Continuing Education Activity
Drug-induced pigmentation represents a complex issue for patients who are prescribed certain medications. These medications may include NSAIDs, tetracyclines, antimalarials, heavy metals, etc. This activity reviews the etiology, epidemiology, pathophysiology, and treatment for drug-induced pigmentation. This activity will present an overview of the etiology, clinical findings, and potential therapeutic factors that are important for members of the interprofessional team in the treatment of patients with drug-induced pigmentation.
Objectives:
- Identify the etiology of drug-induced pigmentation.
- Review the history and physical exam of a patient with drug-induced pigmentation.
- Summarize the treatment and management options available for drug-induced pigmentation.
- Outline interprofessional team strategies for improving care coordination and communication to advance drug-induced pigmentation and improve outcomes.
Introduction
Drug-induced pigmentation is a form of abnormal skin pigmentation that is caused by drugs through several different mechanisms. Several drugs have associations with pigmentation, including cytotoxic agents, analgesics, anticoagulants, antimicrobials, antiretrovirals, metals, and antiarrhythmic, etc. Various causes can contribute to the pigmentation that may involve an accumulation of melanin synthesis or even the synthesis of particular substances. Histological findings are relatively diverse but can include substances that are primarily within the dermal macrophages. Diagnosing a patient with drug-induced pigmentation can be difficult, as it is essential to rule out other conditions that may be leading to the skin findings.
Additionally, it is especially difficult to make the diagnosis in patients on multiple drugs. The recommendation is to perform a complete medical history, along with a thorough skin examination on the patient. The hope is that there will be more research on the specific effects of drug-induced pigmentation and potential treatment options.
Etiology
Drug-induced pigmentation is the diagnosis when the pigmentation is temporally associated with drug use, and other potential causes have been ruled out. Several drugs can cause pigmentation from antimalarials to antiretrovirals. Therefore, clinicians should be vigilant in examining a patient’s full medical history to determine the specific drug that appears to be causing the patient’s symptoms.[1]
Epidemiology
The incidence of drug-induced pigmentation is difficult to ascertain because of a lack of reported cases and a dearth of information from patients regarding their treatment. However, estimates are that about 20% of cases of pigmentation are thought to be drug-induced. No significant differences between gender, age, and racial groups have been noted, although individuals with darker skin may display more severe hyperpigmentation.[2] More prospective studies investigating this issue are needed.[1][3]
Pathophysiology
The pathophysiology of drug-induced pigmentation is thought to involve several different mechanisms. It could be due to the accumulation of melanin (e.g., antimalarials), either by a direct trigger of the medication or nonspecific inflammation caused by the drug. This form of pigmentation is worsened by sun exposure, explaining patients’ worsened pigmentation in sunny areas. Additionally, the drug itself can accumulate and cause pigmentation. The drug can remain within dermal macrophages and even undergo chemical changes to newer types of particles, as exhibited by gold complexes. Finally, the last two mechanisms for drugs that can cause pigmentation involves the synthesis of new pigment (lipofuscin) or accumulation of iron (minocycline).[4] The latter is thought to involve damaged blood vessels and lysis of red blood cells.[3]
History and Physical
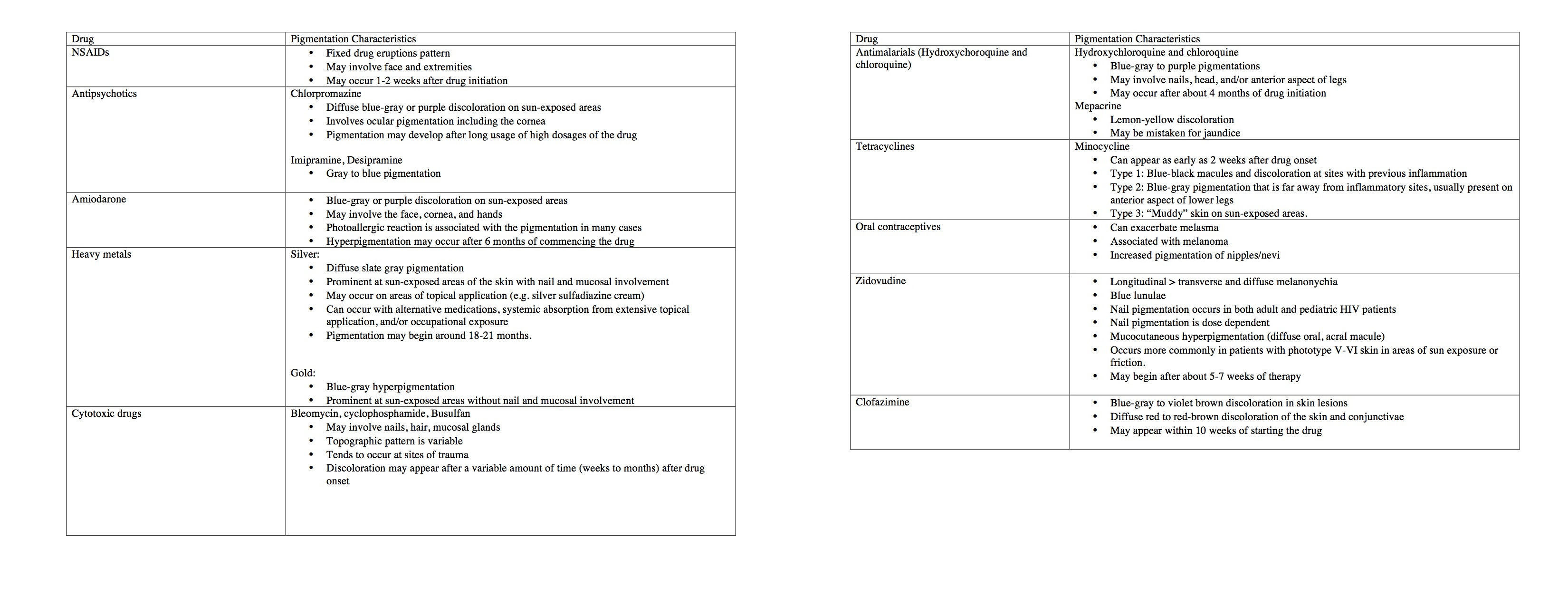
In regards to clinical findings, drug-induced pigmentation varies from other causes of pigmentation. The most crucial distinction is that when the treatment with the drug stops, the pigmentation also begins to fade. For example, with the discontinuation of paclitaxel, the pigmentation also resolves shortly thereafter.[5] The discoloration associated with drug-induced pigmentation also tends to have a slower occurrence, with gradually worsening over months to a year. Moreover, particular drugs may have specific patterns of pigmentation. For example, NSAIDS typically involve fixed eruptions, whereas psychotropics are known for presenting with a blue-gray appearance and are related to sun exposure. Certain drugs are also associated with nail pigmentation. For example, antimalarials are more likely to cause nail beds that have transversal bands, whereas cytotoxic drugs such as cisplatin are more likely to present with longitudinal pigmented bands.[3] See the table for an overview of the characteristic pigmentation findings associated with particular drugs.
Evaluation
When evaluating whether a patient has pigmentation related to medication use, it is crucial to take into consideration several points. First, it is vital to take a thorough medical history of the patient, which involves noting all the medications the patient is taking and carefully evaluating any that have pigmentation-related side effects. Common drugs that are known to cause pigmentation include NSAIDS, antimalarials, amiodarone, anticoagulants, antimicrobials, antiretrovirals, and tetracyclines. Additionally, a provider should note when the pigmentation starts and if there are any changes, such as increased or decreased intensity, after altering the usage of the drug. For example, amiodarone-induced pigmentation exhibits a dose-dependent relationship in regards to its appearance.[6]
Treatment / Management
Initially, if there is another drug that can substitute as therapy for the patient’s condition, then that should be a consideration. If that is not possible, an effective approach involves reducing the dosage of a drug. Some drugs such as amiodarone have a dose-dependent correlation with the amount of discoloration experienced.[3] In these cases, decreasing the intake of a drug can dramatically reduce the dyschromia present. Additionally, specific drug-induced pigmentation is avoidable by limiting sun exposure. These drugs include antimalarials, psychotropic, amiodarone, and tetracyclines.[3] In these cases, patients should receive counsel on proper outside wear, such as sunglasses and protective, covered clothing. If the suggestions mentioned above failed to work, there are also some topical and laser treatments available. However, the efficacy of these treatment methods remains elusive.
Differential Diagnosis
Several pigmentation-related skin conditions should merit consideration before a diagnosis of drug-induced pigmentation is made. Melasma can present as a light, dark brownish discoloration. Addison disease usually involves pigmentation of the oral mucosa. Blue nails are one of the characteristic findings of Wilson disease, which also includes visceral involvement of other organs such as the liver. Vitamin deficiencies, such as niacin, can present with pellagra and the classic triad of dementia, diarrhea, and dermatitis.[7] Finally, Kaposi sarcoma should be on the differential for HIV-infected individuals.
Prognosis
The prognosis of the pigmentation is generally good, but extra-dermal manifestations of the pigmentation may exacerbate it. For example, hydroxychloroquine may cause pigmentation of the oral mucosa, and minocycline can cause pigmentation of heart valves.[8][9] Otherwise, drug-induced pigmentation does not correlate with increased mortality. There may be psychological or social impacts depending upon the individual patient.
Complications
The complications and associated symptoms of the pigmentation depend on the specific drug. NSAIDs are known to cause fixed drug eruptions, most probably through a hapten-type interaction. Antimalarials, amiodarone, and antipsychotics involve blue to gray discoloration in various areas from the face to the lower extremities. Anticonvulsants can cause brown-gray discoloration that resembles melasma. The pigmentation can also deposit in other areas such as the nails (antimalarials and minocycline). Antipsychotics, antimalarials, and amiodarone can even lead to corneal pigmentation.[3]
Deterrence and Patient Education
Patient education is vital in all stages of managing drug-related pigmentation from diagnosis to treatment. Obtaining a thorough medical history is crucial for making a diagnosis of drug-induced pigmentation. Therefore, it is necessary that patients provide a full, accurate history regarding their past and current medication use. Additionally, when removing or adjusting the medication used for treating drug-induced pigmentation, it is essential that the patient correctly understand the new regimen of the medication to avoid further exacerbation of the pigmentation caused by the previous drug usage. For drugs that are associated with sun exposure, patients should understand the importance of sun protection.[10]
Enhancing Healthcare Team Outcomes
A coordinated effort is especially needed when it comes to managing drug-induced pigmentation. Dermatologists need to work with patient’s other specialists come up with the best medication or dosage to avoid the pigmentation-related symptoms as much as possible. Moreover, future medical providers should be aware of the patient’s history of drug-relate pigmentation so that they can be mindful of the issue when prescribing new medications.
Addressing pigmentation secondary to drug therapy requires an interprofessional team approach, including physicians, specialists, specialty-trained nurses, and pharmacists, all collaborating across disciplines to achieve optimal patient results. [Level V]