Introduction
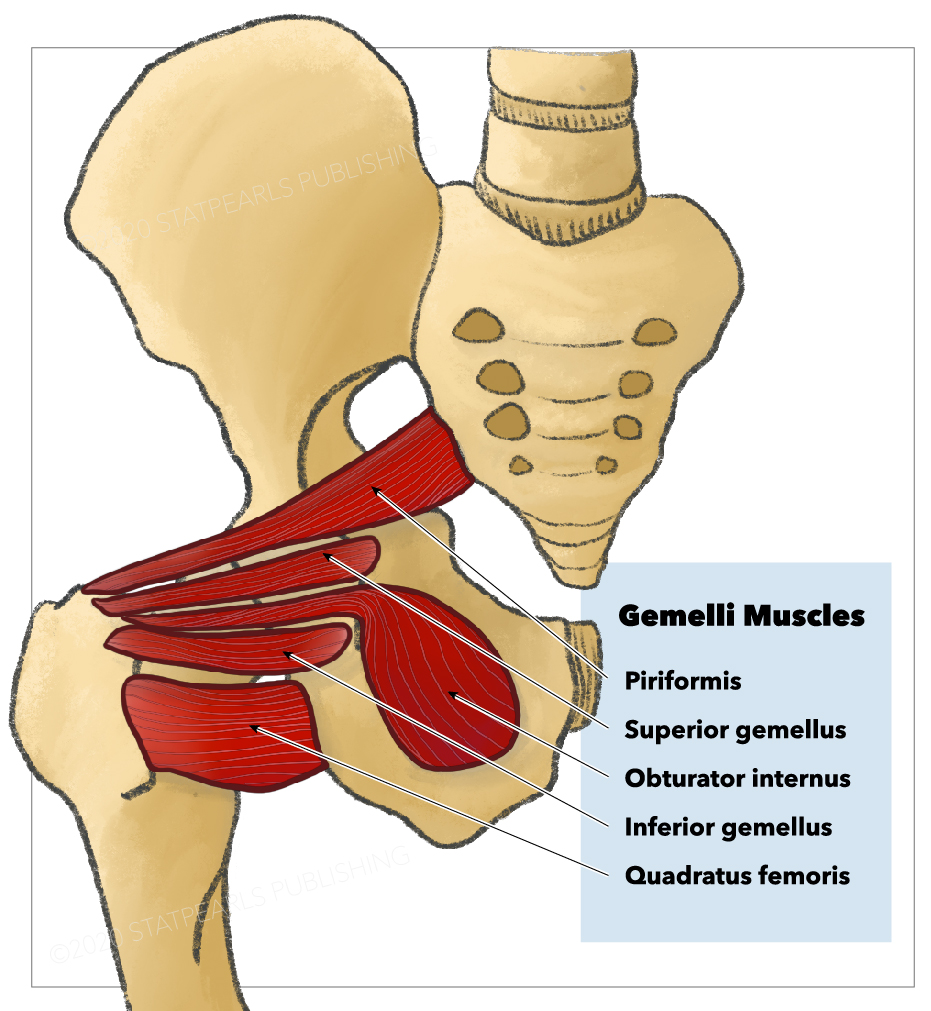
The superior and inferior gemellus muscles are a pair of small triangle-shaped muscles found among the posterior hip and gluteal musculature in the posterior proximal lower extremity, commonly referred to collectively as the gemelli muscles. The gemelli muscles are two of six short external rotator muscles in the gluteal region of the proximal thigh. The remaining external rotators include the piriformis, obturator internus, quadratus femoris, and obturator externus muscles. The superior and inferior gemelli join the obturator internus as a conjoined tendon, sometimes referred to as the triceps coxae.[1]
The gemelli muscles assist in external rotation of the thigh and have implications in sciatic nerve dysfunction known as deep gluteal space syndrome or gemelli-obturator syndrome.[2][3][4] The gemelli muscles, in conjunction with the obturator internus, are important surgical landmarks in the Kocher-Langenbeck and posterior approach to the hip, as well as essential for identifying and protecting the medial circumflex femoral artery.[5] The surgical approaches described are useful for surgical hip dislocations, total hip arthroplasty, hip hemiarthroplasty, loose body removal, treatment of posterior wall and column acetabular, and pelvic ring fractures.[1]
Structure and Function
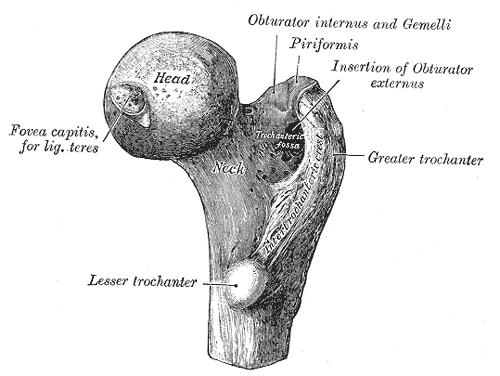
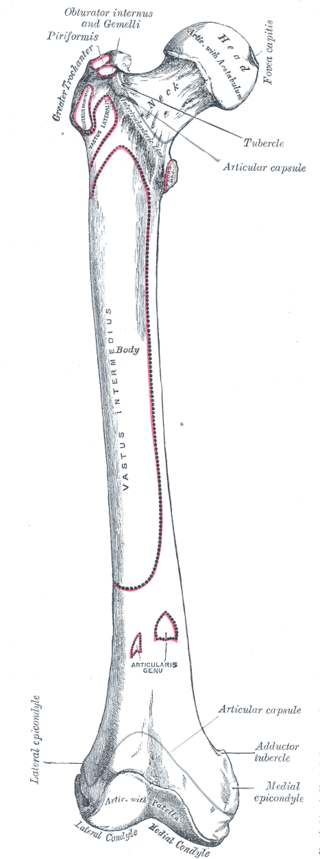
The superior gemellus muscle originates at the ischial spine, while the inferior gemellus muscle originates from the ischial tuberosity. Together with the obturator internus, the two gemelli muscles insert on the posteromedial surface of the greater trochanter of the femur.[2]
The primary function of the gemelli muscles is to externally (laterally) rotate the thigh and extend the hip. They also contribute to the abduction of the hip while in a flexed position. The two gemelli muscles work synergistically with the obturator internus and the remaining short external rotator to produce movement.[2]
Embryology
The limb buds of the embryo appear around four to five weeks of gestation as the mesoderm migrates into the limb bud and forms a posterior condensation and an anterior condensation to eventually create the muscular and skeletal components of the lower limb.[6][7][8] Around the fourth to the fifth week of gestation, myoblasts migrate from the somites. The posterior condensation or dorsal muscle mass of the limb will develop into the extensor and abductor musculature of the lower limb, and the anterior condensation or ventral muscle mass of the limb will develop into the flexor and adductor musculature of the lower limb.[6][7][8]
Several factors influence the formation of the limb bud musculature, including retinoic acid, sonic hedgehog (SHH), HOX genes, apical ectodermal ridge (AER), and the zone of polarizing activity (ZPA). Retinoic acid is a global organizing gradient that initiates the production of transcription factors that specify regional differentiation and limb polarization. The apical ectodermal ridge (AER) produces fibroblast growth factor (FGF), which promotes the outgrowth of the limb buds by stimulating mitosis.[6][7][8] This process is contingent on FGF and AER function; without appropriate signaling, limb development may cease. The specific fibroblast growth factor involved in hindlimb development is FGF10, which is stimulated by T-box transcription factor 4 (Tbx4).
The zone of polarizing activity (ZPA) produces SHH, which promotes the organization of the limb bud along the anterior-posterior axis. SHH activates specific HOX genes–Hoxd-9, Hoxd-10, Hoxd-11, Hoxd-12, and Hoxd-13–which are essential in limb polarization and regional specification. These genes control patterning and, consequently, the morphology of the developing limb in the human embryo. Errors in expression, signaling, and maintenance of these pathways can lead to malformations in limb development.[6][7][8]
Blood Supply and Lymphatics
The inferior gluteal artery supplies the superior and inferior gemelli muscles. The inferior gluteal artery arises from the anterior trunk of the internal iliac artery before passing between the second and third sacral segments of the sacral plexus and exiting the greater sciatic foramen under the piriformis to supply the gemelli muscles.
The lower limb lymphatic vessels can divide into two major groups—superficial and deep vessels. The superficial lymph vessels of the lower limb can further divide into two groups: a medial group, which follows the greater saphenous vein, and a lateral group, which follows the small saphenous vein.[6] Deep lymph vessels, including the anterior tibial, posterior tibial, and peroneal vessels, follow the course of the corresponding blood vessels.[6]
The lymph vessels of the lower limb drain into the popliteal, superficial inguinal, deep inguinal, external iliac, and lumbar or aortic lymph nodes.[6]
Nerves
The nerve innervates the superior gemellus muscle to the obturator internus (L4-S2), and the nerve innervates the inferior gemellus to the quadratus femoris (L4-S1). Each of these nerves is a branch of the sacral plexus. They are formed by the fourth and fifth lumbar ventral rami and the first four sacral ventral rami (L4-S4).
The nerve to the obturator internus passes through the greater sciatic foramen as it exits the pelvis inferior to the piriformis muscle. The nerve provides innervation to the superior gemellus as it passes and then returns into the pelvis through the lesser sciatic foramen and provides innervation to the obturator internus.
The nerve to the quadratus femoris exits the pelvis through the greater sciatic foramen deep to the piriformis muscle. It descends deep to the short external rotators terminating in the deep surface of the quadratus femoris, supplying the inferior gemellus muscle en route.
Physiologic Variants
The superior gemellus, inferior gemellus, and obturator internus muscles were historically regarded as a single muscle, given their common insertion and function. Current evidence suggests these muscles are separate entities owing to different origins and innervations.[9] Several authors have reported the presence of physiologic variants of the gemelli muscles, including the presence of two superior gemelli, the absence of both gemelli, and variations of their origins and insertions.[10] Surgeon awareness of the possibility of anatomical variants may help surgeons when accessing this region during surgical intervention.
Surgical Considerations
The most common surgical implication of the gemelli muscles involves the posterior surgical approach to the hip. The posterior approach to the hip, also known as the Kocher-Langenbeck approach, is a common surgical approach used for total and hemi- hip arthroplasty due to several advantages, including clear anatomical layer, lower incidence of heterotopic ossification, and intact hip abductors.[11] Following the initial approach, the triceps coxae muscles are elevated from their insertion approximately 1 to 2 cm on the posterior aspect of the greater trochanter.[12]
Surgeon preference may elevate the conjoint tendon directly off the bone. While an injury to these muscles is inevitable, controversy exists regarding how to minimize injury, whether the muscles should be repaired, and the effect of the repair. Recent literature highlights the significant reduction in risk of posterior dislocation when a thorough posterior capsule repair is performed with particular attention paid to the deep external rotators, including the triceps coxae muscles.[11][12][13] Consequently, an effective repair of the gemelli and obturator internus muscles may be essential early in the postoperative period to reduce the risk of reduction and aid in postoperative recovery and rehabilitation.[11]
Clinical Significance
Posterior hip or gluteal pain and sciatica are among the more common diagnostic and therapeutic challenges for orthopedic surgeons and general medical providers. Historically, the term “piriformis syndrome” encompassed several pathologies in this region. Recent advances in imaging techniques and evaluation of muscle and nerve kinematics have resulted in the new preferred terminology, “deep gluteal syndrome (DGS).”[2] DGS is characterized by pain and/or dysesthesias in the buttock, hip, or posterior thigh with or without radicular pain due to non-discogenic sciatic nerve entrapment.[2][3][12]
DGS encompasses several pathologic processes, including piriformis syndrome, gemelli-obturator syndrome, and tumoral compression, among others. Gemelli-obturator syndrome is a dynamic compression of the sciatic nerve when the gemelli obturator complex becomes stretched. The sciatic nerve courses deep to the piriformis muscle and superficial to the triceps coxae muscles. Consequently, this interaction may result in compression of the sciatic nerve, resulting in the clinical presentation of sciatic pain and requiring inclusion in the differential diagnosis of non-discogenic sciatica.[2]
To differentiate the causes of DGS, physical examination maneuvers and imaging techniques can contribute to a definitive diagnosis. Magnetic resonance imaging (MRI) can assist the clinician evaluate anatomical variants in soft tissues. Treatment of DGS targets the underlying cause and typically involves imaging-guided intra- and/or extra-articular injections, physical therapy, and anti-inflammatory drugs.[4] In rare cases that fail conservative management (including physical therapy, analgesic, anti-inflammatory drugs, and injections), surgical treatment (open or endoscopic) may be considered.[4]