Introduction
Anemia is defined by a deficiency in hemoglobin, causing decreased oxygen capacity within the blood. Many of these causes are iatrogenic, but some can be genetic, secondary to malignancy or chronic inflammation, impairment of globin chain synthesis or acquired forms. Genes that are involved in iron metabolism may also be responsible, causing severe congenital deficiencies in iron and sequestration of iron. Iron is then trapped within the mitochondria, forming a "ring" around the early red blood cell. It was not until the 1960s in which this became a known variant of anemia. These congenital diseases include sideroblastic anemia which can be either monosyndromic or polysyndromic (systemic expressivity).[1]
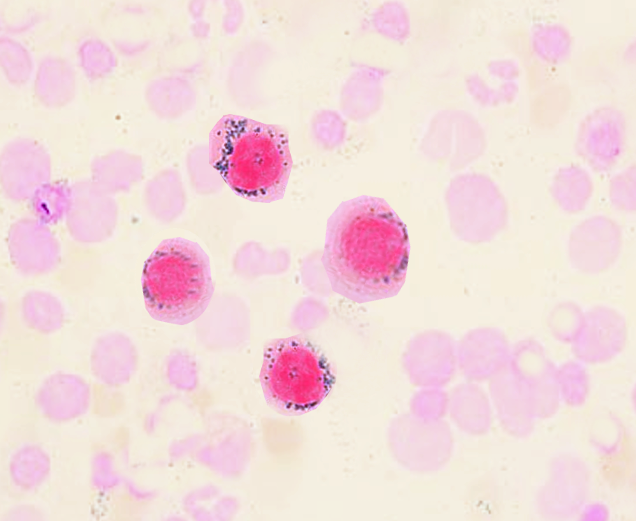
Refractory anemia with ringed sideroblasts is a version of myelodysplastic syndrome (MDS) which is characterized by anemia and the presence of >/= to 15% ring sideroblasts in the marrow. Generally, the patient presents with normochromic, normocytic anemia with overall erythroid hyperplasia.[1][2] Often, the level of hemoglobin is generally in the range of 9 to 12 g/dL, though lower levels may be present. The red blood cells may show dimorphism and populations can also show hypochromia. The platelets and neutrophils are hyperplastic with variable degrees of dyserythropoiesis and occasional megaloblastoid features. Granulopoiesis and megakaryocytopoiesis are normal findings and present within a majority of the cases.