The Ross procedure, or the switch or pulmonary autograft procedure, is a cardiac surgery in which a diseased aortic valve is replaced with the patient's pulmonary valve. This is followed by replacing the pulmonary valve with a pulmonary allograft. The Ross procedure was first developed in the late 1960s and has been performed many times. It is the only operation that allows for an aortic valve replacement with a living valve substitute. This activity describes the indications, contraindications, and steps involved in the Ross procedure and highlights the interprofessional team's role in managing patients with aortic valve disease.
Objectives:
Identify the indications for the Ross procedure.
Assess the technique involved in performing the Ross procedure.
Evaluate the complications associated with the Ross procedure.
Communicate the role of the interprofessional team is to provide effective care and surveillance of patients undergoing the Ross procedure.
Introduction
The Ross procedure, also known as the switch procedure, is a cardiac surgery procedure in which the diseased aortic valve is replaced with the patient's pulmonary valve, followed by the replacement of the pulmonary valve with a pulmonary homograft. Sometimes, some children and infants need aortic valve replacement for various reasons. However, inserting a prosthetic valve is not a good option; firstly, there are no small-sized aortic valves available, and secondly, since the child grows, the prosthetic valve remains the same size and leads to symptoms of left ventricular outflow obstruction tract. In addition, some people do not want to take oral anticoagulant medications for life and hence a Ross procedure would be ideal for them. Unlike a prosthetic valve, the Ross procedure has excellent hemodynamics, and the risk of embolic complications is almost zero. Finally, as the child grows, so does the valve. Unfortunately, it is now realized that the Ross procedure also has limitations; the pulmonary homograft develops regurgitation or stenosis after 15-20 years, necessitating another procedure. The Ross procedure was first developed in the late 1960s and has been performed many times since then. It remains the only operation that allows for an aortic valve replacement with a living valve substitute.[1] Over the years, the original procedure has been gradually modified to perfect the surgical outcome, but the main principles outlining the procedure remain. This chapter details the anatomy of the aortic valve, indications, contraindications, equipment, personnel, preparation, technique, complications, and clinical significance of the Ross procedure.
Anatomy and Physiology
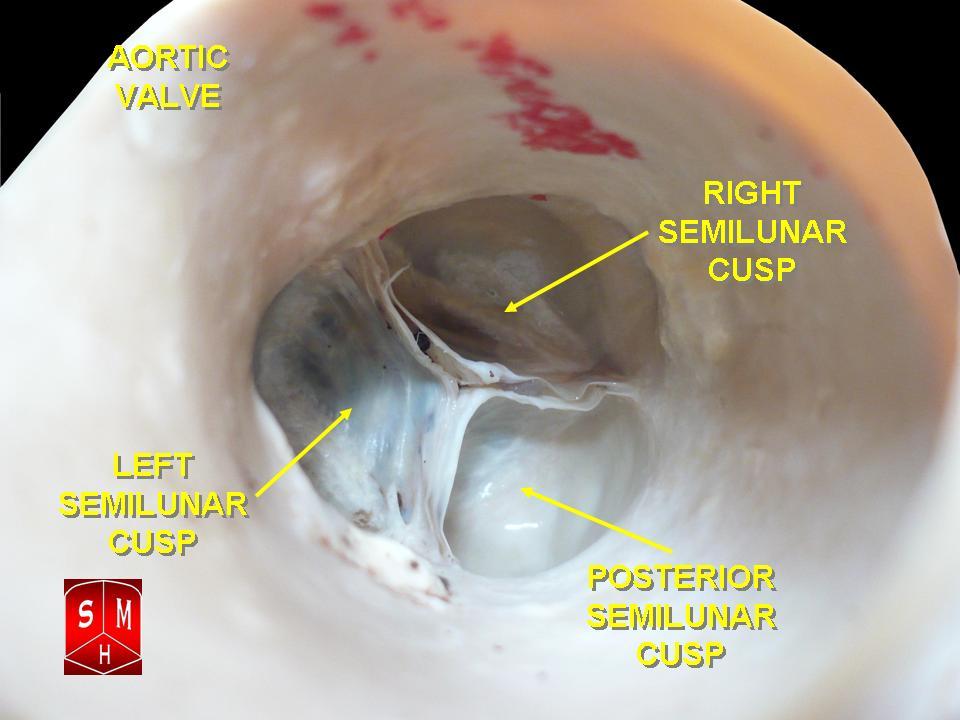
Four chambers comprise the heart. The superior 2 chambers are the right and left atria, while the bottom 2 chambers are named the right and left ventricles. Atrioventricular valves separate the atria and ventricles. There are 2 semilunar valves: the pulmonic valve separates the right ventricle and the pulmonary artery. In contrast, the aortic valve separates the left ventricle and the aorta (see Image. The Aortic Valve). The right side of the heart pumps blood at a lower pressure into the pulmonary vasculature to be oxygenated. The left side of the heart pumps blood in the systemic circulation at a much higher pressure. Therefore, the valves on the left side of the heart are subject to higher pressures. During the Ross procedure, it is critical to know the anatomy of the left main coronary artery and its take-off. In addition, the surgeon should know the course of the left coronary artery, its proximal septal branches, and their relationship to the aortic root and the right ventricular outflow tract. In addition, when harvesting the pulmonary autograft, the surgeon should have an appreciation of the subpulmonary conal musculature to facilitate the dissection. Finally, if the left ventricular outflow tract needs enlargement (Ross Konno procedure), the surgeon must be familiar with the location of the conduction system.
Indications
Indications for the Ross procedure include:
Aortic valve disease in children with congenital aortic stenosis (most common indication)
Females of childbearing age wanting to bear children in the future with bicuspid aortic valve and small aortic annulus
Some variations of left ventricular outflow obstructive disease
Native or prosthetic valve endocarditis, depending on the extent of the disease
Some forms of adult aortic regurgitation with a dilated aorta
Severe forms of aortic valve disease are not amenable to repair[2][3]
Contraindications
Absolute contraindications for the Ross procedure include:
Relative contraindications for the Ross procedure, due to a higher risk of autograft dysfunction, include:
Rheumatic valve disease
Dysplastic dilated aortic root
Equipment
Before the procedure, an echo should assess the aortic valve, the left ventricular outflow tract obstruction, and any other cardiac abnormality. The pulmonary valve should also be assessed for stenosis or regurgitation. Echocardiography also allows for sizing the aortic and pulmonary annulus. If the aortic annulus is smaller than the pulmonary annulus by 2-3 mm, the surgeon may be required to perform an aortic root enlargement procedure. See Video. Aortic Valve Movement.
The Ross procedure is performed via a median sternotomy under cardiopulmonary bypass. The postoperative course is the same as for any other open-heart surgery patient. Patients are usually weaned off the ventilator the same night and extubated in the morning.
Personnel
For a successful, safe procedure, a trained cardiothoracic surgeon, anesthesiologist, cardiologist, imaging specialist, surgical assistants/nursing, scrub/operating room technicians, and ancillary staff are recommended.
Preparation
The primary goal in preparation for the Ross and any other surgical procedure is to achieve sterility. This means the chest needs to be shaved and sterilized, followed by the placement of sterile drapes to allow access to the surgical field only once the opening of the chest during the procedure has occurred. The Ross procedure is conducted under general anesthesia; therefore, pre-anesthetic evaluation and intubation are utilized to maintain the airway and sedation. Depending on the center and the operator, pre-operative and perioperative transesophageal echo may be performed.
Technique or Treatment
Following a median sternotomy, the Ross procedure begins with standard exposure of the heart and the aorta, followed by establishing cardioplegia and initiation of cardiopulmonary bypass. The ascending aorta is opened transversely about a centimeter above the origin of the right coronary artery. The aorta is opened, and the aortic valve is inspected. In some cases, the valve may be repaired. If repair is impossible, the pulmonary artery is opened, and the valve is inspected to ensure normal anatomy. If the decision is made to proceed with the Ross procedure, the aorta is separated from the aorta, the diseased aortic valve is excised, and the coronary buttons are prepared. Next, the pulmonary valve is excised.
The main pulmonary artery is opened transversely proximal to the bifurcation if no abnormalities are present. The pulmonary valve is then inspected for anomalies. Again, the valve replacement is performed using the full root approach if no abnormalities exist. The full root approach is most commonly used about 90% of the time because it has the lowest risk of pulmonary autograft failure.[2] Depending on the anatomy, another approach may be better in rare circumstances, such as the sub-coronary, sub-coronary with retained noncoronary sinus, or cylinder approaches. In this topic, we describe the full root approach because it is the most commonly used method. The full root approach is begun by moving the root out of the surgical plane and pushing it upwards. The posterior pulmonary artery root is cut to the muscle to visualize the right ventricular outflow tract through the incision. Next, the pulmonary artery is separated from the aorta, and a clamp designates the most proximal area to the pulmonary valve. The surgeon must be aware of the left anterior descending coronary artery and the first septal while dissecting on the lateral side.
In the next step, an opening into the right ventricular outflow tract is created, dividing the anterior right ventricle and partially scoring the right ventricle's posterior muscle. Following this, the pulmonary artery root is excised and separated. Next, removing the aortic valve and root occurs after carefully cutting out the ostia with buttons from the native aorta. Once the pulmonary valve is removed, it is sized and prepared for implantation into the aortic root. Now the pulmonic autograft is anastomosed to the LVOT, followed by reimplantation of the right and the left coronary arteries onto the autograft, followed by proximal anastomosis of the pulmonic autograft, and hemostasis is secured.A cryopreserved pulmonary homograft is then trimmed as needed and implanted into the pulmonary root. After weaning from cardiopulmonary bypass, a transesophageal echocardiogram is done to assess the function of the autograft and the homograft.[4] Before discharge, an echocardiogram is repeated to ensure that both the aortic and pulmonary valves function normally. Patients are then examined every 4-6 weeks with echos. It is important to cover patients with antibiotics before any procedure.
Complications
Potential complications with the Ross procedure include:
Complications related to surgery occur in 3-5% of patients, with early mortality of 1-3%. In experienced centers, the mortality rates are negligible. Long-term survival of 80-90 % has been reported at 10 years and 70-80% at 20 years. Early autograft failure is rare but does occur within the first 6 months. In most cases, the cause is technical problems such as leaflet injury or distortion caused during the valve harvesting. The pulmonary homograft in most series lasts about 15-20 years and then develops regurgitation or stenosis due to calcific degeneration. However, today, the percutaneous placement of a pulmonary valve is being performed instead of open-heart surgery.
Undoubtedly, the Ross procedure is superior to the prosthetic valves. Unfortunately, recent data show that in some patients, there is increasing enlargement of the new aortic root following the Ross procedure, leading to aortic regurgitation, especially when there was a mismatch of the aortic and pulmonary roots at the time of the initial surgery. Patients who undergo the Ross procedure do not require anticoagulation and have minimal restrictions on their lifestyle. They are also able to participate in exercise programs without limitations. However, the Ross procedure is demanding, and lifelong monitoring of the patients is required. Reoperations have been infrequent, and with the availability of percutaneous valve implantation techniques, the morbidity of REDO open heart surgery can be avoided.
Clinical Significance
Multiple studies have shown a durable, long-term clinical success from this procedure with an extremely low mortality rate. Because this procedure uses biological valves, it obviates the need for oral anticoagulation, which would have otherwise been necessary for this particular group of patients, who would have needed mechanical valves.[6] The Ross procedure also eliminates the need for aortic valve replacement for up to 20 years. This is probably due to 2 factors. One is that the autographed pulmonary valve in the place of the aortic valve can grow as the patient grows, and the second is that there are lower pressures on the right side of the heart, creating less stress on the pulmonary valve replacement. Subsequently, this leads to a reduced failure rate. This procedure is an excellent option for children and youth to improve survival. It remains the only operation that allows for an aortic valve replacement with a living valve substitute.
Enhancing Healthcare Team Outcomes
The Ross procedure is major cardiovascular surgery. Therefore, utilizing an interprofessional team working across disciplines is imperative to care for these patients. The enthusiasm for this procedure has varied over the last several decades, with studies demonstrating lower mortality, bleeding, thromboembolism, and endocarditis compared to mechanical valve replacement but with the need for a higher risk of reintervention of the auto and allograft valves because of structural deterioration. Further, operator experience and expertise are essential for achieving excellent clinical outcomes, and therefore, this procedure should be performed at high-volume centers of excellence. A team of cardiac surgeons, cardiologists, cardiac nursing specialists, and specialty-trained cardiac pharmacists must coordinate evaluation, surgical care, and long-term postoperative follow-up to achieve the best outcomes. The nurses must assist with monitoring the patient post-operatively and long-term to identify potential complications early. The nurses must also assist the medical team in educating the patient and the family regarding expected outcomes and warning signs to watch for as well. The cardiac pharmacist should ensure that there is no potential for drug-drug interactions and that the surgical team leader appropriately doses medications during the perioperative period. Communicating potential risks to the medical team and the clinical pharmacist can help prevent adverse outcomes. Only a collaborative interprofessional team approach results in good long-term outcomes in patients undergoing the Ross procedure.
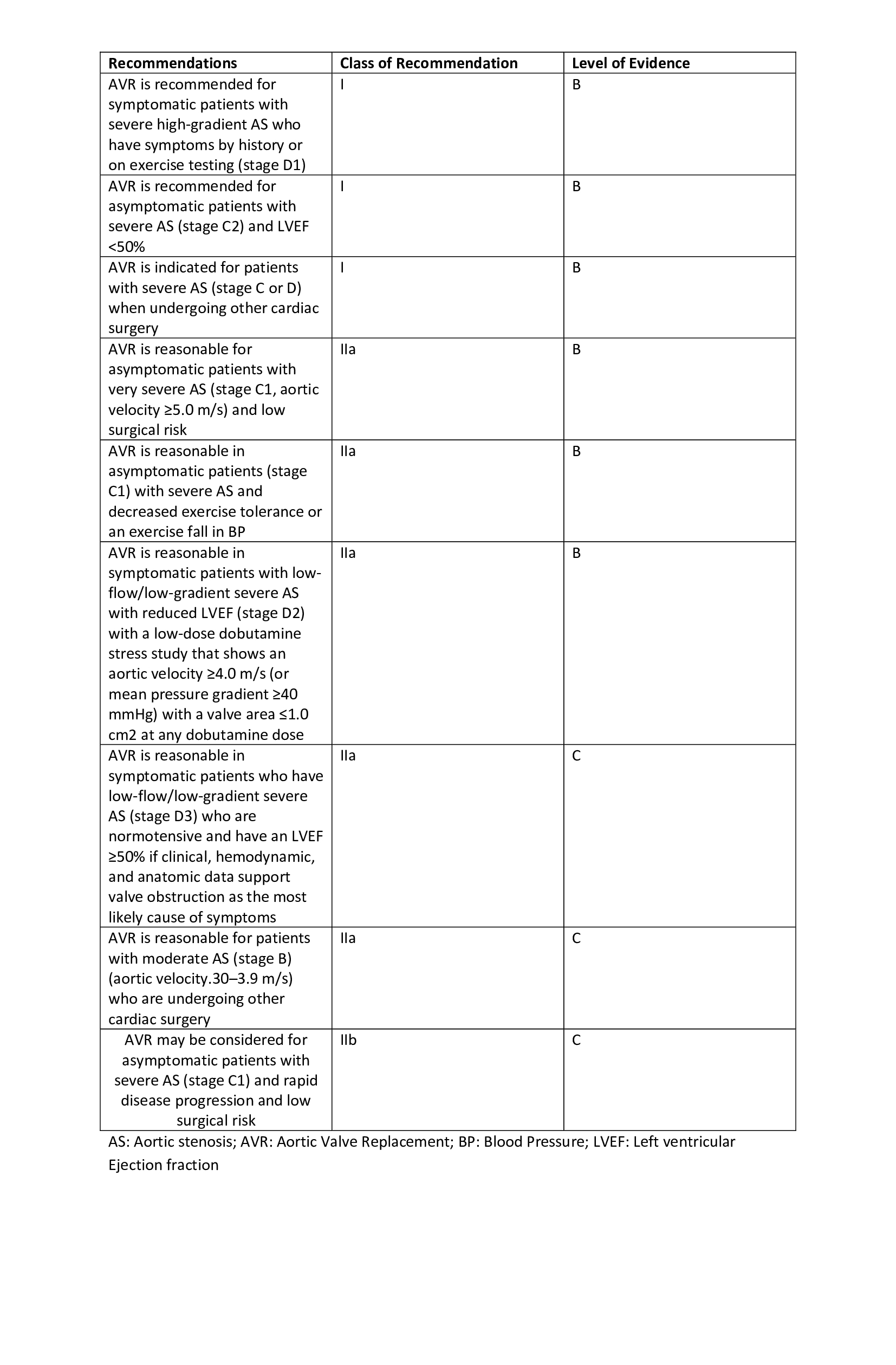
The American College of Cardiology/American Heart Association recommends Ross as a Class IIb. In contrast, the Society for Thoracic Surgeons recommends this as a Class III indication in patients needing aortic valve surgery (see Image. Recommendations for Aortic Valve Replacement). Because of the above recommendations, the utilization of the Ross procedure has been on the decline. The emergence of transcatheter valve replacements for degenerating bioprosthetic valves, which in the case of the Ross procedure are the auto and allografts, are easily replaceable without the need for open-heart surgery. In the future, this may provide a new lease of life for the Ross procedure.[7][8][9][10]
(Click Image to Enlarge)
The Aortic Valve. The aortic valve resides centrally between the ascending aorta and the left ventricular outflow tract.
<p>Valveguru, <a href="https://creativecommons.org/licenses/by-sa/3.0">Public Domain</a>, via Wikimedia Commons</p>
(Click Image to Enlarge)
Recommendations for Aortic Valve Replacement Table. The recommendations, classes of recommendations, and level of evidence for aortic valve replacement are detailed in the table.
Mazine A, El-Hamamsy I, Verma S, Peterson MD, Bonow RO, Yacoub MH, David TE, Bhatt DL. Ross Procedure in Adults for Cardiologists and Cardiac Surgeons: JACC State-of-the-Art Review. Journal of the American College of Cardiology. 2018 Dec 4:72(22):2761-2777. doi: 10.1016/j.jacc.2018.08.2200. Epub
[PubMed PMID: 30497563]
Morita K, Kurosawa H. [Indications for and clinical outcome of the Ross procedure: a review]. Nihon Geka Gakkai zasshi. 2001 Apr:102(4):330-6
[PubMed PMID: 11344686]
Zakkar M, Bruno VD Mr, Visan AC, Curtis S, Angelini G, Lansac E, Stoica S. Surgery for Young Adults With Aortic Valve Disease not Amenable to Repair. Frontiers in surgery. 2018:5():18. doi: 10.3389/fsurg.2018.00018. Epub 2018 Mar 2
[PubMed PMID: 29564333]
Crowe ME, Rocha CA, Wu E, Carr JC. Complications following the ross procedure: cardiac MRI findings. Journal of thoracic imaging. 2006 Aug:21(3):213-8
[PubMed PMID: 16915066]
Bourguignon T, El Khoury R, Candolfi P, Loardi C, Mirza A, Boulanger-Lothion J, Bouquiaux-Stablo-Duncan AL, Espitalier F, Marchand M, Aupart M. Very Long-Term Outcomes of the Carpentier-Edwards Perimount Aortic Valve in Patients Aged 60 or Younger. The Annals of thoracic surgery. 2015 Sep:100(3):853-9. doi: 10.1016/j.athoracsur.2015.03.105. Epub 2015 Jul 14
[PubMed PMID: 26187006]
El-Hamamsy I, Bouhout I. The Ross procedure: time for a hard look at current practices and a reexamination of the guidelines. Annals of translational medicine. 2017 Mar:5(6):142. doi: 10.21037/atm.2017.01.64. Epub
[PubMed PMID: 28462222]
Morgan GJ, Sadeghi S, Salem MM, Wilson N, Kay J, Rothman A, Galindo A, Martin MH, Gray R, Ross M, Aboulhosn JA, Levi DS. SAPIEN valve for percutaneous transcatheter pulmonary valve replacement without "pre-stenting": A multi-institutional experience. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2019 Feb 1:93(2):324-329. doi: 10.1002/ccd.27932. Epub 2018 Oct 23
[PubMed PMID: 30351525]