Introduction
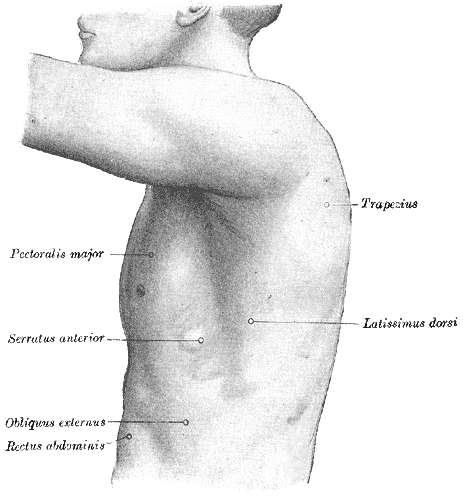
The latissimus dorsi is a broad, flat muscle occupying most of the lower posterior thorax (see Image. Surface Anatomy of the Thorax). The muscle's primary function is to move the upper extremity, but it is also considered an accessory muscle of respiration. Due to this muscle's broad attachment to several vertebral spinous processes and the thoracolumbar fascia, ongoing research looks at what role the muscle plays in trunk movement. Currently, the evidence is mixed on how much influence this muscle has on spine extension, lateral flexion, or rotation. Even though the muscle has a broad attachment to the trunk and strong actions on the humerus, using this muscle for surgical transposition appears to have a limited reduction of normal function.[1][2][3][4]
Structure and Function
The latissimus dorsi is considered a muscle contributing to both thoracic and brachial (i.e., arm) motion. The muscle has attachments to the lower six vertebral spinous processes anterior to the attachment of the trapezius. Through direct attachment and the thoracolumbar fascia, the latissimus dorsi attaches to a variable number of the lumbar and sacral spinous processes (T6 to S5 levels) and the supraspinous ligament. Other muscle attachments include the posterior iliac crest, lower three to four ribs, where it interdigitates with the external oblique muscle, and the inferior angle of the scapula.
The muscle fibers are situated in various orientations, with the superior-most fibers almost horizontally oriented and the inferior fibers more vertically oriented on the thorax. As the muscle fibers extend toward the axilla, the fibers wind around the anterior aspect of the teres major muscle to insert as a flat tendon on the floor of the intertubercular sulcus. As the fibers coalesce to insert on the humerus, the fascicles twist around each other such that the most superior fibers to the midline insert on the lowest part of the sulcus and the lower fibers to the midline insert higher in the sulcus. The latissimus dorsi attachment on the intertubercular sulcus extends further superiorly than does the attachment of the teres major on the lateral lip of the sulcus.
Through the anterior attachment on the humerus, the latissimus dorsi acts with the teres major and pectoralis major muscles to adduct and medially rotate the humerus. The latissimus dorsi, along with the teres major, is active in the extension of the humerus. Extension and adduction are strongest when the motion is started from a position of partial flexion or abduction or a combination of the two motions. The muscle is active in moving the trunk anterior and superior when the upper extremities are fixed overhead, as in climbing or performing an activity such as a chin-up. Research has demonstrated that the latissimus dorsi is also active during deep inspiration and with forceful respiratory functions such as coughing and sneezing.
Embryology
The latissimus dorsi is considered an extrinsic muscle of the back, meaning it is a muscle that originates from the myogenic cells in the developing upper limb buds rather than from the myotomal dorsal epaxial division of the somite where the intrinsic (deep back) muscles take origin. The latissimus dorsi and teres major muscles, embryologically, are closely related as they both originate from the pre-muscle sheath of the arm. Unlike teres major, which develops in the limb bud, latissimus dorsi spreads across the posterior aspect of the thorax and trunk as the myoblasts migrate out of the limb bud into the axial mesenchyme posteriorly. It is not until an embryo is at least 20 mm long that the fibers of latissimus dorsi reach the iliac crest, whereas teres major is already well-developed by the time an embryo is 14 mm in length.
Blood Supply and Lymphatics
The latissimus dorsi muscle is supplied predominantly by the thoracodorsal artery, a continuation of the subscapular artery, which is a branch of the third part of the axillary artery. The thoracodorsal artery and its venae comitantes enter the muscle at a single point on the anterior surface of the muscle, 6 cm to 12 cm from the bifurcation of the subscapular artery and 1 cm to 4 cm medial to the lateral margin of the muscle. In addition to the thoracodorsal artery, the latissimus dorsi also receives blood supply from the dorsal perforating branches of the inferior three posterior intercostal arteries and the superior three lumbar arteries.
The lymphatic drainage of this muscle follows the typical pattern of lymphatic drainage with superficial and deep lymphatics, which will drain into the posterior group of six to seven axillary lymph nodes positioned along the subscapular vessels on the inferior edge of the posterior axillary wall. The afferent lymphatic vessels to these nodes drain the skin and superficial muscles from the inferior portion of the neck to the iliac crest. Efferent vessels from these nodes drain into the apical and central axillary nodes.
Nerves
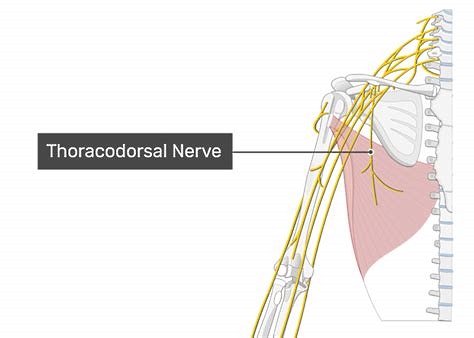
The thoracodorsal nerve, a branch of the posterior cord of the brachial plexus (C6 to C8 with C7 predominant), provides innervation to the latissimus dorsi. The nerve will travel in the neurovascular bundle with the thoracodorsal artery and its associated veins. The branching of the artery and nerve are closely related. See Figure. The Thoracodorsal Nerve.
Muscles
The latissimus dorsi works collaboratively with the teres major and pectoralis major to perform actions of the upper extremity. Together, these muscles will work to adduct, medially rotate, and extend the arm at the glenohumeral joint. Muscle testing of the latissimus dorsi muscle occurs in a prone position with the arm adducted and fully extended with the elbow extended. Resistance is applied to the forearm into the abduction and slight flexion.
If the latissimus dorsi is short or tight, the back will extend and rotate as the upper extremity is flexed into an overhead position, as in reaching for an object on a high shelf. The accommodation of extension and rotation of the spine allows for the achievement of the overhead position of the upper extremity.
Physiologic Variants
Several variants of the latissimus dorsi may occur. A muscular arch may exist between the axillary border of the latissimus dorsi extending anteriorly to the axillary vessels and nerves and joining with the tendon of the pectoralis major, coracobrachialis, or the fascia of the biceps brachii. Also, a fibrous connection may exist between the tendon of the latissimus dorsi near its insertion site and the long head of the triceps brachii. Other variations may occur, but the listed ones are the most common.
Surgical Considerations
The latissimus dorsi is frequently used as a myocutaneous flap for reconstructive surgeries. It has been used for chest wall and post-mastectomy reconstruction surgery and as early as 1978 for head and neck reconstruction surgery. The advantages of using this muscle for reconstructions include the long vascular pedicle, large volume of tissue, and minimal donor site morbidity, to name a few. Minimal functional losses in adduction or medial rotation are associated with using this muscle for reconstructions as long as the other muscles associated with those movements remain intact. However, if the patient requires shoulder mobility and latissimus dorsi muscle function for ambulation with crutches or using a wheelchair, loss of the latissimus dorsi muscle could lead to non-desirable functional limitations in mobility.[5][6][7][8]
Clinical Significance
The latissimus dorsi may be implicated in patients with restrictions of shoulder motion of abduction, flexion, and lateral rotation. Assessment of this muscle is crucial for patients with upper extremity pathology. Proper function and coordination with the teres major and pectoralis major muscles are essential for smooth and fluid movements of the upper extremity. For patients with low back pain, it is important to assess the length and flexibility of the latissimus dorsi due to the attachments on the spine and pelvis. A decrease in length or an increase in stiffness of this muscle can lead to alterations in movement patterns and/or postures which can exacerbate low back pain.
The latissimus dorsi is implicated in posterior shoulder dislocations following seizures or electrical shocks/electrocutions. The powerful internal rotators of the arm (the latissimus dorsi, the pectoralis muscles, and the subscapularis) overpower the external rotators, causing internal rotation of the shoulder with posterior and superior displacement.[9]