Definition/Introduction
The asterion, derived from the Greek word asterion meaning “starry,” is an anatomical landmark on the human skull.

The asterion, derived from the Greek word asterion meaning “starry,” is an anatomical landmark on the human skull.
The asterion is an anatomical landmark on the lateral aspect of the skull formed at the junction of the occipital bone, the temporal bone, and the parietal bone (see Image. Asterion Landmark). Its definition can also be a confluence of the lambdoid suture, which is the junction of the occipital and parietal bones, the occipitomastoid suture, which is a junction of the occipital and temporal bones, and the parietomastoid suture, which is a junction of the parietal and temporal bones. It is a visible landmark on the human skull that is seen when the removal of the soft tissue from the bony surfaces takes place. Asterion is internally related to the transverse and sigmoid sinuses. It signifies the site of the closed mastoid fontanelle. Asterion corresponds to the posterior end of the parietotemporal suture, the Pterion forming the anterior end. It is used as a surface landmark for the radiological and anthropological measurement of the skull. The sutural anatomy of the asterion is useful in retrosigmoid surgical approaches to the posterior fossa.[1] The location of the asterion has been studied in various population demographics, trying to demonstrate whether it can be used as a reliable landmark for surgical approaches.
Asterion is used only as a referral superficial anatomical landmark for neuronavigation and imaging modalities. It is more valuable in underdeveloped nations where advanced imaging techniques are not readily available.[2][3] A study was conducted on 100 dried skulls to determine the reliability of the asterion as a landmark for the intracranial procedure. It was found to be positioned over the posterior fossa dura on only 32% of the right and 25% on the left. The asterion was located over the transverse or the sigmoid sinus, 61% on the right and 66% on the left. Thus a burr hole placed at the Asterion may open directly into the sinuses.[4] Retrosigmoid technique is important for tumor resection from the cerebellopontine angle, such as with vestibular schwannoma removal. A 2007 study sought to provide the best location on the surface anatomy of the skull through which to drill and perform an endoscopic retrosigmoid keyhole approach in the skull base minimally invasive surgery. A burr hole of 2 cm in diameter created at the midpoint between the asterion and the mastoid tip was suitable for exposing structures in the cerebellopontine angle in endoscopic minimally invasive surgery.[5] Surgeons can work with both hands using the endoscope and the cannula simultaneously. This approach was proposed to improve maneuverability during minimally invasive retrosigmoid surgery.[6]
A study on 100 dried skulls was conducted using a 2 mm drill bit perpendicular to the skull at the asterion. The distance of the asterion from the zygomatic process, the suprameatal crest, and the mastoid tip were studied. It was found to be located superficial to transverse sigmoid sinus junction in 87%, inferior in 11%, and superior in 2% of the skulls. The location and anatomical relations of the asterion might prove beneficial in microvascular trigeminal root decompression and petrosal approaches.[7] The surface and intracranial location of the asterion and anatomical relation with the dural venous sinuses have been studied to help neurosurgeons avoid fatal complications while using the burr hole technique in retrosigmoid approaches.[8][9]
The asterion may also play a part in the placement of hearing implants. A study was conducted to find an alternative site for implanting the floating mass transducer of a bone conduction hearing implant, which is ordinarily implanted on the mastoid. In patients with prior mastoid surgery or anatomical difficulties precluding appropriate placement of the mass transducer, an alternative method should be in place. A retrosigmoid approach was proposed, using pre-operative computed tomography scanning and avoiding the sigmoid sinus by targeting a point approximately 1.9 cm posterior, 1.7 cm inferior to the asterion, 3.3 cm posterior, and 2.1 cm superior to the mastoid notch.[10]
Asterion meningiomas, although rare, arise at the junction of sigmoid and transverse sinuses, that is, the sinudural angle. Asterion meningiomas can be completely resected without complications. A study on 7 patients proposed that the non-dominant transverse/sigmoid sinus should be resected during these procedures. In contrast, more studies are needed to determine whether resecting a dominant transverse/sigmoid sinus is safe.[11] The risk of recurrence usually depends on the extent of resection, such that it avoids venous outflow obstruction leading to significant neurological sequelae. If a meningioma completely obstructs the venous sinus, gross resection of the intravascular portion should be performed.
Interprofessional healthcare team members who are involved in procedures involving the skull should be aware of the asterion, its location, and its clinical significance.
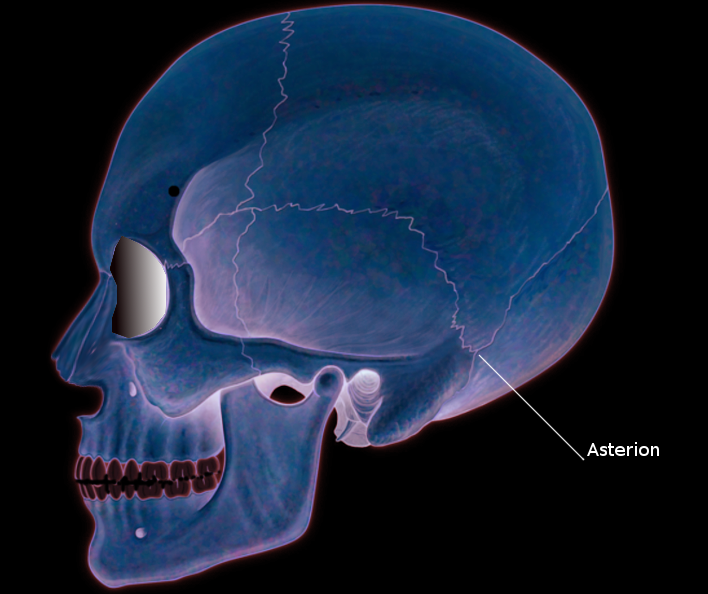
Asterion Landmark
Contributed by S Bhimji, MD
Ersoy M, Evliyaoglu C, Bozkurt MC, Konuskan B, Tekdemir I, Keskil IS. Epipteric bones in the pterion may be a surgical pitfall. Minimally invasive neurosurgery : MIN. 2003 Dec:46(6):363-5 [PubMed PMID: 14968406]
Venter G, Prigge L, Viljoen BL, DE Beer FC, Bam LC. Evaluation of the inion and asterion as neurosurgical landmarks for dural venous sinuses: osteological study on a sample of South African skull specimens. Journal of neurosurgical sciences. 2021 Apr:65(2):200-206. doi: 10.23736/S0390-5616.19.04596-X. Epub 2019 Mar 18 [PubMed PMID: 30916524]
Mwachaka PM, Hassanali J, Odula PO. Anatomic position of the asterion in Kenyans for posterolateral surgical approaches to cranial cavity. Clinical anatomy (New York, N.Y.). 2010 Jan:23(1):30-3. doi: 10.1002/ca.20888. Epub [PubMed PMID: 19918868]
Day JD, Tschabitscher M. Anatomic position of the asterion. Neurosurgery. 1998 Jan:42(1):198-9 [PubMed PMID: 9442525]
Xia Y, Li XP, Han DM, Zheng J, Long HS, Shi JF. Anatomic structural study of cerebellopontine angle via endoscope. Chinese medical journal. 2007 Oct 20:120(20):1836-9 [PubMed PMID: 18028782]
Arıcıgil M, Arbağ H, Dündar MA, Aziz SK, Yılmaz MT. Minimally Invasive Endoscopic Retrosigmoid Approach to the Cerebellopontine Angle Using a Novel Surgical Instrument: A Cadaveric Study. The journal of international advanced otology. 2018 Dec:14(3):472-477. doi: 10.5152/iao.2018.4474. Epub [PubMed PMID: 30644376]
Ucerler H, Govsa F. Asterion as a surgical landmark for lateral cranial base approaches. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2006 Oct:34(7):415-20 [PubMed PMID: 16963269]
Babacan S, Yildiz-Yilmaz M, Kafa IM, Coşkun I. The Surface and Intracranial Location of Asterion. The Journal of craniofacial surgery. 2019 Nov-Dec:30(8):e753-e755. doi: 10.1097/SCS.0000000000005757. Epub [PubMed PMID: 31689738]
Martinez F, Laxague A, Vida L, Prinzo H, Sgarbi N, Soria VR, Bianchi C. [Topographic anatomy of the asterion]. Neurocirugia (Asturias, Spain). 2005 Oct:16(5):441-6 [PubMed PMID: 16276452]
Arnold H, Schulze M, Wolpert S, Hirt B, Tropitzsch A, Zimmermann R, Radeloff A, Löwenheim H, Reimann K. Positioning a Novel Transcutaneous Bone Conduction Hearing Implant: a Systematic Anatomical and Radiological Study to Standardize the Retrosigmoid Approach, Correlating Navigation-guided, and Landmark-based Surgery. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2018 Apr:39(4):458-466. doi: 10.1097/MAO.0000000000001734. Epub [PubMed PMID: 29494472]
Level 1 (high-level) evidenceVrionis FD, Robertson JH, Heilman CB, Rustamzedah E. Asterion meningiomas. Skull base surgery. 1998:8(3):153-61 [PubMed PMID: 17171051]