Introduction
The occipital bone is the most posterior cranial bone and the main bone of the occiput. It is considered a flat bone, like all other cranial bones, meaning that its primary function is either for protection or to provide a broad surface for muscle attachment. The scalp, which consists of five layers, covers the bone. Going from superficial to deep, the scalp layers are skin, dense connective tissue, aponeurosis of the occipitofrontalis muscle, loose areolar connective tissue, and the periosteum. Within the dense connective tissue are the occipital artery and vein, and the lesser and greater occipital nerves. The inner part of the bone forms the posterior cranial fossa.
Structure and Function
The occipital bone is a very complex bone that serves primarily to protect the cerebellum and the occipital lobes of the cerebrum and to provide attachment to several muscles and ligaments described below. It is trapezoidal and shallowly curved on itself. It consists of outer and inner layers of cortical bone that sandwich cancellous bone, or diploe. It borders the parietal bones on either side superiorly to form the lambdoid suture, and the mastoid portion of the temporal bone to form the occipitomastoid suture on either side inferolaterally. The sphenoid bone articulates with it anteriorly via the inferior angle, and with the atlas inferiorly. The foramen magnum is part of the occipital bone, through which the medulla oblongata, the accessory nerves, the anterior and posterior spinal arteries, the vertebral arteries, the alar ligaments, and the tectorial membranes passes. It consists of three parts, including the basilar, condylar, and squamous parts, all of which have outer (facing the outside) and inner (facing the brain) parts.
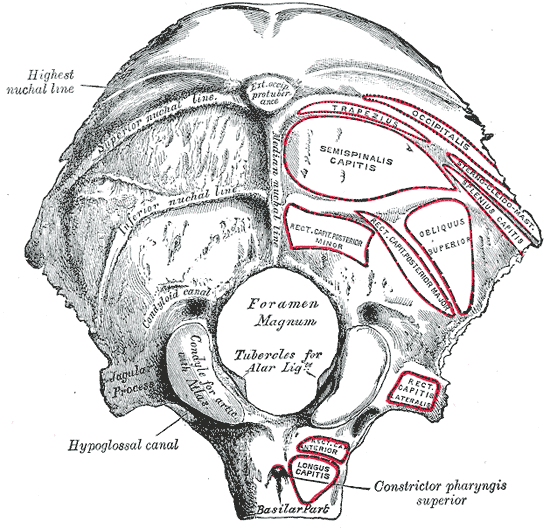
The squamous part of the occipital bone is the most posterior and largest portion. It is the part of the bone that borders the parietal and temporal bone, and the posterior part of the foramen magnum. The outer squamous part contains several ridges or lines, crests, and prominences. There are three horizontal so-called nuchal lines. Superiorly to inferiorly, they are the supreme (also known as the highest), superior, and inferior nuchal lines. The supreme nuchal line begins about where the skull starts to curve inward to make the inferior surface and extends from midline to the lambdoid sutures on either side, curving slightly downward as it moves laterally. The superior nuchal line is larger than the supreme nuchal line, and it also extends from midline to the lambdoid sutures, curving slightly more than the supreme nuchal line laterally. At its midline is a prominence called the external occipital protuberance, with its highest point termed the inion. The superior nuchal line makes an intersection with a vertical midline ridge of bone called the medial nuchal line, which is also known as the external occipital crest, forming an uppercase “T” on the surface of the occipital bone. The superior nuchal line provides an attachment surface on its inferomedial side for the semispinalis capitis muscle, and on its inferolateral side for the obliquus capitis superior. The medial nuchal line extends caudally in a straight line to the foramen magnum, and with the inion, serves as the attachment for the nuchal ligament and the trapezius muscle. The inferior nuchal line transects the medial nuchal line approximately at its midpoint, curving more downward than the supreme or superior nuchal lines.
The cranial, or inner surface of the occipital bone makes up the base of the posterior cranial fossa. On the squamous part of the inner surface is a midline vertical ridge called the median internal occipital crest that runs from a median prominence called the internal occipital protuberance to the foramen magnum. The median internal occipital crest provides attachment for the falx cerebri and contains a groove for the occipital sinus. Running from the internal occipital protuberance to the superior border is the groove for the superior sagittal sinus. On each side of the internal occipital protuberance is a groove for the transverse sinus. The meeting point of the superior sagittal sinus, the straight sinus, and the occipital sinus is called the confluence of the sinuses, which drains the venous blood into the right and left transverse sinuses. These internal structures form a lower case “t”: the top of the “t” is comprised of the superior sagittal sinus groove, the intersection of the lines making the “t” is the internal occipital protuberance, the horizontal line of the “t” are the grooves for the transverse sinus, and the lower part of the “t” is the median internal occipital crest. This lower case “t” is also known as the cruciform eminence, due to its cross, or crucifix-like structure. Therefore, this structure divides the concave internal surface of the occipital bone to make four distinct fossae: two upper fossae, and two lower fossae. The upper fossae are called the cerebral fossa and hold the occipital lobes of the cerebrum. The lower fossae are called the cerebellar fossae and hold the hemispheres of the cerebellum. The inferior edge of the squamous part of the inner occipital bone makes up the posterior part of the foramen magnum. It contains a landmark called the opisthion, the midpoint of the posterior margin of the foramen magnum. It has a twin at the midpoint of the most anterior margin of the foramen magnum called the basion, located on the basilar part of the occipital bone, that lines up with the dens of the atlas.
The condylar part makes up the lateral edges of the foramen magnum on the undersurface of the occipital bone and is also known as the exoccipitals. It is made up of protuberances on either side of the foramen magnum called the occipital condyles, serving as an articular surface to the superior facets of the atlas. At the base of the condyles on the cranial (inner) side is the hypoglossal canal where the hypoglossal nerve exits, and a branch of the ascending pharyngeal artery enters. Posterior to the condyles is the condyloid fossa, a depression that articulates with the superior facet of the atlas during neck extension. Within the fossa is the condylar canal, where there may be an occipital emissary vein that perforates the bone to connect the occipital sinus, sigmoid sinus, and suboccipital venous plexus. The capsules of the atlantooccipital articulation attach to the margins, and medial to these is a tubercle where the alar ligament attaches. The jugular process comprises the anterolateral part of the bone on either side, on which the rectus capitis lateralis muscle inserts. Anterior to these processes is the jugular notch, forming the posterior portion of the jugular foramen.[1]
The inner surface of the condylar part makes up the sides of the foramen magnum and contains the hypoglossal canals, as previously mentioned. More lateral to the hypoglossal canal is the jugular foramen, located at the junction of the occipital bone and the petrous portion of the temporal bone.[2]
The basilar part makes up the anterior portion of the foramen magnum on the undersurface of the occipital bone and connects to the sphenoid bone. It is thick and quadrilateral in shape. The anterior atlantooccipital membrane attaches to its inferior surface immediately anterior to the foramen magnum. Even more anterior to the foramen magnum is the pharyngeal tubercle, the attachment site of the fibrous raphe of the pharynx. On either side of the midline of its inferior surface, the basilar part provides muscular attachment of the longus capitis and rectus capitis anterior muscles. The upper surface of the basilar part supports the medulla oblongata with its broad, shallow groove called the clivus, where the abducens nerve also runs nearby. It also provides attachment to the tectorial membrane near the foramen magnum. The lateral surface of the basilar part forms a junction with the petrous portion of the temporal bone to form the inferior petrosal sulcus, in which the inferior petrosal sinus lies. The inferior petrosal sinus receives veins from the medulla, pons, the inferior surface of the cerebellum, and the internal auditory veins and drains into the internal jugular vein. The inner basilar part contains the basion, as previously mentioned.
Embryology
The occipital bone, like all other bones of the skull, develops from neural crest cells and paraxial mesoderm. It develops through both intramembranous and endochondral ossification. Intramembranous ossification refers to connective tissue membrane replacement with bony tissue, whereas endochondral ossification refers to the replacement of hyaline cartilage with bony tissue. The occipital plane, part of the squamous occipital bone, develops via the former model, and the remainder of the occipital bone forms via endochondral ossification.
There are typically four nuclei in the occipital plane to develop via intramembranous ossification. The nuchal plane of the squamous occipital bone ossifies via endochondral ossification from two nuclei. Occasionally, a Kerckring center will form at the posterior margin of the foramen magnum that will go on to form a separate ossicle. The condylar occipital bone ossifies from two centers, one center for either side of the foramen magnum, and the basilar part ossifies from two centers as well. Ossification of the occipital bone may occur as early as the ninth week of gestation. There had been much debate regarding the development and ossification process in the past, but recent studies of the complex gene and molecule interactions involved have helped with clarification.[3]
Blood Supply and Lymphatics
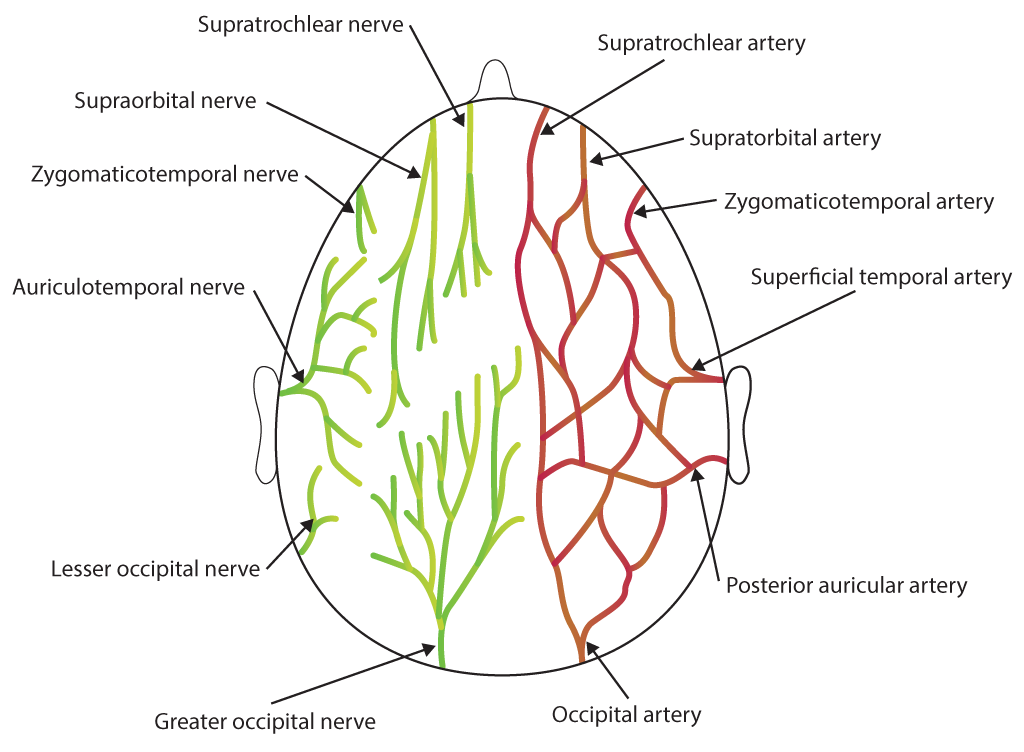
The occipital area receives its blood supply from the occipital artery, and the blood drains via the occipital vein. The occipital artery has its origin from the external carotid artery, where it is deep to the digastric posterior belly and the hypoglossal nerve winds around it. It travels superiorly and posteriorly, passing superficially to the internal carotid artery and the vagus nerve, before anastomosing with the deep cervical artery as it courses just beneath the mastoid process of the temporal bone. It then travels along the deep to the sternocleidomastoid and splenius capitis muscles until it reaches the occipital bone's superior nuchal line, where it then travels superficially to the semispinalis capitis muscle. After it has coursed about halfway across the semispinalis capitis and just lateral of the trapezius, the artery then courses vertically up the back of the head superficial to the occipital belly of the occipitofrontalis. It ascends tortuously up the head in the superficial fascia, anastomosing with a branch of the posterior auricular artery. Then at the crown of the head, it anastomoses with the parietal branch of the superficial temporal artery.
The occipital artery supplies blood to more than just the occipital area, as evidenced by its several branches, including the auricular, descending, meningeal, muscular, and sternocleidomastoid branches. The auricular branch supplies the area behind the ear, and a mastoid branch supplies the mastoid air cells, diploe, and dura mater. The descending branch is the largest division and contains a deep and superficial portion. The superficial portion provides blood to the trapezius, and the deep portion anastomoses with a branch of the costocervical trunk, providing collateral circulation via the external carotid and the subclavian artery. The meningeal branch supplies the posterior cranial fossa dura mater. The muscular branches supply several muscles along the course of the occipital artery, including the digastric and longus capitis muscles. The sternocleidomastoid branch divides at the carotid triangle into upper and lower branches and supplies the muscle it is named after.
The occipital vein originates from small vessels on the posterior aspect of the scalp and drains the superficial muscles and skin of the occipital region. It is superficial to the occipital fascia and the occipital artery and anastomoses laterally with the parietal branch of the superficial temporal vein and inferolateral to the posterior auricular vein. It then runs into the inferior portion of the posterior auricular vein, where it becomes the external jugular vein. The occipital vein also has an anastomosis with the intracranial confluence of the sinuses via the occipital emissary vein. The occipital lymph nodes are located posterior to the occipital artery and vein, with the occipital lymph vessels draining into the jugulodigastric lymph node, which then drains into the jugular lymph vessels.
Nerves
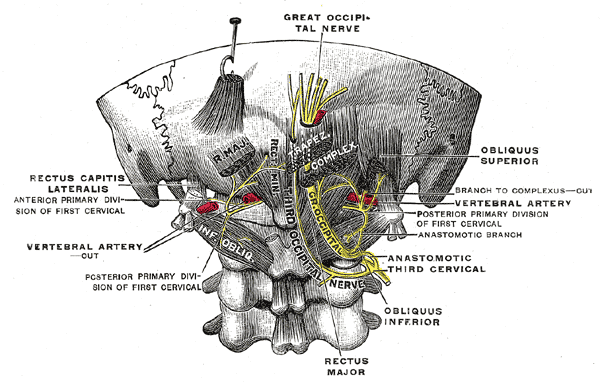
Sandwiching the occipital artery and vein is the lesser occipital nerve branch anteriorly and the greater occipital nerve branch posteriorly. The lesser occipital nerve, as well as the greater occipital nerve, branches off of spinal nerve C2 just as it passes directly inferior to the first cervical vertebra, carrying fibers originating from the ventral primary ramus. It supplies cutaneous innervation to the surface of the auricle posteriorly, as well as the adjacent posterior portion of the scalp.[4][5]
In contrast to the lesser occipital nerve, the greater occipital nerve carries fibers from the dorsal primary ramus of spinal nerve C2, specifically its medial branch. It innervates the skin of the posterior scalp and the muscles of the posterior neck, the multifidus cervicis muscle, and the semispinalis capitis muscle. It also contains pain and proprioceptive branches for the suboccipital muscles and meningeal branches to the posterior cranial fossa.
The posterior auricular nerve innervates the occipital belly of the occipitofrontalis muscle that covers much of the surface area of the occipital bone.
As mentioned above, the occipital bone contains the foramen magnum, through which the spinal cord and accessory spinal nerve travel along with several blood vessels.
Muscles
The occipital belly of the occipitofrontalis covers much of the occipital bone.[6] This muscle helps move the scalp, elevate the eyebrow, and wrinkle the forehead skin. Its origin is from the lateral two-thirds of the supreme nuchal line of the occipital bone (as well as the mastoid process of the temporal bone) and inserts at the epicranial aponeurosis. The occipital artery and vein supply blood flow and drainage, and the occipital lymph nodes and vessels drain lymph. The posterior auricular nerve innervates it; the facial nerve innervates the remainder of the occipitofrontalis.
Several muscles attach to the inferior part of the occipital bone, whose insertions were discussed in the “Structure and Function” section. The most medial and superficial of these is the trapezius, with its multiple origins, one of which is the external occipital protuberance. Its innervation and blood supply will not be discussed here.
Just deep and on either side of the vertebrae are the left and right semispinalis capitis muscles, serving to extend and flex the cervical and thoracic spine and head laterally. These muscles are innervated by the dorsal primary rami of spinal nerves C3 to T6 and receive blood from the posterior intercostal arteries, the deep cervical artery, and the lumbar arteries.
Deeper still are the left and right rectus capitis posterior minor muscles, which help extend the head. Lateral of the rectus capitis posterior minor muscles are the rectus capitis major muscles, which help with ipsilateral rotation and head extension. Lateral and superficial to the major rectus capitis is the obliquus capitis superior muscle, which serves the same function as the former. The rectus capitis posterior minor, posterior major, and obliquus superior muscles are all innervated by the suboccipital nerve and blood supplied by the occipital artery.
The most lateral muscle of the occipital bone is the rectus capitis lateralis, serving to flex the head laterally. This muscle receives innervation from the spinal nerves C1 to C2 and receives arterial supply via the deep cervical artery. The longus capitis and the rectus capitis anterior muscles are anterolateral and anteromedial muscles of the occipital bone, whose function is to flex the head and neck.
The cervical plexus innervates the longus capitis, and the ventral primary rami of the spinal nerves C1 to C4 and receive arterial flow from the deep cervical artery. The rectus capitis anterior receives its nerve supply from the ventral primary rami of the spinal nerves C1 and receives arterial flow from the ascending cervical artery.
Physiologic Variants
The occipital emissary vein may not be present in all individuals, and it may only pass through a singular condylar canal, or through multiple, smaller clustered canals.[7]
The jugular tubercle on the upper surface of the lateral condylar part of occipital bone may sometimes have an oblique groove for cranial nerves IX, X, and XI.
The occipital artery may sometimes branch to give the mastoid artery; most of the time, this artery arises from the auricular branch of the occipital artery.
Cerebral dural sinus venous blood flow in the torcular Herophili, also known as the confluence of the sinuses, on occipital bone’s inner surface is variable.[8] It categorizes into four types based on the continuity between the transverse sinus grooves and the superior sagittal sinus grooves. In descending order of frequency, these types are the right dominant type, confluence type, bifurcation type, and left dominant type.[9]
Surgical Considerations
See lacerations below in clinical significance.
Clinical Significance
Deep lacerations to the occiput and scalp, in general, are inclined to bleed profusely for several reasons:
- The firm adherence of the dense connective tissue to the blood vessels prevents vasoconstriction.
- The pulling effect of the occipitofrontalis muscle prevents the closing of the actively bleeding vessel and the surrounding skin.
- There are numerous anastomoses of the scalp blood vessels, such as the anastomosis of the occipital and the posterior auricular veins.
The scalp veins may be used for venous catheterization as they offer easy access with little risk, with the occipital vein being among the most commonly used. Scalp catheterization is utilized in infants and neonates after unsuccessful attempts at cannulation of extremity veins as the scalp veins in this population have less overlying subcutaneous fat and are more prominent compared to other peripheral sites, and they are less obscured by hair, providing easier visualization and cannulation.[10]
The ‘danger area of the scalp’ refers to the layer of loose areolar connective tissue as it contains the valveless emissary veins that connect the superficial veins in the subaponeurotic space with the intracranial venous sinuses. Although not always present, the occipital emissary vein connects the occipital vein to the confluence of the sinuses. This connection makes it possible for an infection to spread from the occipital scalp to the meninges.
Since the abducens nerve runs near the clivus of the basilar part of the occipital bone, increased intracranial pressure may trap the nerve at this point, causing abducens palsy. The clivus also serves as a critical landmark for ensuring anatomical atlanto-occipital alignment on cervical spine x-rays.
Occipital trauma may cause a basilar skull fracture, which would present with ecchymosis behind the ears, or “battle sign.” If occipital bone surrounding the foramen magnum is fractured, there is a higher risk of damage to the exiting blood vessels and nerves described above.
During delivery, it is crucial to identify the location of the fetal occiput. Several genetic disorders may present with a prominent occiput, the most common of which is trisomy 18, or Edwards syndrome. This condition is important to identify because of its association with heart (most commonly VSDs and ASDs) and renal defects, among others, and survival beyond one year of life is rare, although many of the afflicted will not make it to birth. Other signs that would be indicative of Trisomy 18 are microcephaly, micrognathia, low-set and malformed ears, and rocker bottom feet. It is associated with omphalocele.