Introduction
Pinna perichondritis is the inflammation of the perichondrial layer surrounding the auricular cartilage. This condition is often a more severe infection than, but frequently mistaken for, pinna cellulitis, which shares its risk factors. Penetrating ear trauma, such as transcartilaginous ear piercing, is the most common cause of this disease. Nonmedical personnel perform most ear piercings, with infection ensuing if sterile conditions are not maintained.
Abscesses arise from neglected infection, resulting in perichondrial detachment that devascularizes the underlying cartilage. The condition may lead to cartilage necrosis and pinna shape alteration. Inflammation may develop from blood collecting within the space between the perichondrium and cartilage and within the cartilaginous layer. Cauliflower ear deformity is a potential complication arising from inflammatory fibrocartilaginous proliferation (see Image. Severe Cauliflower Ear Deformity). Bacterial perichondritis can also progress to a severe soft tissue or systemic infection if left untreated.
Auricle Histology
The auricle, or external ear pinna, is composed of elastic cartilage encased in a dense perichondrium containing elastic fibers. Auricular skin hosts sparse hairs, sebaceous glands, and eccrine sweat glands. The auricle's skin has keratinized stratified squamous epithelium that tightly adheres to the perichondrium, except in the posterior aspect where fatty subcutaneous and skeletal muscle layers exist.
The perichondrium serves crucial functions. This fibrous covering provides structural support to the auricle's elastic cartilage, maintaining ear shape and integrity. The pinna's cartilage is avascular and thus depends on the highly vascularized perichondrium for oxygen and nutritional support. Chondroblasts within the inner perichondrium facilitate the repair and growth of cartilage tissue. This fibrous layer also acts as an attachment site for the overlying skin.[1][2] Perichondrial pathology, such as inflammation or infection, can lead to complications like auricular deformity or abscess formation, highlighting the importance of maintaining the integrity of this fibrous layer.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Pinna perichondritis has various triggers, but penetrating auricular cartilage trauma is the most commonly cited in the literature.[3][4] The increasing popularity of transcartilaginous ear piercings has been implicated as the cause of the rising perichondritis cases in the past decade. Transcartilaginous ear piercings carry a greater risk of infection and abscess formation than lobule piercings.[5] The infection risk increases after exposing the wound to freshwater or hot tubs immediately after the piercing.[6] Less common pinna perichondritis causes include untreated middle or external ear infections that spread to the pinna and cartilage, iatrogenic injury, immunosuppression, and other forms of minor trauma, such as ear scratching, insect bites, and acupuncture. A significant proportion of patients with this condition have no identifiable cause.
The most common organism isolated in pinna perichondritis cases is Pseudomonas aeruginosa, which has a predilection for infecting damaged cartilage. This bacterial species is responsible for up to 100% of piercing-related infections and is often associated with ear perichondrial abscess formation.[7] Other causative organisms include Staphylococcus aureus, Escherichia coli, and Proteus spp, with Staphylococcus being the most common organism when abscess does not form.[8] Fungal infection has been occasionally reported and may be linked to perioperative prophylactic antibiotic administration for otologic surgery.[9] Perichondritis may also arise from viral infections like herpes zoster and monkeypox that create skin vesicular lesions, which establish a bacterial entry route into the deep pinna structures.[10] Less common etiologies include retained ear wick after placement for otitis externa and recurrent infection of a congenital intraauricular sinus tract.
Epidemiology
Pinna perichondritis is uncommon. The condition's incidence is unknown, though it has been reported that the number of cases doubled between 1990 and 1998 in England. This increase seems to parallel the rising popularity of cartilaginous ear piercings among adolescents and young adults.[11] A 2015 systematic review revealed that women are more than 7 times as likely as men to develop complications from transcartilaginous ear piercing. This outcome is attributed to the relative frequency of ear piercings between sexes rather than a physiological difference. The mean age of patients developing complications from transcartilaginous ear piercing is 19 years.
Another study revealed that treatment delay of more than 5 days significantly increased the likelihood of hospitalization, as did Pseudomonas aeruginosa compared to Staphylococcus aureus infection. Pseudomonas accounted for 87% of the cases in the study. Perichondritis after scapha piercing was associated with long-term ear deformity in 100% of patients, contrasting with the 43% occurrence rate in patients with helical piercings (see Image. Auricle Surface Anatomy).
Pathophysiology
Trauma can cause cartilage microfractures, separating the perichondrium from the underlying cartilage. Cartilaginous tissue is subsequently devascularized, leading to necrosis and space formation for blood or pus accumulation.[11] The cartilage's scanty blood supply makes it especially susceptible to infection even with careful implementation of the aseptic technique during ear piercing.[12] Chondritic infection can spread to the perichondrium and overlying skin, resulting in perichondritis, cellulitis, and abscess formation.
If neglected, significant necrosis and hematoma can arise and produce cosmetic deformity. Blood collection in the cartilage fracture lines can cause an inflammatory reaction, inducing fibrocartilage deposition and the development of the auricular deformity colloquially called the "cauliflower ear."[13][14]
Histopathology
Van Wijk et al's 2008 cadaveric study revealed that ear-piercing techniques caused perichondrial tearing from the cartilage, leading to microfractures, blood and pus accumulation, and abscess formation. Greater injury occurred at the exit sites, similar to a gunshot wound, with no significant disparity between hypodermic needles and piercing guns observed. However, cadaveric models may not correlate with in vivo tissue injury patterns with 100% accuracy.[15]
History and Physical
History
Pinna perichondritis is a clinical diagnosis. Therefore, taking a focused history and performing a thorough physical examination are essential. Individuals with pinna perichondritis often present with significant pain, swelling, and erythema localized to the external ear, with purulent discharge in severe cases. Fever and cervical node swelling may occur if the infection spreads beyond the outer ear. A recent history of ear or lateral facial trauma may be elicited, eg, from piercing, acupuncture, abrasions, burns, lacerations, or insect bites. Clinicians should ask about relevant symptoms such as hearing loss, otorrhea, and cranial nerve abnormalities, which may indicate a different diagnosis, such as otitis externa, otitis media, or mastoiditis. Particular attention should be paid to comorbidities in the patient’s past medical history, such as diabetes and immunosuppression, which can increase the likelihood of infections.
Physical Examination
Physical examination should include a comprehensive ear exam with inspection, palpation, and otoscopy. Auricular perichondritis typically presents with an erythematous, swollen, hot, and tender pinna (see Image. Pinna Perichondritis). Examination may reveal soft tissue abscess or necrosis. Palpation typically demonstrates a tender pinna. The mastoid process and preauricular and postauricular regions should also be examined for tenderness. The lobule is classically spared in perichondritis and chondritis, differentiating these conditions from pinna cellulitis, which tends to involve the entire auricle.[16][17] Notably, perichondritis and cellulitis are caused by different microbiological agents. Any area affected by pinna cellulitis should be marked at presentation to monitor treatment response.
Systemic symptoms, such as pyrexia or an erythematous extension beyond the pinna, suggest that the infection has spread beyond the external ear. Careful otoscopy should be performed, with the unaffected ear examined first. The clinician should look for external ear canal debris, discharge, erythema, or swelling. These findings indicate otitis externa, primarily treated with external auditory canal debridement, topical antibiotics, and dry ear precautions. The tympanic membrane should also be assessed for an air-fluid level or perforation that can point to middle ear pathology. A cranial nerve assessment and cervical lymph node evaluation should be performed as indicated.
Relapsing polychondritis should be entertained if a patient presents with nasal, joint, tracheobronchial, and bilateral pinna inflammation. The syndrome is an autoimmune condition typically treated with oral steroids.[18]
Evaluation
Routine blood tests are not usually indicated in simple pinna perichondritis. However, substantial edema or erythema of the surrounding area, an abscess, or necrosis warrants laboratory testing, including complete blood count, basic metabolic panel (or complete, depending on clinical presentation), C-reactive protein, blood cultures, and coagulation profile. These tests should be included as part of a sepsis screen in an unstable patient. Culture swabs should be taken from the affected area and any discharge present or obtained from incision and drainage. Imaging is not indicated unless intracranial pathologies, such as malignant otitis externa, are suspected.
Treatment / Management
Antibiotic therapy is the treatment mainstay for pinna perichondritis. Management depends on the presence of an abscess and its severity. Outpatient oral fluoroquinolones often suffice for cases without abscesses. Levofloxacin is an example that has antistaphylococcal and antipseudomonal activity. The presence of an abscess requires both surgical drainage and fluoroquinolone treatment. Abscesses are approached similarly to an auricular hematoma, with incision, irrigation, a pressure dressing, and potentially drain placement.[19]
Patients with abscesses are more likely to have Pseudomonal infections and require hospitalization for intravenous antibiotic administration. Preferred options include third and fourth-generation cephalosporins, aminoglycosides, and fluoroquinolones. However, fluoroquinolones have been historically avoided in the pediatric population due to the risk of developing arthralgia and tendon rupture. However, a 2011 meta-analysis of fluoroquinolone use in children demonstrated a low incidence of musculoskeletal side effects, which all resolved on medication withdrawal. No studies showed associated growth disturbances, suggesting that a short fluoroquinolone course is safe for pediatric patients.[20] Pinna perichondritis is painful. Thus, adequate analgesia should also be provided.(A1)
Incision and drainage of auricular abscesses and seromas may be performed with minimal scarring and cosmetic impact. A curvilinear incision along the medial helical aspect of the anterior pinna is typically adequate for draining abscesses, which typically involve the scaphoid fossa. This approach allows effective pus drainage without creating conspicuous scars (see Image. Incision and Drainage of an Auricular Hematoma). An incision may also be made with similarly unobtrusive scarring at the conchal bowl's outer edge along the medial antihelical margin. Pressure should be applied once the fluid collection is cultured and drained to prevent reaccumulation, similar to auricular hematoma management.
The cartilage window technique has been employed for subperichondrial abscesses, but through-and-through mattress suturing appears to be more effective for preventing pus reaccumulation. The cartilage window technique involves making a skin incision as previously described and then removing a roughly 1 x 1 cm cartilage piece with its overlying perichondrium from the area of the fluid collection while preserving the underlying perichondrium. The skin can then be primarily closed or left to granulate by secondary intention with or without drain or packing placement.[21] Mattress suturing is substantially less involved and requires nothing more than running a through-and-through stitch back and forth across the affected area to keep the skin and perichondrium apposed to the underlying cartilage. An absorbable suture, such as a 4-0 plain gut on a small Keith needle, is typically used. Cotton dental rolls or clothing buttons may also be employed to pressure the ear, typically held in place by mattress sutures.[22][23](B2)
Cases unrelated to auricular trauma but arising from conditions like otitis externa, herpes zoster oticus, and relapsing polychondritis require treatment of the primary pathology.
Auricular deformity may develop in some patients despite appropriate perichondritis management. Reconstruction, if required, should be delayed 6 to 12 months after infection resolution to improve surgical exposure and optimize healing.[24] The reconstruction type employed depends on the deformity observed, but treatment is generally performed according to cauliflower ear management principles (see Image. Surgical Repair of Cauliflower Ear).[25]
Ideally, the native cartilage is unfurled and sutured into place. However, auricles that have lost normal contour may require grafting using contralateral conchal cartilage—with costal cartilage being an acceptable alternative—to restore normal height and projection. Severe deformities may warrant replacing most or all of the auricular cartilage with a costal cartilage framework. Postauricular flaps may be used if additional skin is required due to soft tissue contraction.[26][27]
Differential Diagnosis
Clinicians should be aware of the various pathologies that can cause a painful, inflamed pinna. The differential diagnosis should thus include the following:
- Auricular abscess
- Auricular cellulitis
- Auricular hematoma
- Dermatological conditions affecting the ear, eg, eczema, psoriasis, and contact reaction
- Erysipelas
- Hemangioma
- Herpes zoster oticus
- Leprosy
- Lymphoma
- Monkeypox
- Otitis externa
- Relapsing polychondritis
- Skin cancer
- Sunburn
A thorough clinical and diagnostic evaluation can differentiate these conditions from pinna perichondritis and help determine the appropriate management strategy.
Prognosis
The symptoms of pinna perichondritis should subside in 2 to 3 days with prompt diagnosis and antibiotic therapy, though pain and tenderness can persist for a month or longer. The condition may cause a cosmetic deformity, depending on the severity of the infection and cartilaginous damage. However, Sosin et al's 2015 systematic review reveals that the presence of an abscess at presentation does not significantly alter the outcomes.
Complications
Perichondritis may lead to cartilage necrosis, minor cosmetic deformity, or a cauliflower ear if left untreated. Scapha perichondritis increases ear deformity risk compared to helical involvement and is more likely when the infection is left untreated for more than 5 days. The infection may spread within the cartilage in some cases, although bacterial chondritis is managed similarly to perichondritis.[28] The infection can also spread beyond the pinna and cause systemic illness due to toxic shock syndrome or endocarditis, necessitating intravenous antibiotics and hospital admission.[29][30]
Deterrence and Patient Education
Patients should be aware of the increased risk of pinna infection with transcartilaginous ear piercing compared to traditional lobule piercing. Healthcare providers should thus discourage the practice of high ear piercing, particularly at walk-in kiosks that may not practice strict sterile techniques.[31] Patients must seek prompt care if pain, swelling, and redness develop on the pierced site, as delaying care may result in permanent auricular deformity. Individuals who delay medical consultation for pinna inflammation or infection should be counseled regarding this possibility.
Pearls and Other Issues
Pinna perichondritis is an infection of the auricular cartilage's perichondrial lining primarily caused by Pseudomonas aeruginosa and Staphylococcus aureus. Minor trauma, such as piercing through the cartilaginous pinna, is typically the inciting factor, though it may arise from other mechanisms. Patients present with auricular erythema, edema, and tenderness, sparing the lobule. A fluid collection may likewise be found under the skin.
The diagnosis of pinna perichondritis is clinical, though laboratory and imaging tests can aid management if infection becomes widespread. The treatment cornerstone is antibiotic administration, with fluoroquinolones being preferred to cover the condition's common bacterial etiologies effectively. The presence of an abscess warrants incision and drainage. Potential complications of pinna perichondritis include sepsis and altered cosmesis, as in cauliflower ear deformity. Patients must be educated about these risks before undergoing a transcartilaginous ear piercing.
Enhancing Healthcare Team Outcomes
Pinna perichondritis must be promptly recognized and treated with the appropriate antibiotic to optimize outcomes. Uncomplicated cases, especially those without abscesses, may be managed in a primary care setting with oral antibiotic therapy. Consultation with infectious disease specialists, microbiologists, or pharmacists is recommended for guidance on antibiotic therapy selection, particularly to determine sensitivities for prevalent local pathogens. On the other hand, pinna perichondritis complicated by an abscess or cartilage necrosis must be referred to an otolaryngologist for urgent surgical incision and drainage or debridement of the pinna. The nursing staff helps coordinate care, assists in surgical procedures, ensures good care delivery for hospitalized patients, and emphasizes important points during patient counseling. This collaborative approach enhances treatment efficacy, minimizes the risk of antibiotic resistance, and improves outcomes for patients with pinna perichondritis.
Media
(Click Image to Enlarge)

Pinna Perichondritis. Classic cartilaginous pinna erythema and sparing of lobule in pinna perichondritis.
Contributed from Bress, E, Cohn, J.E. Perichondritis: inspect the lobule. Int J Emerg Med 13, 51 (2020). CC 4.0 license.
(Click Image to Enlarge)

Severe Cauliflower Ear Deformity. This patient has fibrocartilaginous overgrowth on the right pinna, partly obstructing the conchal bowl. The cartilage cannot support a normal auricular structure.
Contributed by Basit Jawad, M.D. and Ryan Winters, M.D.
(Click Image to Enlarge)
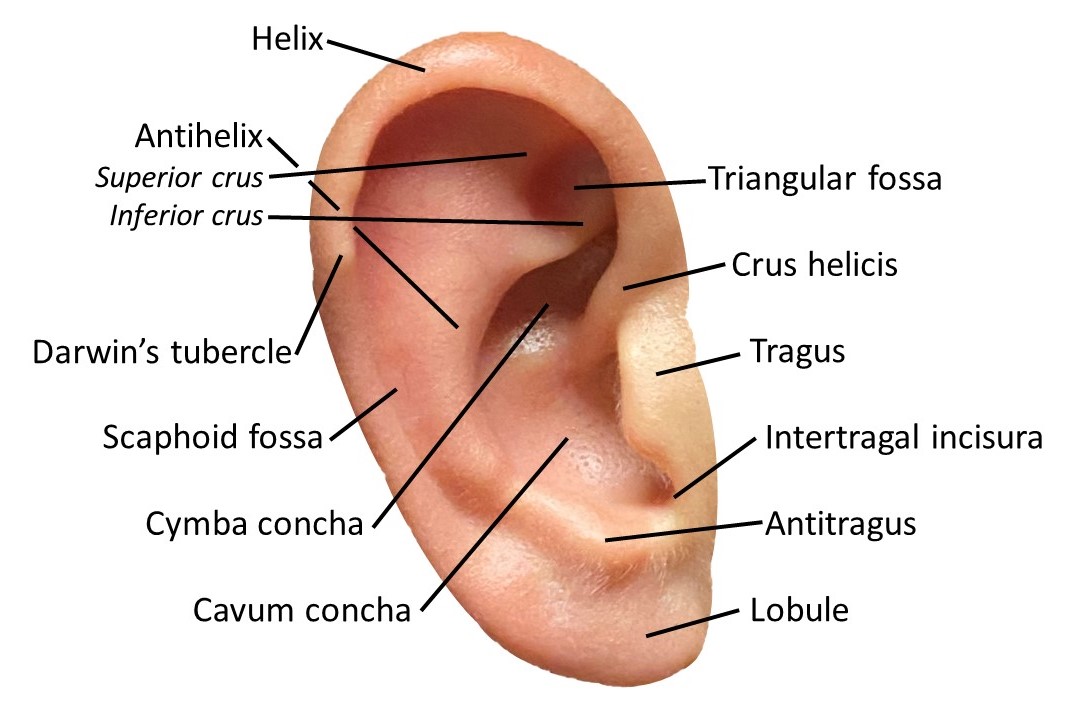
Auricle Surface Anatomy. This image shows the ear auricle's parts, parts, including the helix and its crus, the antihelix and its superior and inferior crura, the Darwin tubercle, triangular and scaphoid fossae, the tragus, conchal cymba and cavum, the intertragal incisura, antitragus, and lobule.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Surgical Repair of Cauliflower Ear. A) Preoperative view. Note the anterior malposition of the helical rim and the excess bulk within the scaphoid fossa. B) The auricular skin is elevated off the underlying cartilage anteriorly and posteriorly via an incision at the junction of the helix and scapha. The perichondrium is scarred and does not elevate easily. C) The skin flaps are replaced, and a quilting suture is passed after reshaping the cartilage with a scalpel, a curette, and a drill. D) Postoperative view at 1 month.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Incision and Drainage of an Auricular Hematoma. Left: An incision is made along the junction of the helix and the scaphoid fossa. Note the fracture on the helical cartilage. Right: The incision is closed, and the anterior auricular skin flap is reopposed to the cartilage using a 4-0 plain gut quilting suture to eliminate dead space and prevent hematoma recurrence. This technique is an alternative to traditional bolster placement and is better tolerated.
Contribued by Marc H Hohman, MD, FACS
References
Sand M, Sand D, Brors D, Altmeyer P, Mann B, Bechara FG. Cutaneous lesions of the external ear. Head & face medicine. 2008 Feb 8:4():2. doi: 10.1186/1746-160X-4-2. Epub 2008 Feb 8 [PubMed PMID: 18261212]
Zucchelli E, Birchall M, Bulstrode NW, Ferretti P. Modeling Normal and Pathological Ear Cartilage in vitro Using Somatic Stem Cells in Three-Dimensional Culture. Frontiers in cell and developmental biology. 2020:8():666. doi: 10.3389/fcell.2020.00666. Epub 2020 Jul 28 [PubMed PMID: 32850801]
Prasad HK, Sreedharan S, Prasad HS, Meyyappan MH, Harsha KS. Perichondritis of the auricle and its management. The Journal of laryngology and otology. 2007 Jun:121(6):530-4 [PubMed PMID: 17319983]
Level 2 (mid-level) evidenceSosin M, Weissler JM, Pulcrano M, Rodriguez ED. Transcartilaginous ear piercing and infectious complications: a systematic review and critical analysis of outcomes. The Laryngoscope. 2015 Aug:125(8):1827-34. doi: 10.1002/lary.25238. Epub 2015 Mar 30 [PubMed PMID: 25825232]
Level 1 (high-level) evidenceLiu ZW, Chokkalingam P. Piercing associated perichondritis of the pinna: are we treating it correctly? The Journal of laryngology and otology. 2013 May:127(5):505-8. doi: 10.1017/S0022215113000248. Epub 2013 Feb 26 [PubMed PMID: 23442437]
Level 3 (low-level) evidenceRowshan HH, Keith K, Baur D, Skidmore P. Pseudomonas aeruginosa infection of the auricular cartilage caused by "high ear piercing": a case report and review of the literature. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2008 Mar:66(3):543-6. doi: 10.1016/j.joms.2006.10.045. Epub [PubMed PMID: 18280391]
Level 3 (low-level) evidenceKlug TE, Holm N, Greve T, Ovesen T. Perichondritis of the auricle: bacterial findings and clinical evaluation of different antibiotic regimens. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2019 Aug:276(8):2199-2203. doi: 10.1007/s00405-019-05463-z. Epub 2019 May 11 [PubMed PMID: 31079204]
Davidi E, Paz A, Duchman H, Luntz M, Potasman I. Perichondritis of the auricle: analysis of 114 cases. The Israel Medical Association journal : IMAJ. 2011 Jan:13(1):21-4 [PubMed PMID: 21446231]
Level 2 (mid-level) evidenceZhang X, Zhang Y, Pu C, Wang L, Ni Y, Huang T. Etiology, Microbiological Isolates, and Antibiotic Susceptibilities in Inpatients with Refractory Auricular Perichondritis: A 10-Year Retrospective Study. Infection and drug resistance. 2024:17():377-386. doi: 10.2147/IDR.S434522. Epub 2024 Jan 31 [PubMed PMID: 38312521]
Level 2 (mid-level) evidenceAntúnez-Estudillo E, Riera Tur L, Caballero García A. Perichondritis and auricular cellulitis related to piercings as first manifestation of monkeypox. Acta otorrinolaringologica espanola. 2024 Mar-Apr:75(2):129-132. doi: 10.1016/j.otoeng.2024.01.001. Epub 2024 Jan 12 [PubMed PMID: 38220050]
Hanif J, Frosh A, Marnane C, Ghufoor K, Rivron R, Sandhu G. Lesson of the week: "High" ear piercing and the rising incidence of perichondritis of the pinna. BMJ (Clinical research ed.). 2001 Apr 14:322(7291):906-7 [PubMed PMID: 11302908]
Level 3 (low-level) evidenceWu J, Collins NP, Wilson SF. Perils of pinna piercing and pseudomonas perichondritis. Australian family physician. 2003 Jul:32(7):516-7 [PubMed PMID: 12901204]
Level 3 (low-level) evidenceOhlsén L, Skoog T, Sohn SA. The pathogenesis of cauliflower ear. An experimental study in rabbits. Scandinavian journal of plastic and reconstructive surgery. 1975:9(1):34-9 [PubMed PMID: 1162288]
Level 3 (low-level) evidencePandya NJ. Experimental production of "cauliflower ear" in rabbits. Plastic and reconstructive surgery. 1973 Nov:52(5):534-7 [PubMed PMID: 4745576]
van Wijk MP, Kummer JA, Kon M. Ear piercing techniques and their effect on cartilage, a histologic study. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2008:61 Suppl 1():S104-9 [PubMed PMID: 17684004]
Staley R, Fitzgibbon JJ, Anderson C. Auricular infections caused by high ear piercing in adolescents. Pediatrics. 1997 Apr:99(4):610-1 [PubMed PMID: 9093311]
Level 3 (low-level) evidenceBress E, Cohn JE. Perichondritis: inspect the lobule. International journal of emergency medicine. 2020 Oct 28:13(1):51. doi: 10.1186/s12245-020-00310-z. Epub 2020 Oct 28 [PubMed PMID: 33115411]
Hirayama K, Iwanaga N, Izumi Y, Yoshimura S, Kurohama K, Yamashita M, Takahata T, Oku R, Ito M, Kawakami A, Migita K. A Case of Relapsing Polychondritis Initiating with Unexplained Fever. Case reports in medicine. 2016:2016():9462489. doi: 10.1155/2016/9462489. Epub 2016 Feb 14 [PubMed PMID: 26981127]
Level 3 (low-level) evidenceKrogmann RJ, Jamal Z, King KC. Auricular Hematoma. StatPearls. 2023 Jan:(): [PubMed PMID: 30285394]
Adefurin A, Sammons H, Jacqz-Aigrain E, Choonara I. Ciprofloxacin safety in paediatrics: a systematic review. Archives of disease in childhood. 2011 Sep:96(9):874-80. doi: 10.1136/adc.2010.208843. Epub 2011 Jul 23 [PubMed PMID: 21785119]
Level 1 (high-level) evidenceBhandary S, Mannil TV. A comparative study in the management of auricular pseudocysts. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2000 Jul:52(3):246-50. doi: 10.1007/BF03006193. Epub [PubMed PMID: 23119685]
Level 2 (mid-level) evidenceBhat VS, Shilpa, Nitha, Ks R. Deroofing of auricular pseudocyst: our experience. Journal of clinical and diagnostic research : JCDR. 2014 Oct:8(10):KC05-7. doi: 10.7860/JCDR/2014/9609.4978. Epub 2014 Oct 20 [PubMed PMID: 25478375]
Greywoode JD, Pribitkin EA, Krein H. Management of auricular hematoma and the cauliflower ear. Facial plastic surgery : FPS. 2010 Dec:26(6):451-5. doi: 10.1055/s-0030-1267719. Epub 2010 Nov 17 [PubMed PMID: 21086231]
Perry AW, Sosin M. Reconstruction of ear deformity from post-piercing perichondritis. Archives of plastic surgery. 2014 Sep:41(5):609-12. doi: 10.5999/aps.2014.41.5.609. Epub 2014 Sep 15 [PubMed PMID: 25276662]
Patel BC, Hohman MH, Hutchison J, Hatcher JD. Cauliflower Ear. StatPearls. 2025 Jan:(): [PubMed PMID: 29261905]
Yotsuyanagi T, Yamashita K, Urushidate S, Yokoi K, Sawada Y, Miyazaki S. Surgical correction of cauliflower ear. British journal of plastic surgery. 2002 Jul:55(5):380-6 [PubMed PMID: 12372365]
Putri IL, Bogari M, Khoirunnisa A, Dhafin FR, Kuswanto D. Surgery of Severe Cauliflower Ear Deformity. Plastic and reconstructive surgery. Global open. 2023 Apr:11(4):e4953. doi: 10.1097/GOX.0000000000004953. Epub 2023 Apr 19 [PubMed PMID: 37091928]
Bellaud G, Canestri A, Gallah S, Merlant M, Cousseau S, Lebrette MG, Slama L, Pialoux G. Bacterial chondritis complications following ear piercing. Medecine et maladies infectieuses. 2017 Feb:47(1):26-31. doi: 10.1016/j.medmal.2016.07.002. Epub 2016 Sep 3 [PubMed PMID: 27596713]
McCarthy VP, Peoples WM. Toxic shock syndrome after ear piercing. The Pediatric infectious disease journal. 1988 Oct:7(10):741-2 [PubMed PMID: 3186344]
Nah SY, Chung MH, Park JE, Durey A, Kim M, Lee JS. Infective endocarditis caused by methicillin-resistant Staphylococcus aureus in a young woman after ear piercing: a case report. Journal of medical case reports. 2011 Aug 1:5():336. doi: 10.1186/1752-1947-5-336. Epub 2011 Aug 1 [PubMed PMID: 21806817]
Level 3 (low-level) evidenceTobar DFC, Kosoko AA. Auricular Perichondritis after a "High Ear Piercing:" A Case Report. Journal of education & teaching in emergency medicine. 2021 Apr:6(2):V30-V33. doi: 10.21980/J8WH16. Epub 2021 Apr 19 [PubMed PMID: 37465706]
Level 3 (low-level) evidence