 Sonography Female Pelvic Pathology Assessment, Protocols, and Interpretation
Sonography Female Pelvic Pathology Assessment, Protocols, and Interpretation
Introduction
Sonography of the pelvis is the first resort and primary evaluation technique for any suspected pelvic pathology after clinical examination. Portable ultrasound machines (PUM) and office ultrasound machines have revolutionized gynecology and obstetrics practice.[1]
No radiation exposure, real-time imaging, the dynamic vascular study of the organs, three dimensional and four-dimensional sonography has given an edge to sonography imaging over various other imaging and diagnostic techniques. Various commonly practiced pelvic sonography techniques are transabdominal, transvaginal, transperineal, and endosonography. Extension of routine pelvic sonography like sonohysterosalpingography, Doppler ultrasound, and three-dimensional and four-dimensional ultrasound have widened the scope of pelvic sonography for various indications over other imaging modalities.
The ultrasound features and signs are based on parameters like the amount of transmission, absorption, the reflection of sound waves, and the angle of reflection. Every tissue has its sound reflection characteristics depending on the size, depth, shape, content, and margins of the organ. The amount of transmission, absorption, and reflection of sound waves is based on these tissue characteristics, which determine normal and abnormal ultrasound image patterns. When there is a complete reflection of sound waves from a structure, it appears hyperechoic (white-bright).
When a structure allows partial penetration of sound waves and partial reflection, the structures take various shades of grey scales in ultrasound images. When there is a complete transmission of sound waves through water, it appears anechoic (black-dark). Hence in transabdominal ultrasound, a full bladder scanning is performed, which allows complete penetration of sound waves to its posterior pelvic structures and displaces the bowel laterally, allowing complete evaluation of pelvic organs. With this understanding, we review the radiological features of the pelvic structures.[2]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Uterus: The uterus is a muscular pear-shaped organ occupying the pelvis with homogeneous isoechoic to hyperechoic texture. Uterine musculature has three layers. The middle myometrial layer forms the major uterine part and is homogeneous in echotexture. The innermost compact, thin and hypoechoic myometrium forms the sub-endometrial halo and is described as a junctional zone. The outermost myometrial layer is thinner and may have dot-like calcifications of arcuate arteries on sonography when the uterus is senile. The uterus helps to give orientation to understand pelvic anatomy with any sonography technique.
Endometrium: Endometrium has a dynamic echo pattern corresponding to the patient's menstrual cycle and hormonal status. The postmenstrual endometrium is thin and linear. Pre ovulatory endometrium has a trilaminar pattern and is 4 to 8 mm thick. Postovulatory endometrium is homogeneous and more echogenic with a 7 to 14 mm thickness.
Cervix: Cervix is a cylindrical structure in continuity with the uterus with a homogeneous echo pattern. Internal os serves as a landmark delineating cervix and the endocervical canal from the uterine body and endometrial cavity, respectively.
Fallopian tube: Fallopian tube is a tubular structure usually not visualized normally in sonography except in case of any pathology enhancing its dimensions.
Ovary: Ovary is an oval structure with hyperechoic stroma and variable anechoic cystic follicles fluctuating in line with the menstrual cycle and varying in size between 5 to 25 mm in diameter. The ovaries are positioned laterally to the uterus and medial to internal iliac vessels.[3]
Vagina: Vagina is a muscular collapsed tubular structure visualized caudally to the cervix appreciated in transabdominal sonography.
Ureters: Ureters are difficult to visualize and are seen in the transverse section near the uterine cervix laterally.
Urinary bladder: Urinary bladder is the anterior-most and an essential landmark in pelvic sonography. In transabdominal scanning, a distended bladder allows better visualization of pelvic structure, as discussed earlier. However, in transvaginal sonography, the empty bladder allows better visualization of the uterus.
Bowel: Bowels are visualized as tubular structures with variable echo patterns and visible peristalsis and are often confused with cystic structures.
Cul-de-sac: Cul-de-sac is a well-defined invaginated fold of the peritoneum posterior to the uterus, normally having minimal free fluid collection following ovulation. Fluid collection in abnormal quantities with internal moving echoes and solid or cystic lesions in cul-de-sacs are of diagnostic significance.
Indications
Pelvic sonography is a screening tool and an important diagnostic modality for various gynecological and obstetric pathologies. Patients with abnormal uterine bleeding (AUB), postmenopausal bleeding, abdominal distension, palpable pelvic mass, abdominal pain, pelvic pain, infertility, recurrent pregnancy loss, and signs of infection should be evaluated by pelvic sonography.[4][5]
Abnormal Uterine Bleeding
Heavy menstrual bleeding is one of the common presentations of structural uterine pathologies like leiomyoma, adenomyosis, and endometrial polyp detected by pelvic sonography. Patients with endometrial hyperplasia and carcinoma present with heavy menstrual and postmenopausal bleeding and require ultrasound screening. Intermenstrual bleeding is frequently associated with an endocervical polyp, carcinoma cervix, estrogen-secreting ovarian tumors, and intrauterine devices.
The most common presentation of endometrial carcinoma and hyperplasia in postmenopausal females is postmenopausal bleeding. Screening such females with pelvic sonography followed by endometrial sampling is highly recommended. Senile vaginitis, urethritis, and endocervical polyp are frequent causes of postmenopausal bleeding.[6]
Abdominal Mass and Pelvic Mass
Ascites and ovarian malignancy frequently present primarily with complaints of increased abdominal girth, abdominal distension, and/or palpable pelvic mass. Large subserosal broad ligament leiomyoma, multiple uterine leiomyomas, adenomyosis with more than 12-week pregnant uterine size, molar pregnancy, rudimentary horn ectopic pregnancy, hematometra, pyometra, choriocarcinoma, ovarian and tubo ovarian mass present as pelvic mass frequently extending up to abdominal cavity. All these mentioned pelvic pathologies can be screened by pelvic sonography.
Pelvic Pain and Dysmenorrhea
Endometriosis, pelvic inflammatory disease, ovarian torsion, tubo ovarian mass, adenomyosis, degenerating leiomyoma, ectopic pregnancy, and cystitis are common pathologies presenting with lower abdominal and pelvic pain having an ultrasound diagnosis.
Infertility, Amenorrhea, and Recurrent Pregnancy Loss
Structural uterine anomalies in the case of the unicornuate uterus, bicornuate uterus, septate uterus, didelphys uterus, and cervical incompetence are associated with causing infertility and recurrent pregnancy loss.[7] In patients with amenorrhea in case of androgen insensitivity syndrome (AIS) and Mayer-Rokitansky-Kuster-Kuster-Hauser (MRKH) syndrome due to absent uterus; due to hypoplastic uterus in case of Turner syndrome; and in case of imperforate hymen with hematometra, ultrasound diagnosis is required. These patients also have infertility. Asherman syndrome is an acquired pathology of amenorrhea and infertility, which can be diagnosed by sonography.
Contraindications
There are very few contraindications for pelvic sonography. Transabdominal sonography (TAS) can be deferred or avoided in case of discomfort due to a full bladder. Transvaginal sonography (TVS) should be avoided in patients with an imperforated and intact hymen, no history of vaginal intercourse, vaginismus, significant vaginal atrophy, vaginal obstruction, secondary vaginal stenosis, recent vaginal surgery, and in cases when the patient denies consent. Sonohysterosalpingography should be avoided in active and heavy menstrual bleeding in case of suspected infection and pregnancy.[8]
Equipment
An ultrasound machine with appropriate transducers is as follows:
- 3.5-7 MHz for transabdominal scans
- 5-12 MHz for transvaginal scans and
- 7-15 MHz for transperineal scans
Probe cover or condom cover for endovaginal probes and ultrasound gel.[8]
Personnel
Physicians or any sonographer trained in diagnostic obstetric ultrasonography may perform pelvic sonography. Obstetricians, gynecologists, and radiologists are the physicians who usually perform pelvic sonography. Nurse practitioners, ultrasound technicians, and other healthcare providers trained as sonographers perform sonography in primary healthcare settings or as routine in many countries where only interpretation is performed by physicians.
Preparation
Transabdominal Sonography
In a transabdominal scan, patients are comfortably positioned in a supine position and examined with a full bladder.
Transvaginal Sonography
In transvaginal sonography, the empty bladder allows better visualization of the uterus. The examination should be relatively painless. The patient is supine in the lithotomy position. Pillow under the buttocks or feet rested in stirrups of the bed allows better positioning and visualization of pelvic organs.[7]
In the women of reproductive age group, knowledge of the last menstrual period and serum beta-hCG levels may be useful. It is good practice to perform TAS with a full bladder in every patient to avoid missing any abdominopelvic mass or adnexal mass, followed by emptying the bladder and performing TVS which allows a more detailed evaluation of pelvic structures.[9]
Technique or Treatment
Uterine imaging measures the length, depth, and width of the uterus. Length is measured from the fundus to the external cervical os in the mid-sagittal plane. Depth: anteroposterior diameter is measured in the same plane, perpendicular to the line of uterine length. Uterine width is measured in the coronal plane of the uterus. Cervix is measured in the midsagittal plane and transverse plane.
Cervical length is measured from internal to external os. Myometrium is assessed for any deviation from normal echotexture and any mass lesion. Various parasagittal and transverse images through the uterus are documented. In the case of multiple leiomyomas, the largest two are measured in three planes.[10][11]
Endometrial thickness is measured perpendicular to the long axis of the uterus in a midsagittal plane, including both the anterior and posterior endometrial lining, excluding the hypoechoic sub-endometrial zone. In the case of fluid collection, it should be excluded from measurement. Any endometrial thickening, mass, or cystic changes should be measured and documented. Color Doppler and pulsed ultrasound may be more informative. IUD, if present, should be mentioned and assessed for its appropriateness of location.
A coronal view of the uterine fundus is taken to evaluate the adnexa, and the probe is angulated laterally towards the broad ligament. Iliac vessels could be identified in the longitudinal plane, and adnexa can be imaged medially to them. Ovaries are measured in 3 orthogonal planes. Follicles are counted, measured, and documented.
Any cystic, solid, or abnormality in the vasculature is documented. The adnexal mass should be assessed for its origin. If on the movement of the transvaginal probe or abdominal wall, if the mass moves with the ovary, it is of ovarian origin. If it doesn't move with the ovary, it is para ovarian, tubular or uterine in origin. This differentiation is important in the day-to-day diagnosis of tubular ectopic pregnancy and hydrosalpinx. Dynamic imaging by giving pressure to the abdominal wall also helps to displace the bowel. Doppler helps to differentiate malignant from benign masses and adnexal cysts from parametrial vessels.
Evaluation of the vaginal cuff and bladder wall before a hysterectomy is a good practice. Cul-de-sac is assessed for any fluid or mass.
Sonohysterosalpingography
Ultrasound is a very useful screening tool to identify endometrial cavity lesions and the causes of infertility. Sonohysterosalpingography (Saline Infusion Sonohysterography-SIS) is a sonography technique to determine the patency of fallopian tubes and is a more comfortable procedure than conventional hysterosalpingography.
Sonohysterosalpingography is a completely radiation-free technique in which saline is infused inside the uterine cavity through the cervix using a self-retaining intracervical insertion of foley's catheter. Saline is infused, and the free flow of saline through the fallopian tube and its exit in the peritoneal cavity is visualized by sonography which confirms the patency of the fallopian tube. (See Figure 1: SIS showing patent fallopian tube) It helps differentiate any endometrium occupying lesions like thickened endometrium, endometrial polyp, and submucosal fibroid.[7][12] (See Figure 2: Saline infusion sonohysterogram, confirming the presence of an intra-cavitary fibroid)
Complications
Discomfort due to the full bladder in TAS, pelvic pain in TVS, and pelvic infection following sonohysterosalpingography are commonly seen as unpleasant adverse events in pelvic sonography. ALARA principle needs to be followed for an ultrasound to avoid unevidenced minor complications occurring due to sonography.
Clinical Significance
Abnormal Uterine Bleeding
AUB has a prevalence rate of 10 to 52 %, with high referrals to health care centers.[13] Every patient with abnormal uterine bleeding requires sonography evaluation. Pelvic sonography helps to determine the organ of origin and characteristics of the pathology and decide the possible next step in managing AUB. The most common causes of AUB are there within the uterus.
In the case of premenopausal females, endometrial hyperplasia, leiomyoma, adenomyosis, endometrial polyps, endocervical polyps, cervical carcinoma, endometrial carcinoma, some pregnancy-related complications like gestational trophoblastic diseases, and retained products of conception are common causes of AUB. TVS is the primary line of investigation for AUB, in which if the uterine cavity is found normal, further evaluation is usually not required, and medical treatment is commenced.[14]
Power Doppler along with grey scale TVS has high specificity and negative predictive value for evaluation of AUB comparable to hysteroscopy.[15]
- Endometrial polyp: Endometrial polyps form the commonest cause of AUB and infertility, with a prevalence rate of around 24% and a malignancy potential of up to 6%.[13] In the presence of focal small smooth marginated echogenic lesion with a single vascular stalk (pedunculated) or broad-based (sessile), arising from the endometrium and regular endometrial-myometrial junction; one can suspect endometrial polyp.
- Leiomyoma: Another important cause of AUB is uterine leiomyoma. It appears as an iso or hypoechoic structure which is well defined, well marginated, rounded and shows minimal vascularity in the doppler study. They can be intramural, submucosal, or subserosal. Submucosal leiomyomas are usually the most symptomatic and frequent cause of AUB of all. Sometimes, it is challenging to differentiate submucosal leiomyomas from endometrial polyps. Sonohysterosalpingography allows better differentiation between these two uterine lesions. When more than half of the size of submucosal leiomyoma projects into the endometrial cavity, it can be removed hysteroscopically. Some leiomyomas may show degenerative changes in the form of necrotic, cystic, or calcified areas or red degenerative changes. (Figure 2: TVS showing the presence of an intra-cavitary fibroid)
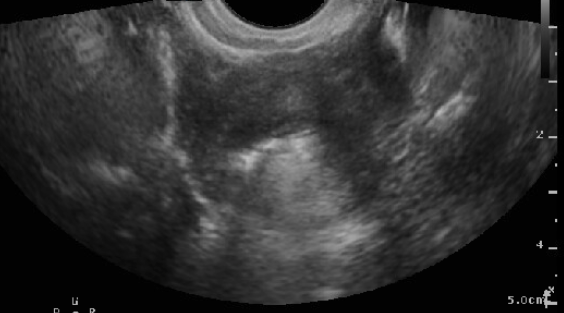
- Adenomyosis: Adenomyosis is a common benign cause of AUB, dysmenorrhea, dyspareunia, and infertility in premenopausal women, but one-third may be asymptomatic. It occurs due to heterotopic endometrial glands and stroma proliferating within the myometrium. Heavy uterine bleeding is the most common symptom and is due to the increased total volume of endometrial glands in the uterine myometrium and endometrium.[16] In women younger than 40 years, the prevalence of adenomyosis in infertile females is 22%, and in infertile women over 40 years, it is 24.4%, in cases of recurrent pregnancy loss, it is 38.2%, and in previous ART failure, it is 34.7%.[17] Sonography features of adenomyosis show asymmetrically enlarged uterus, loss of endomyometrial differentiation - irregular or interrupted junctional zone (JZ), heterogeneous architecture, intramyometrial cystic areas, hyperechoic islands, fan-shaped shadowing in the myometrium, echogenic sub endometrial lines, buds in the myometrium and translesional vascularity.[18] TVS has a sensitivity and specificity of 83.8% and 63.9%, respectively, and three-dimensional TVS has pooled sensitivity and specificity of 88.9% and 56.0%, respectively, for diagnosing adenomyosis.[19][20] (Figure 3: Adenomyosis Uterus)
- Endometritis: It is one of the common causes of polymenorrhea. Thickened endometrium with internal fluid or gas suggests endometritis. It may be associated with other pelvic inflammatory signs like parametrial inflammation, fluid collection in the pouch of Douglas, and/or pyosalpinx.
Malignant and premalignant conditions like endometrial cancer, cervical cancer, and endometrial hyperplasia present with postmenopausal bleeding, heavy menstrual bleeding, and intermenstrual bleeding. Power Doppler has sensitivity and specificity of 81.81% and 100% for endometrial polyp, 72.72% and 98.9% for endometrial hyperplasia, and 75% and 100% for endometrial carcinoma.[21]
- Endometrial hyperplasia: It is diagnosed by measuring combined endometrial thickness. There may be focal or diffuse endometrial thickening with or without internal cystic spaces. Combined endometrial thickness of more than 8 mm in the proliferative phase and more than 16 mm in the secretory phase in premenopausal females require histopathological evaluation of the endometrium. In postmenopausal females with postmenopausal bleeding, the endometrial thickness of more than 5 mm, and without postmenopausal bleeding, the endometrial thickness of 8-11 mm requires endometrial sampling and histopathological evaluation.[22] In an observational study on 2216 women with AUB, endometrial evaluation as per (International Endometrial Tumor Analysis) IETA terminology showed that endometrial thickness < 3 mm, three-layer pattern, linear midline, and single vessel without branching make endometrial cancer unlikely.[23]
- Endometrial cancer: Postmenopausal bleeding is a presenting feature in 90% of cases of endometrial cancer.[24] Radiological features of endometrial cancer are thickened, irregular-shaped, heterogeneous endometrial lesions with collection in the endometrial cavity. It has internal vascularity of multifocal origin in the endometrial cavity and is with or without myometrial invasion. Invasion of the myometrium makes the diagnosis certain in most cases.
- Endometrial atrophy: Endometrial atrophy is the most common cause of postmenopausal uterine bleeding.[24] In postmenopausal females with atrophic vaginitis, there is usually a thin endometrium of less than 4 mm.
- Cervical cancer: Cervical causes like cervical polyp, endocervical fibroid, cervical intraepithelial neoplasia, and carcinoma cervix present with AUB. As seen on sonography, benign lesions like endocervical fibroid and polyp are echogenic, well-defined, and well-marginated mass lesions. Cervical cancer appears as irregular-shaped mass lesions arising from the cervix, occupying the cervical canal and vagina, and has increased vascularity.
- Retained products of conception (RPOC): In a woman of reproductive age group with abnormal uterine bleeding and a history of amenorrhea, sonography screening of retained products of conception is required in line with a positive pregnancy test. Retained products of conception appear as heterogeneous lesions with mixed echogenicity in the endometrial canal with an endometrial thickness of more than 15 mm with or without internal vascularity.[25] However, RPOC more than 30 mm and increased vascularity involving more than half the thickness of myometrium has an increased tendency to bleed.[26] Clinical history of amenorrhea and ill-defined echogenicity differentiates retained products of conception from well-defined endometrial fibroid and polyp.
- Gestational trophoblastic disease (GTD): Women with GTD present with a history of amenorrhea followed by abnormal uterine bleeding, disproportionate uterine enlargement for gestational age, and raised beta HCG levels. Sonography and clinical examination show an enlarged uterus filled with multiple cystic structures without the presence of fetal or placental parts, a snowstorm appearance in the hydatidiform mole, and the presence of fetal or placental parts in the partial mole. (Figure 4: Sonography of Complete Molar Pregnancy-Snow storm appearance) Choriocarcinoma: Choriocarcinoma is a less common gestational trophoblastic disease that presents with irregular vaginal bleeding after a history of vaginal delivery remotely and with suboptimally raised beta HCG levels. In sonography, the uterus is enlarged with heterogeneous infiltrative mass invading myometrium and beyond and has increased internal vascularity and vascular malformations, like arteriovenous shunts and pseudoaneurysms. There may be the presence of bilateral theca lutein cysts.[27]
- Intrauterine device (IUD): In females of the reproductive age group, Cu IUCD is a common cause of AUB, and it appears as a highly echogenic linear structure in the endometrial cavity on sonography. Sonography is used in the detection of displaced IUDs. (Figure 5: Sonography Intrauterine device displaced in the cervix))
Other rare causes of AUB are estrogen-secreting ovarian tumors like granulosa cell tumors and thecoma, which causes endometrial thickening and abnormal uterine bleeding.
Abdominal Mass and Pelvic Mass
Pelvic pathologies may present with abdominal mass or pelvic mass. The patients with abdominal mass may present with abdominal pain, ascites, or palpable mass, which on bimanual pelvic examination and sonography may be revealed of pelvic origin. Pelvic masses are not palpable, and patients with pelvic masses usually present with abdominal pain, dysmenorrhea, or menstrual complaints.
Adnexal masses are commonly encountered as abdominal and pelvic mass lesions and are of diagnostic dilemma. Large cysts, endometriosis, and ovarian torsion are a few painful lesions. There is a structured diagnostic approach based on the appearance and organ of origin of the adnexal mass lesion. Adnexal mass can be anechoic cystic, complex cystic, or solid, and it can be ovarian or extra ovarian. Sonography is the gold standard for ovarian cyst diagnosis.
The organ of origin is determined by the positive beak sign (acute angles with the organ of origin), embedded organ sign, phantom organ sign, and prominent feeding artery sign from the vascular channels of the organ of origin. Although specific pathologic diagnosis of adnexal neoplasms can not be made by sonography, it is a great tool to differentiate between benign and malignant lesions and narrow down the provisional differential diagnosis. There should be an integration between clinical findings, radiology, and laboratory parameters.
Findings that increase the likelihood of malignancy are thick wall, thick irregular septa, vascularity in wall and septa, solid component, vascularity within the solid element, ascites, metastatic omental deposits, omental thickening, old age patients, postmenopausal females, and elevated CA-125 levels.
The primary goal of assessing adnexal mass is to differentiate benign and malignant lesions and to determine the surgical line of management. Nearly 2% of the adnexal tumors are malignant or borderline tumors.[28] 'IOTA Simple rules' is a classification of sonography features for ovarian tumors into three features - benign, malignant, and borderline. The classification system consists of five features of benign ovarian tumors called B-features and five features of malignant ovarian tumors called M-features.
Unilocular cysts, presence of solid components <7 mm, presence of acoustic shadow, smooth multilocular tumor with the tumor measuring <10 cm, and color score 1 - no blood flow on color Doppler are B-features and irregular solid tumor, presence of ascites, at least four papillary structures, irregular multilocular solid tumor with the largest diameter ≥10 cm, color score 4 - very strong blood flow are M-features. Based on the presence of B or M features, the tumor is classified as benign or malignant. Tumour having both features is classified as a borderline tumor.[29][30]
Anechoic Cystic Adnexal Mass
Thin-walled anechoic cysts are benign, while solid elements increase the risk of malignancy. Size is an important clue towards diagnosis; a cyst < 3 cm in premenopausal women is likely physiologic, while a cyst > 6 cm at any age is likely neoplastic. If the lesion is anechoic cystic and does not arise from the ovary, para ovarian cyst, para tubal cyst, hydrosalpinx, or fluid-filled bowel loop could be the likely diagnosis. In case of physiological cysts, follow-up after six weeks is advisable to check the resolution. Below are the anechoic adnexal cysts commonly encountered-
- Physiological and functional cysts of the ovary: One should be aware of the rule of 1-2-3. According to this, in the 1st week of the menstrual cycle, a 1 cm cyst is a follicle; while a 2 cm cyst in the 2nd week of the menstrual cycle is generally a dominant follicle; a 3 cm cyst in the 3rd week of the menstrual cycle is considered as corpus luteum. Any anechoic cyst that appears as a thin-walled anechoic unilocular intraovarian cyst measuring less than 6 cm in size resolves over time. Therefore a 6-week follow-up scan is advisable. These anechoic cysts more than 3 cm in size are known as functional cysts. Oral contraceptive pills resolve physiological cysts and prevent new cyst formation. Any anechoic round structure in the body is considered cysts, and similarly are these physiological cysts of the ovary. However, while reporting these physiological findings, it is advisable to report these ovaries as 'normal ovaries' to avoid any misinterpretation for it to be considered a pathological finding.[31]
- Paraovarian and paratubal cysts: These are separate from ovaries, generally thin-walled anechoic cysts which do not change in size over time. They arise from mesonephric, paramesonephric, or mesothelioma remnants.[32]
- Inclusion cyst of ovary: They occur due to invagination of ovarian cortical surface epithelium, which loses connection with the ovarian surface. They are typical of small size, approximately 1 to 13 mm, but rarely may go up to 10 cm. They have thin, smooth walls, and the location is typically within 1 to 2 mm from the outer surface of the ovary.
- Serous cystadenoma: Serous cystadenoma is a benign epithelial ovarian tumor with a thin-walled, unilocular, anechoic cyst. Occasionally, it may have thin septations. Rarely can it present as a large complex multilocular cyst.[33]
- Hydrosalpinx: Hydrosalpinx appears as an elongated tubular anechoic lesion with an incomplete septa sign. There is a history of prior pelvic inflammatory disease or endometriosis. [34]
- Peritoneal inclusion cysts: These are seen surrounding ovarian tissue, giving a spider web pattern. They are irregular in shape, with poorly defined walls formed by adjacent organs. They are believed to be arising from the fluid collection within a pool formed by postoperative adhesions. Therefore the history of prior surgery is there in almost all cases. Sometimes, it may present as a septated complex cystic lesion. Size may be variable from small localized collection to the large cystic mass occupying pelvis and lower abdomen.[35][36]
Complex Cystic Adnexal Mass
They have internal contents, including moving echoes, debris, solidified or partially liquified areas, or septations. History is of utmost importance to provide a provisional diagnosis and to take an idea about the next possible step in management. While scanning, if the pain and probe tenderness is present and a complex cystic lesion is visualized, one should consider hemorrhagic cyst, adnexal torsion, tubo ovarian abscess, or oophoritis.
- Hemorrhagic cyst of the ovary: It occurs due to hemorrhage into the corpus luteum or some other functional cysts. It has a variety of appearances depending on the age of the hemorrhage. In the acute phase of hemorrhage, internal contents appear as echogenic lace-like strands with internal moving echoes. In the subacute phase, septations are present, which represent fibrin strands giving cog web signs, and there is clot formation. Later on, clot retraction occurs, which appears as a non-vascular, solid, echogenic area within the cyst. Acute angles with the ovary suggest the ovarian origin of the lesion. The wall of the lesion is thick and irregular and may have a prominent color flow in the wall of the cyst. They are usually managed conservatively.[37]
- Dermoid cyst (mature teratoma): It is a germ cell tumor of the ovary, a very commonly seen lesion with a variety of appearances depending on tissue and contents. Fatty content within it with internal debris gives an echogenic appearance. Bright linear echoes may represent hair content. Fat-fluid or fluid-fluid levels are seen. Internal echogenic nodules with posterior acoustic shadowing may represent dense elements likely to be calcification or tooth-like element. It mostly occurs in the reproductive age group and can occur bilaterally. Rarely, they may present as an anechoic cyst with wall calcification and small echogenic nodule within the cyst and with distal acoustic shadow.[38]
- Endometrioma (chocolate cyst): It is due to localized endometriosis of the ovary. They are varied in appearance, but the most common appearance is a unilocular cyst with acoustic enhancement posterior to the cyst and diffuse homogenous ground glass appearance resulting from hemorrhagic debris. While less typical features are: punctate echogenic wall foci due to calcification or cholesterol crystals. They are usually bilateral, adherent, and occupy the pouch of Douglas. Multiple locules and septations may be present in a few cases. Other sites of endometriotic deposits are cul-de-sac, uterosacral ligaments, uterus, and colon.[39][40]
- Mucinous cystadenoma: It is an epithelial ovarian tumor, typically a thin-walled multilocular large cyst with thin septations. Components of cysts have low-level internal echogenicity due to mucinous contents.[41][42]
- Cystadenocarcinoma: It is a malignant epithelial tumor characterized by thick irregular walls, thick irregular septations, papillary wall projections, and solid elements with increased vascularity. The pulse wave doppler shows low resistance flow due to neovascularization which are immature vessels (Resistive index tends to be low in malignancy, less than 0.4). They may be bilateral and associated with signs of metastatic disease, ascites, omental thickening, and serosal metastases on the liver and/or spleen may be present.
- Endometrioid carcinoma of the ovary: These are malignant epithelial tumors with non-specific varied imaging findings. A large complex cystic mass with solid components is seen. Endometrial thickening may be present. 30% of tumors are bilateral, and 15 to 20% are associated with endometriosis.[42]
- Clear cell carcinoma: They are malignant epithelial cell tumors. Sonographically, this ovarian lesion is characterized by unilocular cystic smooth marginated mass with solid nodular protrusions and vascularity on color doppler. However, as radiological features are non-specific, histopathological diagnosis is necessary.[42][43]
- Granulosa cell tumor (sex cord-stromal tumor of the ovary): It has a varying appearance, including cystic to multiloculated solid cystic or solid structure. It is less likely to have a papillary projection, which is more common in epithelial ovarian tumors. Due to estrogen secretion, there will be endometrial hyperplasia or polyp associated with postmenopausal bleeding. The perimenopausal and postmenopausal age group is more commonly involved. Rarely may it show signs of precocious puberty when it occurs in childhood, but it is rare.[44]
- Pyosalpinx: Pyosalpinx radiologically appears as an elongated dilated serpentine tubular cystic structure adjacent to the uterus with low-level internal echoes due to the higher protein content of internal debris. This echogenic appearance differentiates it from hydrosalpinx, which has clear anechoic fluid. It can be isolated or a component of tubo-ovarian abscess and pelvic inflammatory disease.[45]
- Tubo-ovarian abscess: Tubo-ovarian mass is a complex hypoechoic multilocular adnexal or retro uterine mass with irregular thick walls, debris-internal echoes, and septations. Free fluid with echoes is noted in the surrounding region and cul-de-sac. It may be associated with signs of infection like vaginal discharge, cervical motion tenderness, pain, fever, and elevated white blood cell count.[46][45]
Solid Adnexal Mass
- Leiomyoma: Adnexal leiomyoma may be subserosal, exophytic, pedunculated, or broad ligament fibroid. Ovaries are seen separate from the mass. It appears as a well-defined, well marginated, solid isoechoic mass with echogenicity similar to the middle layer of the myometrium. Sometimes degenerative cystic or necrotic areas are seen if the lesion is larger. In pedunculated exophytic lesions, blood flow is seen connecting to the uterus. MRI helps differentiate leiomyoma and primary ovarian stromal tumors, which have a similar sonographic appearance.
- Adnexal torsion: It can occur as primary ovarian torsion of the normal ovary, in which the responsible causes are long Fallopian tubes or absent mesosalpinx, mainly seen in young females. Secondary ovarian torsion is due to the large ovarian or para ovarian mass lesions, which act as the lead point for the twisting of the fallopian tube and ovarian pedicle. A unilateral lesion with severe ipsilateral pain is the most common presentation. Enlarged ovary ( > 4 cm ), ovarian edema, variable echogenicity hypo or hyperechoic, and peripherally displaced follicles with central edematous stroma are the common radiological features of ovarian torsion. The ovary is in midline position with the uterus pulled to the affected side. The Whirlpool sign indicates the twisting of the pedicle. Free fluid is seen in the pelvis. The wall of the ovarian lesion is edematous. Doppler findings are variable. Blood flow is not always absent. Little or no ovarian venous flow has high sensitivity toward the diagnosis of torsion. Arterial flow may be present, but the absence of arterial flow is a poor prognostic sign. In the case of intermittent torsion, there may be normal vascularity. In most cases, the torsion is unilateral. Bilateral torsion is very rare.[47][48]
- Ovarian metastasis: These are mixed echogenic tumors, predominantly solid and with few cystic areas with internal vascularity. It may be unilateral or bilateral. Most common tumors that metastasize to ovaries are from the colon, stomach, breast, lung, or contralateral ovary. Krukenberg tumors are generally bilateral metastatic ovarian tumors that contain mucin-secreting signet ring cells, usually of gastrointestinal origin, that form 30-40% of all ovarian metastases. Other rare primaries include metastasis from the pancreas, gallbladder, endometrial carcinoma, melanoma, renal cell carcinoma, hepatocellular carcinoma, leukemia, transitional cell carcinoma of the bladder, and neuroblastoma.
- Primary ovarian malignancy: It shows heterogeneous mixed echogenic solid cystic areas with vascularity in solid components. It may show other signs of malignancy such as ascites, omental thickening, and serosal metastases on the liver &/or spleen. It is challenging to determine pathological diagnosis from ultrasound, as narrated previously.
- Brenner tumor of the ovary: Brenner tumor is a benign surface epithelial tumor of the ovary most of the time. They are solid hypoechoic masses or sometimes multi or unilocular cystic areas with anechoic or low-level echoes within. Calcifications are common. They are commonly seen in postmenopausal females. Ascites and fluid in the pouch of Douglas are rare. But large mass, papillary projections, marked vascularity, and signs of metastasis may favor malignant lesions found in the 5th and 7th decades of a female's life.[49]
- Fibrothecoma: They appear as homogeneous hypoechoic solid mass (a fibrous tissue character) with posterior acoustic shadowing. They may show a heterogeneous appearance due to cystic degeneration and have a very close differential diagnosis to broad ligament fibroid, especially when bilateral ovaries are atrophic and not visualized. They may be associated with endometrial thickening if it secretes estrogen and may present with abnormal uterine bleeding. It is typically seen in women aged 40 to 60 years. The patient may have associated hirsutism and amenorrhea if it secretes androgen.[50][51]
- Sertoli Leydig cell tumor: These are sex cord-stromal tumors and are well-defined hyperechoic solid masses with few intratumoral cysts. Mild vascularity is noted on color doppler mode. They are hormonally active tumors and secrete androgen. The patients are usually less than 30 years old and present with virilization.[52]
- Endometrioid carcinoma: They are typically mixed cystic and solid adnexal mass but may also appear solid. 30% are bilateral. They may show endometrial hyperplasia due to hormonal stimulation and may present as abnormal uterine bleeding. They are associated with endometriosis in 15-20% of cases.
- Ovarian lymphoma: They are homogeneous, solid bilateral masses. Ascites is usually absent. Most cases of ovarian involvement are seen in patients with systemic disease. Primary ovarian lymphoma is rare. It may occur as secondary ovarian lymphoma, which is almost always non-Hodgkins type, and occurs late as a manifestation of advanced systemic lymphoma.[53]
- Pelvic kidney: Kidneys malpositioned in the pelvis appear as reniform in shape with the collecting system and with ipsilateral empty renal fossa. Urinary tract abnormalities are usually associated with Mullerian abnormalities.[54][55]
Pelvic Pain and Dysmenorrhoea
Dysmenorrhea is the most common cause of pelvic pain in females. Secondary dysmenorrhea may occur due to endometriosis, pelvic inflammatory disease, adenomyosis, adnexal torsion, or leiomyoma. Other causes of pelvic pain are interstitial cystitis and ectopic pregnancy.[56]
- Endometriosis: Transvaginal pelvic ultrasonography is highly accurate and sensitive for detecting typical ovarian endometriomas. Assessment of the Ultrasound-Based Endometriosis Staging System score (UBESS) in predicting surgical difficulty showed a better prediction of the surgical plan for endometrioma and vaginal and digestive tract involvement compared to the anterior compartment and uterosacral ligaments.[57] UBESS evaluates uterus and adnexa, ovarian mobility, the status of the cul-de-sac, non-bowel, and bowel deep infiltrating endometriosis, and anterior, lateral, and posterior pelvic compartments. Ground glass appearance of the ovary, ovarian immobility, site-specific tenderness, loss of sliding sign in the cul-de-sac, presence of solid hypoechoic nodules, hypoechoic linear thickening, hypoechoic irregular shaped plaques in non-ovarian non-bowel sites, non-compressible hypoechoic lesion on muscularis propria of the bowel- all these sonography signs suggests endometriosis.[58]
- Ectopic pregnancy: It presents as pelvic pain, vaginal bleeding, and shock in the first trimester of pregnancy. In the case of tubal pregnancy, on pelvic sonography, there is an echogenic ring-like mass separate from the ovary within the fallopian tube. Probe tenderness is present. Transvaginal ultrasound has better sensitivity. Viable ectopic pregnancy may show a yolk sac or embryo with embryonic cardiac pulsations. Hemoperitoneum appears as a mixed echogenic collection in the abdominal cavity, and ruptured ectopic mass in the cul-de-sac appears as a heterogeneous mass cul-de-sac. Ultrasound-guided aspiration of the blood from the abdominal cavity confirms the diagnosis of hemoperitoneum.[59]
- Appendicitis: It is suspected in the case of right iliac fossa pain and tenderness. It appears as a blind-ended tubular non-compressible, non-peristaltic structure adjacent to iliac vessels with thick walls and a diameter of more than 7 mm. It may show appendicolith and fluid surrounding it. Sometimes the appendicular mucocele may extend to the pelvis and be confused with the adnexal lesion when it is very large. Organ tracing and organ of origin signs with step-by-step ruling out technique should be used in case of any diagnostic dilemma.
- Oophoritis: Oophoritis may appear as a bulky inflamed vascular ovary without any pedicle twisting. Probe tenderness is present with surrounding free fluid in the pelvis and pouch of Douglas.[45]
Infertility and Amenorrhoea
- Polycystic ovarian syndrome: Polycystic ovarian syndrome (PCOS) patients commonly present with amenorrhea, infertility, hirsutism, acne, and obesity. 30% of patients seeking infertility treatment have PCOS. [60] Polycystic ovaries have a stroma more hyperechoic than uterine myometrium and an ovarian volume of more than 10 ccs with twelve or more peripherally placed ovarian follicles of 2 to 9 mm. Diagnosis of PCOS is made based on revised Rotterdam criteria, 2003.[61][62][63]
- Congenital abnormalities: Normal karyotype: The congenital structural abnormalities of the female reproductive tract with normal karyotype involve genital anomalies with failure of canalization of the Mullerian tubercle like imperforate hymen and transverse vaginal septum. On sonography, hematocolpos and hematometra may be noted. These patients present with cyclical abdominal pain at menarcheal age and primary amenorrhea.[64][65] MRKH syndrome, also known as Mullerian agenesis, has a normal karyotype and shows an absent uterus and cervix with small fibromuscular condensation near the gonadal site. Bilateral ovaries are present at the adnexal site.[66] Unicornuate uterus with rudimentary horn is a frequent cause of infertility and ectopic pregnancy. Abnormal karyotype: Androgen insensitivity syndrome patients have primary amenorrhea, an absent uterus, and a shallow vagina. Ovaries are absent in such patients and have testicles on the extragonadal side. The karyotype of these patients is 46, XY. Hypoplastic uterus in patients with Turner syndrome has a uterine length of less than 5 cm and intercornual distance of less than 2 cm and presents with infertility.[67][68] All patients with congenital abnormalities of reproductive organs should be screened for congenital urinary tract abnormalities.
- Asherman syndrome: In Asherman syndrome, the uterine cavity has multiple synechiae with damaged endometrium and compromised vascularity. This leads to amenorrhea, failed implantation, and infertility. On ultrasound, an interrupted endometrium line is noted in the sagittal plane with punctate echogenic foci within the endometrium. Echogenic fibrotic septae with or without calcification are seen on ultrasound. Asherman syndrome is better appreciated in 3D transvaginal sonography, which gives a 3D representation of the uterine cavity, which is noted as irregular with intermittent narrowing.[69][70]
Recurrent Pregnancy Loss
- Müllerian duct fusion abnormalities: Patients with Müllerian duct fusion abnormality have a normal karyotype. Septate uterus and bicornuate uterus lead to recurrent pregnancy loss and cause imaging dilemmas. It occurs due to failed resorption of the fibrous septum.[71] In the bicornuate uterus, two cornuas are more divergent with more than 105 degrees intercornual angle in contrast to the septate uterus, where the intercornual angle is less than 75 degrees. In the septate uterus, the fundus is convex or flat, and the fundal cleft is shallow with less than 1 cm depth. In the bicornuate uterus, the fundal cleft is more than 1 cm deep. The Septate uterus has a partial or complete muscular septum within the uterine cavity, and implantation at this avascular septum leads to a failed pregnancy. Uterine didelphys show two divergent uterine horns with two separate endometrial cavities and two cervices (bicollis) or one cervix (unicollis) with a large fundal cleft. It occurs due to the non-fusion of the two Mullerian ducts.[55][72]
- Cervical incompetence: Cervical incompetence, as determined by the history of recurrent second-trimester abortions and preterm birth, may have sonography suggesting decreased cervical length, funneling, and easy cervical deformation under pressure in cervical elastography.[73]
Transperineal ultrasound is helpful in the evaluation of urinary incontinence by assessment of pelvic floor muscles and their postoperative mesh complications after surgical repair.[74] Evaluation of parametrial spread of malignancy and rectovaginal endometriosis is done by transrectal ultrasound[75] and is beyond the scope of the article to discuss in detail.
Enhancing Healthcare Team Outcomes
An appropriate reporting pattern with a clear representation of sonography findings without vague terms and a clear description of pathology avoids unnecessary secondary and alternative imaging of pathology and enhances the healthcare outcomes of the sonography reporting team. Clear communication between the reporting team and treating clinician helps in the most accurate diagnosis, treatment, and follow-up plan for the patient.
We discuss here and recommend reporting patterns by eminent sonography bodies in obstetrics and gynecology. Uterine pathologies like leiomyoma and adenomyosis are the most common benign pelvic pathologies. With the trending lifestyle and improved health care facilities, there is a special place for conservative management of such lesions in the case of young and infertile patients.
With precise sonographic evaluation and reporting of these lesions, mode of surgery, type of surgery - conservative or radical and fertility treatments, proper selection of cases for minimally invasive techniques like uterine artery embolization, laparoscopic morcellation, and fibroid ablation is possible. Hence, a meticulous reporting pattern has been suggested by the morphological uterine sonographic assessment (MUSA) group. The terms and definitions formed and recommended in reporting are aimed to have homogeneity for clinical research, to predict the risk of various uterine pathologies, and to determine the precise line of treatment in various clinical scenarios.
As per its recommendation, the uterine myometrium is reported to mention the dimensions of uterine corpus and cervix, serosal contour - lobulated or regular, myometrial walls- symmetrical or asymmetrical, and echogenicity- homogeneous or heterogeneous. The junctional zone is described as regular, irregular, or interrupted, and presence of cystic areas, hyperechogenic dots, hyperechogenic buds, and lines. The myometrium should be assessed for echogenicity - homogeneous or heterogeneous. Any pathological lesion may be detailed for its echotexture, ill-defined, or well-defined site and size.
FIGO classification for myoma localization is the preferred way to report the position of the myoma to the uterus. It could be 0: pedunculated and intracavitary; 1: submucosal and < 50% intramural; 2: submucosal and ≥ 50% intramural; 3: 100% intramural, but in contact with the endometrium; 4: intramural; 5: subserosal and ≥ 50% intramural; 6: subserosal and < 50% intramural; 7: subserosal and pedunculated; 8: other (e.g.parasitic, cervical).[6] [Level 1]
The presence of myometrial cysts with acoustic shadowing and internal shadowing, hyperechogenic islands, and echogenic spots should be mentioned. Vascularity of the uterus should be assessed with Doppler and reported with associated pathology.[18] [Level 1]
A few of the minor reporting glitches with ambiguous and vague description patterns in reporting pelvic sonography should be abandoned. Follicles are anechoic structures in the ovary varying in size throughout the menstrual cycle. Reporting normal follicles less than 25 mm as cysts may be misunderstood as an abnormal finding of cystic mass, or highlighting it as multiple may confuse it with polycystic ovaries. Similarly, the corpus luteum, referred to as a cyst, is misunderstood as an abnormal finding. In all these cases, which are normal cyclical menstrual changes in the ovary, reporting it as cysts should be deferred, and terms like 'normal ovary with dominant follicle' or 'normal ovary with multiple small follicles' or 'normal ovary with corpus luteum' should be preferred.[76] [Level 1]
Since most benign ovarian lesions have distinct, defined sonographic features which funnel down the diagnostic dilemma, a more specific sonographic description should be given beyond the sonographic term like 'ovarian neoplasm' or 'complex ovarian or adnexal mass.' As complex mass hints at a solid component present in mass, the terminology 'complex adnexal mass' may create a diagnostic dilemma for the treating physician and dilute the differentiation between benign and malignant lesions. Hence, more detailed evaluation and reporting in terms of solid component, multilocularity, echotexture, vascularity, presence of papillary projections, regularity of mass, and ascites should be reported to give a clear picture to the treating physician, which helps in triaging the patient properly and avoids unnecessary alternative imaging.
It is advisable to provide animated or schematic diagrams of possible pathological diagnoses rather than just sonography images. This helps the treating clinician with the spatial orientation of the pathology. The sonographer should provide the orientation of adjacent vital structures like vessels and ureters when the anatomical relation of the structures deviates from normal, which will help surgeons to avoid inadvertent injury to these structures. With the recent advent of volumetric ultrasound imaging, volume contrast imaging (VCI) modes, 3D printers, and tomographic ultrasound imaging (TUI)- a post-processing modality that enables localization of multiple fibroids and determining the tumor spread. A picture is worth a thousand words.
Media
(Click Image to Enlarge)
Sonohysterosalpingogram showing patent fallopian tube (hyper-echoic bubbles seen flowing through the cornua and outside of the uterine cavity) Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)

A: TVUS image of sagittal uterus with well circumscribed, suspected uterine fibroid within the endometrium. B. Saline infusion sonohysterogram, confirming the presence of an intra-cavitary fibroid Contributed by Jenna Kahn, MD
(Click Image to Enlarge)

Adenomyosis Uterus Contributed by Zalak Karena, MS
(Click Image to Enlarge)

Sonography of Complete Molar Pregnancy-Snow storm appearance Contributed by Zalak Karena, MS
(Click Image to Enlarge)

Sonography: Displaced Intrauterine device (IUD) Contributed by Zalak Karena, MS
References
Recker F, Weber E, Strizek B, Gembruch U, Westerway SC, Dietrich CF. Point-of-care ultrasound in obstetrics and gynecology. Archives of gynecology and obstetrics. 2021 Apr:303(4):871-876. doi: 10.1007/s00404-021-05972-5. Epub 2021 Feb 8 [PubMed PMID: 33558990]
Jensen JA. Medical ultrasound imaging. Progress in biophysics and molecular biology. 2007 Jan-Apr:93(1-3):153-65 [PubMed PMID: 17092547]
Schwimer SR, Lebovic J. Transvaginal pelvic ultrasonography: accuracy in follicle and cyst size determination. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 1985 Feb:4(2):61-3 [PubMed PMID: 3882987]
Moorthy RS. TRANSVAGINAL SONOGRAPHY. Medical journal, Armed Forces India. 2000 Jul:56(3):181-183. doi: 10.1016/S0377-1237(17)30160-0. Epub 2017 Jun 10 [PubMed PMID: 28790701]
Timmerman D, Valentin L. Imaging in gynecological disease. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2007 May:29(5):483-4 [PubMed PMID: 17444563]
Level 2 (mid-level) evidenceMunro MG, Critchley HO, Broder MS, Fraser IS, FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2011 Apr:113(1):3-13. doi: 10.1016/j.ijgo.2010.11.011. Epub 2011 Feb 22 [PubMed PMID: 21345435]
Kondagari L, Kahn J, Singh M. Sonography Gynecology Infertility Assessment, Protocols, and Interpretation. StatPearls. 2025 Jan:(): [PubMed PMID: 34283459]
Nahlawi S, Gari N. Sonography Transvaginal Assessment, Protocols, and Interpretation. StatPearls. 2023 Jan:(): [PubMed PMID: 34283450]
Hill LM, Breckle R. Value of a postvoid scan during adnexal sonography. American journal of obstetrics and gynecology. 1985 May 1:152(1):23-5 [PubMed PMID: 3887924]
Level 3 (low-level) evidenceDodson MG, Deter RL. Definition of anatomical planes for use in transvaginal sonography. Journal of clinical ultrasound : JCU. 1990 May:18(4):239-42 [PubMed PMID: 2160990]
Rottem S, Thaler I, Goldstein SR, Timor-Tritsch IE, Brandes JM. Transvaginal sonographic technique: targeted organ scanning without resorting to "planes". Journal of clinical ultrasound : JCU. 1990 May:18(4):243-7 [PubMed PMID: 2160991]
Sabry ASA, Fadl SA, Szmigielski W, Alobaidely A, Ahmed SSH, Sherif H, R H Yousef R, Mahfouz A. Diagnostic value of three-dimensional saline infusion sonohysterography in the evaluation of the uterus and uterine cavity lesions. Polish journal of radiology. 2018:83():e482-e490. doi: 10.5114/pjr.2018.80132. Epub 2018 Nov 30 [PubMed PMID: 30655928]
Kaveh M, Sadegi K, Salarzaei M, Parooei F. Comparison of diagnostic accuracy of saline infusion sonohysterography, transvaginal sonography, and hysteroscopy in evaluating the endometrial polyps in women with abnormal uterine bleeding: a systematic review and meta-analysis. Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques. 2020 Sep:15(3):403-415. doi: 10.5114/wiitm.2020.93791. Epub 2020 Mar 19 [PubMed PMID: 32904526]
Level 1 (high-level) evidenceGoyal BK, Gaur I, Sharma S, Saha A, Das NK. Transvaginal sonography versus hysteroscopy in evaluation of abnormal uterine bleeding. Medical journal, Armed Forces India. 2015 Apr:71(2):120-5. doi: 10.1016/j.mjafi.2014.12.001. Epub 2015 Feb 16 [PubMed PMID: 25859072]
Veena P, Baskaran D, Maurya DK, Kubera NS, Dorairaj J. Addition of power Doppler to grey scale transvaginal ultrasonography for improving the prediction of endometrial pathology in perimenopausal women with abnormal uterine bleeding. The Indian journal of medical research. 2018 Sep:148(3):302-308. doi: 10.4103/ijmr.IJMR_96_17. Epub [PubMed PMID: 30425220]
Cunningham RK, Horrow MM, Smith RJ, Springer J. Adenomyosis: A Sonographic Diagnosis. Radiographics : a review publication of the Radiological Society of North America, Inc. 2018 Sep-Oct:38(5):1576-1589. doi: 10.1148/rg.2018180080. Epub [PubMed PMID: 30207945]
Puente JM, Fabris A, Patel J, Patel A, Cerrillo M, Requena A, Garcia-Velasco JA. Adenomyosis in infertile women: prevalence and the role of 3D ultrasound as a marker of severity of the disease. Reproductive biology and endocrinology : RB&E. 2016 Sep 20:14(1):60. doi: 10.1186/s12958-016-0185-6. Epub 2016 Sep 20 [PubMed PMID: 27645154]
Van den Bosch T, Dueholm M, Leone FP, Valentin L, Rasmussen CK, Votino A, Van Schoubroeck D, Landolfo C, Installé AJ, Guerriero S, Exacoustos C, Gordts S, Benacerraf B, D'Hooghe T, De Moor B, Brölmann H, Goldstein S, Epstein E, Bourne T, Timmerman D. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2015 Sep:46(3):284-98. doi: 10.1002/uog.14806. Epub 2015 Aug 10 [PubMed PMID: 25652685]
Level 3 (low-level) evidenceVannuccini S, Petraglia F. Recent advances in understanding and managing adenomyosis. F1000Research. 2019:8():. pii: F1000 Faculty Rev-283. doi: 10.12688/f1000research.17242.1. Epub 2019 Mar 13 [PubMed PMID: 30918629]
Level 3 (low-level) evidenceAndres MP, Borrelli GM, Ribeiro J, Baracat EC, Abrão MS, Kho RM. Transvaginal Ultrasound for the Diagnosis of Adenomyosis: Systematic Review and Meta-Analysis. Journal of minimally invasive gynecology. 2018 Feb:25(2):257-264. doi: 10.1016/j.jmig.2017.08.653. Epub 2017 Aug 30 [PubMed PMID: 28864044]
Level 1 (high-level) evidenceBatra S, Khanna A, Shukla RC. Power Doppler sonography - A supplement to hysteroscopy in abnormal uterine bleeding: Redefining diagnostic strategies. Indian journal of cancer. 2022 Apr-Jun:59(2):194-202. doi: 10.4103/ijc.IJC_676_19. Epub [PubMed PMID: 33753626]
Buckley E, Kondagari L. Sonography Postmenopausal Assessment, Protocols, and Interpretation. StatPearls. 2025 Jan:(): [PubMed PMID: 34033403]
Van Den Bosch T, Verbakel JY, Valentin L, Wynants L, De Cock B, Pascual MA, Leone FPG, Sladkevicius P, Alcazar JL, Votino A, Fruscio R, Lanzani C, Van Holsbeke C, Rossi A, Jokubkiene L, Kudla M, Jakab A, Domali E, Epstein E, Van Pachterbeke C, Bourne T, Van Calster B, Timmerman D. Typical ultrasound features of various endometrial pathologies described using International Endometrial Tumor Analysis (IETA) terminology in women with abnormal uterine bleeding. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2021 Jan:57(1):164-172. doi: 10.1002/uog.22109. Epub [PubMed PMID: 32484286]
Goldstein RB, Bree RL, Benson CB, Benacerraf BR, Bloss JD, Carlos R, Fleischer AC, Goldstein SR, Hunt RB, Kurman RJ, Kurtz AB, Laing FC, Parsons AK, Smith-Bindman R, Walker J. Evaluation of the woman with postmenopausal bleeding: Society of Radiologists in Ultrasound-Sponsored Consensus Conference statement. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2001 Oct:20(10):1025-36 [PubMed PMID: 11587008]
Level 3 (low-level) evidenceHamel CC, van Wessel S, Carnegy A, Coppus SFPJ, Snijders MPML, Clark J, Emanuel MH. Diagnostic criteria for retained products of conception-A scoping review. Acta obstetricia et gynecologica Scandinavica. 2021 Dec:100(12):2135-2143. doi: 10.1111/aogs.14229. Epub 2021 Aug 12 [PubMed PMID: 34244998]
Level 2 (mid-level) evidenceAkiba N, Iriyama T, Nakayama T, Seyama T, Sayama S, Kumasawa K, Komatsu A, Yabe S, Nagamatsu T, Osuga Y, Fujii T. Ultrasonographic vascularity assessment for predicting future severe hemorrhage in retained products of conception after second-trimester abortion. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2021 Feb:34(4):562-568. doi: 10.1080/14767058.2019.1610739. Epub 2019 Apr 29 [PubMed PMID: 31006292]
Expert Panel on Women’s Imaging Panel, Dudiak KM, Maturen KE, Akin EA, Bell M, Bhosale PR, Kang SK, Kilcoyne A, Lakhman Y, Nicola R, Pandharipande PV, Paspulati R, Reinhold C, Ricci S, Shinagare AB, Vargas HA, Whitcomb BP, Glanc P. ACR Appropriateness Criteria® Gestational Trophoblastic Disease. Journal of the American College of Radiology : JACR. 2019 Nov:16(11S):S348-S363. doi: 10.1016/j.jacr.2019.05.015. Epub [PubMed PMID: 31685103]
Marret H, Cayrol M. [Sonographic diagnosis of presumed benign ovarian tumors]. Journal de gynecologie, obstetrique et biologie de la reproduction. 2013 Dec:42(8):730-43. doi: 10.1016/j.jgyn.2013.09.028. Epub 2013 Nov 5 [PubMed PMID: 24200073]
Solanki V, Singh P, Sharma C, Ghuman N, Sureka B, Shekhar S, Gothwal M, Yadav G. Predicting Malignancy in Adnexal Masses by the International Ovarian Tumor Analysis-Simple Rules. Journal of mid-life health. 2020 Oct-Dec:11(4):217-223. doi: 10.4103/jmh.JMH_103_20. Epub 2021 Jan 21 [PubMed PMID: 33767562]
Timmerman D, Van Calster B, Testa A, Savelli L, Fischerova D, Froyman W, Wynants L, Van Holsbeke C, Epstein E, Franchi D, Kaijser J, Czekierdowski A, Guerriero S, Fruscio R, Leone FPG, Rossi A, Landolfo C, Vergote I, Bourne T, Valentin L. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. American journal of obstetrics and gynecology. 2016 Apr:214(4):424-437. doi: 10.1016/j.ajog.2016.01.007. Epub 2016 Jan 19 [PubMed PMID: 26800772]
Jeong YY, Outwater EK, Kang HK. Imaging evaluation of ovarian masses. Radiographics : a review publication of the Radiological Society of North America, Inc. 2000 Sep-Oct:20(5):1445-70 [PubMed PMID: 10992033]
Barloon TJ, Brown BP, Abu-Yousef MM, Warnock NG. Paraovarian and paratubal cysts: preoperative diagnosis using transabdominal and transvaginal sonography. Journal of clinical ultrasound : JCU. 1996 Mar-Apr:24(3):117-22 [PubMed PMID: 8838299]
Fatum M, Rojansky N, Shushan A. Papillary serous cystadenofibroma of the ovary--is it really so rare? International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2001 Oct:75(1):85-6 [PubMed PMID: 11597627]
Patel MD, Acord DL, Young SW. Likelihood ratio of sonographic findings in discriminating hydrosalpinx from other adnexal masses. AJR. American journal of roentgenology. 2006 Apr:186(4):1033-8 [PubMed PMID: 16554575]
Savelli L, de Iaco P, Ghi T, Bovicelli L, Rosati F, Cacciatore B. Transvaginal sonographic appearance of peritoneal pseudocysts. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2004 Mar:23(3):284-8 [PubMed PMID: 15027019]
Level 2 (mid-level) evidenceNatkanska A, Bizon-Szpernalowska MA, Milek T, Sawicki W. Peritoneal inclusion cysts as a diagnostic and treatment challenge. Ginekologia polska. 2021:92(8):583-586. doi: 10.5603/GP.a2021.0142. Epub [PubMed PMID: 34541630]
Nemoto Y, Ishihara K, Sekiya T, Konishi H, Araki T. Ultrasonographic and clinical appearance of hemorrhagic ovarian cyst diagnosed by transvaginal scan. Journal of Nippon Medical School = Nippon Ika Daigaku zasshi. 2003 Jun:70(3):243-9 [PubMed PMID: 12928726]
Kim HC, Kim SH, Lee HJ, Shin SJ, Hwang SI, Choi YH. Fluid-fluid levels in ovarian teratomas. Abdominal imaging. 2002 Jan-Feb:27(1):100-5 [PubMed PMID: 11740619]
Level 2 (mid-level) evidenceȘtefan RA, Ștefan PA, Mihu CM, Csutak C, Melincovici CS, Crivii CB, Maluțan AM, Hîțu L, Lebovici A. Ultrasonography in the Differentiation of Endometriomas from Hemorrhagic Ovarian Cysts: The Role of Texture Analysis. Journal of personalized medicine. 2021 Jun 28:11(7):. doi: 10.3390/jpm11070611. Epub 2021 Jun 28 [PubMed PMID: 34203314]
Ameye L, Timmerman D, Valentin L, Paladini D, Zhang J, Van Holsbeke C, Lissoni AA, Savelli L, Veldman J, Testa AC, Amant F, Van Huffel S, Bourne T. Clinically oriented three-step strategy for assessment of adnexal pathology. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2012 Nov:40(5):582-91. doi: 10.1002/uog.11177. Epub [PubMed PMID: 22511559]
Marko J, Marko KI, Pachigolla SL, Crothers BA, Mattu R, Wolfman DJ. Mucinous Neoplasms of the Ovary: Radiologic-Pathologic Correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2019 Jul-Aug:39(4):982-997. doi: 10.1148/rg.2019180221. Epub [PubMed PMID: 31283462]
Taylor EC, Irshaid L, Mathur M. Multimodality Imaging Approach to Ovarian Neoplasms with Pathologic Correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2021 Jan-Feb:41(1):289-315. doi: 10.1148/rg.2021200086. Epub 2020 Nov 13 [PubMed PMID: 33186060]
Shetty M. Imaging and Differential Diagnosis of Ovarian Cancer. Seminars in ultrasound, CT, and MR. 2019 Aug:40(4):302-318. doi: 10.1053/j.sult.2019.04.002. Epub 2019 Apr 25 [PubMed PMID: 31375171]
Kilinc YB, Sari L, Toprak H, Gultekin MA, Karabulut UE, Sahin N. Ovarian Granulosa Cell Tumor: A Clinicoradiologic Series with Literature Review. Current medical imaging. 2021:17(6):790-797. doi: 10.2174/1573405616666201228153755. Epub [PubMed PMID: 33371855]
Revzin MV, Mathur M, Dave HB, Macer ML, Spektor M. Pelvic Inflammatory Disease: Multimodality Imaging Approach with Clinical-Pathologic Correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2016 Sep-Oct:36(5):1579-96. doi: 10.1148/rg.2016150202. Epub [PubMed PMID: 27618331]
Kinay T, Unlubilgin E, Cirik DA, Kayikcioglu F, Akgul MA, Dolen I. The value of ultrasonographic tubo-ovarian abscess morphology in predicting whether patients will require surgical treatment. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2016 Oct:135(1):77-81. doi: 10.1016/j.ijgo.2016.04.006. Epub 2016 Jun 17 [PubMed PMID: 27381446]
Dawood MT, Naik M, Bharwani N, Sudderuddin SA, Rockall AG, Stewart VR. Adnexal Torsion: Review of Radiologic Appearances. Radiographics : a review publication of the Radiological Society of North America, Inc. 2021 Mar-Apr:41(2):609-624. doi: 10.1148/rg.2021200118. Epub 2021 Feb 12 [PubMed PMID: 33577417]
Ssi-Yan-Kai G, Rivain AL, Trichot C, Morcelet MC, Prevot S, Deffieux X, De Laveaucoupet J. What every radiologist should know about adnexal torsion. Emergency radiology. 2018 Feb:25(1):51-59. doi: 10.1007/s10140-017-1549-8. Epub 2017 Sep 7 [PubMed PMID: 28884300]
Wilson MP, Katlariwala P, Hwang J, Low G. Radiographic Features of a Benign Mixed Brenner Tumor and Mucinous Cystadenoma: A Rarely Identified Ovarian Neoplasm on Imaging. Journal of clinical imaging science. 2020:10():22. doi: 10.25259/JCIS_1_2020. Epub 2020 Apr 27 [PubMed PMID: 32363084]
Conte M, Guariglia L, Benedetti Panici P, Scambia G, Rabitti C, Capelli A, Mancuso S. Ovarian fibrothecoma: sonographic and histologic findings. Gynecologic and obstetric investigation. 1991:32(1):51-4 [PubMed PMID: 1662660]
Paladini D, Testa A, Van Holsbeke C, Mancari R, Timmerman D, Valentin L. Imaging in gynecological disease (5): clinical and ultrasound characteristics in fibroma and fibrothecoma of the ovary. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2009 Aug:34(2):188-95. doi: 10.1002/uog.6394. Epub [PubMed PMID: 19526595]
Level 2 (mid-level) evidenceChen J, Liu Y, Zhang Y, Wang Y, Chen X, Wang Z. Imaging, clinical, and pathologic findings of Sertoli-leydig cell tumors. Science progress. 2021 Apr-Jun:104(2):368504211009668. doi: 10.1177/00368504211009668. Epub [PubMed PMID: 33848213]
Kouakou B, Kamara I, Silue AD, Meite N, Botti RP, Tolo-Diebkile A, Sanogo I. [Retrospective study about 20 cases of ovarian Burkitt lymphoma at Yopougon teaching hospital in Côte d'Ivoire]. Bulletin du cancer. 2019 Mar:106(3):275-278. doi: 10.1016/j.bulcan.2018.12.011. Epub 2019 Feb 14 [PubMed PMID: 30771880]
Level 2 (mid-level) evidenceDorosiev E, Muzikadzhieva G, Mladenov B, Stoev I, Velev D. Renal abnormalities associated with Mayer-Rokitansky-Küster-Hauser syndrome. Folia medica. 2021 Oct 31:63(5):815-818. doi: 10.3897/folmed.63.e63325. Epub [PubMed PMID: 35851218]
Jayaprakasan K, Ojha K. Diagnosis of Congenital Uterine Abnormalities: Practical Considerations. Journal of clinical medicine. 2022 Feb 25:11(5):. doi: 10.3390/jcm11051251. Epub 2022 Feb 25 [PubMed PMID: 35268343]
Osayande AS, Mehulic S. Diagnosis and initial management of dysmenorrhea. American family physician. 2014 Mar 1:89(5):341-6 [PubMed PMID: 24695505]
Chaabane S, Nguyen Xuan HT, Paternostre A, Du Cheyron J, Harizi R, Mimouni M, Fauconnier A. [Endometriosis: Assessment of the Ultrasound-Based Endometriosis Staging System score (UBESS) in predicting surgical difficulty]. Gynecologie, obstetrique, fertilite & senologie. 2019 Mar:47(3):265-272. doi: 10.1016/j.gofs.2018.12.003. Epub 2019 Jan 26 [PubMed PMID: 30691974]
Menakaya U, Reid S, Lu C, Gerges B, Infante F, Condous G. Performance of ultrasound-based endometriosis staging system (UBESS) for predicting level of complexity of laparoscopic surgery for endometriosis. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2016 Dec:48(6):786-795. doi: 10.1002/uog.15858. Epub [PubMed PMID: 26764187]
Lee R, Dupuis C, Chen B, Smith A, Kim YH. Diagnosing ectopic pregnancy in the emergency setting. Ultrasonography (Seoul, Korea). 2018 Jan:37(1):78-87. doi: 10.14366/usg.17044. Epub 2017 Aug 19 [PubMed PMID: 29061036]
Barthelmess EK, Naz RK. Polycystic ovary syndrome: current status and future perspective. Frontiers in bioscience (Elite edition). 2014 Jan 1:6(1):104-19 [PubMed PMID: 24389146]
Level 3 (low-level) evidenceBello FA, Odeku AO. POLYCYSTIC OVARIES: A COMMON FEATURE IN TRANSVAGINAL SCANS OF GYNAECOLOGICAL PATIENTS. Annals of Ibadan postgraduate medicine. 2015 Dec:13(2):108-9 [PubMed PMID: 27162523]
Level 2 (mid-level) evidenceBalen AH, Laven JS, Tan SL, Dewailly D. Ultrasound assessment of the polycystic ovary: international consensus definitions. Human reproduction update. 2003 Nov-Dec:9(6):505-14 [PubMed PMID: 14714587]
Level 3 (low-level) evidenceMoschos E, Twickler DM. Prediction of polycystic ovarian syndrome based on ultrasound findings and clinical parameters. Journal of clinical ultrasound : JCU. 2015 Mar:43(3):157-63. doi: 10.1002/jcu.22182. Epub 2014 Jun 4 [PubMed PMID: 24898321]
Level 2 (mid-level) evidenceMentessidou A, Mirilas P. Surgical disorders in pediatric and adolescent gynecology: Vaginal and uterine anomalies. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2023 Mar:160(3):762-770. doi: 10.1002/ijgo.14362. Epub 2022 Aug 12 [PubMed PMID: 35880405]
Ramdani H, Benbrahim FZ, Jidal M, Zamani O, Drissi M, En-Nouali H, El Fenni J. Primary amenorrhea secondary to imperforate hymen. Clinical case reports. 2022 Apr:10(4):e05786. doi: 10.1002/ccr3.5786. Epub 2022 Apr 26 [PubMed PMID: 35498351]
Level 3 (low-level) evidenceAbdellaoui M, Fenni JE, Edderai M. [Mayer-Rokitansky-Küster-Hauser syndrome: a cause of primary amenorrhea: about a case]. The Pan African medical journal. 2021:40():260. doi: 10.11604/pamj.2021.40.260.29181. Epub 2021 Dec 23 [PubMed PMID: 35251454]
Level 3 (low-level) evidenceRodrigues EB, Braga J, Gama M, Guimarães MM. Turner syndrome patients' ultrasound profile. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology. 2013 Jul:29(7):704-6. doi: 10.3109/09513590.2013.797391. Epub [PubMed PMID: 23772782]
Level 2 (mid-level) evidenceAkierman SV, Skappak CD, Girgis R, Ho J. Turner Syndrome and apparent absent uterus: a case report and review of the literature. Journal of pediatric endocrinology & metabolism : JPEM. 2013:26(5-6):587-9. doi: 10.1515/jpem-2012-0408. Epub [PubMed PMID: 23443264]
Level 3 (low-level) evidenceAhmadi F, Javam M. Role of 3D sonohysterography in the investigation of uterine synechiae/asherman's syndrome: pictorial assay. Journal of medical imaging and radiation oncology. 2014 Apr:58(2):199-202. doi: 10.1111/1754-9485.12137. Epub 2013 Dec 3 [PubMed PMID: 24314038]
Tan IF, Robertson M. The role of imaging in the investigation of Asherman's syndrome. Australasian journal of ultrasound in medicine. 2011 Aug:14(3):15-18. doi: 10.1002/j.2205-0140.2011.tb00118.x. Epub 2015 Dec 31 [PubMed PMID: 28191115]
Chandler TM, Machan LS, Cooperberg PL, Harris AC, Chang SD. Mullerian duct anomalies: from diagnosis to intervention. The British journal of radiology. 2009 Dec:82(984):1034-42. doi: 10.1259/bjr/99354802. Epub 2009 May 11 [PubMed PMID: 19433480]
Acharya PT, Ponrartana S, Lai L, Vasquez E, Goodarzian F. Imaging of congenital genitourinary anomalies. Pediatric radiology. 2022 Apr:52(4):726-739. doi: 10.1007/s00247-021-05217-2. Epub 2021 Nov 5 [PubMed PMID: 34741177]
Zhang L, Zheng Q, Xie H, Du L, Wu L, Lin M. Quantitative cervical elastography: a new approach of cervical insufficiency prediction. Archives of gynecology and obstetrics. 2020 Jan:301(1):207-215. doi: 10.1007/s00404-019-05377-5. Epub 2019 Nov 22 [PubMed PMID: 31758303]
Fleischer AC, Harvey SM, Kurita SC, Andreotti RF, Zimmerman CW. Two-/three-dimensional transperineal sonography of complicated tape and mesh implants. Ultrasound quarterly. 2012 Dec:28(4):243-9. doi: 10.1097/RUQ.0b013e3182749585. Epub [PubMed PMID: 23149508]
Griffiths A, Koutsouridou R, Vaughan S, Penketh R, Roberts SA, Torkington J. Transrectal ultrasound and the diagnosis of rectovaginal endometriosis: a prospective observational study. Acta obstetricia et gynecologica Scandinavica. 2008:87(4):445-8. doi: 10.1080/00016340801948318. Epub [PubMed PMID: 18382872]
Level 2 (mid-level) evidenceBrown DL, Dudiak KM, Laing FC. Adnexal masses: US characterization and reporting. Radiology. 2010 Feb:254(2):342-54. doi: 10.1148/radiol.09090552. Epub 2010 Jan 20 [PubMed PMID: 20089722]