Learning Outcome
- Describe the causes of stroke
- Recall the presentation of stroke
- List the nursing diagnosis of stroke
- Summarize the management of stroke

A stroke is an acute compromise of the cerebral perfusion or vasculature or cerebrovascular accident (CVA). Approximately 85% of strokes are ischemic and rest are hemorrhagic.[1] In this discussion, we mainly confine to ischemic strokes. Over the past several decades, the incidence of stroke and mortality are decreasing.[2] Stroke is the leading cause of adult disability worldwide. It is thus critical to recognize stroke early and treat it rapidly to prevent or minimize morbidity and mortality. There are many causes of stroke. Hypertension is the leading cause of ischemic stroke. In the younger population, there are numerous causes of stroke including clotting disorders, carotid dissection, and illicit drug abuse. In the acute setting, a quick history and examination to be performed. As time is brain it is very important not to waste any time. As acute stroke management is evolving rapidly we have to consider patients for IV tPA up to 4.5 hours and mechanical thrombectomy up to 6 hours. The recent DAWN trial showed that we can extend the window for mechanical thrombectomy up to 24 hours in selected cases of large vessel occlusion.[3]
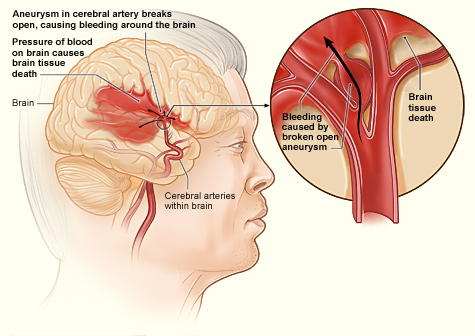
Ischemic etiologies can further be divided into embolic, thrombotic, and lacunar. In general, the common risk factors for stroke include hypertension, diabetes, smoking, obesity, atrial fibrillation, and drug use. Of all the risk factors, Hypertension is the most common modifiable risk factor for stroke. Hypertension is most prevalent in blacks and also occur earlier in life.[1] According to JNC8, the recommended blood pressure targets in patients with stroke should be less than 140/90mm Hg.[4] Chronic uncontrolled hypertension causes small vessel strokes mainly in the internal capsule, thalamus, pons, and cerebellum.[5] Lifestyle measures such as weight loss, salt restriction, taking more fruits and vegetables (Such as Mediterranean diet)[6] are helpful in decreasing the blood pressure. Every 10 mm Hg reduction in blood pressure is associated with a 1/3rd reduction in stroke risk in primary prevention.[7] One-third of the adults in the USA have elevated LDL, leading to plaque formation in the intracerebral vasculature. Eventually, due to the excessive plaque build-up thrombotic strokes occur. In the older population, the risk of cardioembolic stroke increases mainly due to atrial fibrillation.[8] The rest 20% of strokes are due to hemorrhagic in nature. Hemorrhagic etiologies can be from hypertension, aneurysm rupture, arteriovenous malformations, venous angiomas, bleeding due to illicit drugs like cocaine, hemorrhagic metastasis, amyloid angiopathy, and other obscure etiologies.
Stroke is the fifth leading cause of death in the US. The incidence of stroke is around 800,000 people annually. Stroke is the leading cause of disability.[9] The incidence of stroke has declined, but the morbidity has increased. Due to longer life expectancy, the lifetime risk of stroke is higher in women.
The most important piece of historical information that the physician should obtain is the time of symptoms onset or time last seen normal. This is critical because it determines the eligibility to receive rtPA or endovascular intervention for stroke. [10] Other important information to obtain is risk factors for arteriosclerosis and cardiovascular disease, diabetes, smoking, atrial fibrillations drug abuse, migraine, seizures, infection trauma or pregnancy.
The stroke exam is a multi-person coordinated rapid exam. While staff obtain vitals, attach telemetry, and obtain IV access, the physician performs rapid neurological evaluation. National Institutes of Health Stroke Scale (NIHSS) is routinely used to get the baseline evaluation. The exam has to be rapid as “time is brain.” One must examine the following items:
With a good history and physical exam, we can localize the stroke. There are various stroke syndromes.
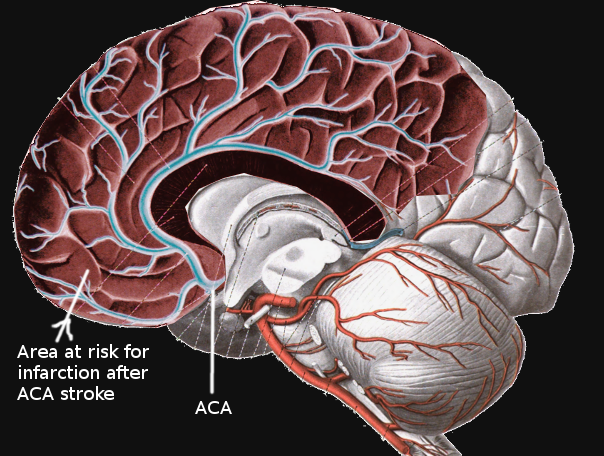
Anterior Cerebral Artery (ACA) Infarction
There is significant collateral blood supply in the anterior circulating artery territory. So, pure ACA strokes are rare. The ACA distribution involves mainly Broca’s area, primary motor, primary sensory and pre-frontal cortex. So patients present with motor aphasia, personality issues, and contralateral leg weakness and numbness. Hand and face are usually spared.
Middle Cerebral Artery (MCA) Infarction
The middle cerebral artery has the main trunk (M1) and it divides into two M2 Branches. The M1 (horizontal branch) supplies the basal ganglia and M2 (Sylvian branches) supplies part of the parietal, frontal and temporal lobes. As MCA supplies a wide territory it is extremely important to rule out MCA occlusion. The MCA syndrome causes contralateral arm and face numbness and weakness, gaze deviation towards the affected side. Aphasia in the left-sided lesions and neglect in the right-sided lesions.
Posterior Cerebral Artery (PCA) Infarction
The posterior cerebral artery mainly supplies occipital lobe, thalamus and some portion of the temporal lobe. The classic presentation of posterior cerebral artery stroke is homonymous hemianopsia. Apart from this hypersomnolence, cognitive issues, the hemisensory loss can be seen when the deep PCA is involved. Some times there is bilateral infarction of distal PCAs producing cortical blindness and the patient is unaware of the blindness and denies it. This is called Anton-Babinski syndrome.
Cerebellar Infarction
The patients with cerebellar strokes present with ataxia, dysarthria, nausea, vomiting, and vertigo.
The initial workup of a stroke patient involves stabilizing the Airway, Breathing, and Circulation (ABC). This is followed by a rapid, concise, history and exam such as the NIHSS which is administered simultaneously as the patient gets IV access, telemetry, and labs were drawn. The patient should then get a stat non-contrasted head CT or a combination of Head CT, CT Angiography, and perfusion imaging. "Time is brain," and so we should not waste any time at all. Ideally, rtPA should be prepared as imaging is occurring, and as soon as the non-contrasted head CT can be visualized, and a bleed is excluded, rtPA should be administered after discussing the risks and benefits, and excluding rtPA contraindications. Time is critical, as only patients who get all the required studies within 4.5 hours qualify for potentially lifesaving thrombolysis. After IV rtPA, the CT angiography should be reviewed to determine if the patient qualifies for endovascular therapy as well.
In recent years there are significant advancements in acute stroke care. Multiple stroke trials in 2015 showed that Endovascular thrombectomy in the first six hours is much better than standard medical care in patients with large vessel occlusion in the arteries of the proximal anterior circulation. These benefits sustained irrespective of geographical location and patient characteristics.[11]
Again in 2018, a significant paradigm shift happened in stroke care. DAWN trial showed significant benefits of Endovascular thrombectomy in patients with large vessel occlusion in the arteries of the proximal anterior circulation. This trial extended the stroke window up to 24 hours in selected patients using perfusion imaging. Due to this, we can treat more patients even up to 24 hours.[3]
All patients should be treated with an antiplatelet agent and a statin, and be admitted for full stroke evaluation. Hypertension is often seen in acute stroke. This should not be aggressively treated. A baseline electrocardiogram is recommended. The following labs would be indicated when a diagnosis of stroke is entertained:
A transthoracic echocardiogram, telemetry monitoring, and neck vessel imaging are necessary to elucidate the etiology of stroke.
Acute ischemic stroke patients who meet the criteria for rtPA and do not have any contraindications should receive IV rtPA. Patients who have large vessel occlusions should be evaluated for possible endovascular intervention. All patients suspected of having an acute ischemic stroke should be admitted for a full neurological workup. Neurology consultation should be obtained. The workup of acute ischemic stroke includes a search for a source of thrombus, which includes carotid evaluation by ultrasound, CTA, MRA, or conventional angiography. A Transthoracic echocardiogram is obtained to ascertain for low ejection fraction, the cardiac source of the clot, or patent foramen ovale. EKG and telemetry are obtained to ascertain for rhythms predisposing to stroke such as atrial fibrillation. Labs such as a fasting lipid panel, and hemoglobin A1C, are obtained to ascertain for modifiable risk factors for stroke. Other labs such as a hypercoagulable panel in young patients or B12 and syphilis testing in selected patients is also obtained. Antiplatelet and statins remain the mainstay of medical management of stroke.
A notable potential complication after fibrinolytic therapy is hemorrhagic transformation. Hemorrhagic transformation is classified as hemorrhagic infarction and parenchymal hematoma, each with 2 subsets. Predictive factors for the occurrence of this complication include increased infarction area, gray matter location, atrial fibrillation, and cerebral embolism, acute hyperglycemia, low platelet count, and poor collateral circulation.[12]
When to start anticoagulation in patients with atrial fibrillation after acute stroke is always a dilemma. Usually, it depends on various factors like the size of the stroke and other comorbidities. Usually, if the size of the stroke is smaller to moderate and no hemorrhage, we start anticoagulation in 7-14 days.[13]
Some times there are patients with small hemorrhagic transformation after acute stroke, and in this scenario, it is better to wait for anticoagulation for a couple of weeks. This delay is not associated with excessive stroke recurrence.[14]
For patients with significant disabilities, physical therapy and occupational therapy consults should be obtained. Similarly, if swallowing and speech are of concern, then speech/swallow consults should be obtained. All patients should have follow-ups arranged with their primary care providers, and with neurology at appropriate times post-discharge. For symptomatic and significant carotid artery stenosis, referrals to vascular or neurological surgery should be sought.
If unresponsive, low blood pressure, loss of consciousness, unable to move extremities or speak.
The management of stroke is with a multidisciplinary team that includes the emergency department physician, nurse practitioner, neurologist, radiologist, and the stroke team. The key is to first identify if the stroke is embolic or hemorrhagic and then institute thrombolytic treatment accordingly. For those who recover, physical, speech and occupational therapy may be necessary. The outcomes for patients with mild embolic strokes are good but those with hemorrhagic strokes tend to have poor outcomes.[15][16](Level V)
Educate the patient on the following:
Stroke continues to carry high morbidity and mortality. In addition, the cost to the healthcare system is enormous. Even though treatments for strokes exist, the outcomes are not satisfactory and many people remain permanently disabled.
To improve outcomes, there is ample evidence indicating that the management of stroke is best done with an interprofessional team that includes the emergency department physician, nurse practitioner, neurologist, radiologist, and the stroke team. The key is to first identify if the stroke is embolic or hemorrhagic and then institute thrombolytic treatment accordingly. For those who recover, physical, speech and occupational therapy may be necessary.
However, today the focus is on stroke prevention as it is more cost-effective. All clinicians have the responsibility for educating the public on methods to prevent strokes. The pharmacist should encourage blood pressure medication compliance since uncontrolled blood pressure is one of the risk factors for stroke. The clinicians including nurses should educate patients on discontinuing smoking, eating a healthy diet, exercising regularly and maintaining healthy body weight. Patients should be provided with supporting literature and educated about stroke and its complications.
For those who have developed a stroke, one may need to involve a social worker to ensure that the home is a safe place and that the patient has the support systems. A dietary consult should be made to educate the patient on what to eat. In addition, some patients may need to enroll in rehabilitation to regain speech, muscle and joint function. Only via an interprofessional team approach and open communication can this lead to improved outcomes and a better quality of life.
Other issues to remember:

Anterior Cerebral Artery Stroke
Contributed by S Bhimji, MD

Writing Group Members, Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jiménez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB, American Heart Association Statistics Committee, Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016 Jan 26:133(4):e38-360. doi: 10.1161/CIR.0000000000000350. Epub 2015 Dec 16 [PubMed PMID: 26673558]
Fang MC, Coca Perraillon M, Ghosh K, Cutler DM, Rosen AB. Trends in stroke rates, risk, and outcomes in the United States, 1988 to 2008. The American journal of medicine. 2014 Jul:127(7):608-15. doi: 10.1016/j.amjmed.2014.03.017. Epub 2014 Mar 25 [PubMed PMID: 24680794]
Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, Yavagal DR, Ribo M, Cognard C, Hanel RA, Sila CA, Hassan AE, Millan M, Levy EI, Mitchell P, Chen M, English JD, Shah QA, Silver FL, Pereira VM, Mehta BP, Baxter BW, Abraham MG, Cardona P, Veznedaroglu E, Hellinger FR, Feng L, Kirmani JF, Lopes DK, Jankowitz BT, Frankel MR, Costalat V, Vora NA, Yoo AJ, Malik AM, Furlan AJ, Rubiera M, Aghaebrahim A, Olivot JM, Tekle WG, Shields R, Graves T, Lewis RJ, Smith WS, Liebeskind DS, Saver JL, Jovin TG, DAWN Trial Investigators. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. The New England journal of medicine. 2018 Jan 4:378(1):11-21. doi: 10.1056/NEJMoa1706442. Epub 2017 Nov 11 [PubMed PMID: 29129157]
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014 Feb 5:311(5):507-20. doi: 10.1001/jama.2013.284427. Epub [PubMed PMID: 24352797]
Shi Y, Wardlaw JM. Update on cerebral small vessel disease: a dynamic whole-brain disease. Stroke and vascular neurology. 2016 Sep:1(3):83-92. doi: 10.1136/svn-2016-000035. Epub 2016 Oct 25 [PubMed PMID: 28959468]
Estruch R, Ros E, Martínez-González MA. Mediterranean diet for primary prevention of cardiovascular disease. The New England journal of medicine. 2013 Aug 15:369(7):676-7. doi: 10.1056/NEJMc1306659. Epub [PubMed PMID: 23944307]
Lawes CM, Bennett DA, Feigin VL, Rodgers A. Blood pressure and stroke: an overview of published reviews. Stroke. 2004 Apr:35(4):1024 [PubMed PMID: 15053002]
Ferro JM. Cardioembolic stroke: an update. The Lancet. Neurology. 2003 Mar:2(3):177-88 [PubMed PMID: 12849239]
Krishnamurthi RV, Moran AE, Feigin VL, Barker-Collo S, Norrving B, Mensah GA, Taylor S, Naghavi M, Forouzanfar MH, Nguyen G, Johnson CO, Vos T, Murray CJ, Roth GA, GBD 2013 Stroke Panel Experts Group. Stroke Prevalence, Mortality and Disability-Adjusted Life Years in Adults Aged 20-64 Years in 1990-2013: Data from the Global Burden of Disease 2013 Study. Neuroepidemiology. 2015:45(3):190-202. doi: 10.1159/000441098. Epub 2015 Oct 28 [PubMed PMID: 26505983]
Xing C, Arai K, Lo EH, Hommel M. Pathophysiologic cascades in ischemic stroke. International journal of stroke : official journal of the International Stroke Society. 2012 Jul:7(5):378-85. doi: 10.1111/j.1747-4949.2012.00839.x. Epub [PubMed PMID: 22712739]
Yew KS, Cheng E. Acute stroke diagnosis. American family physician. 2009 Jul 1:80(1):33-40 [PubMed PMID: 19621844]
M Das J, Naqvi IA. Anton Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 30844182]
Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, Dávalos A, Majoie CB, van der Lugt A, de Miquel MA, Donnan GA, Roos YB, Bonafe A, Jahan R, Diener HC, van den Berg LA, Levy EI, Berkhemer OA, Pereira VM, Rempel J, Millán M, Davis SM, Roy D, Thornton J, Román LS, Ribó M, Beumer D, Stouch B, Brown S, Campbell BC, van Oostenbrugge RJ, Saver JL, Hill MD, Jovin TG, HERMES collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet (London, England). 2016 Apr 23:387(10029):1723-31. doi: 10.1016/S0140-6736(16)00163-X. Epub 2016 Feb 18 [PubMed PMID: 26898852]
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL, American Heart Association Stroke Council. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2018 Mar:49(3):e46-e110. doi: 10.1161/STR.0000000000000158. Epub 2018 Jan 24 [PubMed PMID: 29367334]
Tadi P, Lui F. Acute Stroke. StatPearls. 2023 Jan:(): [PubMed PMID: 30570990]
Paciaroni M, Agnelli G, Falocci N, Tsivgoulis G, Vadikolias K, Liantinioti C, Chondrogianni M, Bovi P, Carletti M, Cappellari M, Zedde M, Ntaios G, Karagkiozi E, Athanasakis G, Makaritsis K, Silvestrelli G, Lanari A, Ciccone A, Putaala J, Tomppo L, Tatlisumak T, Abdul-Rahim AH, Lees KR, Alberti A, Venti M, Acciarresi M, D'Amore C, Becattini C, Mosconi MG, Cimini LA, Soloperto R, Masotti L, Vannucchi V, Lorenzini G, Tassi R, Guideri F, Acampa M, Martini G, Sohn SI, Marcheselli S, Mumoli N, De Lodovici ML, Bono G, Furie KL, Tadi P, Yaghi S, Toni D, Letteri F, Tassinari T, Kargiotis O, Lotti EM, Flomin Y, Mancuso M, Maccarrone M, Giannini N, Bandini F, Pezzini A, Poli L, Padovani A, Scoditti U, Denti L, Consoli D, Galati F, Sacco S, Carolei A, Tiseo C, Gourbali V, Orlandi G, Giuntini M, Chiti A, Giorli E, Gialdini G, Corea F, Ageno W, Bellesini M, Colombo G, Monaco S, Maimone Baronello M, Karapanayiotides T, Caso V. Early Recurrence and Major Bleeding in Patients With Acute Ischemic Stroke and Atrial Fibrillation Treated With Non-Vitamin-K Oral Anticoagulants (RAF-NOACs) Study. Journal of the American Heart Association. 2017 Nov 29:6(12):. doi: 10.1161/JAHA.117.007034. Epub 2017 Nov 29 [PubMed PMID: 29220330]
Paciaroni M, Bandini F, Agnelli G, Tsivgoulis G, Yaghi S, Furie KL, Tadi P, Becattini C, Zedde M, Abdul-Rahim AH, Lees KR, Alberti A, Venti M, Acciarresi M, D'Amore C, Mosconi MG, Cimini LA, Altavilla R, Volpi G, Bovi P, Carletti M, Rigatelli A, Cappellari M, Putaala J, Tomppo L, Tatlisumak T, Marcheselli S, Pezzini A, Poli L, Padovani A, Masotti L, Vannucchi V, Sohn SI, Lorenzini G, Tassi R, Guideri F, Acampa M, Martini G, Ntaios G, Athanasakis G, Makaritsis K, Karagkiozi E, Vadikolias K, Liantinioti C, Chondrogianni M, Mumoli N, Consoli D, Galati F, Sacco S, Carolei A, Tiseo C, Corea F, Ageno W, Bellesini M, Colombo G, Silvestrelli G, Ciccone A, Lanari A, Scoditti U, Denti L, Mancuso M, Maccarrone M, Ulivi L, Orlandi G, Giannini N, Gialdini G, Tassinari T, De Lodovici ML, Bono G, Rueckert C, Baldi A, D'Anna S, Toni D, Letteri F, Giuntini M, Lotti EM, Flomin Y, Pieroni A, Kargiotis O, Karapanayiotides T, Monaco S, Maimone Baronello M, Csiba L, Szabó L, Chiti A, Giorli E, Del Sette M, Imberti D, Zabzuni D, Doronin B, Volodina V, Michel P, Vanacker P, Barlinn K, Pallesen LP, Barlinn J, Deleu D, Melikyan G, Ibrahim F, Akhtar N, Gourbali V, Caso V. Hemorrhagic Transformation in Patients With Acute Ischemic Stroke and Atrial Fibrillation: Time to Initiation of Oral Anticoagulant Therapy and Outcomes. Journal of the American Heart Association. 2018 Nov 20:7(22):e010133. doi: 10.1161/JAHA.118.010133. Epub [PubMed PMID: 30571487]
Langhorne P, Stott DJ, Robertson L, MacDonald J, Jones L, McAlpine C, Dick F, Taylor GS, Murray G. Medical complications after stroke: a multicenter study. Stroke. 2000 Jun:31(6):1223-9 [PubMed PMID: 10835436]
Xu Y, Parikh NS, Jiao B, Willey JZ, Boehme AK, Elkind MSV. Decision Analysis Model for Prehospital Triage of Patients With Acute Stroke. Stroke. 2019 Apr:50(4):970-977. doi: 10.1161/STROKEAHA.118.023272. Epub [PubMed PMID: 30908159]
Rohde D, Gaynor E, Large M, Conway O, Bennett K, Williams DJ, Callaly E, Dolan E, Hickey A. Stroke survivor cognitive decline and psychological wellbeing of family caregivers five years post-stroke: a cross-sectional analysis. Topics in stroke rehabilitation. 2019 Apr:26(3):180-186. doi: 10.1080/10749357.2019.1590972. Epub 2019 Mar 23 [PubMed PMID: 30907273]