Introduction
The hyoglossus muscle is one of the four intrinsic muscles of the tongue. It is a quadrilateral muscle that originates along the whole length of the hyoid bone and inserts into the side of the tongue. The hyoglossus acts to both depress and retract the tongue. It receives its motor innervation via the hypoglossal nerve. Its bloody supply is comprised mainly through the sublingual branch of the lingual artery with additional supply from the submental branch of the facial artery.
Structure and Function
Structure
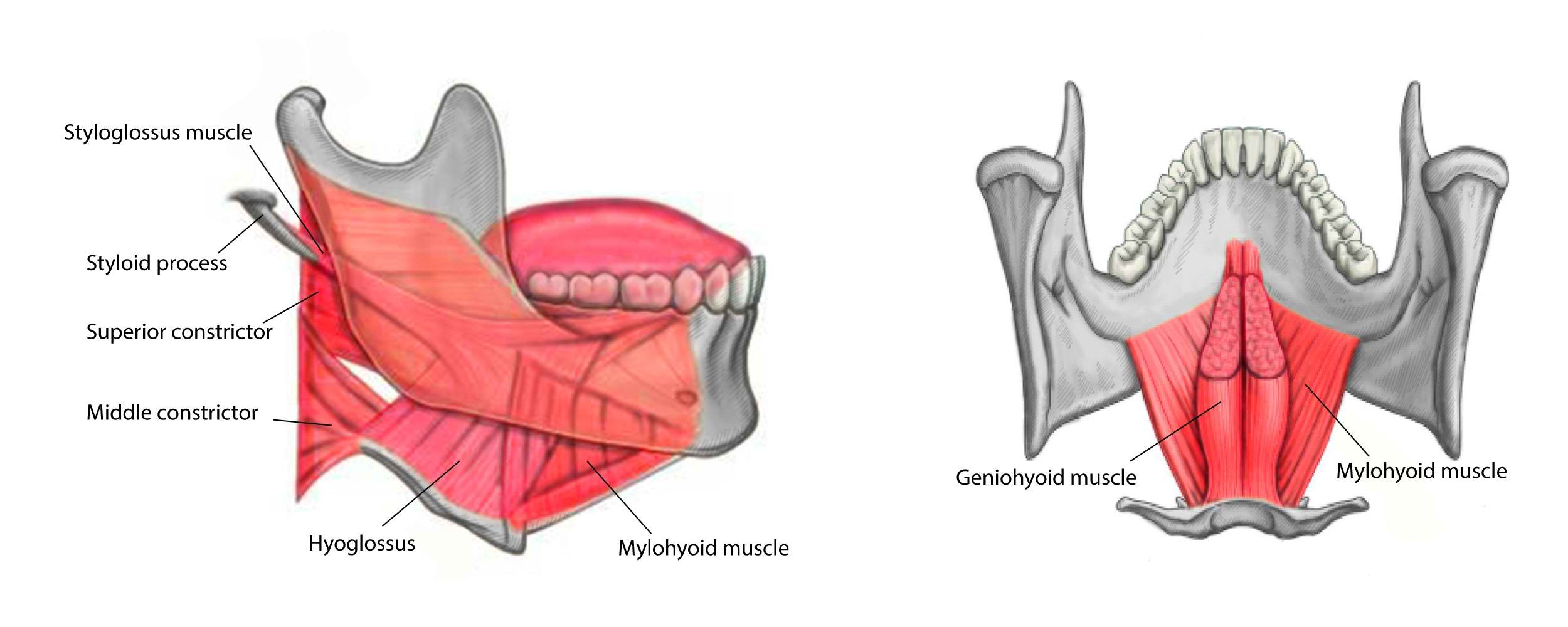
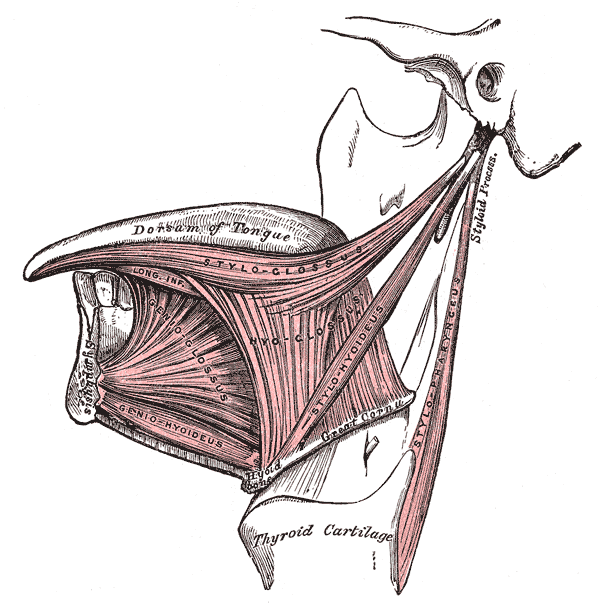
The hyoglossus muscle is one of the extrinsic muscles of the tongue. It is a thin, quadrilateral muscle that consists of two main parts. The anterior quadrilateral part arises from the hyoid body, and the posterior triangular part arises from the greater cornu of the hyoid bone. Both parts ascend towards the tongue external to the genioglossus. They insert into the side of the posterior half of the tongue between the styloglossus laterally and the inferior longitudinal muscle medially, with the posterior part attaching posteroinferiorly to the anterior part.
The anterior part is thicker than the posterior part and can be subdivided into 10 to 15 parallel bundles by the perimysium. Most of these bundles ascend in a posterolateral direction towards their insertion; however, the posterior internal slip of the anterior part diverges and merges into the insertion of the posterior part of the hyoglossus. In contrast to the anterior part, the posterior part is composed of 3 bundles, and instead of being parallel, these fibers converge towards their insertion. The fibers of these bundles all ascend in different directions, with the anterior bundle ascending posteriorly, the middle bundle ascending vertically and the posterior bundle ascending posteriorly.[1]
Function
The hyoglossus muscle is one of the four extrinsic muscles of the tongue, and, alongside the styloglossus, it acts as one of the two tongue base retractor muscles. The main action of the hyoglossus is to cause retraction and downward compression of the lower third of the tongue.[2] This action of tongue base retraction plays a key role during normal physiological swallowing as it aids bolus propulsion.[3] This control of tongue movement also plays a role in the articulation of speech.[4]
Embryology
The hyoglossus is a skeletal muscle and, like all skeletal muscles, derives from the dermatomyotomes of the paraxial mesoderm on both sides of the neural tube. At approximately day 25, the paraxial mesoderm starts to segment, forming structures known as metamers. This indicates the beginning of somite development which progresses along a craniocaudal gradient and in a symmetrical manner. This is what results in the adult body having symmetrical musculature and bones. By around day 32, more than 30 somite pairs are present, with 38 or 39 somite pairs being formed by the end of this process. These pairs can be split up into the following subdivisions:
- Occipital – containing 4 pairs
- Cervical – containing 8 pairs
- Thoracic – containing 12 pairs
- Lumbar – containing 5 pairs
- Sacral – containing 5 pairs
- Coccygeal – containing either 4 or 5 pairs
Of importance to the hyoglossus are the four occipital pairs as these develop into the occipital myotomes. The occipital myotomes move until they reach the floor of what will become the oral cavity. These myotomes go on to form the muscles of the pharynx and anterior neck, including the intrinsic and extrinsic muscles of the tongue, except for palatoglossus, which is derived from the fourth branchial arch. As the hyoglossus derives from the myoblasts originating in the occipital somites, it is innervated by the hypoglossal nerve (cranial nerve XII).
Blood Supply and Lymphatics
The hyoglossus muscle receives a dual blood supply. The main supply originates from the lingual artery, which is the third branch of the external carotid artery. The lingual artery gives rise to four main branches:
- The deep lingual artery
- The sublingual artery
- The suprahyoid branch
- The dorsal lingual branch
The sublingual artery branches off the lingual artery at the anterior border of the hyoglossus muscle and is the branch of the lingual artery that supplies the hyoglossus.
The other blood supply of the hyoglossus muscle comes from the fourth branch of the external carotid artery, the facial artery. As the facial artery leaves the submandibular gland, it gives off the submental branch. The significance of the submental artery in the hyoglossus’ blood supply varies due to the variability of the sublingual artery. In some specimens, it is seen that the sublingual artery anastomoses with the submental artery. However, sometimes the sublingual artery is completely absent, and in these cases, it is replaced with a branch of the submental artery.[5]
The venous drainage of the hyoglossus is through the lingual vein.
The lymphatic drainage of the hyoglossus is directly through the deep cervical group of lymph nodes.
Nerves
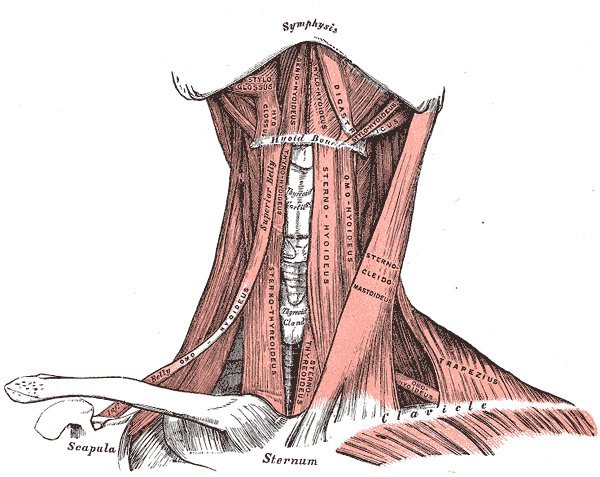
The hypoglossal nerve is the twelfth cranial nerve. It originates from the posterior portion of the medulla oblongata and exits the skull in the posterior fossa through the hypoglossal canal. It then descends between the sternocleidomastoid muscle, which lies superiorly, and the external carotid artery, which lies deep to the nerve. The hypoglossal nerve then turns horizontally and travels to the greater cornu of the hyoid bone, where it comes close to the lingual artery.
The hypoglossal nerve innervates all the intrinsic muscles of the tongue, as well as the extrinsic muscles of the tongue, except for palatoglossus.[6]
Muscles
The muscles of the tongue can be split into intrinsic and extrinsic muscles. The intrinsic muscles of the tongue originate and insert within the tongue. The 4 intrinsic muscles are the superior longitudinal, inferior longitudinal, transverse, and vertical muscles of the tongue, and they all act to change the shape and size of the tongue.
The extrinsic muscles of the tongue all originate outside of the tongue and then insert onto the tongue. There are 4 extrinsic muscles, genioglossus, hyoglossus, stylogossus, and palatoglossus. The hyoglossus muscle depresses and retracts the tongue. The styloglossus also acts to retract the tongue as well as elevating the sides of the tongue. The genioglossus muscle mainly acts to protrude the tongue but can also depress the tongue. The palatoglossus muscle elevates the posterior part of the tongue and is the only extrinsic muscle innervated by the vagus nerve (cranial nerve X) instead of the hypoglossal nerve. It is also important to note the chondroglossus, which acts to depress the lingual root. The chondroglossus is most commonly described as part of the hyoglossus muscle; however, some argue that it is an extrinsic tongue muscle in its own regard as it differs from the hyoglossus in its origin and course.[1][7]
Surgical Considerations
Oral cancers often present on the lateral portion of the tongue, and depending on the spread of cancer and its invasion of the surrounding tongue muscles, the surgical procedure differs. This can range from a mucosectomy in precancerous or superficial suspicious lesions to a total glossectomy in those with massive infiltrating lesions—the more invasive the surgery, the increased likelihood that the tongue muscles will be affected.
The removal of extrinsic and intrinsic tongue muscles will inhibit their proper functioning. Consequently, this condition makes it difficult for patients who require more invasive surgery to perform the functions that require these muscles. This includes swallowing, speech.[8] One way to mitigate this loss of function is through the reconstruction of the tongue via forearm-free flaps. It has also be found that if these free flaps are made to be 30 to 80 % larger than the resected area of the glossectomy, this may improve the ability to regain the abovementioned functions post-surgery.[9]
Clinical Significance
Airway Patency
The effect of the extrinsic muscles on the tongue plays a vital role in the patency of the airway. The main muscle responsible for airway dilation is the genioglossus, and if this muscle has decreased function, it can lead to airway constriction or obstruction. However, the role of the tongue retractor muscles (styloglossus and hyoglossus) in ensuring upper airway patency is not fully understood. Some studies have shown that in response to hypoxia and hypercapnia, both the hyoglossus and styloglossus muscles are activated alongside the genioglossus muscle.[10]
Knowledge of how to optimally ensure airway patency is of particular importance in patients with obstructive sleep apnea, as it can help reduce symptoms. One of the newer treatment options offered to select patients with obstructive sleep apnoea is hypoglossal nerve stimulation. As the hypoglossal nerve provides innervation to genioglossus, styloglossus, and hyoglossus, knowing which branches of the hypoglossal nerve to stimulate to optimize airway patency can improve patient outcomes. However, although the co-activation of these muscles has been seen in hypoxia and hypercapnia, studies looking at the ideal placement of electrodes for hypoglossal nerve stimulation have concluded that ensuring the tongue retractors are activated as little as possible resulted in better airway patency.[11]
This result is mainly accomplished by ensuring the lateral division of the hypoglossal nerve was not stimulated as this division had a greater proportion of fibers to the styloglossus and hyoglossus muscle compared to the medial division of the hypoglossal nerve, which mainly resulted in genioglossus muscle contraction.[12][13]
Swallowing
The hyoglossus also plays a key role in swallowing and is especially important in swallowing difficulties due to atypical first and second epiglottic movements. The first epiglottic movement is horizontal, and the second is the full inversion of the epiglottis. It has been suggested that the cause of impairments in these movements may be due to a reduction in both tongue base retraction and elevation of the larynx. In these cases, the hyoglossus, alongside the styloglossus and long pharyngeal muscles, should be the focus for rehabilitation.[14]