atrophy and foveoschisis. Oman journal of ophthalmology. 2016 May-Aug:9(2):104-6. doi: 10.4103/0974-620X.184529. Epub [PubMed PMID: 27433038]
Jena S, Tripathy K, Chawla R, Mansour AM. Ultrawide field imaging to document the progression of gyrate atrophy of the choroid and retina over 5 years. BMJ case reports. 2021 Aug 17:14(8):. doi: 10.1136/bcr-2021-244695. Epub 2021 Aug 17 [PubMed PMID: 34404670]
Level 3 (low-level) evidenceDave VP, Pappuru RR. An unusual presentation of nonarteritic ischemic optic neuropathy with subretinal fluid treated with intravitreal bevacizumab. Indian journal of ophthalmology. 2016 Jan:64(1):87-8. doi: 10.4103/0301-4738.178143. Epub [PubMed PMID: 26953030]
Patel R, Patel BC, Chauhan S. Neuroretinitis. StatPearls. 2024 Jan:(): [PubMed PMID: 34033389]
Cunha-Vaz JG, Travassos A. Breakdown of the blood-retinal barriers and cystoid macular edema. Survey of ophthalmology. 1984 May:28 Suppl():485-92 [PubMed PMID: 6379947]
Level 3 (low-level) evidenceWolter JR. The histopathology of cystoid macular edema. Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. Albrecht von Graefe's archive for clinical and experimental ophthalmology. 1981:216(2):85-101 [PubMed PMID: 6910356]
Cusick M, Chew EY, Chan CC, Kruth HS, Murphy RP, Ferris FL 3rd. Histopathology and regression of retinal hard exudates in diabetic retinopathy after reduction of elevated serum lipid levels. Ophthalmology. 2003 Nov:110(11):2126-33 [PubMed PMID: 14597519]
Little K, Ma JH, Yang N, Chen M, Xu H. Myofibroblasts in macular fibrosis secondary to neovascular age-related macular degeneration - the potential sources and molecular cues for their recruitment and activation. EBioMedicine. 2018 Dec:38():283-291. doi: 10.1016/j.ebiom.2018.11.029. Epub 2018 Nov 22 [PubMed PMID: 30473378]
Kaur K, Gurnani B. Slit-Lamp Biomicroscope. StatPearls. 2025 Jan:(): [PubMed PMID: 36512656]
Martinez J, Smiddy WE, Kim J, Gass JD. Differentiating macular holes from macular pseudoholes. American journal of ophthalmology. 1994 Jun 15:117(6):762-7 [PubMed PMID: 8198160]
Sander B, Larsen M, Engler C, Strøm C, Moldow B, Larsen N, Lund-Andersen H. Diabetic macular oedema: a comparison of vitreous fluorometry, angiography, and retinopathy. The British journal of ophthalmology. 2002 Mar:86(3):316-20 [PubMed PMID: 11864891]
Level 2 (mid-level) evidenceLaursen ML, Moeller F, Sander B, Sjoelie AK. Subthreshold micropulse diode laser treatment in diabetic macular oedema. The British journal of ophthalmology. 2004 Sep:88(9):1173-9 [PubMed PMID: 15317711]
Level 3 (low-level) evidenceRuia S, Tripathy K. Fluorescein Angiography. StatPearls. 2024 Jan:(): [PubMed PMID: 35015403]
Naseripour M, Hemmati S, Chaibakhsh S, Gordiz A, Miri L, Abdi F. Cystoid macular oedema without leakage in fluorescein angiography: a literature review. Eye (London, England). 2023 Jun:37(8):1519-1526. doi: 10.1038/s41433-022-02230-z. Epub 2022 Sep 10 [PubMed PMID: 36088420]
Prenner JL, Capone A Jr, Ciaccia S, Takada Y, Sieving PA, Trese MT. Congenital X-linked retinoschisis classification system. Retina (Philadelphia, Pa.). 2006 Sep:26(7 Suppl):S61-4 [PubMed PMID: 16946682]
Level 2 (mid-level) evidenceRao P, Dedania VS, Drenser KA. Congenital X-Linked Retinoschisis: An Updated Clinical Review. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2018 May-Jun:7(3):169-175. doi: 10.22608/APO.201803. Epub 2018 Apr 9 [PubMed PMID: 29633586]
Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, Davis M, Rand L, Siebert C. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The New England journal of medicine. 1993 Sep 30:329(14):977-86 [PubMed PMID: 8366922]
Level 1 (high-level) evidence. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet (London, England). 1998 Sep 12:352(9131):837-53 [PubMed PMID: 9742976]
Level 1 (high-level) evidenceACCORD Study Group, ACCORD Eye Study Group, Chew EY, Ambrosius WT, Davis MD, Danis RP, Gangaputra S, Greven CM, Hubbard L, Esser BA, Lovato JF, Perdue LH, Goff DC Jr, Cushman WC, Ginsberg HN, Elam MB, Genuth S, Gerstein HC, Schubart U, Fine LJ. Effects of medical therapies on retinopathy progression in type 2 diabetes. The New England journal of medicine. 2010 Jul 15:363(3):233-44. doi: 10.1056/NEJMoa1001288. Epub 2010 Jun 29 [PubMed PMID: 20587587]
Level 1 (high-level) evidenceKeech AC, Mitchell P, Summanen PA, O'Day J, Davis TM, Moffitt MS, Taskinen MR, Simes RJ, Tse D, Williamson E, Merrifield A, Laatikainen LT, d'Emden MC, Crimet DC, O'Connell RL, Colman PG, FIELD study investigators. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): a randomised controlled trial. Lancet (London, England). 2007 Nov 17:370(9600):1687-97 [PubMed PMID: 17988728]
Level 1 (high-level) evidenceNg EW, Shima DT, Calias P, Cunningham ET Jr, Guyer DR, Adamis AP. Pegaptanib, a targeted anti-VEGF aptamer for ocular vascular disease. Nature reviews. Drug discovery. 2006 Feb:5(2):123-32 [PubMed PMID: 16518379]
Level 3 (low-level) evidenceDiabetic Retinopathy Clinical Research Network, Scott IU, Edwards AR, Beck RW, Bressler NM, Chan CK, Elman MJ, Friedman SM, Greven CM, Maturi RK, Pieramici DJ, Shami M, Singerman LJ, Stockdale CR. A phase II randomized clinical trial of intravitreal bevacizumab for diabetic macular edema. Ophthalmology. 2007 Oct:114(10):1860-7 [PubMed PMID: 17698196]
Level 3 (low-level) evidence. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Archives of ophthalmology (Chicago, Ill. : 1960). 1985 Dec:103(12):1796-806 [PubMed PMID: 2866759]
Level 1 (high-level) evidenceMichaelides M, Kaines A, Hamilton RD, Fraser-Bell S, Rajendram R, Quhill F, Boos CJ, Xing W, Egan C, Peto T, Bunce C, Leslie RD, Hykin PG. A prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (BOLT study) 12-month data: report 2. Ophthalmology. 2010 Jun:117(6):1078-1086.e2. doi: 10.1016/j.ophtha.2010.03.045. Epub 2010 Apr 22 [PubMed PMID: 20416952]
Level 1 (high-level) evidenceMitchell P, Bandello F, Schmidt-Erfurth U, Lang GE, Massin P, Schlingemann RO, Sutter F, Simader C, Burian G, Gerstner O, Weichselberger A, RESTORE study group. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011 Apr:118(4):615-25. doi: 10.1016/j.ophtha.2011.01.031. Epub [PubMed PMID: 21459215]
Level 1 (high-level) evidenceNguyen QD, Brown DM, Marcus DM, Boyer DS, Patel S, Feiner L, Gibson A, Sy J, Rundle AC, Hopkins JJ, Rubio RG, Ehrlich JS, RISE and RIDE Research Group. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology. 2012 Apr:119(4):789-801. doi: 10.1016/j.ophtha.2011.12.039. Epub 2012 Feb 11 [PubMed PMID: 22330964]
Level 1 (high-level) evidenceElman MJ, Bressler NM, Qin H, Beck RW, Ferris FL 3rd, Friedman SM, Glassman AR, Scott IU, Stockdale CR, Sun JK, Diabetic Retinopathy Clinical Research Network. Expanded 2-year follow-up of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2011 Apr:118(4):609-14. doi: 10.1016/j.ophtha.2010.12.033. Epub [PubMed PMID: 21459214]
Level 1 (high-level) evidenceDo DV, Nguyen QD, Boyer D, Schmidt-Erfurth U, Brown DM, Vitti R, Berliner AJ, Gao B, Zeitz O, Ruckert R, Schmelter T, Sandbrink R, Heier JS, da Vinci Study Group. One-year outcomes of the da Vinci Study of VEGF Trap-Eye in eyes with diabetic macular edema. Ophthalmology. 2012 Aug:119(8):1658-65. doi: 10.1016/j.ophtha.2012.02.010. Epub 2012 Apr 24 [PubMed PMID: 22537617]
Level 1 (high-level) evidenceBrown DM, Schmidt-Erfurth U, Do DV, Holz FG, Boyer DS, Midena E, Heier JS, Terasaki H, Kaiser PK, Marcus DM, Nguyen QD, Jaffe GJ, Slakter JS, Simader C, Soo Y, Schmelter T, Yancopoulos GD, Stahl N, Vitti R, Berliner AJ, Zeitz O, Metzig C, Korobelnik JF. Intravitreal Aflibercept for Diabetic Macular Edema: 100-Week Results From the VISTA and VIVID Studies. Ophthalmology. 2015 Oct:122(10):2044-52. doi: 10.1016/j.ophtha.2015.06.017. Epub 2015 Jul 18 [PubMed PMID: 26198808]
Diabetic Retinopathy Clinical Research Network, Wells JA, Glassman AR, Ayala AR, Jampol LM, Aiello LP, Antoszyk AN, Arnold-Bush B, Baker CW, Bressler NM, Browning DJ, Elman MJ, Ferris FL, Friedman SM, Melia M, Pieramici DJ, Sun JK, Beck RW. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. The New England journal of medicine. 2015 Mar 26:372(13):1193-203. doi: 10.1056/NEJMoa1414264. Epub 2015 Feb 18 [PubMed PMID: 25692915]
Level 1 (high-level) evidenceWells JA, Glassman AR, Ayala AR, Jampol LM, Bressler NM, Bressler SB, Brucker AJ, Ferris FL, Hampton GR, Jhaveri C, Melia M, Beck RW, Diabetic Retinopathy Clinical Research Network. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema: Two-Year Results from a Comparative Effectiveness Randomized Clinical Trial. Ophthalmology. 2016 Jun:123(6):1351-9. doi: 10.1016/j.ophtha.2016.02.022. Epub 2016 Feb 27 [PubMed PMID: 26935357]
Level 2 (mid-level) evidenceBaker CW, Glassman AR, Beaulieu WT, Antoszyk AN, Browning DJ, Chalam KV, Grover S, Jampol LM, Jhaveri CD, Melia M, Stockdale CR, Martin DF, Sun JK, DRCR Retina Network. Effect of Initial Management With Aflibercept vs Laser Photocoagulation vs Observation on Vision Loss Among Patients With Diabetic Macular Edema Involving the Center of the Macula and Good Visual Acuity: A Randomized Clinical Trial. JAMA. 2019 May 21:321(19):1880-1894. doi: 10.1001/jama.2019.5790. Epub [PubMed PMID: 31037289]
Level 1 (high-level) evidenceCampochiaro PA, Heier JS, Feiner L, Gray S, Saroj N, Rundle AC, Murahashi WY, Rubio RG, BRAVO Investigators. Ranibizumab for macular edema following branch retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010 Jun:117(6):1102-1112.e1. doi: 10.1016/j.ophtha.2010.02.021. Epub 2010 Apr 15 [PubMed PMID: 20398941]
Level 1 (high-level) evidenceBrown DM, Campochiaro PA, Singh RP, Li Z, Gray S, Saroj N, Rundle AC, Rubio RG, Murahashi WY, CRUISE Investigators. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010 Jun:117(6):1124-1133.e1. doi: 10.1016/j.ophtha.2010.02.022. Epub 2010 Apr 9 [PubMed PMID: 20381871]
Level 1 (high-level) evidenceClark WL, Boyer DS, Heier JS, Brown DM, Haller JA, Vitti R, Kazmi H, Berliner AJ, Erickson K, Chu KW, Soo Y, Cheng Y, Campochiaro PA. Intravitreal Aflibercept for Macular Edema Following Branch Retinal Vein Occlusion: 52-Week Results of the VIBRANT Study. Ophthalmology. 2016 Feb:123(2):330-336. doi: 10.1016/j.ophtha.2015.09.035. Epub 2015 Oct 30 [PubMed PMID: 26522708]
Brown DM, Heier JS, Clark WL, Boyer DS, Vitti R, Berliner AJ, Zeitz O, Sandbrink R, Zhu X, Haller JA. Intravitreal aflibercept injection for macular edema secondary to central retinal vein occlusion: 1-year results from the phase 3 COPERNICUS study. American journal of ophthalmology. 2013 Mar:155(3):429-437.e7. doi: 10.1016/j.ajo.2012.09.026. Epub 2012 Dec 4 [PubMed PMID: 23218699]
Level 1 (high-level) evidenceKorobelnik JF, Holz FG, Roider J, Ogura Y, Simader C, Schmidt-Erfurth U, Lorenz K, Honda M, Vitti R, Berliner AJ, Hiemeyer F, Stemper B, Zeitz O, Sandbrink R, GALILEO Study Group. Intravitreal Aflibercept Injection for Macular Edema Resulting from Central Retinal Vein Occlusion: One-Year Results of the Phase 3 GALILEO Study. Ophthalmology. 2014 Jan:121(1):202-208. doi: 10.1016/j.ophtha.2013.08.012. Epub 2013 Sep 29 [PubMed PMID: 24084497]
Level 1 (high-level) evidenceDugel PU, Koh A, Ogura Y, Jaffe GJ, Schmidt-Erfurth U, Brown DM, Gomes AV, Warburton J, Weichselberger A, Holz FG, HAWK and HARRIER Study Investigators. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology. 2020 Jan:127(1):72-84. doi: 10.1016/j.ophtha.2019.04.017. Epub 2019 Apr 12 [PubMed PMID: 30986442]
Level 1 (high-level) evidencePenha FM, Masud M, Khanani ZA, Thomas M, Fong RD, Smith K, Chand A, Khan M, Gahn G, Melo GB, Khanani AM. Review of real-world evidence of dual inhibition of VEGF-A and ANG-2 with faricimab in NAMD and DME. International journal of retina and vitreous. 2024 Jan 17:10(1):5. doi: 10.1186/s40942-024-00525-9. Epub 2024 Jan 17 [PubMed PMID: 38233896]
Taubenslag KJ, Kim SJ, Grzybowski A. Anti-inflammatory Pharmacotherapy for the Prevention of Cystoid Macular Edema After Cataract Surgery. American journal of ophthalmology. 2021 Dec:232():1-8. doi: 10.1016/j.ajo.2021.06.009. Epub 2021 Jun 19 [PubMed PMID: 34157275]
Friedman SM, Almukhtar TH, Baker CW, Glassman AR, Elman MJ, Bressler NM, Maker MP, Jampol LM, Melia M, Diabetic Retinopathy Clinical Research Network. Topical nepafenec in eyes with noncentral diabetic macular edema. Retina (Philadelphia, Pa.). 2015 May:35(5):944-56. doi: 10.1097/IAE.0000000000000403. Epub [PubMed PMID: 25602634]
Level 1 (high-level) evidence. Focal photocoagulation treatment of diabetic macular edema. Relationship of treatment effect to fluorescein angiographic and other retinal characteristics at baseline: ETDRS report no. 19. Early Treatment Diabetic Retinopathy Study Research Group. Archives of ophthalmology (Chicago, Ill. : 1960). 1995 Sep:113(9):1144-55 [PubMed PMID: 7661748]
Romero-Aroca P, Reyes-Torres J, Baget-Bernaldiz M, Blasco-Suñe C. Laser treatment for diabetic macular edema in the 21st century. Current diabetes reviews. 2014 Mar:10(2):100-12 [PubMed PMID: 24852439]
Writing Committee for the Diabetic Retinopathy Clinical Research Network, Fong DS, Strauber SF, Aiello LP, Beck RW, Callanan DG, Danis RP, Davis MD, Feman SS, Ferris F, Friedman SM, Garcia CA, Glassman AR, Han DP, Le D, Kollman C, Lauer AK, Recchia FM, Solomon SD. Comparison of the modified Early Treatment Diabetic Retinopathy Study and mild macular grid laser photocoagulation strategies for diabetic macular edema. Archives of ophthalmology (Chicago, Ill. : 1960). 2007 Apr:125(4):469-80 [PubMed PMID: 17420366]
Level 1 (high-level) evidenceDiabetic Retinopathy Clinical Research Network. A randomized trial comparing intravitreal triamcinolone acetonide and focal/grid photocoagulation for diabetic macular edema. Ophthalmology. 2008 Sep:115(9):1447-9, 1449.e1-10. doi: 10.1016/j.ophtha.2008.06.015. Epub 2008 Jul 26 [PubMed PMID: 18662829]
Level 1 (high-level) evidenceMiller SD. Argon laser photocoagulation for macular edema in branch vein occlusion. American journal of ophthalmology. 1985 Feb 15:99(2):218-9 [PubMed PMID: 4038586]
Level 3 (low-level) evidence. Evaluation of grid pattern photocoagulation for macular edema in central vein occlusion. The Central Vein Occlusion Study Group M report. Ophthalmology. 1995 Oct:102(10):1425-33 [PubMed PMID: 9097788]
Level 1 (high-level) evidencePearson PA, Comstock TL, Ip M, Callanan D, Morse LS, Ashton P, Levy B, Mann ES, Eliott D. Fluocinolone acetonide intravitreal implant for diabetic macular edema: a 3-year multicenter, randomized, controlled clinical trial. Ophthalmology. 2011 Aug:118(8):1580-7. doi: 10.1016/j.ophtha.2011.02.048. Epub [PubMed PMID: 21813090]
Level 1 (high-level) evidenceCampochiaro PA, Brown DM, Pearson A, Chen S, Boyer D, Ruiz-Moreno J, Garretson B, Gupta A, Hariprasad SM, Bailey C, Reichel E, Soubrane G, Kapik B, Billman K, Kane FE, Green K, FAME Study Group. Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema. Ophthalmology. 2012 Oct:119(10):2125-32. doi: 10.1016/j.ophtha.2012.04.030. Epub 2012 Jun 21 [PubMed PMID: 22727177]
Level 1 (high-level) evidenceScott IU, Ip MS, VanVeldhuisen PC, Oden NL, Blodi BA, Fisher M, Chan CK, Gonzalez VH, Singerman LJ, Tolentino M, SCORE Study Research Group. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular Edema secondary to branch retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 6. Archives of ophthalmology (Chicago, Ill. : 1960). 2009 Sep:127(9):1115-28. doi: 10.1001/archophthalmol.2009.233. Epub [PubMed PMID: 19752420]
Level 1 (high-level) evidenceTripathy K. Commentary: Posterior subtenon triamcinolone - The unsung hero for managing various ocular disorders. Indian journal of ophthalmology. 2023 Jan:71(1):181-182. doi: 10.4103/ijo.IJO_1963_22. Epub [PubMed PMID: 36588232]
Level 3 (low-level) evidenceLavezzo MM, Sakata VM, Morita C, Rodriguez EE, Abdallah SF, da Silva FT, Hirata CE, Yamamoto JH. Vogt-Koyanagi-Harada disease: review of a rare autoimmune disease targeting antigens of melanocytes. Orphanet journal of rare diseases. 2016 Mar 24:11():29. doi: 10.1186/s13023-016-0412-4. Epub 2016 Mar 24 [PubMed PMID: 27008848]
Boyer DS, Yoon YH, Belfort R Jr, Bandello F, Maturi RK, Augustin AJ, Li XY, Cui H, Hashad Y, Whitcup SM, Ozurdex MEAD Study Group. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014 Oct:121(10):1904-14. doi: 10.1016/j.ophtha.2014.04.024. Epub 2014 Jun 4 [PubMed PMID: 24907062]
Level 1 (high-level) evidenceGillies MC, Lim LL, Campain A, Quin GJ, Salem W, Li J, Goodwin S, Aroney C, McAllister IL, Fraser-Bell S. A randomized clinical trial of intravitreal bevacizumab versus intravitreal dexamethasone for diabetic macular edema: the BEVORDEX study. Ophthalmology. 2014 Dec:121(12):2473-81. doi: 10.1016/j.ophtha.2014.07.002. Epub 2014 Aug 22 [PubMed PMID: 25155371]
Level 1 (high-level) evidenceHaller JA, Bandello F, Belfort R Jr, Blumenkranz MS, Gillies M, Heier J, Loewenstein A, Yoon YH, Jacques ML, Jiao J, Li XY, Whitcup SM, OZURDEX GENEVA Study Group. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010 Jun:117(6):1134-1146.e3. doi: 10.1016/j.ophtha.2010.03.032. Epub 2010 Apr 24 [PubMed PMID: 20417567]
Level 1 (high-level) evidenceMaturi RK, Glassman AR, Liu D, Beck RW, Bhavsar AR, Bressler NM, Jampol LM, Melia M, Punjabi OS, Salehi-Had H, Sun JK, Diabetic Retinopathy Clinical Research Network. Effect of Adding Dexamethasone to Continued Ranibizumab Treatment in Patients With Persistent Diabetic Macular Edema: A DRCR Network Phase 2 Randomized Clinical Trial. JAMA ophthalmology. 2018 Jan 1:136(1):29-38. doi: 10.1001/jamaophthalmol.2017.4914. Epub [PubMed PMID: 29127949]
Level 1 (high-level) evidenceGupta A, Singh P, Tripathy K. Morning Glory Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 35593815]
Piccolino FC, De La Longrais RR, Manea M, Cicinelli S. Posterior cystoid retinal degeneration in central serous chorioretinopathy. Retina (Philadelphia, Pa.). 2008 Jul-Aug:28(7):1008-12. doi: 10.1097/IAE.0b013e31816b4b86. Epub [PubMed PMID: 18698305]
Level 2 (mid-level) evidenceKessel L, Hamann S, Wegener M, Tong J, Fraser CL. Microcystic macular oedema in optic neuropathy: case series and literature review. Clinical & experimental ophthalmology. 2018 Dec:46(9):1075-1086. doi: 10.1111/ceo.13327. Epub 2018 Jun 20 [PubMed PMID: 29799159]
Level 2 (mid-level) evidenceSipperley JO, Quigley HA, Gass DM. Traumatic retinopathy in primates. The explanation of commotio retinae. Archives of ophthalmology (Chicago, Ill. : 1960). 1978 Dec:96(12):2267-73 [PubMed PMID: 718521]
Level 3 (low-level) evidenceKedarisetti KC, Narayanan R, Stewart MW, Reddy Gurram N, Khanani AM. Macular Telangiectasia Type 2: A Comprehensive Review. Clinical ophthalmology (Auckland, N.Z.). 2022:16():3297-3309. doi: 10.2147/OPTH.S373538. Epub 2022 Oct 10 [PubMed PMID: 36237488]
Tripathy K, Shah SS, Waymack JR. Central Retinal Artery Occlusion. StatPearls. 2024 Jan:(): [PubMed PMID: 29262124]
Sun JK, Lin MM, Lammer J, Prager S, Sarangi R, Silva PS, Aiello LP. Disorganization of the retinal inner layers as a predictor of visual acuity in eyes with center-involved diabetic macular edema. JAMA ophthalmology. 2014 Nov:132(11):1309-16. doi: 10.1001/jamaophthalmol.2014.2350. Epub [PubMed PMID: 25058813]
Level 2 (mid-level) evidenceUji A, Murakami T, Nishijima K, Akagi T, Horii T, Arakawa N, Muraoka Y, Ellabban AA, Yoshimura N. Association between hyperreflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic macular edema. American journal of ophthalmology. 2012 Apr:153(4):710-7, 717.e1. doi: 10.1016/j.ajo.2011.08.041. Epub 2011 Dec 3 [PubMed PMID: 22137207]
Level 2 (mid-level) evidenceLiang MC, Vora RA, Duker JS, Reichel E. Solid-appearing retinal cysts in diabetic macular edema: a novel optical coherence tomography finding. Retinal cases & brief reports. 2013 Summer:7(3):255-8. doi: 10.1097/ICB.0b013e31828eef49. Epub [PubMed PMID: 25391118]
Level 3 (low-level) evidenceKashani AH, Lee SY, Moshfeghi A, Durbin MK, Puliafito CA. OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY OF RETINAL VENOUS OCCLUSION. Retina (Philadelphia, Pa.). 2015 Nov:35(11):2323-31. doi: 10.1097/IAE.0000000000000811. Epub [PubMed PMID: 26457395]
Forooghian F, Stetson PF, Meyer SA, Chew EY, Wong WT, Cukras C, Meyerle CB, Ferris FL 3rd. Relationship between photoreceptor outer segment length and visual acuity in diabetic macular edema. Retina (Philadelphia, Pa.). 2010 Jan:30(1):63-70. doi: 10.1097/IAE.0b013e3181bd2c5a. Epub [PubMed PMID: 19952996]
Ota M, Nishijima K, Sakamoto A, Murakami T, Takayama K, Horii T, Yoshimura N. Optical coherence tomographic evaluation of foveal hard exudates in patients with diabetic maculopathy accompanying macular detachment. Ophthalmology. 2010 Oct:117(10):1996-2002. doi: 10.1016/j.ophtha.2010.06.019. Epub 2010 Aug 17 [PubMed PMID: 20723993]
Level 2 (mid-level) evidenceRanchod TM, Fine SL. Primary treatment of diabetic macular edema. Clinical interventions in aging. 2009:4():101-7 [PubMed PMID: 19503772]
Patel D, Patel SN, Chaudhary V, Garg SJ. Complications of intravitreal injections: 2022. Current opinion in ophthalmology. 2022 May 1:33(3):137-146. doi: 10.1097/ICU.0000000000000850. Epub 2022 Mar 9 [PubMed PMID: 35266893]
Level 3 (low-level) evidenceFlaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, Ying GS. Diabetic Retinopathy Preferred Practice Pattern®. Ophthalmology. 2020 Jan:127(1):P66-P145. doi: 10.1016/j.ophtha.2019.09.025. Epub 2019 Sep 25 [PubMed PMID: 31757498]