Erbium-doped yttrium-aluminum-garnet (Er:YAG) laser skin resurfacing is an effective means of managing a number of cutaneous conditions and lesions. Its main indications include treatment of photoaging, rhytids, and benign and malignant cutaneous lesions. For many years, carbon dioxide (CO2) lasers (wavelength 10,600 nm) were the only lasers available for laser skin rejuvenation; nowadays, there are many more options, including the solid-state erbium-doped yttrium aluminum garnet Er:YAG (2,940 nm), diode (810 and 940 nm), and erbium:glass lasers (1,540 and 1,550 nm). This activity reviews the indications and technique for Er:YAG laser facial resurfacing and highlights the role of the interprofessional team in evaluating and treating patients who undergo Er:YAG laser treatments.
Objectives:
Identify the indications for Er:YAG laser resurfacing.
Outline the relevant anatomy and mechanism of action of Er:YAG laser treatments.
Describe the technique of Er:YAG laser resurfacing.
Explain the potential complications of Er:YAG laser resurfacing and summarize their management.
Introduction
With the passage of time, skin ages and accumulates photodamage. This results in loss of elasticity, changes in pigmentation, and the development of scarring from trauma, acne, and other insults.[1] Laser skin resurfacing has become a gold standard option for the rejuvenation of facial skin’s texture, tone, and elasticity.[2] For many years, carbon dioxide (CO2) lasers (wavelength 10,600 nm) were the only lasers available for laser skin rejuvenation; nowadays, there are many more options, including the solid-state erbium-doped yttrium aluminum garnet Er:YAG (2,940 nm), diode (810 and 940 nm), and erbium:glass lasers (1,540 and 1,550 nm).[2]
Er:YAG lasers were first FDA approved in 1996 for cutaneous resurfacing, and a comparative trial with CO2 lasers demonstrated that Er:YAG had equal efficacy with a trend towards more rapid recovery. Initially, short-pulse Er:YAG lasers were approved, with pulse lengths of 250-350 μs; however, variable and longer-pulse Er:YAG lasers with pulse widths of 500 μs to 10 ms were subsequently approved in 1999. The long-pulse and variable-pulse lasers introduced in 1999 were designed to provide enhanced coagulation, reducing bleeding compared to short-pulse Er:YAG treatments.
Anatomy and Physiology
The emitted peak wavelength of Er:YAG lasers is 2,940 nm, which is closest to the absorption peak of water at 3,000 nm. When an Er:YAG laser pulse is applied, the flashlamp-pumped crystal lasing medium emits light energy, which is absorbed by water in the epidermis and papillary dermis, resulting in two effects that promote skin rejuvenation. The first is vaporization of the epidermis, which requires the dermal appendages (hair follicles and sweat glands) to resurface the skin in order to heal. Secondly, thermal injury in the dermis stimulates collagen production, which improves the appearance of photodamaged skin while reducing visible rhytids and scars.[3][4] Furthermore, the vaporizing water acts as a heat sink, which decreases the amount of thermal damage sustained by the surrounding tissues. This cooling allows Er:YAG lasers to pass over the same target area multiple times during the same treatment session with a lower risk of causing a burn, providing improved results with fewer treatment sessions.[5]
Laser skin rejuvenation treatments are generally classified into two categories, ablative and non-ablative. Ablative lasers vaporize and/or coagulate the most superficial layers of skin, which results in rejuvenation via reepithelialization and collagen stimulation. The classic example of an ablative laser used for skin rejuvenation is the CO2 laser. Non-ablative laser treatments do not remove the epidermis but nonetheless cause controlled thermal injury, which stimulates the production of collagen and elastin. Examples include the diode, erbium:glass, and neodymium:YAG (Nd:YAG 1,320 nm) lasers. While ablative treatments typically provide more dramatic results, non-ablative lasers are preferred by many patients because of their lower risk profile and decreased post-treatment recovery time. However, more treatments with non-ablative lasers are often required to achieve the same effect as a single treatment with an ablative laser. The Er:YAG laser is considered an ablative laser.
Ablative laser energy delivery is commonly performed in one of two ways: with full-field therapy or via a fractionated beam. While a full-field approach treats the entire area of interest, fractionated treatments ablate microscopic vertical columns within the treatment area while leaving intervening areas that remain unaffected. This approach leaves uninjured skin and dermal appendages, which promote reepithelialization, reduce adverse side effects, and stimulate collagen production.[6] In either case, the goal is to ablate down to the papillary dermis, which will maximize collagen stimulation and tissue tightening while minimizing scarring. The depth at which the papillary dermis is found varies throughout the face, with the eyelids being the thinnest at about 150 μm and the chin being thickest at approximately 200 μm. Likewise, the thickness of the dermis varies from about 200 μm in the eyelids to approximately 1300 μm in the chin. The neck is the thinnest, with an epidermal thickness of roughly 100 μm and a dermal thickness of approximately 150 μm.
Indications
Er:YAG full-field laser skin resurfacing may be employed for the treatment of facial actinic damage, dyschromia, rhytids, scarring, skin laxity, or even for improvement in coarse skin texture. Full-field treatment is usually limited to Fitzpatrick skin types I-II to reduce the occurrence of adverse effects; however, in some cases, Fitzpatrick skin types III-IV may be treated using more conservative parameters.[5]
The Fitzpatrick skin classification categorizes skin pigmentation by its ability to tan and resistance to burning with sun exposure. Patients with type I skin always burn and never tan; they have very fair skin, often freckled with red or blonde hair and green or blue eyes. Patients with type II skin burn easily and only tan minimally, typically with fair skin, blonde or brown hair, and blue eyes. Patients with type III skin burn moderately but may also tan to a light brown color; they are generally fair-skinned with brown hair and brown eyes. Patients with type I-III skin are of predominantly European descent. Patients with type IV skin may be of Mediterranean or East Asian descent and also have dark hair and eyes; they burn only minimally and tan to a moderate brown color. Patients with type V skin rarely burn and tan darkly; they may be of South Asian descent. Patients with type VI skin never burn and do not typically demonstrate any skin changes with sun exposure. They are generally of sub-Saharan African descent.[7][8] For patients of skin type V-VI, resurfacing with a fractionated beam is considered the safest option because of its lower likelihood of causing pigmentary abnormalities. However, even fractionated Er:YAG treatments in these patients should be undertaken with great care. Low fluence (energy density) settings should be used, and the laser should be fired once in an inconspicuous area (test spot) and allowed to heal for 2 to 3 weeks prior to undertaking a full treatment.
Patients undergoing Er:YAG laser resurfacing can experience visible improvement of facial rhytids 3 to 8 weeks following treatment, particularly in the periorbital and perioral areas.[9] Histologically, there is a notable increase in dermal collagen at six weeks post-treatment. Er:YAG lasers have also been proven effective for removing benign, premalignant, and malignant skin lesions. Khatri et al. demonstrated that the short pulse Er:YAG laser could be used by applying multiple passes over the target lesion until it was no longer visibly apparent.[10] This approach has also been proven effective for congenital melanocytic nevi in neonates and acquired melanocytic nevi in adults, although hyper- or hypopigmentation may result in the treated area.[11] Seborrheic keratoses, acrochordons, and superficial intradermal cysts are also amenable to such spot treatments with the Er:YAG laser.
Contraindications
Contraindications to Er:YAG laser facial resurfacing include recent isotretinoin use (within the past 6-12 months), history of radiation therapy, history of keloid scarring, or presence of ectropion if the lower eyelid is to be targeted. Patients with fair skin (Fitzpatrick I-II) are good candidates for both fractionated and full field ablation, but darker-skinned patients (Fitzpatrick III-IV) should only undergo fractionated treatments. Patients with Fitzpatrick type V-VI skin should generally avoid Er:YAG laser skin resurfacing because of the high risk of post-procedure dyspigmentation. Patients with vitiligo may also be at a higher risk of developing post-treatment dyspigmentation. Conditions that inhibit or delay healing, such as diabetes and certain therapies for autoimmune diseases, are also relative contraindications for Er:YAG laser treatment. Lastly, patients with active infections, such as acne, cellulitis, impetigo, or herpes outbreaks, should wait until the infections are cleared to proceed with Er:YAG laser resurfacing.
Equipment
In addition to the laser itself, safety goggles rated for protection at 2,940 nm are required for all members of the healthcare team present during the treatment to avoid corneal injury. The Er:YAG laser delivers energy in the near-infrared range so that the goggles will appear transparent to the naked eye. The patient should either receive safety goggles or steel eye shields, depending on where the laser is to be applied. Whenever lasers are in use, particularly if there will be an oxygen source, a fire extinguisher should be readily available, as well as a container of water with which to douse the fire, if necessary. Additionally, to combat smoke and microorganism particulate inhalation, there should be a smoke evacuator with an ultra-low particulate air (ULPA) filter present, and healthcare team members should wear laser-rated masks rather than standard surgical masks.
Personnel
Laser resurfacing is not a personnel-intensive procedure; only the clinician and a laser operator, such as a nurse, are required to provide the treatment in an office setting. For full field ablation of large areas, such as the entire face, general anesthesia is recommended, which would require an anesthesia provider.
Preparation
A thorough history and physical examination are essential when evaluating patients for Er:YAG laser therapy. Before initiating treatment, patients must be fully informed of treatment risks and expectations; they should also be assessed for contraindications to therapy. If perioral treatment is planned, the patient should be asked about a history of cold sores, which could be reactivated by the laser. Underlying cutaneous conditions at the treatment sites, such as vitiligo, should be assessed. The history should also include an account of sun exposure, sunscreen use, and family/personal history of skin cancers.
Prior to laser resurfacing, if the perioral area is to be treated, patients should receive prophylactic antiviral medications to prevent herpes simplex outbreaks in the post-treatment period. Herpes lesions can cause scarring and may also be superinfected with bacteria, such as Staphylococcus aureus. An example of an effective prophylactic regimen is valacyclovir 500 mg PO BID x14 days starting the day prior to or the day of treatment.[12]
Technique or Treatment
For spot treatment of cutaneous lesions, pulses of 10 μm in depth and 10 to 40 pulses per second are employed. Reepithelialization of treated areas typically occurs within 4 to 7 days. For larger lesions, full field laser skin resurfacing can be applied to a subregion (such as for small areas of acne scarring), an entire facial aesthetic subunit (such as for the cheeks and forehead), or the entire face.[13] A treatment depth of 250 μm is sufficient for generalized skin rejuvenation, while greater treatment depths of up to 1000 μm are required for deeper scars caused by acne, surgery, or trauma. Several commercially available systems can deliver Er:YAG laser energy, some of which utilize a tube and mirror transmission system and some of which use optical fiber. Many can also deliver energy by other means, such as with an Nd:YAG lasing medium or with intense pulsed light. Prior to beginning a laser procedure, it is recommended that the laser operator test fire the system, often on a wooden tongue depressor.
Increasing the duration of individual pulses during Er:YAG treatment results in increased tissue heating below the zone of ablation. While this can lead to improved clinical results, increased heating has also been associated with an increased risk of adverse effects. Greater treatment density while maintaining short pulse widths, however, can produce more effective skin rejuvenation with fewer treatments. This is usually achieved by increasing the overlap of pulse areas or passing over the treatment more than once during the treatment session.[14]
The coagulation capability of the Er:YAG laser - sometimes also known as "CO2 emulation" because of the CO2 laser's tendency to coagulate tissue - allows for greater skin tightening with reduced bleeding. When multiple passes are used, the first pass is done in the "ablate" mode to remove the superficial layers of the epidermis and dermis and expose the underlying collagen in the dermis. Subsequent passes in the "coagulation" mode can achieve greater depth of ablation and thermal injury to the upper and mid-papillary dermis.[15] When full field ablation is performed, and to a lesser extent when using a fractionated beam, it is advisable to hold a smoke evacuator with a ULPA filter within 2 cm of the tissue being ablated to prevent inhalation of smoke that may contain aerosolized microorganisms, such as viruses; this is particularly important when ablating skin lesions, such as papillomas. Pinpoint bleeding generally ensues after either fractionated or full field ablation; nonadherent gauze soaked in a vasoconstrictor, such as oxymetazoline or epinephrine, can be very helpful for controlling blood loss.
Superficial resurfacing can be achieved with a fluence of 5 to 10 J/cm^2 or a treatment depth of fewer than 250 μm. This approach removes part or all of the epidermis and can result in mild improvement in the appearance of photoaging with a shorter "down-time" and recovery period, as well as a decreased requirement for anesthesia. Increasing the fluence from 5 to 10 J/cm^2 can result in more erythema and discomfort but also achieves a greater clinical result. Ablation with Er:YAG laser is carried out until the clinical endpoint is reached, indicating adequate treatment. Er:YAG laser endpoints include the appearance of petechial bleeding (indicating ablation entering the papillary dermis), a yellow color (termed chamois color), which indicates ablation of the midpapillary dermis, and visual effacement of rhytids.[14] However, these clinical endpoints are not typically apparent when using fractionated beam delivery, only for full-field ablation. Ideally, the boundaries of the treated area should correspond to the boundaries of facial aesthetic units to make the edges of the treatment area less apparent. When performing a full facial ablation, most clinicians will feather the laser along the jawline to blend the treated area into the neck but not treat the neck itself because its dermis is very thin (approximately 140 μm), and it does not heal as well or as rapidly as the face because it lacks a high concentration of pilosebaceous units.
Using local, regional, or general anesthesia can significantly decrease patient discomfort. General anesthesia or intravenous sedation may be required for larger treatment areas or more aggressive resurfacing treatments, particularly full-field ablation. Resurfacing of smaller regions, fractionated treatments, or treatments that are more superficial in depth can be accomplished with regional nerve blocks or local anesthetic infiltration. A topical anesthetic is used for nearly all treatments, with additional modalities added as needed.
Post-procedure care involves covering the treatment area with a saline-moistened gauze immediately, followed by occlusive dressings with ointment or hydrocolloid to promote a moist wound healing environment until skin reepithelialization is completed 5 to 7 days post-treatment. Erythema will persist beyond the time it takes for skin to reepithelialize, with erythema from fractionated treatments taking less time to resolve than that from full field ablation, which may last as long as 3 or 4 months.
Complications
Short-term complications of Er:YAG therapy include the development of erythema and bleeding, as well as reactivation of herpes simplex virus infection. In some cases, bacteria (such as Staphylococcus sp) or even fungi (such as Candida sp) may cause secondary facial infections, but these are usually managed easily with appropriate antimicrobials. Post-inflammatory changes in pigmentation and the development of scarring may also occur. Hypo- and hyperpigmentation are among the most common side effects of ablative laser therapy.[16] Compared to CO2, Er:YAG is considered less likely to cause hyperpigmentation of treatment areas, although some studies have demonstrated similar side effect profiles for the two modalities of laser skin resurfacing.[17]
Increased Er:YAG pulse duration is associated with an increased risk of pigment changes, potentially because a longer pulse duration deposits more energy per pulse and thereby causes more thermal damage to surrounding tissue. The use of a fractionated beam delivery system decreases the risk of pigmentary changes. Pigmentary changes often fade with time; hyperpigmentation is more common than hypopigmentation and more likely to resolve. For persistent hyperpigmentation, 4% topical hydroquinone will help lighten the skin. For hypopigmentation, which is thought to result from inflammation that compromises melanocyte function, topical steroids may be helpful. Other options include sun exposure, blue laser therapy, intense pulsed light, and fractionated CO2 laser treatments.[18]
The risks of prolonged post-procedure erythema and pigment changes are greater in patients with darker skin (Fitzpatrick skin types III-VI). Other noted complications include the appearance of acne, milia, and dermatitis in the treated region. Some patients will complain of a persistently visible grid or checkerboard pattern after fractionated beam treatment, but this usually fades over time. It may be addressed with topical steroids or additional laser resurfacing when it does not resolve spontaneously. More problematic is when too much energy is delivered, resulting in a burn and subsequent scar. This may also be treated with laser resurfacing, as any other scar could be, but patients are often understandably reluctant to pursue this option due to prior experience with adverse laser treatment outcomes.
Ocular injury is among the most serious complications that may result from Er:YAG laser treatment. The cornea is the most likely structure to be damaged because of the Er:YAG laser's chromophore water. Ocular injury may be prevented with the use of ocular lubricant and corneal shields for the patient during treatment. Members of the healthcare team should wear protective glasses that will block light at 2,940 nm. An ophthalmologist should be consulted in the event of corneal injury.
The risk for complications can be reduced by performing a thorough pre-procedure history and physical examination. Appropriate patient selection is critical. Patient education also improves the chance of achieving satisfactory outcomes. The importance of sun protection in reducing the occurrence of post-inflammatory pigmentation changes should be emphasized. Patients should be educated on post-procedure wound care and informed about the normal post-treatment course and changes that occur during healing. The risk for infection, scarring, and delays with healing should be clearly outlined.
Clinical Significance
Er:YAG laser skin resurfacing is an effective treatment modality for a range of cutaneous indications, from spot treatment of lesions to full-field resurfacing. Emitting light at a peak wavelength of 2,940 nm, the laser's energy is absorbed by water in the epidermis and dermis. Epidermal ablation and resultant re-epithelialization can treat actinic damage, dyschromia, and coarse skin texture. Thermal injury in the dermis below the zone of ablation stimulates collagen production, reducing skin laxity and improving the appearance of static rhytids. With an appropriate selection of candidates for treatment with Er:YAG lasers, patients can achieve significantly improved skin appearance. Er:YAG laser facial skin resurfacing is most effective for patients with Fitzpatrick skin types I-II but can also be employed for Fitzpatrick skin types III-IV with careful laser pulse frequency and depth adjustment.
Not only is the Er:YAG laser effective as a stand-alone treatment, but it can also be combined with other techniques, including CO2 laser treatment. The combined use of CO2 and Er:YAG lasers have been shown to decrease crusting and pruritus following treatment as compared to treatment using CO2 lasers alone.[19] Er:YAG laser therapy can also be an excellent adjunct to surgical facial rejuvenation, including facelifting and blepharoplasty.[20]
Enhancing Healthcare Team Outcomes
A well-integrated, multi-disciplinary health care team will maximize patient outcomes after treatment with Er:YAG laser resurfacing. Additionally, a thorough patient evaluation that follows a well-established routine is essential for achieving optimal outcomes. Dermatologists, plastic surgeons, and laser operators, when working together as a team, are ideally suited to determine whether Er:YAG laser treatment is the appropriate treatment modality to address patient concerns. Pharmacy and anesthesiology can provide recommendations for pre-procedure and post-procedure management.
Patient education regarding what to expect during the treatment and pre-procedure and post-procedure care is important to optimize outcomes for patients and health care providers. Equally important is ensuring that the patient and clinician share a common picture of the goals and expectations for treatment to avoid dissatisfaction with the result. Nurses and physician assistants are also critical for supporting patients, particularly during the post-treatment period, when patients often have second thoughts about the procedure, discomfort, and, rarely, complications.
Utilizing an interprofessional health care team to deliver Er:YAG laser treatments improve situational awareness regarding the progression of recovery and the development of complications, facilitating a more timely response to any adverse events.[21] [Level 4]
Contributed by Ahmad M. Al Aboud, M.D., Perlita Perlac, BSN-RN, Anne Rose Encomienda, BSN-RN, Nidzma Ahaja, BSN-RN, Norhaya Nassa, BSN-RN.
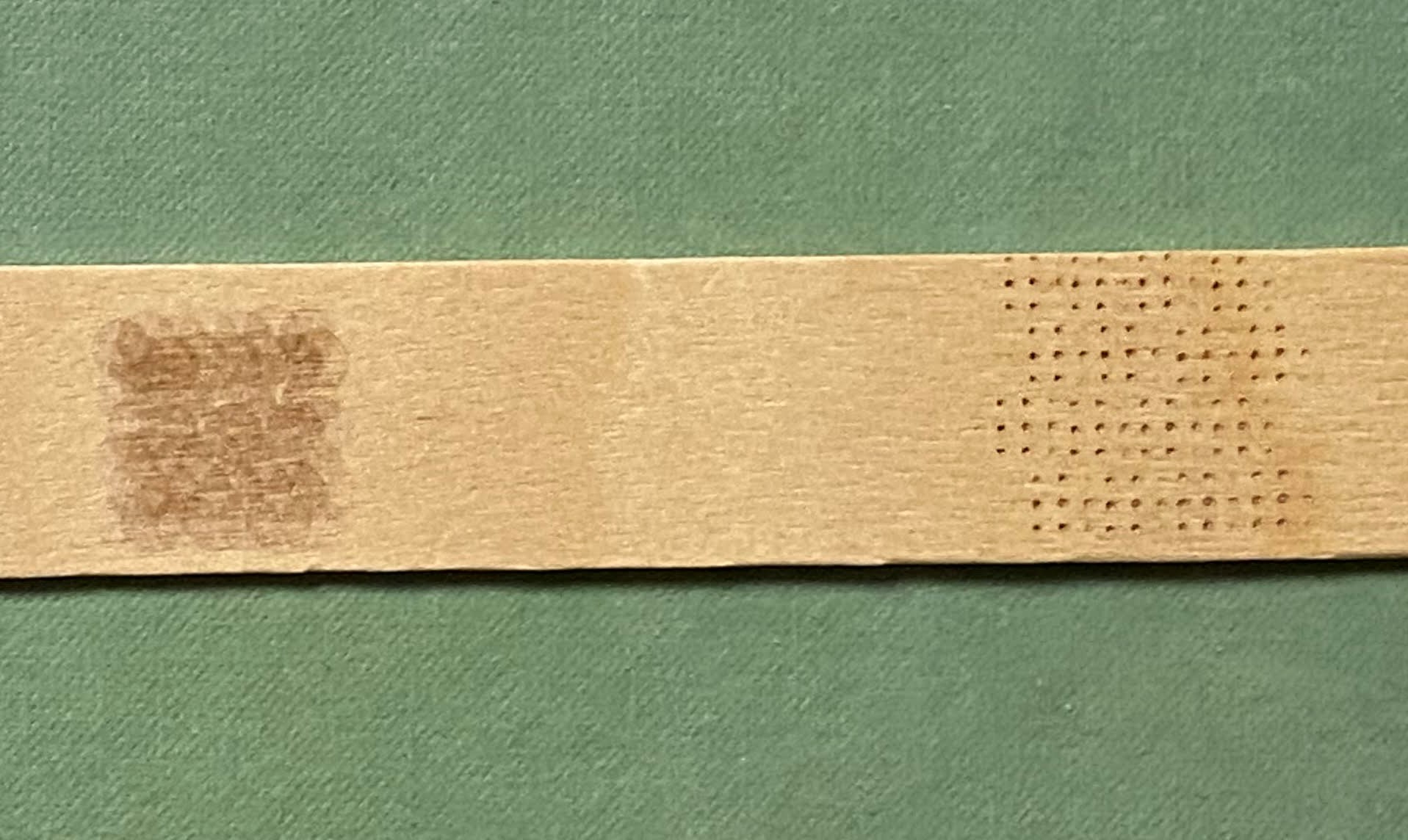
(Click Image to Enlarge)
Tongue depressor used to test fire the Er:YAG laser. On the left is the pattern generated for full field ablation (note the overlapping spots with no intervening unaffected areas) and on the right is the fractionated beam.
Contributed by Marc H Hohman, MD, FACS
(Click Image to Enlarge)
Er:YAG laser device with tube and mirror delivery system. Note the foot pedal used to fire the laser sitting at the base of the device, and the ULPA filter smoke evacuator located to the left of the laser. Also note the fire extinguisher on the wall, immediately available.
Contributed by Marc H Hohman, MD, FACS
Li D, Lin SB, Cheng B. Complications and posttreatment care following invasive laser skin resurfacing: A review. Journal of cosmetic and laser therapy : official publication of the European Society for Laser Dermatology. 2018 Jun:20(3):168-178. doi: 10.1080/14764172.2017.1400166. Epub 2017 Dec 13
[PubMed PMID: 29236557]
Alexiades-Armenakas MR, Dover JS, Arndt KA. The spectrum of laser skin resurfacing: nonablative, fractional, and ablative laser resurfacing. Journal of the American Academy of Dermatology. 2008 May:58(5):719-37; quiz 738-40. doi: 10.1016/j.jaad.2008.01.003. Epub
[PubMed PMID: 18423256]
Jasin ME. Achieving superior resurfacing results with the erbium:YAG laser. Archives of facial plastic surgery. 2002 Oct-Dec:4(4):262-6
[PubMed PMID: 12437434]
Holcomb JD. Versatility of erbium YAG laser: from fractional skin rejuvenation to full-field skin resurfacing. Facial plastic surgery clinics of North America. 2011 May:19(2):261-73. doi: 10.1016/j.fsc.2011.04.005. Epub
[PubMed PMID: 21763988]
Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Archives of dermatology. 1988 Jun:124(6):869-71
[PubMed PMID: 3377516]
Khatri KA. Ablation of cutaneous lesions using an erbium:YAG laser. Journal of cosmetic and laser therapy : official publication of the European Society for Laser Dermatology. 2003 Dec:5(3-4):150-3
[PubMed PMID: 14741818]
Ostertag JU, Quaedvlieg PJ, Kerckhoffs FE, Vermeulen AH, Bertleff MJ, Venema AW, van der Geer S, Krekels GA. Congenital naevi treated with erbium:YAG laser (Derma K) resurfacing in neonates: clinical results and review of the literature. The British journal of dermatology. 2006 May:154(5):889-95
[PubMed PMID: 16634892]
Gilbert S, McBurney E. Use of valacyclovir for herpes simplex virus-1 (HSV-1) prophylaxis after facial resurfacing: A randomized clinical trial of dosing regimens. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2000 Jan:26(1):50-4
[PubMed PMID: 10632686]
Perez MI, Bank DE, Silvers D. Skin resurfacing of the face with the Erbium:YAG laser. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 1998 Jun:24(6):653-8; discussion 658-9
[PubMed PMID: 9648573]
Kim YJ, Lee HS, Son SW, Kim SN, Kye YC. Analysis of hyperpigmentation and hypopigmentation after Er:YAG laser skin resurfacing. Lasers in surgery and medicine. 2005 Jan:36(1):47-51
[PubMed PMID: 15662626]
Tanzi EL, Alster TS. Single-pass carbon dioxide versus multiple-pass Er:YAG laser skin resurfacing: a comparison of postoperative wound healing and side-effect rates. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2003 Jan:29(1):80-4
[PubMed PMID: 12534517]
McDaniel DH, Lord J, Ash K, Newman J. Combined CO2/erbium:YAG laser resurfacing of peri-oral rhytides and side-by-side comparison with carbon dioxide laser alone. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 1999 Apr:25(4):285-93
[PubMed PMID: 10417584]
Smalley PJ. Keys to Building a Safe and Effective Healthcare Laser Program. Laser therapy. 2018 Mar 31:27(1):11-20. doi: 10.5978/islsm.18-OA-01. Epub
[PubMed PMID: 29795966]
Use the mouse wheel to zoom in and out, click and drag to pan the image