Introduction
The cornea is a five-layered structure that provides the majority of the total refractive power of the eye (Fig. 1). In the past, penetrating keratoplasty (PK) had been the gold standard surgical treatment of corneal diseases for any layer, including diseases of the endothelium. With the improvement in technology and innovation over the last two decades, endothelial keratoplasty (EK) techniques involving transplantation of corneal components have been deployed to treat these diseases (Table 1). When compared to PK, EK introduces less foreign antigens, has improved visual recovery and outcomes, minimizes astigmatism, has less risk of dehiscence, and results in better globe stability.[1][2][3][4]
History of Endothelial Keratoplasty Techniques
The first endothelial transplant was developed by Dr. Tillett in 1956. The technique required a large incision and used a partial thickness graft created by the trephination of half of the posterior donor cornea.[5] During the 1960s, Dr. Barraquer developed a method of EK using a microkeratome for an anterior approach similar to a laser-assisted in situ keratomileusis (LASIK) flap followed by posterior trephination and suturing of the graft.[6] These techniques were complex, challenging to replicate, and unable to address the issues posed by PK. In 1998, Melles et al. made a significant advancement in the field by dissecting out a posterior stromal pocket using an intrastromal approach and securing the graft with air instead of the typical suturing that produced tension likely to pull the graft out of place.[7][8] Some refinements of this technique were made by Dr. Terry, who coined the term deep lamellar endothelial keratoplasty (DLEK) (Fig. 2A).[9] However, this procedure was technically challenging and not universally adopted.
Next, in 2004, Melles et al. revolutionized the field with what is now called Descemet stripping endothelial keratoplasty (DSEK), after a few modifications made by Price et al.[10] DSEK utilizes a novel technique, "descemetorhexis," via an internal approach to remove the pathologic host Descemet membrane and endothelium. This procedure creates a smooth surface for graft application and removes the source of disease while sparing posterior stroma (Fig. 2B).[11] The use of a microkeratome to remove anterior stroma of the donor cornea was described by Dr. Gorovoy[12] and is now referred to as Descemet stripping automated endothelial keratoplasty (DSAEK). However, DSAEK is commonly referred to as DSEK as well. DSAEK has shown to have better visual outcomes compared to the original DSEK, and the technique continued to be refined, such as the addition of venting incisions in the cornea after graft application enhances graft adherence.[13]
DSAEK had become widely adopted, and eye bank produced precut tissue has proven to be reliable; thus, replacing the need for preparation by surgeons.[14][15][16] A study by Neff et al. found that thinner grafts, specifically those ≤ 131 μm, were associated with improved visual outcomes;[17] although the correlation between graft thickness and clinical outcomes has been disputed.[18][19] Another iteration using thinner grafts with less stroma, Ultrathin DSAEK (UT-DSAEK) developed by Busin et al. in 2013, was shown to have the same or better outcomes with faster recovery and similar complications as DSEK.[20][21] Comparing thicknesses, UT-DSAEK grafts are around 100 μm, whereas DSEK and DSAEK grafts are closer to 200 μm.[22] Melles et al., however, continued to innovate with the development of Descemet membrane endothelial keratoplasty (DMEK).
DMEK uses a graft consisting of endothelium and DM without any stroma (Fig. 2C). The graft is around 10-15 μm in thickness and prepared via a descemetorhexis performed on the donor eye.[22][23] A similar technique, pre-Descemet Endothelial Keratoplasty (PDEK), is prepared using pneumodissection to include the pre-Descemet layer in the graft, which helps with graft handling.[24] Compared to DSAEK, DMEK has better visual outcomes, faster recovery time, and lower immune rejection rate. However, it was not widely adopted due to the increased surgical skill required and higher rates of complications such as graft detachment and the need to rebubble.[25][26] Although short-lived, DMEK technique with a stromal rim (DMEK-S) was an attempt to hybridize the ease of handling inside the eye from DSEAK and retain visual benefits of DMEK developed by Studeny et al. (Fig. 2D).[27] Refinement of DMEK techniques continued, such as the development of pre- and intraoperative manipulations to better identify DMEK graft orientation, use of gas bubble tamponade that decreases chances of detachment, and eye bank technicians becoming proficient at producing preloaded DMEK grafts.[1][28][29][30]
The femtosecond laser has also been used to assist in EK procedures. Femtosecond laser-assisted DSEK (FS-DSEK) has been used to produce successful DSEK grafts consistently. However, a visual improvement from FS-DSEK appears limited when compared to DSAEK or PK.[31][32] Femtosecond and excimer laser-assisted EK (FELEK) uses a Femtosecond laser to dissect a thin graft that is smoothened with excimer photoablation. FELEK has shown some success on a small cohort of patients and may provide similar results to DMEK with less of a learning curve.[33] Femtosecond laser-enabled descemetorhexis DMEK (FE-DMEK) or Femtosecond laser-assisted DMEK (F-DMEK) has been used to perform the descemetorhexis for DMEK, resulting in fewer graft detachments and need for rebubbling when compared to manual descemetorhexis.[34][35][36]
In settings with a scarcity of donor tissue, some modified or newer techniques may offer a solution. Hemi-DMEK and quarter-DMEK are variations involving grafts with smaller, modified shapes prepared by surgeons, and they appear to have similar visual outcomes, although with lower endothelial cell density.[30][37][38] Mini-DMEK is another technique where a graft is shaped and sized to fit a patient's particular endothelial defect. It has been used to treat acute corneal hydrops secondary to keratoconus in a small cohort of patients.[39]
The observation of corneal clearing despite nonattachment of grafts in some cases has led to investigating techniques that do not use transplants, and instead, rely on primary intention healing of the endothelium (Fig. 2E).[40][41] These techniques have been termed Descemetorhexis without endothelial keratoplasty (DWEK) coined by Kaufman et al. or, increasingly becoming the norm, Descemet stripping only (DSO) proposed by Dr. Gorovoy.[40][42] ROCK inhibitors have also been used with DSO to salvage failing cases, speed up the recovery, and improve endothelial cell density in patients with Fuchs endothelial dystrophy.[43][44]
Further comparison studies are warranted, but DSO may provide similar visual outcomes to DMEK after a longer recovery time without the risk of rejection, detachment, or need for immunosuppression.[45] Corneal clearance, despite subtotal detachment of grafts, has also inspired a purposed technique, Descemet membrane endothelial transfer (DMET), involving a focally attached free-floating graft to serve as a source of endothelial cells (Fig. 2F).[46][47] However, retrospective studies of DMEK cases with subtotal detachment do not always have satisfying results[48], and it is not entirely clear whether corneal clearance is due to endothelial cell transfer or simply primary intention healing of host endothelium.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The cornea protects internal structures of the eye and provides 40-44 D of refractive power, which is approximately 70% of total refraction. The layers of the cornea, from anterior to posterior, include the epithelium, Bowman layer, stroma, Descemet membrane, and endothelium (Fig. 1). The epithelium is a protective layer and provides a smooth surface for the tear film-cornea interface that contributes to refractive power. Bowman layer is the most anterior portion of the stroma and assists in maintaining corneal shape. The stroma is the primary refracting medium of the cornea and source of mechanical strength. The stromal collagen fibers are organized in parallel bundles called fibrils that are arranged in layers at right angles to one another called lamellae. The lamellae are highly interlaced anteriorly but become less so posteriorly. This puts the posterior stroma at risk of becoming swollen when hydrated. The cornea is highly innervated with subepithelial and stromal plexuses supplied by the ophthalmic nerve. Descemet membrane is secreted by endothelial cells and serves as an attachment for endothelium to the stroma via numerous hemidesmosomes.[49] Although somewhat controversial, a strong pre-Descemet layer (also referred to as "Dua Layer") has been discovered on the posterior stroma using pneumodissection and may have clinical and surgical significance.[50]
The endothelium is a monolayer of hexagonal cells with extensive lateral interdigitations and incomplete belt of tight junctions. According to the pump-and-leak hypothesis, anterior chamber contents gradually leak into the corneal stroma supplying it with nutrients.[51] The activity of the endothelial cells creates a net flux of ions out of the stroma into the aqueous humor, ensuring the removal of water from the stroma. Dehydration of the stroma is essential for corneal clarity. Endothelial cell density gradually decreases with age. To compensate for cell loss, endothelial cells migrate, increase in size, and lose their hexagonal morphology. Unfortunately, once cell density falls below a 500-700 cell/mm threshold due to aging or disease, the endothelial capacity to pump may become insufficient, and corneal stromal edema will follow. It was believed that endothelial cells do not undergo mitosis in adults. The cells have shown to exhibit contact inhibition, and there is a scarcity of positive growth factors and abundancy of negative growth factors in the anterior chamber. However, ex vivo and in vitro growth of endothelial cells has been demonstrated, and progenitor-like endothelial cells have been identified at the endothelium-trabecular meshwork transition zone.[41][49][52]
Endothelial Diseases
Diseases affecting the corneal endothelium leading to the surgical intervention will be briefly described.
Fuchs Endothelial Corneal Dystrophy (FECD)
FECD is the most common corneal dystrophy. It presents bilaterally in the second to third decade of life, but there is also a rare early-onset subtype. It displays autosomal dominant inheritance, but sporadic cases are most common. The characteristic features of FECD are the formation of excrescences from the Descemet membrane called guttae, loss of corneal endothelial cell density, and progressive corneal edema. The guttae are visible upon slit-lamp examination, and they develop centrally then coalesce and begin appearing peripherally over the years. Evaluating the distribution of guttae serves as the basis for clinical staging. The endothelial cells in FECD have less antioxidant gene expression and more apoptosis-related factors leading to decreased endothelial cell density. The chronic corneal edema that results causes progressive blurry vision and may lead to painful epithelial bullae.[53][54]
Pseudophakic and Aphakic Bullous Keratopathy
This disease is a complication of cataract surgery after an artificial intraocular lens is placed (pseudophakic) or not (aphakic). Incidence is 1-2% of cataract surgeries, and risk factors include advanced age or concurrent endothelial disease. The loss of endothelial cells in this disease is a consequence of surgical trauma such as heat from phacoemulsification or high irrigation and aspiration rates, causing turbulence and rapidly moving lens particles. The loss of endothelial cells results in corneal stromal edema, subepithelial bullae, tearing, decreased vision, and pain.[55]
Iridocorneal Endothelial Syndrome (ICE)
ICE is a rare syndrome made up of three clinical variants that include Chandler syndrome, progressive essential iris atrophy, and Cogan-Reese syndrome. Common to all variants is the pathologic proliferation of corneal endothelial cells that migrate to the iridocorneal angle and iris, possibly due to a viral trigger. Pathognomonic to ICE syndrome are endothelial "ICE cells" that have a dark-light reversed pattern on specular microscopy found in areas of the cornea with a hammered silver appearance. Hallmarks of the disease include irregular endothelium structure, blockage of the iridocorneal angle, and iris abnormalities (e.g., atrophy, corectopia, or polycoria). These changes lead to secondary glaucoma and corneal edema and decompensation.[56][57]
Posterior Polymorphous Dystrophy (PPCD):
PPCD is a rare, autosomal-dominant, bilateral disease affecting the Descemet membrane and corneal endothelium. This disease has variable expressivity, and presentations range from asymptomatic irregularities of the endothelium to symptomatic corneal edema or glaucoma. It typically presents asymptomatically in the first decade of life then progresses at varying rates. Findings on specular microscopy include asymmetric patches of geographic gray hazy lesions, grouped vesicles, and broad bands with scalloped margins as well as stratified epithelium-like endothelium. Other common findings are anterior synechiae and glaucoma.[58][59]
Congenital Hereditary Endothelial Dystrophy (CHED):
CHED is a rare inherited disease affecting the corneal endothelium characterized by ground glass-like corneal opacification due to endothelium failure and corneal edema as well as and nystagmus. It presents at or shortly after birth. Two genetic forms exist, namely, CHED1, which is autosomal dominant, and CHED2, which is autosomal recessive. CHED2 is more common than CHED1 and share similarities with PPCD, e.g., similar specular microscopy findings.[58][59]
Indications
Patients with endothelial dysfunction and visual disability are appropriate candidates. Fuchs endothelial corneal dystrophy, aphakic or pseudophakic bullous keratopathy, and previous penetrating or endothelial graft failures are the most common indications. Less common indications include endothelial failure secondary to trauma, iridocorneal endothelial syndrome, posterior polymorphous dystrophy, and congenital hereditary endothelial dysfunction.[1][60] DMEK has also been used to salvage a failed PK with better visual outcomes and similar four-year survival as repeat PK and DSEK.[26][61]
Contraindications
In extensive disease resulting in full-thickness stromal scarring such as advanced bullous keratopathy, a PK may be more appropriate. The stromal scaring and opacities lead to failure to improve patient vision as well as limit the surgeon's view.[26] Some relative contraindications for DMEK include cases where patients have glaucoma tubes, aphakia, or iris defects because the thin grafts may be lost; therefore, DSAEK or a hybrid DMEK may be preferred.[60] Ocular pressurization may be necessary for graft attachment, so pre-phthisic or hypotonic eyes are contraindicated to avoid the progression of bulbar atrophy.[26]
Equipment
Along with basic ophthalmologic operating room equipment, a microkeratome may be required depending on the technique. Donor tissue used for DSEK and DMEK may be prepared by the surgeon, usually on the day of surgery or obtained from an eye bank. Glide or mechanical injection devices for the insertion of grafts will be needed for DSEK. An intraocular lens injector may be used for DMEK graft insertion. A viscoelastic substance or air injection may be used for better visualization, and anterior chamber irrigation may be used to maintain anterior chamber depth.
Personnel
These procedures need an anesthesiologist, circulating nurse, scrub tech, assistant, and operating ophthalmologist who is comfortable with performing the complicated techniques that may be required.
Preparation
If the surgeon prepares the DSEK graft, it may be obtained manually or by using a microkeratome and special techniques (DSAEK/UT-DSAEK), which produce smoother, thinner grafts with better outcomes.[12][20] If the surgeon is preparing the DMEK graft, the tissue may be collected by scoring and peeling it off the posterior cornea or using pneumodissection at the cost of a smaller graft size and more endothelial cell loss. Pneumodissection may also be used to retain the pre-Descemet layer (PDEK), allowing for easier handling.[1][24][62][63] Grafts collected from diabetic donors are associated with graft failure and should be used with caution or avoided.[64][65] Other risk factors associated with decreased graft survival in DSEAK include previous glaucoma surgery and a history of previous graft rejection.[66]
If patients are concurrently suffering from lens opacities, cataract extraction, and intraocular lens insertion may be combined with the DSEK or DMEK as a single-stage "triple procedure" without increasing complication risk.[67][68] However, DSEK and DMEK increase the risk of early cataract development in phakic patients, especially those over 50 years of age.[69][70] A discussion over the risks and benefits of combined endothelial and cataract procedures in older patients with clear lenses is warranted.
Technique or Treatment
Deep Lamellar Endothelial Keratoplasty (DELK)
A 9.0-mm incision is created in the sclera 1.0-mm peripheral to the superior limbus, and viscoelastic is injected. The creation of a deep lamellar pocket is a challenging task and is developed over the entire area under the cornea using a series of curved blades, a specialized trephination device, and scissors. A similar method is used to collect the graft from trephined donor tissue. The viscoelastic is removed, the air is injected into the patient's anterior chamber, and the disk of donor tissue is introduced into the endothelium side with a viscoelastic coated spatula and adhered to the cornea.[9]
Descemet Stripping Endothelial Automated Keratoplasty (DSAEK)
A 3-5 mm incision is created in the cornea/sclera or limbus. A descemetorhexis is performed to remove the pathologic Descemet membrane and endothelium using a reverse Sinskey hook and forceps. Injected the anterior chamber with viscoelastic or air may improve visualization.[11][13] The introduction of the graft into the eye is accomplished in several ways. Originally, forceps were used to pull the graft that was folded in a "tri-fold" or "taco" configuration with the endothelium on the inside. Traumatic cell loss is an issue with DSEK graft insertion, especially in patients with shallow anterior chambers and particularly in Asian patients, which may lead to primary graft failure.[13][71] To address this, several specialized insertion devices have been developed.[72] Glide devices, such as the Busin glide, fold the graft as it is pulled or pushed into the anterior chamber and allow for equal unfolding, which minimizes the risk of the graft flipping.[73][74] Mechanical injection devices are also used and may be preloaded with grafts prepared by eye bank technicians, and these closed systems do have the same backflow from irrigation as glides.[16][72] An air bubble is used to adhere the graft to the cornea; then, after 10-30 min, a balanced salt solution is used to partially replace the air to help prevent pupil block.[1]
Descemet Membrane Endothelial Keratoplasty (DMEK)
Incision and descemetorhexis as in DSEK are performed; however, the thinner graft means a smooth surface on the recipient eye is essential. The donor tissue will spontaneously curl with endothelium facing out, and staining the tissue with trypan blue may help improve visualization of the graft. The graft is preloaded in an intraocular lens injector and flushed to insert into the eye.[29] Insertion and unrolling of the graft are achieved with bursts of balanced salt solution or air and tapping the peripheral cornea followed by adherence of the graft with an air bubble.[25][75] The graft must be oriented with endothelium facing down and toward the anterior chamber. To ensure this, several techniques to evaluate orientation include intraoperative slit-lamp, optical coherence tomography (OCT), and real-time ultrasound biomicroscopy or by marking one face with stamping or staining before insertion.[28][76][77][78][79] Air removal 30 min to 2h later or inferior peripheral iridotomy prior to insertion is done to help prevent pupil block.[1][80]
Descemet Stripping Only (DSO)
This procedure only involves a descemetorhexis, which is performed similarly to DSEK and DMEK. Preoperatively, the pupil may be dilated for a better red reflex and visualization of the Descemet membrane. Rho-associated kinase inhibitors may play a role in postoperative recovery and improvement of endothelial cell density.[40]
Complications
Graft Detachment
The most common early post-op complication in DSAEK and DMEK is graft detachment. DSEK graft detachments often resolve spontaneously, and rebubbling is reserved for complete detachments. Strategies to prevent DSEK detachment include ensuring the recipient site as larger or greater than graft size, counseling patients to avoid eye rubbing, using a long-acting gas (20% sulfur hexafluoride) bubble tamponade, and using intraoperative OCT to appreciate fluid in the graft-host interface that may be massaged out or drained via venting incisions.[1][13][81]
The incidence of DMEK detachment varies, but some reports rate it as high as 74%. DMEK detachment is less likely to resolve spontaneously due to the graft's tendency to roll up. Detachments of the central cornea or involving more than one-third of the graft may require rebubbling, which is often successful but may result in a decreased endothelial cell density. If there is total detachment or the graft has rolled up, the patient may need regrafting.[1][26][82]
Primary Graft Failure
Primary graft failure is defined as the lack of improvement of corneal edema requiring regrafting. Primary graft failure may be attributed, in part, to the quality of donor tissue; however, the complexity of these techniques and potential for graft trauma may mean a surgeon's skill is a significant factor. The difference in surgeon familiarity and skill with these procedures may cause a "center effect" seen when comparing graft failure rates by low volume surgeons in the midst of a learning curve versus those performed at high-volume transplant centers.[83] After overcoming an apparent learning curve, the rate of rebubbling and regrafting is similar between DSEK and DMEK along with improved survival of DMEK grafts.[84][85] A 2018 report by the American Academy of Ophthalmology reviewing the safety and outcomes of DMEK and DSEK in the literature found that the primary graft failure rate for DMEK ranges from 0-12.5% with a mean of 1.7% and ranges from 0-29% with a mean of 5% for DSEK.[84]
Pupillary Block and Increasing IOP
Pupillary block by air may lead to serious glaucomatous damage to the eye. This risk is highest in DMEK as more air is used, and the associated risk is greater still with DMEK triple procedures. It should be suspected if there is increasing intraocular pressure (IOP), obscured iridotomy, or presence of pain or loss of vision. Prevention of pupillary block includes peripheral iridotomy and removal of some air to avoid complete filling of the anterior chamber after graft adhesion.[26][80] Post-keratoplasty glaucoma and increasing IOP is another common complication after DSEK and DMEK that is usually due to steroid responsiveness. Risk factors include a previous diagnosis of glaucoma or elevated IOP, and treatment may include tapering the steroid dose.[86][87]
Rejection
The presentation of immune rejection in DSEK is more subtle than after PK and often diagnosed incidentally. A study by Price et al. found that 35% of diagnosed patients were asymptomatic. Signs include diffuse or focal precipitates on slit-lamp examination, corneal edema, anterior chamber cells, and rarely Khodadoust Line. The risk of rejection is higher for African Americans, preexisting glaucoma, and steroid responders. A retrospective analysis by Price et al. found in 1312 DSEK cases for FECD, there was a 5-year rejection rate of 7.9%. DSEK rejection is typically treated with tapering doses of topical steroids.[88][89][90] Of note, a case of an autologous DSEK procedure was used to treat a patient with previous endothelial graft rejection.[91]
DMEK rejection is diagnosed by the presence of retrocorneal precipitates on the graft on the slit-lamp examination. A retrospective analysis of 905 eyes found a very low rejection incidence of 2.4% over four years. Local steroid therapy resolves most cases, and some authors recommend prophylactic topical steroid therapy for the first 1-2 years postoperatively.[90][92]
Intraoperative Hyphema
Intraoperative hyphema may occur with DMEK, and this risk was shown to be higher in cases with combined cataract surgery. However, hyphema was not shown to significantly affect endothelium cell loss, visual acuity outcomes, or rebubbling rates.[93]
Clinical Significance
Meta-analyses of retrospective studies comparing DMEK and DSAEK have found that DMEK provided better visual outcomes and patient satisfaction but with increased, easily treated complications.[94][95][96] A randomized trial comparing visual outcomes of UT-DSAEK and DMEK in 50 eyes from 38 patients found that DMEK provided better visual acuity at 3, 6, and 12 months with similar complication rates although with less average endothelial cell counts.[22]
Further investigation to explain this difference in visual acuity compared to corneal haze and light scatter produced by DMEK and DSAEK had found no difference. One potential explanation may be the greater amount of higher-order aberrations in the posterior cornea after UT-DSAEK.[97] The mean 5-year graft survival and endothelial cell loss between DSAEK and DMEK are similar. Reports of DMEK 5-year survival range from 90 to 96% and 85 to 96% for DSAEK procedures.[66][89][98][99] Previous glaucoma surgery (tube-shunt or trabeculectomy) were associated with poorer DSAEK 5-year survival.[66]
Endothelial keratoplasty is, in many ways, better treatment for many cases of endothelial disease when compared to PK. Still, the question now is which of the multitude of techniques is best for patients. Most large random randomized control trials in the literature focus on DSEAK versus DMEK techniques and many studies are usually limited to the treatment of FECD or pseudophakic bullous keratopathy. As techniques are developed, standardized, and adopted, large randomized studies comparing the various surgeries with different diseases are needed to fully elucidate how to achieve the best, cost-effective outcomes for patients. It is in the patients' best interest for surgeons to seek mentorship and adequately prepare for new techniques before adopting them since the learning curve for more complex procedures may be steep.[100]
Enhancing Healthcare Team Outcomes
EK procedures have the potential to significantly improve patients' visual outcomes while avoiding the complications associated with previous techniques. Rapid development has led to a variety of techniques that may be more appropriate than others in particular situations, so healthcare teams need to refer and treat appropriate candidates with procedures that are suited to a surgeon's skills and patients' particular risk factors. The healthcare team should also be aware of the potential complications that need to be prevented, monitored, and treated should they occur.
Media
(Click Image to Enlarge)
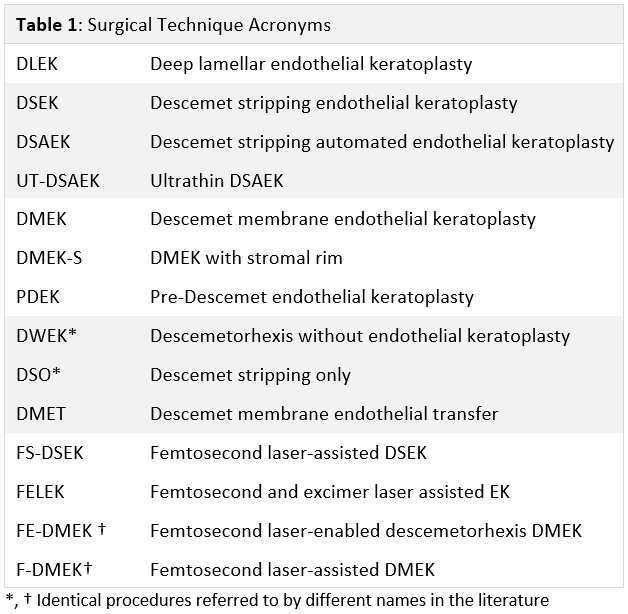
Table 1: Surgical Technique Acronyms Courtesy of Moshirfar & Thomson
(Click Image to Enlarge)
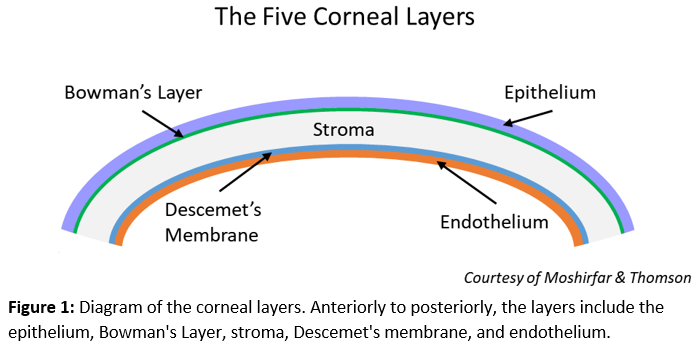
Figure 1: Diagram of corneal layers Illustrated by Andrew Thomson
(Click Image to Enlarge)
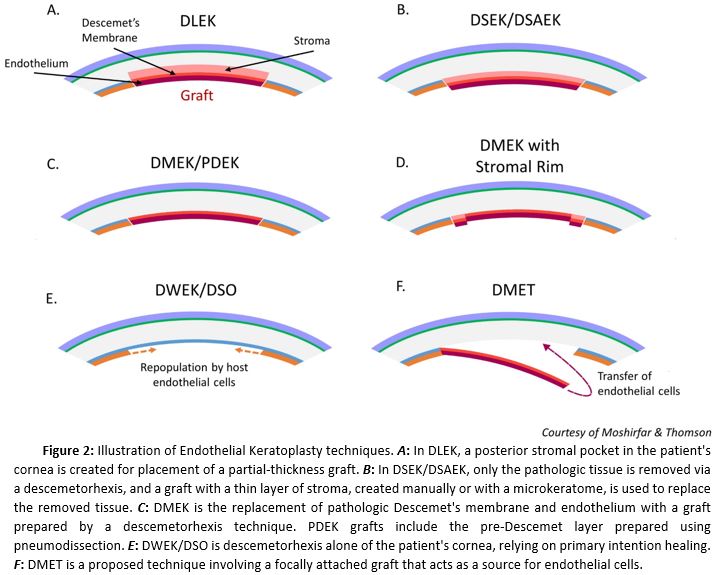
Figure 2: Illustration of Endothelial Keratoplasty Techniques Illustrated by Andrew Thomson
References
Price MO, Gupta P, Lass J, Price FW Jr. EK (DLEK, DSEK, DMEK): New Frontier in Cornea Surgery. Annual review of vision science. 2017 Sep 15:3():69-90. doi: 10.1146/annurev-vision-102016-061400. Epub 2017 Jul 11 [PubMed PMID: 28697678]
Güell JL, El Husseiny MA, Manero F, Gris O, Elies D. Historical Review and Update of Surgical Treatment for Corneal Endothelial Diseases. Ophthalmology and therapy. 2014 Dec:3(1-2):1-15. doi: 10.1007/s40123-014-0022-y. Epub 2014 Feb 18 [PubMed PMID: 25134494]
Moshirfar M, Ding Y, Shah TJ. A Historical Perspective on Treatment of Fuchs' Endothelial Dystrophy: We have Come a Long Way. Journal of ophthalmic & vision research. 2018 Jul-Sep:13(3):339-343. doi: 10.4103/jovr.jovr_94_18. Epub [PubMed PMID: 30090191]
Level 3 (low-level) evidenceZhang J, Patel DV, McGhee CNJ. The Rapid Transformation of Transplantation for Corneal Endothelial Diseases: An Evolution From Penetrating to Lamellar to Cellular Transplants. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2019 Nov-Dec:8(6):441-447. doi: 10.1097/APO.0000000000000265. Epub [PubMed PMID: 31789646]
TILLETT CW. Posterior lamellar keratoplasty. American journal of ophthalmology. 1956 Mar:41(3):530-3 [PubMed PMID: 13302358]
Barraquer JI. Lamellar keratoplasty. (Special techniques). Annals of ophthalmology. 1972 Jun:4(6):437-69 [PubMed PMID: 4555325]
Melles GR,Eggink FA,Lander F,Pels E,Rietveld FJ,Beekhuis WH,Binder PS, A surgical technique for posterior lamellar keratoplasty. Cornea. 1998 Nov; [PubMed PMID: 9820943]
Level 3 (low-level) evidenceMelles GR, Lander F, van Dooren BT, Pels E, Beekhuis WH. Preliminary clinical results of posterior lamellar keratoplasty through a sclerocorneal pocket incision. Ophthalmology. 2000 Oct:107(10):1850-6; discussion 1857 [PubMed PMID: 11013184]
Level 2 (mid-level) evidenceTerry MA, Ousley PJ. Deep lamellar endothelial keratoplasty in the first United States patients: early clinical results. Cornea. 2001 Apr:20(3):239-43 [PubMed PMID: 11322409]
Price FW Jr, Price MO. Descemet's stripping with endothelial keratoplasty in 50 eyes: a refractive neutral corneal transplant. Journal of refractive surgery (Thorofare, N.J. : 1995). 2005 Jul-Aug:21(4):339-45 [PubMed PMID: 16128330]
Level 2 (mid-level) evidenceMelles GR, Wijdh RH, Nieuwendaal CP. A technique to excise the descemet membrane from a recipient cornea (descemetorhexis). Cornea. 2004 Apr:23(3):286-8 [PubMed PMID: 15084862]
Gorovoy MS. Descemet-stripping automated endothelial keratoplasty. Cornea. 2006 Sep:25(8):886-9 [PubMed PMID: 17102661]
Level 2 (mid-level) evidencePrice FW Jr, Price MO. Descemet's stripping with endothelial keratoplasty in 200 eyes: Early challenges and techniques to enhance donor adherence. Journal of cataract and refractive surgery. 2006 Mar:32(3):411-8 [PubMed PMID: 16631048]
Level 2 (mid-level) evidencePrice MO, Baig KM, Brubaker JW, Price FW Jr. Randomized, prospective comparison of precut vs surgeon-dissected grafts for descemet stripping automated endothelial keratoplasty. American journal of ophthalmology. 2008 Jul:146(1):36-41. doi: 10.1016/j.ajo.2008.02.024. Epub 2008 Apr 24 [PubMed PMID: 18439566]
Level 1 (high-level) evidenceRose L, Briceño CA, Stark WJ, Gloria DG, Jun AS. Assessment of eye bank-prepared posterior lamellar corneal tissue for endothelial keratoplasty. Ophthalmology. 2008 Feb:115(2):279-86 [PubMed PMID: 17599413]
Level 2 (mid-level) evidencePalioura S, Colby K. Outcomes of Descemet Stripping Endothelial Keratoplasty Using Eye Bank-Prepared Preloaded Grafts. Cornea. 2017 Jan:36(1):21-25 [PubMed PMID: 27741016]
Neff KD, Biber JM, Holland EJ. Comparison of central corneal graft thickness to visual acuity outcomes in endothelial keratoplasty. Cornea. 2011 Apr:30(4):388-91. doi: 10.1097/ICO.0b013e3181f236c6. Epub [PubMed PMID: 21045647]
Level 2 (mid-level) evidenceShinton AJ, Tsatsos M, Konstantopoulos A, Goverdhan S, Elsahn AF, Anderson DF, Hossain P. Impact of graft thickness on visual acuity after Descemet's stripping endothelial keratoplasty. The British journal of ophthalmology. 2012 Feb:96(2):246-9. doi: 10.1136/bjophthalmol-2011-300462. Epub 2011 Oct 25 [PubMed PMID: 22028474]
Level 2 (mid-level) evidenceFeizi S, Javadi MA. Effect of Donor Graft Thickness on Clinical Outcomes after Descemet Stripping Automated Endothelial Keratoplasty. Journal of ophthalmic & vision research. 2019 Jan-Mar:14(1):18-26. doi: 10.4103/jovr.jovr_55_17. Epub [PubMed PMID: 30820282]
Level 2 (mid-level) evidenceBusin M, Madi S, Santorum P, Scorcia V, Beltz J. Ultrathin descemet's stripping automated endothelial keratoplasty with the microkeratome double-pass technique: two-year outcomes. Ophthalmology. 2013 Jun:120(6):1186-94. doi: 10.1016/j.ophtha.2012.11.030. Epub 2013 Mar 1 [PubMed PMID: 23466268]
Dickman MM, Kruit PJ, Remeijer L, van Rooij J, Van der Lelij A, Wijdh RH, van den Biggelaar FJ, Berendschot TT, Nuijts RM. A Randomized Multicenter Clinical Trial of Ultrathin Descemet Stripping Automated Endothelial Keratoplasty (DSAEK) versus DSAEK. Ophthalmology. 2016 Nov:123(11):2276-2284. doi: 10.1016/j.ophtha.2016.07.036. Epub [PubMed PMID: 27659544]
Level 1 (high-level) evidenceChamberlain W, Lin CC, Austin A, Schubach N, Clover J, McLeod SD, Porco TC, Lietman TM, Rose-Nussbaumer J. Descemet Endothelial Thickness Comparison Trial: A Randomized Trial Comparing Ultrathin Descemet Stripping Automated Endothelial Keratoplasty with Descemet Membrane Endothelial Keratoplasty. Ophthalmology. 2019 Jan:126(1):19-26. doi: 10.1016/j.ophtha.2018.05.019. Epub 2018 Jun 23 [PubMed PMID: 29945801]
Level 1 (high-level) evidenceMelles GR, Ong TS, Ververs B, van der Wees J. Preliminary clinical results of Descemet membrane endothelial keratoplasty. American journal of ophthalmology. 2008 Feb:145(2):222-227 [PubMed PMID: 18061137]
Agarwal A, Dua HS, Narang P, Kumar DA, Agarwal A, Jacob S, Agarwal A, Gupta A. Pre-Descemet's endothelial keratoplasty (PDEK). The British journal of ophthalmology. 2014 Sep:98(9):1181-5. doi: 10.1136/bjophthalmol-2013-304639. Epub 2014 Mar 21 [PubMed PMID: 24659352]
Price MO, Giebel AW, Fairchild KM, Price FW Jr. Descemet's membrane endothelial keratoplasty: prospective multicenter study of visual and refractive outcomes and endothelial survival. Ophthalmology. 2009 Dec:116(12):2361-8. doi: 10.1016/j.ophtha.2009.07.010. Epub 2009 Oct 28 [PubMed PMID: 19875170]
Level 2 (mid-level) evidenceTrindade BLC, Eliazar GC. Descemet membrane endothelial keratoplasty (DMEK): an update on safety, efficacy and patient selection. Clinical ophthalmology (Auckland, N.Z.). 2019:13():1549-1557. doi: 10.2147/OPTH.S178473. Epub 2019 Aug 16 [PubMed PMID: 31496646]
Studeny P, Farkas A, Vokrojova M, Liskova P, Jirsova K. Descemet membrane endothelial keratoplasty with a stromal rim (DMEK-S). The British journal of ophthalmology. 2010 Jul:94(7):909-14. doi: 10.1136/bjo.2009.165134. Epub 2009 Oct 22 [PubMed PMID: 19850580]
Level 2 (mid-level) evidenceVeldman PB, Dye PK, Holiman JD, Mayko ZM, Sáles CS, Straiko MD, Galloway JD, Terry MA. The S-stamp in Descemet Membrane Endothelial Keratoplasty Safely Eliminates Upside-down Graft Implantation. Ophthalmology. 2016 Jan:123(1):161-4. doi: 10.1016/j.ophtha.2015.08.044. Epub 2015 Oct 4 [PubMed PMID: 26439215]
Parekh M, Ruzza A, Ferrari S, Busin M, Ponzin D. Preloaded Tissues for Descemet Membrane Endothelial Keratoplasty. American journal of ophthalmology. 2016 Jun:166():120-125. doi: 10.1016/j.ajo.2016.03.048. Epub 2016 Apr 8 [PubMed PMID: 27066719]
Godinho JV, Mian SI. Update on Descemet membrane endothelial keratoplasty. Current opinion in ophthalmology. 2019 Jul:30(4):271-274. doi: 10.1097/ICU.0000000000000577. Epub [PubMed PMID: 31045882]
Level 3 (low-level) evidenceCheng YY, van den Berg TJ, Schouten JS, Pels E, Wijdh RJ, van Cleynenbreugel H, Eggink CA, Rijneveld WJ, Nuijts RM. Quality of vision after femtosecond laser-assisted descemet stripping endothelial keratoplasty and penetrating keratoplasty: a randomized, multicenter clinical trial. American journal of ophthalmology. 2011 Oct:152(4):556-566.e1. doi: 10.1016/j.ajo.2011.03.012. Epub 2011 Jun 17 [PubMed PMID: 21683332]
Level 1 (high-level) evidenceChen H, Tian L, Le Q, Zhao F, Zhao Y, Chen Y, Yang Y, Hong J, Xu J. Femtosecond laser-assisted Descemet's stripping endothelial keratoplasty: a prospective study of 6-month visual outcomes, corneal thickness and endothelial cell loss. International ophthalmology. 2020 Aug:40(8):2065-2075. doi: 10.1007/s10792-020-01383-8. Epub 2020 Apr 21 [PubMed PMID: 32318937]
Trinh L, Saubaméa B, Auclin F, Denoyer A, Lai-Kuen R, El Hamdaoui M, Labbé A, Despiau MC, Brignole-Baudouin F, Baudouin C. Femtosecond and excimer laser-assisted endothelial keratoplasty (FELEK): a new technique of endothelial transplantation. Journal francais d'ophtalmologie. 2014 Mar:37(3):211-9. doi: 10.1016/j.jfo.2013.07.009. Epub 2014 Feb 18 [PubMed PMID: 24559515]
Einan-Lifshitz A, Sorkin N, Boutin T, Showail M, Borovik A, Alobthani M, Chan CC, Rootman DS. Comparison of Femtosecond Laser-Enabled Descemetorhexis and Manual Descemetorhexis in Descemet Membrane Endothelial Keratoplasty. Cornea. 2017 Jul:36(7):767-770. doi: 10.1097/ICO.0000000000001217. Epub [PubMed PMID: 28594697]
Pilger D, von Sonnleithner C, Bertelmann E, Maier AB, Joussen AM, Torun N. Exploring the precision of femtosecond laser-assisted descemetorhexis in Descemet membrane endothelial keratoplasty. BMJ open ophthalmology. 2018:3(1):e000148. doi: 10.1136/bmjophth-2018-000148. Epub 2018 Dec 27 [PubMed PMID: 30687781]
Sorkin N, Mednick Z, Einan-Lifshitz A, Trinh T, Santaella G, Telli A, Chan CC, Rootman DS. Three-Year Outcome Comparison Between Femtosecond Laser-Assisted and Manual Descemet Membrane Endothelial Keratoplasty. Cornea. 2019 Jul:38(7):812-816. doi: 10.1097/ICO.0000000000001956. Epub [PubMed PMID: 30973405]
Gerber-Hollbach N, Parker J, Baydoun L, Liarakos VS, Ham L, Dapena I, Melles GR. Preliminary outcome of hemi-Descemet membrane endothelial keratoplasty for Fuchs endothelial dystrophy. The British journal of ophthalmology. 2016 Nov:100(11):1564-1568. doi: 10.1136/bjophthalmol-2015-307783. Epub 2016 Feb 2 [PubMed PMID: 26837507]
Birbal RS, Ni Dhubhghaill S, Baydoun L, Ham L, Bourgonje VJA, Dapena I, Oellerich S, Melles GRJ. Quarter-Descemet Membrane Endothelial Keratoplasty: One- to Two-Year Clinical Outcomes. Cornea. 2020 Mar:39(3):277-282. doi: 10.1097/ICO.0000000000002127. Epub [PubMed PMID: 31490274]
Level 2 (mid-level) evidenceBachmann B, Händel A, Siebelmann S, Matthaei M, Cursiefen C. Mini-Descemet Membrane Endothelial Keratoplasty for the Early Treatment of Acute Corneal Hydrops in Keratoconus. Cornea. 2019 Aug:38(8):1043-1048. doi: 10.1097/ICO.0000000000002001. Epub [PubMed PMID: 31276462]
Garcerant D, Hirnschall N, Toalster N, Zhu M, Wen L, Moloney G. Descemet's stripping without endothelial keratoplasty. Current opinion in ophthalmology. 2019 Jul:30(4):275-285. doi: 10.1097/ICU.0000000000000579. Epub [PubMed PMID: 31033737]
Level 3 (low-level) evidenceVan den Bogerd B, Dhubhghaill SN, Koppen C, Tassignon MJ, Zakaria N. A review of the evidence for in vivo corneal endothelial regeneration. Survey of ophthalmology. 2018 Mar-Apr:63(2):149-165. doi: 10.1016/j.survophthal.2017.07.004. Epub 2017 Aug 4 [PubMed PMID: 28782549]
Level 3 (low-level) evidenceKaufman AR, Nosé RM, Pineda R 2nd. Descemetorhexis Without Endothelial Keratoplasty (DWEK): Proposal for Nomenclature Standardization. Cornea. 2018 Apr:37(4):e20-e21. doi: 10.1097/ICO.0000000000001528. Epub [PubMed PMID: 29384812]
Macsai MS, Shiloach M. Use of Topical Rho Kinase Inhibitors in the Treatment of Fuchs Dystrophy After Descemet Stripping Only. Cornea. 2019 May:38(5):529-534. doi: 10.1097/ICO.0000000000001883. Epub [PubMed PMID: 30720541]
Moloney G,Petsoglou C,Ball M,Kerdraon Y,Höllhumer R,Spiteri N,Beheregaray S,Hampson J,DʼSouza M,Devasahayam RN, Descemetorhexis Without Grafting for Fuchs Endothelial Dystrophy-Supplementation With Topical Ripasudil. Cornea. 2017 Jun; [PubMed PMID: 28476048]
Huang MJ, Kane S, Dhaliwal DK. Descemetorhexis Without Endothelial Keratoplasty Versus DMEK for Treatment of Fuchs Endothelial Corneal Dystrophy. Cornea. 2018 Dec:37(12):1479-1483. doi: 10.1097/ICO.0000000000001742. Epub [PubMed PMID: 30222714]
Dirisamer M, Yeh RY, van Dijk K, Ham L, Dapena I, Melles GR. Recipient endothelium may relate to corneal clearance in descemet membrane endothelial transfer. American journal of ophthalmology. 2012 Aug:154(2):290-296.e1. doi: 10.1016/j.ajo.2012.02.032. Epub 2012 May 23 [PubMed PMID: 22633346]
Dirisamer M, Ham L, Dapena I, van Dijk K, Melles GR. Descemet membrane endothelial transfer: "free-floating" donor Descemet implantation as a potential alternative to "keratoplasty". Cornea. 2012 Feb:31(2):194-7. doi: 10.1097/ICO.0b013e31821c9afc. Epub [PubMed PMID: 22146548]
Level 3 (low-level) evidenceBirbal RS, Parker J, Dirisamer M, Janićijević A, Baydoun L, Dapena I, Melles GRJ. Descemet Membrane Endothelial Transfer: Ultimate Outcome. Cornea. 2018 Feb:37(2):141-144. doi: 10.1097/ICO.0000000000001395. Epub [PubMed PMID: 28968295]
Sridhar MS. Anatomy of cornea and ocular surface. Indian journal of ophthalmology. 2018 Feb:66(2):190-194. doi: 10.4103/ijo.IJO_646_17. Epub [PubMed PMID: 29380756]
Dua HS, Faraj LA, Said DG, Gray T, Lowe J. Human corneal anatomy redefined: a novel pre-Descemet's layer (Dua's layer). Ophthalmology. 2013 Sep:120(9):1778-85. doi: 10.1016/j.ophtha.2013.01.018. Epub 2013 May 25 [PubMed PMID: 23714320]
Barry PA, Petroll WM, Andrews PM, Cavanagh HD, Jester JV. The spatial organization of corneal endothelial cytoskeletal proteins and their relationship to the apical junctional complex. Investigative ophthalmology & visual science. 1995 May:36(6):1115-24 [PubMed PMID: 7730021]
Level 3 (low-level) evidenceBourne WM. Biology of the corneal endothelium in health and disease. Eye (London, England). 2003 Nov:17(8):912-8 [PubMed PMID: 14631396]
Vedana G, Villarreal G Jr, Jun AS. Fuchs endothelial corneal dystrophy: current perspectives. Clinical ophthalmology (Auckland, N.Z.). 2016:10():321-30. doi: 10.2147/OPTH.S83467. Epub 2016 Feb 18 [PubMed PMID: 26937169]
Level 3 (low-level) evidenceEghrari AO, Riazuddin SA, Gottsch JD. Fuchs Corneal Dystrophy. Progress in molecular biology and translational science. 2015:134():79-97. doi: 10.1016/bs.pmbts.2015.04.005. Epub 2015 Jul 15 [PubMed PMID: 26310151]
Pricopie S, Istrate S, Voinea L, Leasu C, Paun V, Radu C. Pseudophakic bullous keratopathy. Romanian journal of ophthalmology. 2017 Apr-Jun:61(2):90-94 [PubMed PMID: 29450379]
Walkden A, Au L. Iridocorneal endothelial syndrome: clinical perspectives. Clinical ophthalmology (Auckland, N.Z.). 2018:12():657-664. doi: 10.2147/OPTH.S143132. Epub 2018 Apr 9 [PubMed PMID: 29670326]
Level 3 (low-level) evidenceSilva L, Najafi A, Suwan Y, Teekhasaenee C, Ritch R. The iridocorneal endothelial syndrome. Survey of ophthalmology. 2018 Sep-Oct:63(5):665-676. doi: 10.1016/j.survophthal.2018.01.001. Epub 2018 Jan 11 [PubMed PMID: 29331589]
Level 3 (low-level) evidenceLin ZN, Chen J, Cui HP. Characteristics of corneal dystrophies: a review from clinical, histological and genetic perspectives. International journal of ophthalmology. 2016:9(6):904-13. doi: 10.18240/ijo.2016.06.20. Epub 2016 Jun 18 [PubMed PMID: 27366696]
Level 3 (low-level) evidenceFeizi S. Corneal endothelial cell dysfunction: etiologies and management. Therapeutic advances in ophthalmology. 2018 Jan-Dec:10():2515841418815802. doi: 10.1177/2515841418815802. Epub 2018 Dec 7 [PubMed PMID: 30560230]
Level 3 (low-level) evidencePle-Plakon PA,Shtein RM, Trends in corneal transplantation: indications and techniques. Current opinion in ophthalmology. 2014 Jul; [PubMed PMID: 24865170]
Level 3 (low-level) evidencePasari A, Price MO, Feng MT, Price FW Jr. Descemet Membrane Endothelial Keratoplasty for Failed Penetrating Keratoplasty: Visual Outcomes and Graft Survival. Cornea. 2019 Feb:38(2):151-156. doi: 10.1097/ICO.0000000000001763. Epub [PubMed PMID: 30222720]
Tenkman LR, Price FW, Price MO. Descemet membrane endothelial keratoplasty donor preparation: navigating challenges and improving efficiency. Cornea. 2014 Mar:33(3):319-25. doi: 10.1097/ICO.0000000000000045. Epub [PubMed PMID: 24452215]
Altaan SL, Gupta A, Sidney LE, Elalfy MS, Agarwal A, Dua HS. Endothelial cell loss following tissue harvesting by pneumodissection for endothelial keratoplasty: an ex vivo study. The British journal of ophthalmology. 2015 May:99(5):710-3. doi: 10.1136/bjophthalmol-2014-306560. Epub 2015 Mar 4 [PubMed PMID: 25740808]
Greiner MA,Rixen JJ,Wagoner MD,Schmidt GA,Stoeger CG,Straiko MD,Zimmerman MB,Kitzmann AS,Goins KM, Diabetes mellitus increases risk of unsuccessful graft preparation in Descemet membrane endothelial keratoplasty: a multicenter study. Cornea. 2014 Nov; [PubMed PMID: 25222000]
Level 2 (mid-level) evidenceTerry MA, Aldave AJ, Szczotka-Flynn LB, Liang W, Ayala AR, Maguire MG, Croasdale C, Daoud YJ, Dunn SP, Hoover CK, Macsai MS, Mauger TF, Pramanik S, Rosenwasser GOD, Rose-Nussbaumer J, Stulting RD, Sugar A, Tu EY, Verdier DD, Yoo SH, Lass JH, Cornea Preservation Time Study Group. Donor, Recipient, and Operative Factors Associated with Graft Success in the Cornea Preservation Time Study. Ophthalmology. 2018 Nov:125(11):1700-1709. doi: 10.1016/j.ophtha.2018.08.002. Epub 2018 Aug 9 [PubMed PMID: 30098353]
Wakimasu K, Kitazawa K, Kayukawa K, Yokota I, Inatomi T, Hieda O, Sotozono C, Kinoshita S. Five-year follow-up outcomes after Descemet's stripping automated endothelial keratoplasty: a retrospective study. BMJ open ophthalmology. 2020:5(1):e000354. doi: 10.1136/bmjophth-2019-000354. Epub 2020 Jan 29 [PubMed PMID: 32154369]
Level 2 (mid-level) evidenceChaurasia S, Price FW Jr, Gunderson L, Price MO. Descemet's membrane endothelial keratoplasty: clinical results of single versus triple procedures (combined with cataract surgery). Ophthalmology. 2014 Feb:121(2):454-8. doi: 10.1016/j.ophtha.2013.09.032. Epub 2013 Nov 16 [PubMed PMID: 24252821]
Level 2 (mid-level) evidenceTerry MA, Shamie N, Chen ES, Phillips PM, Shah AK, Hoar KL, Friend DJ. Endothelial keratoplasty for Fuchs' dystrophy with cataract: complications and clinical results with the new triple procedure. Ophthalmology. 2009 Apr:116(4):631-9. doi: 10.1016/j.ophtha.2008.11.004. Epub 2009 Feb 8 [PubMed PMID: 19201480]
Burkhart ZN, Feng MT, Price FW Jr, Price MO. One-year outcomes in eyes remaining phakic after Descemet membrane endothelial keratoplasty. Journal of cataract and refractive surgery. 2014 Mar:40(3):430-4. doi: 10.1016/j.jcrs.2013.08.047. Epub 2014 Jan 11 [PubMed PMID: 24417895]
Level 2 (mid-level) evidencePrice MO, Price DA, Fairchild KM, Price FW Jr. Rate and risk factors for cataract formation and extraction after Descemet stripping endothelial keratoplasty. The British journal of ophthalmology. 2010 Nov:94(11):1468-71. doi: 10.1136/bjo.2009.175174. Epub 2010 May 27 [PubMed PMID: 20508038]
Level 2 (mid-level) evidenceAlkatan H, Al-Rajhi A, Al-Shehri A, Khairi A. Histopathological findings of failed grafts following Descemet's stripping automated endothelial keratoplasty (DSAEK). Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2012 Jan:26(1):79-85. doi: 10.1016/j.sjopt.2011.05.006. Epub 2011 Jun 1 [PubMed PMID: 23960973]
Khan SN, Shiakolas PS, Mootha VV. Descemet's Stripping Automated Endothelial Keratoplasty Tissue Insertion Devices. Journal of ophthalmic & vision research. 2015 Oct-Dec:10(4):461-8. doi: 10.4103/2008-322X.176899. Epub [PubMed PMID: 27051492]
Busin M, Bhatt PR, Scorcia V. A modified technique for descemet membrane stripping automated endothelial keratoplasty to minimize endothelial cell loss. Archives of ophthalmology (Chicago, Ill. : 1960). 2008 Aug:126(8):1133-7. doi: 10.1001/archopht.126.8.1133. Epub [PubMed PMID: 18695109]
Bahar I, Kaiserman I, Sansanayudh W, Levinger E, Rootman DS. Busin Guide vs Forceps for the Insertion of the Donor Lenticule in Descemet Stripping Automated Endothelial Keratoplasty. American journal of ophthalmology. 2009 Feb:147(2):220-226.e1. doi: 10.1016/j.ajo.2008.08.029. Epub 2008 Oct 18 [PubMed PMID: 18930446]
Kruse FE, Laaser K, Cursiefen C, Heindl LM, Schlötzer-Schrehardt U, Riss S, Bachmann BO. A stepwise approach to donor preparation and insertion increases safety and outcome of Descemet membrane endothelial keratoplasty. Cornea. 2011 May:30(5):580-7 [PubMed PMID: 21598430]
Burkhart ZN, Feng MT, Price MO, Price FW. Handheld slit beam techniques to facilitate DMEK and DALK. Cornea. 2013 May:32(5):722-4. doi: 10.1097/ICO.0b013e31827797e7. Epub [PubMed PMID: 23407317]
Saad A, Guilbert E, Grise-Dulac A, Sabatier P, Gatinel D. Intraoperative OCT-Assisted DMEK: 14 Consecutive Cases. Cornea. 2015 Jul:34(7):802-7. doi: 10.1097/ICO.0000000000000462. Epub [PubMed PMID: 26002152]
Level 3 (low-level) evidenceNahum Y, Galor O, Atar M, Bahar I, Livny E. Real-time intraoperative ultrasound biomicroscopy for determining graft orientation during Descemet's membrane endothelial keratoplasty. Acta ophthalmologica. 2021 Feb:99(1):e96-e100. doi: 10.1111/aos.14515. Epub 2020 Jun 24 [PubMed PMID: 32578923]
Livny E, Bahar I, Nahum Y. "Ghost DMEK" Technique: Circular Peripheral Staining of Descemet's Membrane Endothelial Keratoplasty Grafts. Cornea. 2019 Feb:38(2):252-255. doi: 10.1097/ICO.0000000000001816. Epub [PubMed PMID: 30422864]
Gonzalez A, Price FW Jr, Price MO, Feng MT. Prevention and Management of Pupil Block After Descemet Membrane Endothelial Keratoplasty. Cornea. 2016 Nov:35(11):1391-1395 [PubMed PMID: 27560030]
von Marchtaler PV, Weller JM, Kruse FE, Tourtas T. Air Versus Sulfur Hexafluoride Gas Tamponade in Descemet Membrane Endothelial Keratoplasty: A Fellow Eye Comparison. Cornea. 2018 Jan:37(1):15-19. doi: 10.1097/ICO.0000000000001413. Epub [PubMed PMID: 29040116]
Feng MT, Price MO, Miller JM, Price FW Jr. Air reinjection and endothelial cell density in Descemet membrane endothelial keratoplasty: five-year follow-up. Journal of cataract and refractive surgery. 2014 Jul:40(7):1116-21. doi: 10.1016/j.jcrs.2014.04.023. Epub [PubMed PMID: 24957432]
Level 2 (mid-level) evidenceGreenrod EB, Jones MN, Kaye S, Larkin DF, National Health Service Blood and Transplant Ocular Tissue Advisory Group and Contributing Ophthalmologists (Ocular Tissue Advisory Group Audit Study 16). Center and surgeon effect on outcomes of endothelial keratoplasty versus penetrating keratoplasty in the United Kingdom. American journal of ophthalmology. 2014 Nov:158(5):957-66. doi: 10.1016/j.ajo.2014.07.037. Epub 2014 Aug 1 [PubMed PMID: 25089353]
Deng SX, Lee WB, Hammersmith KM, Kuo AN, Li JY, Shen JF, Weikert MP, Shtein RM. Descemet Membrane Endothelial Keratoplasty: Safety and Outcomes: A Report by the American Academy of Ophthalmology. Ophthalmology. 2018 Feb:125(2):295-310. doi: 10.1016/j.ophtha.2017.08.015. Epub 2017 Sep 15 [PubMed PMID: 28923499]
Dunker SL, Veldman MHJ, Winkens B, van den Biggelaar FJHM, Nuijts RMMA, Kruit PJ, Dickman MM, Dutch Cornea Consortium. Real-World Outcomes of DMEK: A Prospective Dutch registry study. American journal of ophthalmology. 2021 Feb:222():218-225. doi: 10.1016/j.ajo.2020.06.023. Epub 2020 Jul 2 [PubMed PMID: 32621899]
Maier AK, Klamann MK, Torun N, Gonnermann J, Schroeter J, Joussen AM, Rieck P. Intraocular pressure elevation and post-DSEK glaucoma after Descemet`s stripping endothelial keratoplasty. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2013 Apr:251(4):1191-8. doi: 10.1007/s00417-012-2203-5. Epub 2012 Nov 20 [PubMed PMID: 23180233]
Level 2 (mid-level) evidenceMaier AB, Pilger D, Gundlach E, Winterhalter S, Torun N. Long-term Results of Intraocular Pressure Elevation and Post-DMEK Glaucoma After Descemet Membrane Endothelial Keratoplasty. Cornea. 2021 Jan:40(1):26-32. doi: 10.1097/ICO.0000000000002363. Epub [PubMed PMID: 32558736]
Price MO, Jordan CS, Moore G, Price FW Jr. Graft rejection episodes after Descemet stripping with endothelial keratoplasty: part two: the statistical analysis of probability and risk factors. The British journal of ophthalmology. 2009 Mar:93(3):391-5. doi: 10.1136/bjo.2008.140038. Epub 2008 Nov 19 [PubMed PMID: 19019938]
Level 2 (mid-level) evidencePrice DA, Kelley M, Price FW Jr, Price MO. Five-Year Graft Survival of Descemet Membrane Endothelial Keratoplasty (EK) versus Descemet Stripping EK and the Effect of Donor Sex Matching. Ophthalmology. 2018 Oct:125(10):1508-1514. doi: 10.1016/j.ophtha.2018.03.050. Epub 2018 May 3 [PubMed PMID: 29731147]
Hos D, Matthaei M, Bock F, Maruyama K, Notara M, Clahsen T, Hou Y, Le VNH, Salabarria AC, Horstmann J, Bachmann BO, Cursiefen C. Immune reactions after modern lamellar (DALK, DSAEK, DMEK) versus conventional penetrating corneal transplantation. Progress in retinal and eye research. 2019 Nov:73():100768. doi: 10.1016/j.preteyeres.2019.07.001. Epub 2019 Jul 3 [PubMed PMID: 31279005]
Myerscough J, Friehmann A, Bovone C, Busin M. Autologous Descemet Stripping Automated Endothelial Keratoplasty to Eliminate Endothelial Rejection in Eyes at High Risk. Cornea. 2020 May:39(5):666-668. doi: 10.1097/ICO.0000000000002184. Epub [PubMed PMID: 31688200]
Hos D, Tuac O, Schaub F, Stanzel TP, Schrittenlocher S, Hellmich M, Bachmann BO, Cursiefen C. Incidence and Clinical Course of Immune Reactions after Descemet Membrane Endothelial Keratoplasty: Retrospective Analysis of 1000 Consecutive Eyes. Ophthalmology. 2017 Apr:124(4):512-518. doi: 10.1016/j.ophtha.2016.12.017. Epub 2017 Jan 13 [PubMed PMID: 28094043]
Level 2 (mid-level) evidenceCrews JW, Price MO, Lautert J, Feng MT, Price FW Jr. Intraoperative hyphema in Descemet membrane endothelial keratoplasty alone or combined with phacoemulsification. Journal of cataract and refractive surgery. 2018 Feb:44(2):198-201. doi: 10.1016/j.jcrs.2017.11.015. Epub 2018 Mar 7 [PubMed PMID: 29525615]
Stuart AJ, Romano V, Virgili G, Shortt AJ. Descemet's membrane endothelial keratoplasty (DMEK) versus Descemet's stripping automated endothelial keratoplasty (DSAEK) for corneal endothelial failure. The Cochrane database of systematic reviews. 2018 Jun 25:6(6):CD012097. doi: 10.1002/14651858.CD012097.pub2. Epub 2018 Jun 25 [PubMed PMID: 29940078]
Level 1 (high-level) evidenceZhu L, Zha Y, Cai J, Zhang Y. Descemet stripping automated endothelial keratoplasty versus descemet membrane endothelial keratoplasty: a meta-analysis. International ophthalmology. 2018 Apr:38(2):897-905. doi: 10.1007/s10792-017-0533-3. Epub 2017 Apr 17 [PubMed PMID: 28417337]
Level 1 (high-level) evidenceMarques RE, Guerra PS, Sousa DC, Gonçalves AI, Quintas AM, Rodrigues W. DMEK versus DSAEK for Fuchs' endothelial dystrophy: A meta-analysis. European journal of ophthalmology. 2019 Jan:29(1):15-22. doi: 10.1177/1120672118757431. Epub 2018 Apr 16 [PubMed PMID: 29661044]
Level 1 (high-level) evidenceHirabayashi KE, Chamberlain W, Rose-Nussbaumer J, Austin A, Stell L, Lin CC. Corneal Light Scatter After Ultrathin Descemet Stripping Automated Endothelial Keratoplasty Versus Descemet Membrane Endothelial Keratoplasty in Descemet Endothelial Thickness Comparison Trial: A Randomized Controlled Trial. Cornea. 2020 Jun:39(6):691-696. doi: 10.1097/ICO.0000000000002256. Epub [PubMed PMID: 31939923]
Level 1 (high-level) evidenceBirbal RS, Ni Dhubhghaill S, Bourgonje VJA, Hanko J, Ham L, Jager MJ, Böhringer S, Oellerich S, Melles GRJ. Five-Year Graft Survival and Clinical Outcomes of 500 Consecutive Cases After Descemet Membrane Endothelial Keratoplasty. Cornea. 2020 Mar:39(3):290-297. doi: 10.1097/ICO.0000000000002120. Epub [PubMed PMID: 31478948]
Level 2 (mid-level) evidenceMadi S, Leon P, Nahum Y, DʼAngelo S, Giannaccare G, Beltz J, Busin M. Five-Year Outcomes of Ultrathin Descemet Stripping Automated Endothelial Keratoplasty. Cornea. 2019 Sep:38(9):1192-1197. doi: 10.1097/ICO.0000000000001999. Epub [PubMed PMID: 31246680]
Koo EH, Pineda R, Afshari N, Eghrari A. Learning Descemet Membrane Endothelial Keratoplasty: A Survey of U.S. Corneal Surgeons. Cornea. 2020 May:39(5):590-593. doi: 10.1097/ICO.0000000000002203. Epub [PubMed PMID: 31724984]
Level 3 (low-level) evidence