Introduction
Trigonocephaly is the premature closure of the metopic suture causing the inability of the frontal bones to grow laterally, thus forming a triangular forehead with an obvious or subtle osseous ridge. The term "trigonocephaly" was coined by Welcker in 1862.[1] The word metopic comes from the Greek word "metopon," which translates to the forehead.[2] The premature fusion of the metopic suture, a type of craniosynostosis, produces a narrow forehead, causing the position of the eyes to be closer than usual (hypotelorism), raised or arched eyebrows, and lateral orbital retrusion with associated bilateral frontotemporal narrowing and compensatory occipital-biparietal widening.[3][4] It should be distinguished from the benign metopic ridge, where hypotelorism and frontotemporal narrowing are absent and have no other clinical features. 3D computed tomography (CT) scans can be used to distinguish them.[5][6]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Trigonocephaly is a post-neurulation defect that leads to premature fusion of the metopic suture, usually occurring before birth.[7] Metopic suture closure starts at 3 to 4 months of age and is completed at 8 to 9 months in most individuals.[8][9] The closure begins at the nasion, proceeding superiorly, and terminates at the anterior fontanelle.[9] Approximately 5.1% of the individuals have the suture open after one year of age. However, by two years of age, it should have closed. Using 3D CT scans, it has been demonstrated that the metopic suture's physiologic fusion occurs between the 3rd to 19th months.[10] Premature closure before the third month will cause trigonocephaly.
The specific etiology of craniosynostosis is unknown.[11] Genetic abnormalities, signaling pathways alterations, environmental factors, metabolic disorders, and intrauterine constraints have been implicated. Intrauterine constraint is defined as a condition where fetal movements are significantly reduced and can not move freely; if prolonged, it can cause craniofacial anomalies.[12] Some reports have associated maternal use of valproic acid with metopic craniosynostosis; however, no association was found in a recent meta-analysis.[13]
Rare non-syndromic cases have been described in which there is the fusion of both the metopic and the sagittal suture producing significant behavior and cognitive and motor impairment.[14] These patients require a combined surgical approach to treat both sutures. Thyroid dysfunction in mothers can contribute to metopic synostosis in children, next only to sagittal and coronal synostosis. Folic acid deficiency before pregnancy has also been proposed as a causative factor for trigonocephaly.[13]
The most notable genetic mutations recently identified in non-syndromic metopic synostosis are FREM1 and SMAD6.[13]
Epidemiology
The number of children born worldwide with craniosynostosis in 2019 was estimated to be 84,665, which included 72,857 with nonsyndromic craniosynostosis.[15] The overall incidence of all types of craniosynostosis is approximately 0.6 per 1000 live births. Metopic craniosynostosis comprises 10% to 31% of all isolated craniosynostosis and is more commonly seen in males.[16][17][18][19] The incidence of metopic craniosynostosis is approximately 1 per 5000 to 15000 live births.[20] It has been noted that the prevalence of metopic craniosynostosis has been increasing over the years in Europe and the United States.[13][17][18][21][22][23][15] It is now the second most common type of craniosynostosis, second only to scaphocephaly.[2][11][24] About three quarts of the patients are male, with a male-to-female ratio of 3.3:1.[21][25]
Nonsyndromic craniosynostosis accounts for approximately 85% of all craniosynostosis.[26] In more than 95% of the cases, it is sporadic. Trigonocephaly is usually nonsyndromic but, in some cases, can be associated with a syndrome. In a study evaluating the role of ethnicity in craniosynostosis, White race and African American parents were the principal ethnic groups identified; metopic craniosynostosis was significantly associated with the White population.[27] Many syndromic craniosynostosis patients have mental retardation. This is more prominent in metopic craniosynostosis than in other single-suture craniosynostoses.[28][29] About one-fourth of the patients with single-suture craniosynostosis have other organ-associated anomalies.
Pathophysiology
Approximately 6% to 10% of patients with trigonocephaly show genetic alterations.[30] Metopic craniosynostosis has been associated with several chromosomal abnormalities, including deletion of chromosome 11q24, 7p, 3q, 13q, 12pter, 22q11, deletion or trisomy of 9p, duplication of 15q25, and ERF and SMAD6 gene mutations.[13][26][31][32][33] Familial cases occur in approximately 5% of the cases, with an 8% frequency in twins.[34][35]
Due to the suture's premature fusion, there is lateral growth restriction of the frontal bone with shortening of the anterior cranial fossa.[9] The fusion of the suture produces a forehead midline bone ridge. The orbits are located closer than normal due to restricted lateral growth. Bitemporal indentations are noted. The anterior fontanelle is closed in about half of the cases.
Approximately 8% to 33% of the patients with metopic craniosynostosis have elevated intracranial pressure (ICP), which can produce neurodevelopmental delays, including speech and language retardation.[36][37][38][39][40][41] In one series, 78% of the patients had elevated ICP during surgery for trigonocephaly; however, most patients in this series were older, with a mean age of 5 years.[42] These findings suggest that uncorrected metopic craniosynostosis can seriously harm language development, motor function, and behavior. As the remaining skull sutures have increased compensatory growth, the cephalic index is maintained within normal limits.[43][44] The posterior skull has compensatory sagittal and transverse growth together with an upper face vertical and sagittal growth.[43] This compensatory growth of the non-fused sutures leads to the widened appearance of the parieto-occipital skull.[45]
History and Physical
Physical examination shows a visible midline forehead bony ridge leading to a deformity resembling a ship's keel. Hypotelorism is frequently noted. Patients have a narrow bitemporal skull dimension with a compensatory expanded biparietal dimension. Eyebrows are usually raised. The earlier the suture closure, the more severe will be the skull deformity.[45]
Cases can be classified as severe, moderate, and mild, depending on the angulation of the frontal bones.[46] Fundoscopy can be used for detecting raised intracranial pressure (ICP) in patients with craniosynostosis; however, papilledema is more commonly found in older children.[47]
Evaluation
The diagnosis is mainly clinical rather than radiological. The most obvious sign in the diagnosis is physical palpation of the anterior midsagittal bony ridge over the forehead. When viewed from the vertex or "birds-eye" view, the triangular shape of the head is characteristic in this condition.
Craniofacial anomalies like hypotelorism and temporal narrowing with parietal widening are, in most cases, sufficient to accurately diagnose craniosynostosis. These additional features differentiate craniosynostosis from the benign metopic ridge.
A head computed tomogram (CT) scan with 3D reconstruction is performed to confirm the diagnosis and plan the surgery. It will show that the frontal bones have a triangular shape, orbits are closer than normal, and there is anterior displacement of the coronal sutures. Widening of the posterior parietal regions, pterional constriction, and flattening of the supraorbital ridges with lateral orbital hypoplasia are also identified.
Prenatal head ultrasound can be used during the second and third trimesters to make the craniosynostosis diagnosis.[48][49][50] It can also be used in infants between the age of 8 to 12 months to avoid radiation exposure and the need for sedation.[51][52][53][54][55]
Radiographic Findings Associated with Metopic Synostosis
The presence of three or more specific findings is diagnostic for 96% of patients with metopic synostosis.[56] these findings are as follows:
- Omega sign - the prematurely fused metopic suture forms an "omega"-shaped invagination intracranially
- Interorbital narrowing - decreased distance between the medial orbital walls
- Upper orbital narrowing - the shape of the upper orbit is narrower than usual
- The frontal bone tangent intersects the orbital midline or more medially when viewed from above
- Posteriorly displaced lateral frontal bone
- Straight lateral frontal bone
- "Pulled" anterior fontanelle - Anterior fontanelle is partially open down the metopic suture
- Upsloping lateral orbital rim - the superior orbital rim is oriented more vertically than horizontally
Treatment / Management
Early operative treatment is recommended to provide the best possibility for the brain to expand and produce a normal configuration of the skull. Surgery goals are to remove the bony ridge of the metopic suture, advance both orbits and the frontal bones, achieve a rounder forehead contour, and prevent psychosocial impact and neurodevelopmental delay.[46] Advancing the orbits and frontal bones will improve the lateral and superior orbital rim projection, expand the lateral and superior frontal bones, and correct the pterional and frontozygomatic restriction.[11]
Endoscopic Surgery
This technique is best used before 3 to 4 months of age due to the skull's pliability. A small incision is made behind the hairline towards the metopic suture. A subgaleal plane is developed from the anterior fontanelle to the nasofrontal suture. A single bur hole is made, and a 30-degree endoscope is used to dissect the dura and the overlying stenosed suture. An osteotomy is made between the anterior fontanelle and the nasion using scissors.[57][58] A helmet is prepared and placed on the patient on the fifth postoperative day. It is used for the next 10 to 12 months to direct cranial growth by allowing cranial expansion. Endoscopic surgery significantly reduces blood loss, operative time, length of stay, and transfusion rate compared to open techniques.[13][59][60][61](B3)
Open Surgery
Open surgery is usually performed before the age of 1 year (9 to 12 months). A less radical procedure is used for cases where the main goal is to remove the midline bony ridge, and there is no need for orbital rim advancement. Drilling of the prominent metopic suture suffices. If there is a temporalis hollow, the temporalis muscle can be partially split and moved to a more anterior position. A zigzag or wavy coronal incision is used to preserve the superficial temporal arteries to maintain a robust blood supply. Dissection of the scalp flaps is done above the periosteal plane to reduce bleeding.
Open surgery requires a larger incision and is usually associated with longer operative time and hospitalization. Blood transfusions are almost always needed. All these drawbacks increased overall healthcare costs. In those cases where cranial reconstruction is required, a bifrontal craniotomy is performed to reconstruct the anterior cranial vault, including the lateral portions of the sphenoid wings, to allow brain expansion. The bifrontal bone flap undergoes radial osteotomies to reshape the bone. The midline ridge requires shaping with the drill. To perform the fronto-orbital advancement, the periosteum above the supraorbital rim is open before the bilateral orbital rim osteotomy and advancement are performed. Orbital osteotomies are performed using a reciprocating bone saw. A free supraorbital bone is created and reshaped to a more convex configuration, especially along the superolateral orbital rim. This is done with several closed wedge osteotomies along the free supraorbital bone bar. If the hypoteloric deformity is severe, an interposition split-thickness cranial bone graft is added. The orbital rim is moved forward, and fixation plates are placed to maintain the advancement.[2][3][13][37][62](B3)
Alternatively, absorbable sutures can be used. Using sutures and avoiding plates and screws reduces surgery costs and allows natural reshaping.[1] The temporal bone is split and advanced to correct the abnormal inward angulation after the lateral orbital rims are advanced. For those patients operated on at an early age, overcorrection by approximately 1.5 cm is recommended to compensate for the impaired bifrontal growth.[3][63] Using preoperative erythropoietin and ferrous sulfate with the addition of perioperative tranexamic acid reduces transfusions in patients with metopic craniosynostosis undergoing craniofacial reconstruction.[37][64](B3)
An alternative approach when reconstructing the orbits is to remodel the orbital rim in situ to preserve the attachment to the zygoma and incline the cephalic portion of the supraorbital rim anteriorly. The fixation is done using resorbable fixation plates. The orbital rim will advance with brain growth. Another alternative approach is the in situ bandeau approach, where the supraorbital bandeau is not separated at its central point at the nasion to maintain its blood supply.[45] Partial osteotomies are made to facilitate the bending of the bandeau. Using bone benders, the bandeau is flattened to bring forward the supraorbital rims and the lateral bone margins. The lateral margins are bent back with greenstick fractures to align with the temporal bones, which are repositioned outward and then fixed to the bandeau with resorbable plates. In another alternative procedure, the supraorbital bandeau is left in situ at the temporal bones. It is split at the midline with a hinge technique, and an interposition bone graft is placed at the nasofrontal area.[65]
Lille’s technique: Involves resection of the metopic suture followed by the construction of a large frontal panel that is stabilized with absorbable plates. This is accompanied by fronto-orbital advancement, parietal craniectomies, and pterional resection. This technique facilitates the optimization of cranial expansion and permits future cranial growth.[66]
Di Rocco technique: This helps to control bleeding over the glabella and ophryon. It follows the principle of direct visualization of emissary metopic veins and the superior sagittal sinus, thereby having better control of hemostasis before removing the last piece of the frontal bone. This is achieved by manipulating the design of the frontal craniotomy so that a triangle of bone based above the glabella at the site of the osteotomy of the bandeau is conserved.[67]
Method of “hypercorrection” proposed by Bennett et al.: This technique helps to attain a better cosmetic result and to reduce relapse and the need for revision surgery. The method involves a fronto-orbital advancement of 2.5 to 3.5 cm and concomitant hyperexpansion of the bitemporal projection. Despite this, some patients may need additional corrections; lateral orbital recession and bitemporal constriction have rarely been reported following this procedure.[68]
Conservative Management
If the deformity is mild or there is only a bony ridge without hypotelorism, a more conservative approach can be used; however, the child should be followed for a minimum of 12 months of age to assess and corroborate adequate cranial growth. Clinical evaluations and family discussions regarding neuropsychological development are engaged during this time.[45] During the first years of life, the child's development is periodically evaluated to ascertain that no language, motor, or behavior problems develop.
Differential Diagnosis
The most common differential diagnosis of trigonocephaly is a metopic ridge, which is physiological and does not need surgery. Trigonocephaly presents at a younger age, and the appearance of the lateral frontal bone and lateral orbit can help distinguish whether the condition is pathological.[4]
The single metopic suture craniosynostosis has to be differentiated from syndromic craniosynostosis, which most commonly involves the coronal suture producing brachycephaly.[69]
- Apert syndrome
- Crouzon syndrome
- Muenke syndrome
- Pfeiffer syndrome
- Saether Chotzen syndrome
- Craniofrontonasal syndrome
- Carpenter syndrome
Secondary synostosis can be caused by several conditions but often involves multiple sutures.[70][71]
- Hyperthyroidism
- Hypercalcemia
- Hypophosphatemia
- Rickets
- Sickle cell anemia
- Thalassemia
- Polycythemia vera
- Microcephaly
- Prematurity
- Teratogens (phenytoin, valproic acid, retinoic acid, aminopterin)
Prognosis
Surgical correction provides adequate cosmetic results in the majority of patients. Comparison at two years of age of the endoscopic strip craniectomy followed by helmet use and the open skull reconstruction showed that both offer an excellent head shape outcome.[72] The majority of surgically corrected patients have academic achievement near the national mean and above-average intelligence quotient; however, neurocognitive function correlates with the severity of craniosynostosis.[73] The mortality rate for all types of craniosynostosis is well below 1%.[3][35]
Untreated patients show problems with cognitive functioning when compared to healthy controls.[74] Patients with untreated severe metopic craniosynostosis have been found to have reduced auditory processing of language stimuli in the frontal cortex, suggesting that the orbitofrontal deformity has a negative effect on the frontal cortex.[16]
Children with metopic craniosynostosis, unoperated or operated, have worse general cognition, motor functioning, attention, verbal and visuospatial abilities, and behavior than their healthy peers.[75] Despite corrective surgery, intellectual disabilities and behavioral disorders may occur or persist.[24][75] These patients can show behavioral, cognitive, and psychological problems and therefore necessitate support and ongoing monitoring.[75] Neurodevelopmental and ophthalmological follow-up in patients with complex craniosynostosis is recommended, even after successful cranial remodeling.
Complications
Surgical complications after metopic craniosynostosis correction are usually relatively few and minor.[37][57][76] These include:
- Excessive blood loss
- Dural tears
- Meningitis
- Stroke
- Pseudomeningoceles
- Hyperthermia
- Hypoactivity
- Local wound infection
- Epidural abscess
- Subcutaneous hematoma
- Epidural hematoma
- Subdural hematoma
- Air embolus
- Incomplete correction
- Temporal hollowing
- Stretched scar/keloid
- Reoperation
- Contact dermatitis from helmet use
- Scalp abrasion from helmet use
Despite the surgical correction, some patients may still present increased ICP, estimated to be 3% of the cases at an average of 57 months after the initial surgery.[37][77][78] This is corrected with a subsequent calvarial expansion surgery.[37] Some patients need another surgery to fill bone defects later in their life.[77]
Late Complications
Contour irregularities in the frontal region and temporal hollowing: This may need further treatment in the form of lipoinjection[79] (if the condition is affecting the academic performance and personality development of the child) or a recontouring procedure using hydroxyapatite onlay (after the age of 14 to 16 years).[37] For those with long-term sequelae, the use of cutting guides to facilitate scheduled complex reconstruction with autologous bone can be useful.[80]
Postoperative and Rehabilitation Care
Patients are sent overnight to the pediatric intensive care unit to closely monitor vital signs and evaluate the necessity of additional blood transfusions. The drain, if placed, is removed the next day. If stable, the patient is sent to the ward for another day. When discharged, the patient is followed at the clinic for wound inspection and suture removal. The head shape is followed at three months, six months, and then annually with photography and anthropometric measurements. The patients are also closely evaluated for behavioral, cognitive, and psychological problems.
Consultations
The following consultations are required:
- Pediatric neurosurgeon
- Plastic surgeon
- Craniofacial surgeon
- Pediatric intensivist
- Pediatric anesthesiologist
- Ophthalmologist
- Geneticist
Deterrence and Patient Education
Surgery for trigonocephaly is advocated before the age of 1 year for better cosmetic results.[81] There is still little consensus in cases of mild trigonocephaly. In a survey sent to 102 craniofacial surgeons, there is a disparity of opinion regarding the management of mild nonsyndromic metopic craniosynostosis.[82] However, all of them agreed to operate in moderate and severe cases. Most surgeons prefer open procedures, but the approach used varies. The ideal timing for orbital advancement is still debated; however, most prefer to perform it between 6-10 months of age.[82]
Screening for SMAD6 mutations is recommended in patients with nonsyndromic metopic craniosynostosis as its presence confers a high risk for recurrence in another pregnancy.[26] In those cases where the mutation is identified, genetic counseling is recommended.
Head 3D CT scans are helpful as an educational tool for families to understand the condition.
Enhancing Healthcare Team Outcomes
An interprofessional team of specialists includes a pediatric neurosurgeon, plastic surgeon, craniofacial surgeon, pediatric anesthesiologist, and a pediatric intensivist that must use an integrated care pathway combined with an evidence-based approach to evaluate and manage patients with metopic craniosynostosis can improve outcomes. Nursing staff round out the interprofessional team. Patients with suspected premature closure of the metopic suture should be closely followed to make an early diagnosis and avoid delays that may cause neurodevelopmental delay and later psychosocial impact on the child. Pediatricians should refer to these patients early for evaluation and possible therapy.
Referrals do not need to include radiographic studies, as these should be ordered by the specialist if necessary. Nurses can assist in assessment, perform patient counseling, and help coordinate activities of the various clinical specialties. Open communication lines between all care team members are crucial to a properly functioning interprofessional management approach, leading to improved patient outcomes. [Level 5]
Media
(Click Image to Enlarge)
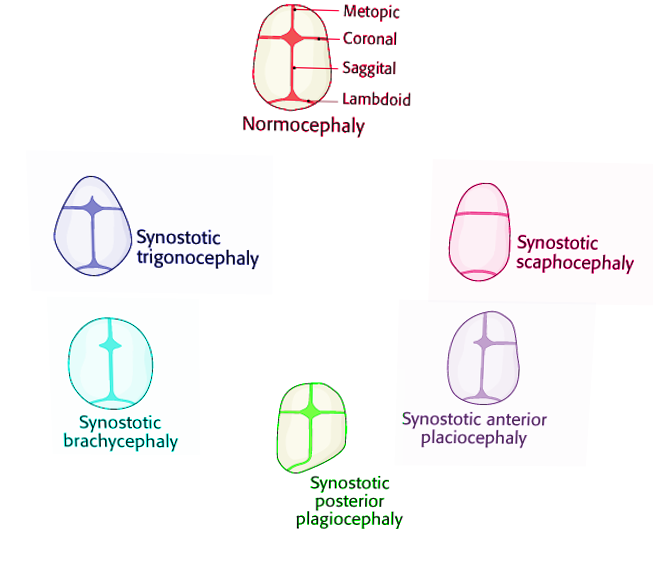
Craniosynostosis Image courtesy Dr Chaigasame
(Click Image to Enlarge)
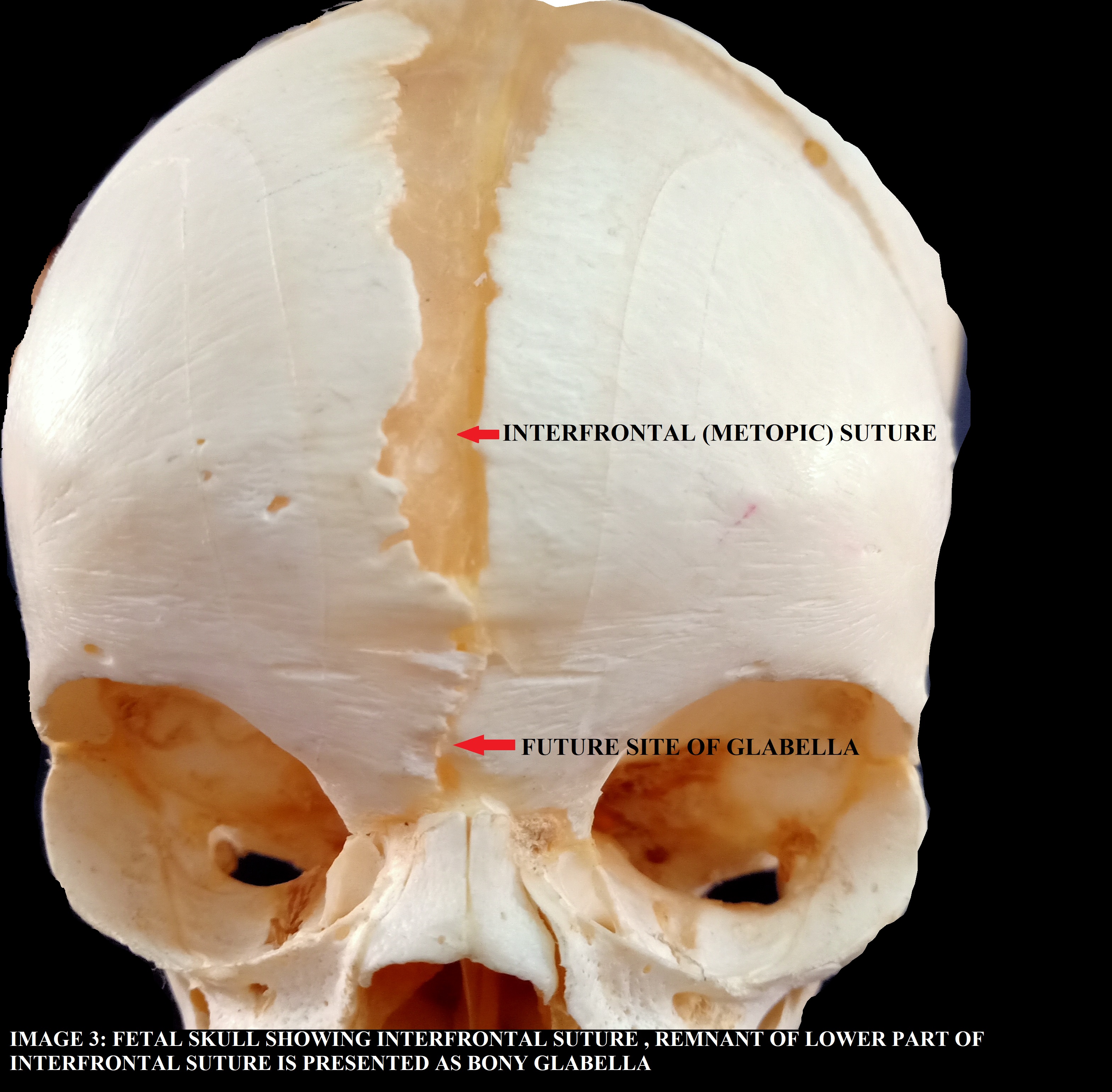
INTERFRONTAL (METOPIC) SUTURE AND FUTURE SITE OF GLABELLA IN FETAL SKULL Contributed by the Dr. Pradip Chauhan (MS ANATOMY), Department of Anatomy, P.D.U. MEDICAL COLLEGE, RAJKOT, Gujarat, India.
References
Mohammad D,Dhandapani S, Trigonocephaly: A simple modified technique. Journal of pediatric neurosciences. 2014 May; [PubMed PMID: 25250065]
Level 3 (low-level) evidencevan der Meulen J, Metopic synostosis. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2012 Sep; [PubMed PMID: 22872249]
Dempsey RF,Monson LA,Maricevich RS,Truong TA,Olarunnipa S,Lam SK,Dauser RC,Hollier LH Jr,Buchanan EP, Nonsyndromic Craniosynostosis. Clinics in plastic surgery. 2019 Apr [PubMed PMID: 30851746]
Blessing M,Gallagher ER, Epidemiology, Genetics, and Pathophysiology of Craniosynostosis. Oral and maxillofacial surgery clinics of North America. 2022 Aug [PubMed PMID: 35787827]
Cho MJ,Kane AA,Seaward JR,Hallac RR, Metopic "ridge" vs. "craniosynostosis": Quantifying severity with 3D curvature analysis. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2016 Sep [PubMed PMID: 27449480]
Birgfeld CB,Heike CL,Al-Mufarrej F,Oppenheimer A,Kamps SE,Adidharma W,Siebold B, Practical Computed Tomography Scan Findings for Distinguishing Metopic Craniosynostosis from Metopic Ridging. Plastic and reconstructive surgery. Global open. 2019 Mar; [PubMed PMID: 31044100]
Hayward R,Jones B,Evans R, Functional outcome after surgery for trigonocephaly. Plastic and reconstructive surgery. 1999 Aug [PubMed PMID: 10654710]
Level 3 (low-level) evidenceVinchon M, The metopic suture: Natural history. Neuro-Chirurgie. 2019 Nov; [PubMed PMID: 31562880]
Weinzweig J,Kirschner RE,Farley A,Reiss P,Hunter J,Whitaker LA,Bartlett SP, Metopic synostosis: Defining the temporal sequence of normal suture fusion and differentiating it from synostosis on the basis of computed tomography images. Plastic and reconstructive surgery. 2003 Oct; [PubMed PMID: 14504503]
Teager SJ,Constantine S,Lottering N,Anderson PJ, Physiologic closure time of the metopic suture in South Australian infants from 3D CT scans. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2019 Feb [PubMed PMID: 30218142]
Jaskolka MS, Current Controversies in Metopic Suture Craniosynostosis. Oral and maxillofacial surgery clinics of North America. 2017 Nov [PubMed PMID: 28987228]
Higginbottom MC,Jones KL,James HE, Intrauterine constraint and craniosynostosis. Neurosurgery. 1980 Jan; [PubMed PMID: 7354899]
Mocquard C,Aillet S,Riffaud L, Recent advances in trigonocephaly. Neuro-Chirurgie. 2019 Nov; [PubMed PMID: 31568780]
Level 3 (low-level) evidenceShimoji T,Kimura T,Shimoji K,Miyajima M, The metopic-sagittal craniosynostosis-report of 35 operative cases. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2017 Aug [PubMed PMID: 28470385]
Level 3 (low-level) evidenceShlobin NA,Baticulon RE,Ortega CA,Du L,Bonfield CM,Wray A,Forrest CR,Dewan MC, Global Epidemiology of Craniosynostosis: A Systematic Review and Meta-Analysis. World neurosurgery. 2022 Aug [PubMed PMID: 35636659]
Level 1 (high-level) evidenceYang JF,Brooks ED,Hashim PW,Reuman HS,Travieso R,Terner J,Mayes LC,Steinbacher DM,Persing JA,McPartland JC, The Severity of Deformity in Metopic Craniosynostosis Is Correlated with the Degree of Neurologic Dysfunction. Plastic and reconstructive surgery. 2017 Feb; [PubMed PMID: 28121881]
van der Meulen J,van der Hulst R,van Adrichem L,Arnaud E,Chin-Shong D,Duncan C,Habets E,Hinojosa J,Mathijssen I,May P,Morritt D,Nishikawa H,Noons P,Richardson D,Wall S,van der Vlugt J,Renier D, The increase of metopic synostosis: a pan-European observation. The Journal of craniofacial surgery. 2009 Mar; [PubMed PMID: 19326483]
Level 2 (mid-level) evidenceSelber J,Reid RR,Chike-Obi CJ,Sutton LN,Zackai EH,McDonald-McGinn D,Sonnad SS,Whitaker LA,Bartlett SP, The changing epidemiologic spectrum of single-suture synostoses. Plastic and reconstructive surgery. 2008 Aug; [PubMed PMID: 18626371]
Level 2 (mid-level) evidenceFearon JA,Singh DJ,Beals SP,Yu JC, The diagnosis and treatment of single-sutural synostoses: are computed tomographic scans necessary? Plastic and reconstructive surgery. 2007 Oct; [PubMed PMID: 17898608]
Cornelissen M,Ottelander Bd,Rizopoulos D,van der Hulst R,Mink van der Molen A,van der Horst C,Delye H,van Veelen ML,Bonsel G,Mathijssen I, Increase of prevalence of craniosynostosis. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2016 Sep; [PubMed PMID: 27499511]
Schraw JM,Woodhouse JP,Langlois PH,Canfield MA,Scheuerle AE,Agopian AJ,Benjamin RH,Lupo PJ, Risk factors and time trends for isolated craniosynostosis. Birth defects research. 2020 Oct 22; [PubMed PMID: 33091229]
Bennett KG,Bickham RS,Robinson AB,Buchman SR,Vercler CJ, Metopic Craniosynostosis: A Demographic Analysis Outside an Urban Environment. The Journal of craniofacial surgery. 2016 May; [PubMed PMID: 27159853]
Di Rocco F,Arnaud E,Meyer P,Sainte-Rose C,Renier D, Focus session on the changing [PubMed PMID: 19357856]
Wójcicki P,Prudel B, Trigonocephaly: Long-term results after surgical correction of metopic suture synostosis. Advances in clinical and experimental medicine : official organ Wroclaw Medical University. 2019 May; [PubMed PMID: 30712337]
Level 3 (low-level) evidenceBoyadjiev SA, Genetic analysis of non-syndromic craniosynostosis. Orthodontics [PubMed PMID: 17651129]
Timberlake AT,Persing JA, Genetics of Nonsyndromic Craniosynostosis. Plastic and reconstructive surgery. 2018 Jun; [PubMed PMID: 29579021]
Sacks GN,Skolnick GB,Trachtenberg A,Naidoo SD,Lopez J,Oh AK,Chao JW,Dorafshar A,Vercler CJ,Buchman SR,Patel K, The Impact of Ethnicity on Craniosynostosis in the United States. The Journal of craniofacial surgery. 2019 Nov-Dec; [PubMed PMID: 31609944]
Anderson FM, Treatment of coronal and metopic synostosis: 107 cases. Neurosurgery. 1981 Feb; [PubMed PMID: 7207779]
Level 3 (low-level) evidenceShillito J Jr,Matson DD, Craniosynostosis: a review of 519 surgical patients. Pediatrics. 1968 Apr; [PubMed PMID: 5643989]
Level 2 (mid-level) evidenceArmand T,Schaefer E,Di Rocco F,Edery P,Collet C,Rossi M, Genetic bases of craniosynostoses: An update. Neuro-Chirurgie. 2019 Nov; [PubMed PMID: 31605683]
Timberlake AT,Choi J,Zaidi S,Lu Q,Nelson-Williams C,Brooks ED,Bilguvar K,Tikhonova I,Mane S,Yang JF,Sawh-Martinez R,Persing S,Zellner EG,Loring E,Chuang C,Galm A,Hashim PW,Steinbacher DM,DiLuna ML,Duncan CC,Pelphrey KA,Zhao H,Persing JA,Lifton RP, Two locus inheritance of non-syndromic midline craniosynostosis via rare {i}SMAD6{/i} and common {i}BMP2{/i} alleles. eLife. 2016 Sep 8; [PubMed PMID: 27606499]
Jehee FS,Johnson D,Alonso LG,Cavalcanti DP,de Sá Moreira E,Alberto FL,Kok F,Kim C,Wall SA,Jabs EW,Boyadjiev SA,Wilkie AO,Passos-Bueno MR, Molecular screening for microdeletions at 9p22-p24 and 11q23-q24 in a large cohort of patients with trigonocephaly. Clinical genetics. 2005 Jun; [PubMed PMID: 15857417]
Level 2 (mid-level) evidenceAzimi C,Kennedy SJ,Chitayat D,Chakraborty P,Clarke JT,Forrest C,Teebi AS, Clinical and genetic aspects of trigonocephaly: a study of 25 cases. American journal of medical genetics. Part A. 2003 Mar 1; [PubMed PMID: 12567409]
Level 3 (low-level) evidenceDhellemmes P,Pellerin P,Lejeune JP,Lepoutre F, Surgical treatment of trigonocephaly. Experience with 30 cases. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 1986; [PubMed PMID: 3791279]
Level 3 (low-level) evidenceDiRocco C,Caldarelli M,Ceddia A,Iannelli A,Velardi F, [Craniostenosis. Analysis of 161 cases surgically treated during the first year of life]. Minerva pediatrica. 1989 Aug; [PubMed PMID: 2601658]
Level 3 (low-level) evidenceTamburrini G, Caldarelli M, Massimi L, Santini P, Di Rocco C. Intracranial pressure monitoring in children with single suture and complex craniosynostosis: a review. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2005 Oct:21(10):913-21 [PubMed PMID: 15871027]
Natghian H,Song M,Jayamohan J,Johnson D,Magdum S,Richards P,Wall S, Long-Term Results in Isolated Metopic Synostosis: The Oxford Experience over 22 Years. Plastic and reconstructive surgery. 2018 Oct; [PubMed PMID: 30020237]
Cohen SR,Persing JA, Intracranial pressure in single-suture craniosynostosis. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association. 1998 May; [PubMed PMID: 9603551]
Renier D,Sainte-Rose C,Marchac D,Hirsch JF, Intracranial pressure in craniostenosis. Journal of neurosurgery. 1982 Sep; [PubMed PMID: 7097333]
Thompson DN,Harkness W,Jones B,Gonsalez S,Andar U,Hayward R, Subdural intracranial pressure monitoring in craniosynostosis: its role in surgical management. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 1995 May; [PubMed PMID: 7648567]
Thompson DN,Malcolm GP,Jones BM,Harkness WJ,Hayward RD, Intracranial pressure in single-suture craniosynostosis. Pediatric neurosurgery. 1995; [PubMed PMID: 7547454]
Shimoji T,Tomiyama N, Mild trigonocephaly and intracranial pressure: report of 56 patients. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2004 Oct; [PubMed PMID: 15185114]
Level 2 (mid-level) evidencePosnick JC,Lin KY,Chen P,Armstrong D, Metopic synostosis: quantitative assessment of presenting deformity and surgical results based on CT scans. Plastic and reconstructive surgery. 1994 Jan; [PubMed PMID: 8278471]
Level 2 (mid-level) evidenceKolar JC,Salter EM, Preoperative anthropometric dysmorphology in metopic synostosis. American journal of physical anthropology. 1997 Jul; [PubMed PMID: 9261497]
Hubli EH,Roberts RA, Correction of metopic synostosis utilizing an in situ bandeau approach. Seminars in plastic surgery. 2014 Aug; [PubMed PMID: 25210504]
Oi S,Matsumoto S, Trigonocephaly (metopic synostosis). Clinical, surgical and anatomical concepts. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 1987; [PubMed PMID: 3427566]
Tuite GF,Chong WK,Evanson J,Narita A,Taylor D,Harkness WF,Jones BM,Hayward RD, The effectiveness of papilledema as an indicator of raised intracranial pressure in children with craniosynostosis. Neurosurgery. 1996 Feb; [PubMed PMID: 8869054]
Cornelissen MJ,Apon I,van der Meulen JJNM,Groenenberg IAL,Kraan-van der Est MN,Mathijssen IMJ,Bonsel GJ,Cohen-Overbeek TE, Prenatal ultrasound parameters in single-suture craniosynostosis. The journal of maternal-fetal [PubMed PMID: 28553772]
Miller C,Losken HW,Towbin R,Bowen A,Mooney MP,Towbin A,Faix RS, Ultrasound diagnosis of craniosynostosis. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association. 2002 Jan; [PubMed PMID: 11772173]
Level 2 (mid-level) evidenceConstantine S,Kiermeier A,Anderson P, The Normal Fetal Cephalic Index in the Second and Third Trimesters of Pregnancy. Ultrasound quarterly. 2020 Sep; [PubMed PMID: 32898393]
Proisy M,Bruneau B,Riffaud L, How ultrasonography can contribute to diagnosis of craniosynostosis. Neuro-Chirurgie. 2019 Nov; [PubMed PMID: 31586456]
Okamoto T,Nuri T,Harada A,Kyutoku S,Ueda K, Cranial Suture Measurement by 2-point Method in Ultrasound Screening of Craniosynostosis. Plastic and reconstructive surgery. Global open. 2019 May; [PubMed PMID: 31333954]
Pogliani L,Zuccotti GV,Furlanetto M,Giudici V,Erbetta A,Chiapparini L,Valentini L, Cranial ultrasound is a reliable first step imaging in children with suspected craniosynostosis. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2017 Sep; [PubMed PMID: 28578511]
Proisy M,Riffaud L,Chouklati K,Tréguier C,Bruneau B, Ultrasonography for the diagnosis of craniosynostosis. European journal of radiology. 2017 May; [PubMed PMID: 28583642]
Hall KM,Besachio DA,Moore MD,Mora AJ,Carter WR, Effectiveness of screening for craniosynostosis with ultrasound: a retrospective review. Pediatric radiology. 2017 May; [PubMed PMID: 28213626]
Level 2 (mid-level) evidenceBirgfeld CB,Saltzman BS,Hing AV,Heike CL,Khanna PC,Gruss JS,Hopper RA, Making the diagnosis: metopic ridge versus metopic craniosynostosis. The Journal of craniofacial surgery. 2013 Jan [PubMed PMID: 23348281]
Level 2 (mid-level) evidenceJimenez DF,McGinity MJ,Barone CM, Endoscopy-assisted early correction of single-suture metopic craniosynostosis: a 19-year experience. Journal of neurosurgery. Pediatrics. 2018 Sep 28; [PubMed PMID: 30265229]
Jimenez DF,Barone CM, Early treatment of anterior calvarial craniosynostosis using endoscopic-assisted minimally invasive techniques. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2007 Dec; [PubMed PMID: 17899128]
Gomar-Alba M,Rivero-Garvia M,Márquez-Rivas J, Letter to the editor regarding: [PubMed PMID: 33053405]
Level 3 (low-level) evidenceLajthia O,Rogers GF,Tsering D,Keating RF,Magge SN, Quantitative outcomes of endoscopic strip craniectomy for metopic craniosynostosis in children with severe trigonocephaly. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2020 Aug 19; [PubMed PMID: 32812117]
Braun TL,Eisemann BS,Olorunnipa O,Buchanan EP,Monson LA, Safety Outcomes in Endoscopic Versus Open Repair of Metopic Craniosynostosis. The Journal of craniofacial surgery. 2018 Jun; [PubMed PMID: 29461368]
Panchal J,Uttchin V, Management of craniosynostosis. Plastic and reconstructive surgery. 2003 May; [PubMed PMID: 12711969]
Fearon JA,Ditthakasem K,Chan WNJ,Herbert M, Long-Term Growth following Trigonocephaly Repairs: Are Overcorrections Necessary? Plastic and reconstructive surgery. 2020 Mar; [PubMed PMID: 32097321]
Escher PJ,Tu AD,Kearney SL,Linabery AM,Petronio JA,Kebriaei MA,Chinnadurai S,Tibesar RJ, A protocol of situation-dependent transfusion, erythropoietin and tranexamic acid reduces transfusion in fronto-orbital advancement for metopic and coronal craniosynostosis. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2020 May 9; [PubMed PMID: 32388812]
Magoon K,Azzolini A,Yang R,Taylor J, In Situ Hinge Technique for the Frontal Bandeau for the Correction of Metopic Craniosynostosis Reduces Operative Time. The Journal of craniofacial surgery. 2019 Sep; [PubMed PMID: 30896507]
Pellerin P,Vinchon M,Dhellemmes P,Wolber A,Guerreschi P, Trigonocephaly: Lille's surgical technique. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2013 Dec [PubMed PMID: 23900629]
di Rocco F, Gleizal A, Lohkamp L, Szathmari A, Paulus C, Mottolese C. Control of metopic emissary veins in trigonocephaly surgery. Technical note. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2018 Dec:34(12):2481-2484. doi: 10.1007/s00381-018-3928-1. Epub 2018 Jul 27 [PubMed PMID: 30054806]
Bennett KG,Liang F,Ranganathan K,Muraszko KM,Vercler CJ,Buchman SR, Surgical Hypercorrection of Trigonocephaly: Evaluation of Surgical Outcomes. The Journal of craniofacial surgery. 2018 Jan [PubMed PMID: 29068967]
Mathijssen IM, Guideline for Care of Patients With the Diagnoses of Craniosynostosis: Working Group on Craniosynostosis. The Journal of craniofacial surgery. 2015 Sep; [PubMed PMID: 26355968]
Huang MH,Mouradian WE,Cohen SR,Gruss JS, The differential diagnosis of abnormal head shapes: separating craniosynostosis from positional deformities and normal variants. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association. 1998 May; [PubMed PMID: 9603553]
Di Rocco F,Rothenbuhler A,Cormier Daire V,Bacchetta J,Adamsbaum C,Baujat G,Rossi M,Lingart A, Craniosynostosis and metabolic bone disorder. A review. Neuro-Chirurgie. 2019 Nov; [PubMed PMID: 31562881]
Pressler MP,Hallac RR,Geisler EL,Seaward JR,Kane AA, Comparison of Head Shape Outcomes in Metopic Synostosis Using Limited Strip Craniectomy and Open Vault Reconstruction Techniques. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association. 2020 Nov 6; [PubMed PMID: 33153285]
Gabrick KS,Wu RT,Singh A,Persing JA,Alperovich M, Radiographic Severity of Metopic Craniosynostosis Correlates with Long-Term Neurocognitive Outcomes. Plastic and reconstructive surgery. 2020 May; [PubMed PMID: 32332546]
Osborn AJ,Roberts RM,Mathias JL,Anderson PJ,Flapper WJ, Cognitive, behavioral and psychological functioning of children and adults with conservatively managed metopic synostosis. Child neuropsychology : a journal on normal and abnormal development in childhood and adolescence. 2020 Sep 8; [PubMed PMID: 32900282]
Osborn AJ,Roberts RM,Mathias JL,Anderson PJ,Flapper WJ, Cognitive, behavioral and psychological functioning in children with metopic synostosis: a meta-analysis examining the impact of surgical status. Child neuropsychology : a journal on normal and abnormal development in childhood and adolescence. 2019 Feb; [PubMed PMID: 29482450]
Level 1 (high-level) evidenceWes AM,Paliga JT,Goldstein JA,Whitaker LA,Bartlett SP,Taylor JA, An evaluation of complications, revisions, and long-term aesthetic outcomes in nonsyndromic metopic craniosynostosis. Plastic and reconstructive surgery. 2014 Jun; [PubMed PMID: 24867728]
Campbell JW,Albright AL,Losken HW,Biglan AW, Intracranial hypertension after cranial vault decompression for craniosynostosis. Pediatric neurosurgery. 1995; [PubMed PMID: 7547460]
Level 3 (low-level) evidencePollack IF,Losken HW,Biglan AW, Incidence of increased intracranial pressure after early surgical treatment of syndromic craniosynostosis. Pediatric neurosurgery. 1996; [PubMed PMID: 8873162]
Level 2 (mid-level) evidenceCastro-Govea Y,Vela-Martinez A,Treviño-Garcia LA, Volumetric lipoinjection of the fronto-orbital and temporal complex with adipose stem cells for the aesthetic restoration of sequelae of craniosynostosis. Archives of plastic surgery. 2018 Mar; [PubMed PMID: 29566469]
Queiros C,Joly A,Paré A,Listrat A,Travers N,Goga D,Laure B, Use of cutting guides during craniosynostosis sequelae surgery: A comparative study between computer-assisted planning and post-operative results. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2017 Jul [PubMed PMID: 28434829]
Level 2 (mid-level) evidenceKampf S,Micko A,Schwartz E,Schopper C,Reinprecht A, Clinical and aesthetic outcome analysis of a case series of trigonocephaly patients after early fronto-orbital advancement. International journal of oral and maxillofacial surgery. 2020 Sep; [PubMed PMID: 32171618]
Level 2 (mid-level) evidenceYee ST,Fearon JA,Gosain AK,Timbang MR,Papay FA,Doumit G, Classification and Management of Metopic Craniosynostosis. The Journal of craniofacial surgery. 2015 Sep; [PubMed PMID: 26267575]