Introduction
Stress echocardiography combines two-dimensional echocardiography with a physical, pharmacological, or less commonly, electrical stress with atrial pacing. [1] Stress-induced ischemia generates new or worsening wall motion abnormalities in the segment supplied by the stenosed coronary artery.[2] Stress echocardiography plays an important role in identifying these wall motion abnormalities in the assessment of ischemic heart disease, and also plays a vital role in the evaluation of systolic or diastolic heart failure, valvular pathologies, nonischemic cardiomyopathy, pulmonary hypertension, and congenital heart disease. [3]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomy involves studying the various wall motion abnormalities and understanding the vascular territories associated with various segments. The segments are studied in six views: the parasternal long axis, the parasternal short axis at the levels of the mitral valve, papillary muscles, and apex, apical four chambers, apical two chambers. The scoring system is based on if the wall motion is normal, hypokinetic, akinetic, or dyskinetic. Based on the wall motion, a score of 1 to 4 is assigned. The American Society of Echocardiography uses a 17-segment model for wall motion abnormalities. [4]
Parasternal long axis (PLAX) view
Segments seen in parasternal long-axis view:
- Basal anteroseptal and mid anteroseptal on the septum: supplied by the left anterior descending artery
- Basal inferolateral and mid inferolateral: supplied by the right coronary artery or left circumflex artery
Apical four chambers (A4C) view
Segments seen in apical four-chamber view:
- Apical cap: supplied by left anterior descending artery, left circumflex artery
- The apical septum, mid inferoseptal: supplied by the left anterior descending artery
- Basal inferoseptal: supplied by right coronary artery
- Apical lateral, mid anterolateral, basal anterolateral: supplied by left circumflex artery
Apical two chambers (A2C) view
Segments saw in apical two-chamber view:
- Basal inferior, mid inferior: supplied by right coronary artery
- Apical anterior: supplied by a right coronary artery or left anterior descending artery
- Apical inferior, basal anterior, mid anterior: supplied by the left anterior descending artery
Parasternal short-axis (SAX) view
Segments seen in parasternal short-axis view at the papillary muscle level:
- Mid anteroseptal, mid anterior supplied by the left anterior descending artery
- Mid inferoseptal: supplied by right coronary artery
- Mid anterolateral, mid inferolateral: supplied by left circumflex artery
- Mid inferior: supplied by right coronary artery
Indications
- The following are indications for stress echocardiography: [5], [6], [7], [8]
- Coronary artery disease diagnosis
- To assess adequacy before and after revascularization
- Risk stratification in known coronary diseases
- Identifying the location of ischemia
- Preoperative risk assessment
- Evaluation for cardiac etiology of exertional dyspnea
- To assess valve disease
- Left bundle branch block
Contraindications
Contraindications to exercise/pharmacologic stress echocardiography: [9], [10]
Absolute
- Acute myocardial infarction within 48 hours
- Acute pericarditis/Myocarditis
- Symptomatic severe aortic stenosis
- Uncontrolled Arrhythmias causing symptoms or instability
- Acute aortic dissection
- High-risk Unstable Angina
- Decompensated or unstable heart failure with left ventricle ejection fraction (LVEF) less than 35%
- Acute pulmonary embolism or pulmonary infarction
Relative
- Left main coronary artery stenosis
- High degree atrioventricular (AV) block
- Severe hypertension (greater than 180/100mm Hg)
- Electrolyte abnormalities
- Mental or physical disability
- Tachycardia or bradyarrhythmia
- Moderate stenotic valvular heart disease
Specific contraindications to dipyridamole (or adenosine) and dobutamine stress echocardiography include severe conduction abnormalities (high-degree AV block without pacemaker), active bronchospasm, Sick sinus syndrome without a pacemaker, systolic blood pressure less than 90 mmHg, and tachyarrhythmias such as atrial fibrillation.
Equipment
Technical equipment for stress echocardiography includes:
- Ultrasound machine
- Probes: 3.5 MHz, 5 MHz
- The digital image acquisition system
- Blood pressure cuff and stethoscope
- Echo beds, workstations, ergonomic chair for the sonographer
- Contrast agitator machine/contrast for border delineation
- Emergency equipment includes a portable defibrillator, oxygen mask, bag-valve-mask resuscitator, intubation equipment, code carts, suction apparatus, syringes, needles, intravenous tubing
Stress echocardiography equipment takes into consideration M-mode, two-dimensional, color, and spectral (both flow and tissue) Doppler imaging for evaluation of ischemic heart disease.
Contrast agents are used as indicated for patients in whom at least two endocardial wall territories are not well visualized.
Technique or Treatment
Tissue harmonic imaging is indicated in stress echocardiography. It improves resolution, reduces artifacts, improves signal-to-noise ratio, greater depth of penetration and improves myocardial signals. Tissue harmonic imaging increases the sensitivity of stress echocardiography as it improves endocardial delineation due to enhanced resolution.[7][11][12][13]
Intravenous contrast agents in combination with harmonic imaging increase the accuracy of the procedure. Increased number of wall segment motion abnormalities can be studied when contrast agents are used.
Stress testing methods:
Exercise stress testing: This is indicated in patients who can exercise. Either treadmill or bicycle can be used for exercise.
- Treadmill stress echocardiography: Bruce protocol is most commonly used for treadmill exercise echocardiography. Exercise capacity is reported in terms of estimated metabolic equivalents of task (METs). Imaging studies are performed at rest and immediately after completion of exercise and compared for evaluation of wall motion abnormalities.
- Bicycle stress echocardiography: Less often used in North America than treadmill stress test. Can be performed using supine or upright bicycle ergometry. Usually, bicycle protocol starts at a workload of 25 watts and increases by 25-watt increments every three minutes until an endpoint is achieved. It is quieter, permits sensitive precordial measurements without much motion artifact. Bicycle exercise offers Doppler information in addition to assessment of regional wall motion abnormalities.
Pharmacologic stress testing: This is indicated in patients who cannot exercise. Dobutamine and vasodilators are used for assessing regional wall motion abnormalities. [10], [14]
- Dobutamine echocardiography: A graded dobutamine infusion starting at 5 mcg/kg/min and increasing at three-minute intervals to 10, 20, 30, and 40 ug/kg/min is the standard for dobutamine stress testing. [8] During dobutamine echocardiography, images are obtained before the start of the infusion, at the end of each stage, and during the recovery. The importance of low dose stages plays a role in recognition of viability and ischemia in segments with abnormal function at rest, even if viability assessment is not the main objective of the test. Endpoints are the achievement of target heart rate (defined as 85% of the age-predicted maximum heart rate), new or worsening wall motion abnormalities of moderate degree, significant arrhythmias, and intolerable symptoms. To achieve the target heart rate, Atropine can be used in divided doses of 0.25 mg to 0.5 mg to a total of 2 mg. Atropine increases the sensitivity of dobutamine echocardiography in patients receiving beta-blockers and in those with single-vessel disease.
- Vasodilator stress testing: Adenosine and Dipyridamole can be used in stress echocardiography. [15] Dipyridamole is administered at up to 0.84 mg/kg in two separate infusions: 0.56 mg/kg over four minutes, followed by four minutes of no dose and, if an adequate physiologic response is not achieved, then an additional 0.28 mg/kg is given over two minutes. [16] Atropine is used to enhance test sensitivity. Also, the addition of a handgrip at peak infusion enhances sensitivity. The duration of action of adenosine is shorter than dipyridamole. Adenosine stress is used to assess myocardial perfusion with contrast echocardiography but has not been used widely as a clinical tool.
- Pacing stress testing: This is indicated in patients with a permanent pacemaker. The target heart rate can be achieved by increasing the pacing. This is indicated in patients who are unable to exercise. The pacing protocol consists of two-minute stages, and an increasing paced heart rate to levels of 85% and 100%, respectively, for pre-peak and peak stress information. [10] Images are obtained at rest, the first stage, and pre-peak and peak heart rate. Termination of stress test occurs with the achievement of age-predicted maximal heart rate, new or worsening moderate regional wall motion abnormalities, greater than 2 mm horizontal or downsloping S-T depression, or presence of intolerable symptoms. [10]
Interpretation:
Imaging obtained at resting and stress phase are compared for interpretation of left ventricular (LV) size, shape, and function. A normal response during stress involves LV size becoming smaller compared to rest, while the shape is maintained, and there is increased endocardial excursion along with systolic wall thickening.
In a patient with multiple vessel diseases, exercise echocardiography demonstrates a dilated LV cavity with changes in the shape and reduction of systolic wall thickening of the septum, anterior, and inferior walls. Prolonged systolic wall thickening may also indicate severe coronary artery disease.
The coronary arteriographic cut off of luminal diameter stenosis at which wall thickening abnormalities occur is 54% for exercise, 58% for dobutamine, and 60% for dipyridamole. The sensitivities for the detection of coronary artery disease (CAD) are 85%, 80%, and 78%, with specificities of 77%, 86%, and 91% for exercise, dobutamine, and dipyridamole stress results. [9] However, diagnostic accuracy varies according to the pretest likelihood of CAD in the patient tested.
Complications
Dobutamine stress echocardiography: The most common cardiovascular side effects associated with dobutamine are angina, hypotension, and cardiac arrhythmias. [17] Atrial fibrillation and nonsustained ventricular arrhythmias occur in about 3% of patients. [18], [19] Sustained ventricular tachycardia is not common. Dobutamine can also induce left ventricular mid-cavity and outflow tract obstruction. Frequent premature atrial or ventricular contractions occur in about 10%. [20]
Vasodilator stress echocardiography: Major adverse reactions include myocardial infarction, asystole, and ventricular tachycardia. [21] Hypotension and bradycardia may occur but can be treated with aminophylline.
Pacing stress echocardiography: Wenckebach's second-degree heart block may occur, requiring atropine administration. [22]
Clinical Significance
In terms of clinical significance and diagnostic accuracy, stress echocardiography has an advantage in terms of specificity over standard exercise electrocardiography. When compared to nuclear perfusion imaging studies, stress echocardiography has similar accuracy, with a moderate sensitivity gap that is well balanced by a higher specificity. Both dipyridamole and dobutamine have overall good tolerance and feasibility. The choice of one test over the other depends on patients' clinical characteristics and the physician's preference. Diagnostic accuracy can significantly be affected by antianginal medical therapy, particularly beta-blocking agents, and therefore, it is recommended to withhold medical therapy at the time of testing to avoid a false-negative result.
Enhancing Healthcare Team Outcomes
Healthcare workers, including nurse practitioners, will frequently encounter patients with heart disease. One of the ways to investigate these patients is with stress echocardiography. Stress echocardiography is the combination of two-dimensional echocardiography with a physical, pharmacological, or less commonly, electrical stress with atrial pacing. Stress-induced ischemia generates new or worsening wall motion abnormalities in the segment supplied by the stenosed coronary artery. Stress echocardiography plays an important role in identifying these wall motion abnormalities in the assessment of ischemic heart disease, and also plays a vital role in the evaluation of systolic or diastolic heart failure, valvular pathologies, nonischemic cardiomyopathy, pulmonary hypertension, and congenital heart disease.
Media
(Click Image to Enlarge)
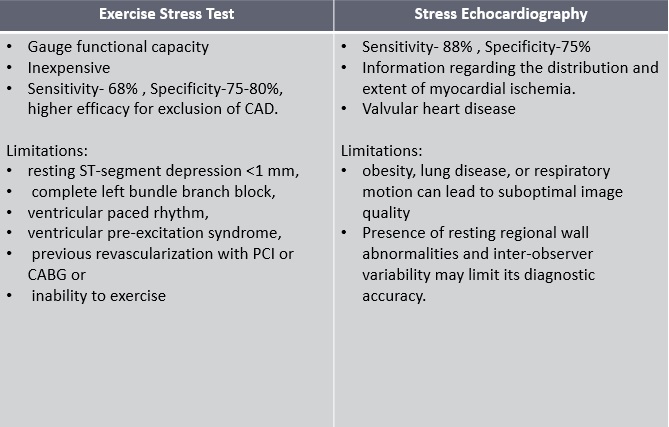
Difference between exercise electrocardiographic stress test and stress echocardiography. Contributed by StatPearls
(Click Image to Enlarge)
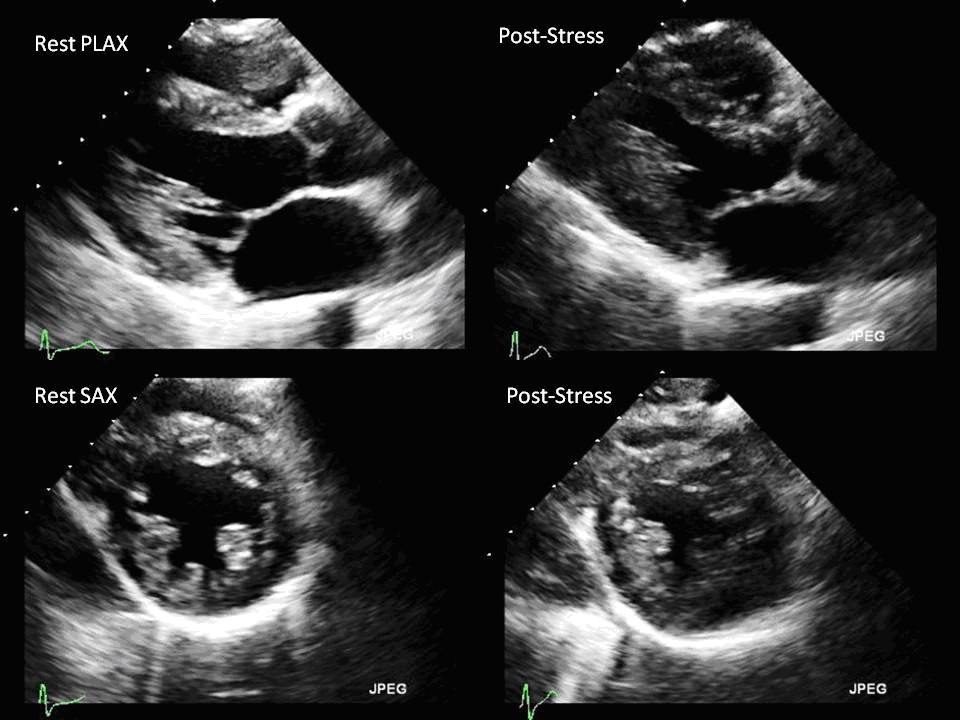
Above images are obtained at resting phase and post stress phase which are then compared for interpretation of left ventricular size, shape and function Contributed by Ateet Kosaraju
References
Picano E, Pasanisi E, Venneri L, Agrusta M, Mottola G, Sicari R. Stress echocardiography. Current pharmaceutical design. 2005:11(17):2137-49 [PubMed PMID: 16026284]
Gillam LD, Marcoff L. Stress Echocardiography. Circulation. Cardiovascular imaging. 2019 Jun:12(6):e009319. doi: 10.1161/CIRCIMAGING.119.009319. Epub 2019 Jun 17 [PubMed PMID: 31203671]
Sicari R, Cortigiani L. The clinical use of stress echocardiography in ischemic heart disease. Cardiovascular ultrasound. 2017 Mar 21:15(1):7. doi: 10.1186/s12947-017-0099-2. Epub 2017 Mar 21 [PubMed PMID: 28327159]
Pellikka PA, Nagueh SF, Elhendy AA, Kuehl CA, Sawada SG, American Society of Echocardiography. American Society of Echocardiography recommendations for performance, interpretation, and application of stress echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2007 Sep:20(9):1021-41 [PubMed PMID: 17765820]
Ágoston G, Morvai-Illés B, Pálinkás A, Varga A. The role of stress echocardiography in cardiovascular disorders. Kardiologia polska. 2019 Nov 22:77(11):1011-1019. doi: 10.33963/KP.15032. Epub 2019 Oct 24 [PubMed PMID: 31647477]
Pellikka PA, Roger VL, Oh JK, Miller FA, Seward JB, Tajik AJ. Stress echocardiography. Part II. Dobutamine stress echocardiography: techniques, implementation, clinical applications, and correlations. Mayo Clinic proceedings. 1995 Jan:70(1):16-27 [PubMed PMID: 7808046]
Aggeli C, Polytarchou K, Varvarousis D, Kastellanos S, Tousoulis D. Stress ECHO beyond coronary artery disease. Is it the holy grail of cardiovascular imaging? Clinical cardiology. 2018 Dec:41(12):1600-1610. doi: 10.1002/clc.23094. Epub 2018 Nov 24 [PubMed PMID: 30315566]
Kossaify A, Bassil E, Kossaify M. Stress Echocardiography: Concept and Criteria, Structure and Steps, Obstacles and Outcomes, Focused Update and Review. Cardiology research. 2020 Apr:11(2):89-96. doi: 10.14740/cr851. Epub 2020 Mar 10 [PubMed PMID: 32256915]
Płońska-Gościniak E, Gackowski A, Kukulski T, Kasprzak JD, Szyszka A, Braksator W, Gąsior Z, Lichodziejewska B, Pysz P. Stress echocardiography. Part I: Stress echocardiography in coronary heart disease. Journal of ultrasonography. 2019:19(76):45-48. doi: 10.15557/JoU.2019.0006. Epub [PubMed PMID: 31088010]
Mulvagh SL, Rakowski H, Vannan MA, Abdelmoneim SS, Becher H, Bierig SM, Burns PN, Castello R, Coon PD, Hagen ME, Jollis JG, Kimball TR, Kitzman DW, Kronzon I, Labovitz AJ, Lang RM, Mathew J, Moir WS, Nagueh SF, Pearlman AS, Perez JE, Porter TR, Rosenbloom J, Strachan GM, Thanigaraj S, Wei K, Woo A, Yu EH, Zoghbi WA, American Society of Echocardiography. American Society of Echocardiography Consensus Statement on the Clinical Applications of Ultrasonic Contrast Agents in Echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2008 Nov:21(11):1179-201; quiz 1281. doi: 10.1016/j.echo.2008.09.009. Epub [PubMed PMID: 18992671]
Level 3 (low-level) evidenceNtoskas T, Ahmad F, Woodmansey P. Safety and efficacy of physiologist-led dobutamine stress echocardiography: experience from a tertiary cardiac centre. Echo research and practice. 2018 Sep 1:5(3):105-112. doi: 10.1530/ERP-18-0038. Epub 2018 Sep 1 [PubMed PMID: 30303679]
Badiani S, Waddingham P, Lloyd G, Bhattacharyya S. Stress echocardiography in valvular heart disease. Expert review of cardiovascular therapy. 2018 Nov:16(11):795-804. doi: 10.1080/14779072.2018.1532791. Epub 2018 Oct 10 [PubMed PMID: 30286667]
Picano E, Ciampi Q, Wierzbowska-Drabik K, Urluescu ML, Morrone D, Carpeggiani C. The new clinical standard of integrated quadruple stress echocardiography with ABCD protocol. Cardiovascular ultrasound. 2018 Oct 2:16(1):22. doi: 10.1186/s12947-018-0141-z. Epub 2018 Oct 2 [PubMed PMID: 30285774]
Berbarie RF, Dib E, Ahmad M. Stress echocardiography using real-time three-dimensional imaging. Echocardiography (Mount Kisco, N.Y.). 2018 Aug:35(8):1196-1203. doi: 10.1111/echo.14050. Epub 2018 Jun 20 [PubMed PMID: 30133883]
Picano E, Sicari R, Varga A. Dipyridamole stress echocardiography. Cardiology clinics. 1999 Aug:17(3):481-99, viii [PubMed PMID: 10453294]
Imran MB, Pálinkás A, Picano E. Head-to-head comparison of dipyridamole echocardiography and stress perfusion scintigraphy for the detection of coronary artery disease: a meta-analysis. Comparison between stress echo and scintigraphy. The international journal of cardiovascular imaging. 2003 Feb:19(1):23-8 [PubMed PMID: 12602478]
Level 1 (high-level) evidenceBigi R. Complications of pharmacologic stress echocardiography in coronary artery disease. Clinical cardiology. 1996 Oct:19(10):776-80 [PubMed PMID: 8896909]
Mansencal N, Mustafic H, Hauguel-Moreau M, Lannou S, Szymanski C, Dubourg O. Occurrence of Atrial Fibrillation During Dobutamine Stress Echocardiography. The American journal of cardiology. 2019 Apr 15:123(8):1277-1282. doi: 10.1016/j.amjcard.2019.01.022. Epub 2019 Jan 31 [PubMed PMID: 30745020]
Pinton R, Lemke W, Garcia LG. [Symptoms, complications and hemodynamic changes related to dobutamine stress echocardiography]. Arquivos brasileiros de cardiologia. 1997 Sep:69(3):161-4 [PubMed PMID: 9595726]
Geleijnse ML, Krenning BJ, Nemes A, van Dalen BM, Soliman OI, Ten Cate FJ, Schinkel AF, Boersma E, Simoons ML. Incidence, pathophysiology, and treatment of complications during dobutamine-atropine stress echocardiography. Circulation. 2010 Apr 20:121(15):1756-67. doi: 10.1161/CIRCULATIONAHA.109.859264. Epub [PubMed PMID: 20404267]
Hirano Y, Yamamoto T, Uehara H, Nakamura H, Wufuer M, Yamada S, Ikawa H, Ishikawa K. [Complications of stress echocardiography]. Journal of cardiology. 2001 Aug:38(2):73-80 [PubMed PMID: 11525112]
Picano E, Alaimo A, Chubuchny V, Plonska E, Baldo V, Baldini U, Pauletti M, Perticucci R, Fonseca L, Villarraga HR, Emanuelli C, Miracapillo G, Hoffmann E, De Nes M. Noninvasive pacemaker stress echocardiography for diagnosis of coronary artery disease: a multicenter study. Journal of the American College of Cardiology. 2002 Oct 2:40(7):1305-10 [PubMed PMID: 12383579]
Level 2 (mid-level) evidence