Learning Outcome
- Understand the clinical signs and symptoms of heart failure
- Understand the pathophysiology of heart failure
- Review the lifestyle modifications recommended for patients with heart failure
Heart failure is a common and complex clinical syndrome that results from any functional or structural heart disorder, impairing ventricular filling or ejection of blood to the systemic circulation to meet the body's needs. Heart failure can be caused by several different diseases. Most patients with heart failure have symptoms due to impaired left ventricular myocardial function. Patients usually present with dyspnea, fatigue, decreased exercise tolerance, and fluid retention, seen as pulmonary and peripheral edema.[1]
Heart failure due to left ventricular dysfunction is categorized according to left ventricular ejection fraction (LVEF) into heart failure with reduced ejection fraction (LVEF 40% or less), known as HFrEF, and heart failure with preserved ejection fraction (LVEF greater than 40%); known as HFpEF.[2]
Heart failure is caused by several disorders, including diseases affecting the pericardium, myocardium, endocardium, cardiac valves, vasculature, or metabolism. The most common causes of systolic dysfunction (HFrEF) are idiopathic dilated cardiomyopathy (DCM), coronary heart disease (ischemic), hypertension, and valvular disease. For diastolic dysfunction (HFpEF), similar conditions have been described as common causes, adding hypertrophic obstructive cardiomyopathy and restrictive cardiomyopathy.[1]
Symptoms of heart failure include those due to excess fluid accumulation (dyspnea, orthopnea, edema, pain from hepatic congestion, and abdominal distention from ascites) and those due to a reduction in cardiac output (fatigue, weakness) most pronounced with physical exertion.[1]
Acute and subacute presentations (days to weeks) are characterized by shortness of breath at rest and/or with exertion, orthopnea, paroxysmal nocturnal dyspnea, and right upper quadrant discomfort due to acute hepatic congestion (right heart failure). Palpitations, with or without lightheadedness, can occur if patients develop atrial or ventricular tachyarrhythmias.
Chronic presentations (months) differ in that fatigue, anorexia, abdominal distension, and peripheral edema may be more pronounced than dyspnea. The anorexia is secondary to several factors, including poor perfusion of the splanchnic circulation, bowel edema, and nausea induced by hepatic congestion.[1]
Characteristic features:
New York Heart Association Functional Classification[3]
Based on symptoms, the patients can be classified using the New York Heart Association (NYHA) functional classification as follows:
Tests used in the evaluation of patients with HF include:
Diuretics, beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, angiotensin receptor neprilysin inhibitor, hydralazine plus nitrate, digoxin, and aldosterone antagonists can produce an improvement in symptoms and are indicated for patients with HF based on their functional classification and severity of symptoms. Combination therapy with these agents improves outcomes and reduces hospitalizations in patients with HF.[3]
Improved patient survival has been documented with the use of beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor neprilysin inhibitor, hydralazine plus nitrate, and aldosterone antagonists. More limited evidence of survival benefit is available for diuretic therapy. Diuretic therapy is mainly used for symptom control. Angiotensin receptor neprilysin inhibitors should not be given within 36 hrs of angiotensin-converting enzyme inhibitors dose.[3]
In African-Americans, hydralazine plus oral nitrate is indicated in patients with persistent NYHA class III to IV HF and LVEF less than 40%, despite optimal medical therapy (beta-blocker, angiotensin-converting enzyme inhibitors, ARB, aldosterone antagonist (if indicated), and diuretics.[3]
Device therapy: Implantable cardioverter-defibrillator (ICD) is used for primary or secondary prevention of sudden cardiac death. Cardiac resynchronization therapy with biventricular pacing can improve symptoms and survival in selected patients who are in sinus rhythm and have a reduced left ventricular ejection fraction and a prolonged QRS duration. Most patients who satisfy the criteria for cardiac resynchronization therapy implantation are also candidates for an implantable cardioverter-defibrillator and receive a combined device.[3]
A ventricular assist device (bridge to transplant or as a destination therapy) or cardiac transplant is reserved for those with severe disease despite all other measures.
The nursing care plan for patients with HF should include:[4]
Prompt assessment by the medical team is indicated in the following situations:
Patients with HF require frequent monitoring of vital signs, including oxygen saturation. They may also require constant monitoring of the heart rate and rhythm via telemetry monitoring. Frequent assessment and monitoring for symptoms is also indicated. All patients with HF require daily weight monitoring.
Heart failure is a serious disorder best managed by an interprofessional team that includes the primary care physician, emergency department physician, cardiologist, radiologist, cardiac nurses, internist, and cardiac surgeons. It is imperative to treat the cause of heart failure. Healthcare workers who look after these patients must be familiar with current guidelines on treatment. The risk factors for heart disease must be modified, and the clinical nurse should educate the patient on the importance of medication compliance and lifestyle modifications. When the condition is not managed appropriately, it is associated with high morbidity and mortality, including poor quality of life.[5]
Nursing care plans for patients with HF must include patient education to improve clinical outcomes and reduce hospital readmissions. Patients need education and guidance on self-monitoring of symptoms at home, medication compliance, daily weight monitoring, dietary sodium restriction to 2 to 3 g/day, and daily fluid restriction to 2 L/day. In addition, patients with HF need aggressive treatment for underlying risk factors and the potential triggers for HF exacerbations. Modifiable risk factors include diabetes mellitus, hypertension, obesity, nicotine use, alcohol use disorder, and recreational drug use, especially cocaine. Patients with sleep apnea and HF should be encouraged to use continuous positive airway pressure (CPAP) therapy as uncontrolled sleep apnea can also increase HF-associated morbidity and mortality.
Discharge planning for patients with HF must include patient education on medication management, medication compliance, low-sodium diet, fluid restriction, activity and exercise recommendations, smoking cessation, and learning to recognize the signs and symptoms of worsening HF. Discharge planning for patients with HF must also include follow-up appointments to ensure patients have a close medical follow-up after discharge. Nurse-driven education at the time of discharge has been shown to improve compliance with therapy and improve patient outcomes in heart failure.[6]
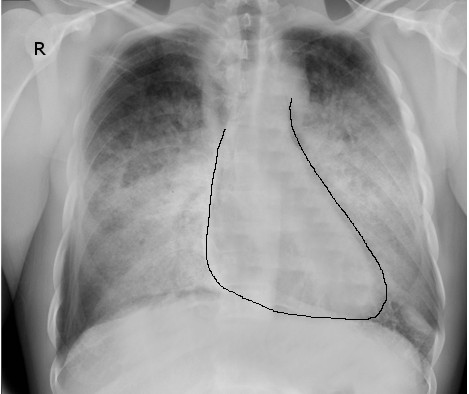
Congestive Heart Failure, Radiograph. Chest radiographs help assess for signs of pulmonary congestion or edema in acute decompensated heart failure.
Contributed by S Bhimji, MD
Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW, ACC/AHA Joint Committee Members. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 May 3:145(18):e895-e1032. doi: 10.1161/CIR.0000000000001063. Epub 2022 Apr 1 [PubMed PMID: 35363499]
CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The New England journal of medicine. 1987 Jun 4:316(23):1429-35 [PubMed PMID: 2883575]
Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nature reviews. Cardiology. 2016 Jun:13(6):368-78. doi: 10.1038/nrcardio.2016.25. Epub 2016 Mar 3 [PubMed PMID: 26935038]
Lind L, Ingelsson M, Sundstrom J, Ärnlöv J. Impact of risk factors for major cardiovascular diseases: a comparison of life-time observational and Mendelian randomisation findings. Open heart. 2021 Sep:8(2):. doi: 10.1136/openhrt-2021-001735. Epub [PubMed PMID: 34518286]
Noubiap JJ, Agbor VN, Bigna JJ, Kaze AD, Nyaga UF, Mayosi BM. Prevalence and progression of rheumatic heart disease: a global systematic review and meta-analysis of population-based echocardiographic studies. Scientific reports. 2019 Nov 19:9(1):17022. doi: 10.1038/s41598-019-53540-4. Epub 2019 Nov 19 [PubMed PMID: 31745178]
Kim KH, Pereira NL. Genetics of Cardiomyopathy: Clinical and Mechanistic Implications for Heart Failure. Korean circulation journal. 2021 Oct:51(10):797-836. doi: 10.4070/kcj.2021.0154. Epub 2021 Jul 22 [PubMed PMID: 34327881]
Rezkalla SH, Kloner RA. Viral myocarditis: 1917-2020: From the Influenza A to the COVID-19 pandemics. Trends in cardiovascular medicine. 2021 Apr:31(3):163-169. doi: 10.1016/j.tcm.2020.12.007. Epub 2020 Dec 29 [PubMed PMID: 33383171]
Muchtar E, Blauwet LA, Gertz MA. Restrictive Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circulation research. 2017 Sep 15:121(7):819-837. doi: 10.1161/CIRCRESAHA.117.310982. Epub [PubMed PMID: 28912185]
Shams P, Ahmed I. Cardiac Amyloidosis. StatPearls. 2025 Jan:(): [PubMed PMID: 35593829]
Brown KN, Pendela VS, Ahmed I, Diaz RR. Restrictive Cardiomyopathy. StatPearls. 2025 Jan:(): [PubMed PMID: 30725919]
Matta AG, Carrié D. Epidemiology, Pathophysiology, Diagnosis, and Principles of Management of Takotsubo Cardiomyopathy: A Review. Medical science monitor : international medical journal of experimental and clinical research. 2023 Mar 6:29():e939020. doi: 10.12659/MSM.939020. Epub 2023 Mar 6 [PubMed PMID: 36872594]
Bairashevskaia AV, Belogubova SY, Kondratiuk MR, Rudnova DS, Sologova SS, Tereshkina OI, Avakyan EI. Update of Takotsubo cardiomyopathy: Present experience and outlook for the future. International journal of cardiology. Heart & vasculature. 2022 Apr:39():100990. doi: 10.1016/j.ijcha.2022.100990. Epub 2022 Mar 7 [PubMed PMID: 35281752]
Ahmad SA, Brito D, Khalid N, Ibrahim MA. Takotsubo Cardiomyopathy. StatPearls. 2025 Jan:(): [PubMed PMID: 28613549]
DeFilippis EM, Beale A, Martyn T, Agarwal A, Elkayam U, Lam CSP, Hsich E. Heart Failure Subtypes and Cardiomyopathies in Women. Circulation research. 2022 Feb 18:130(4):436-454. doi: 10.1161/CIRCRESAHA.121.319900. Epub 2022 Feb 17 [PubMed PMID: 35175847]
Wong CM, Hawkins NM, Jhund PS, MacDonald MR, Solomon SD, Granger CB, Yusuf S, Pfeffer MA, Swedberg K, Petrie MC, McMurray JJ. Clinical characteristics and outcomes of young and very young adults with heart failure: The CHARM programme (Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity). Journal of the American College of Cardiology. 2013 Nov 12:62(20):1845-54. doi: 10.1016/j.jacc.2013.05.072. Epub 2013 Jul 10 [PubMed PMID: 23850914]
Sciomer S, Moscucci F, Salvioni E, Marchese G, Bussotti M, Corrà U, Piepoli MF. Role of gender, age and BMI in prognosis of heart failure. European journal of preventive cardiology. 2020 Dec:27(2_suppl):46-51. doi: 10.1177/2047487320961980. Epub [PubMed PMID: 33238736]
Volpe M, Gallo G. Obesity and cardiovascular disease: An executive document on pathophysiological and clinical links promoted by the Italian Society of Cardiovascular Prevention (SIPREC). Frontiers in cardiovascular medicine. 2023:10():1136340. doi: 10.3389/fcvm.2023.1136340. Epub 2023 Mar 13 [PubMed PMID: 36993998]
Kim DY, Kim SH, Ryu KH. Tachycardia induced Cardiomyopathy. Korean circulation journal. 2019 Sep:49(9):808-817. doi: 10.4070/kcj.2019.0199. Epub [PubMed PMID: 31456374]
Anakwue RC, Onwubere BJ, Anisiuba BC, Ikeh VO, Mbah A, Ike SO. Congestive heart failure in subjects with thyrotoxicosis in a black community. Vascular health and risk management. 2010 Aug 9:6():473-7 [PubMed PMID: 20730063]
Schoenenberger AW, Schoenenberger-Berzins R, der Maur CA, Suter PM, Vergopoulos A, Erne P. Thiamine supplementation in symptomatic chronic heart failure: a randomized, double-blind, placebo-controlled, cross-over pilot study. Clinical research in cardiology : official journal of the German Cardiac Society. 2012 Mar:101(3):159-64. doi: 10.1007/s00392-011-0376-2. Epub 2011 Nov 5 [PubMed PMID: 22057652]
DiNicolantonio JJ, Liu J, O'Keefe JH. Thiamine and Cardiovascular Disease: A Literature Review. Progress in cardiovascular diseases. 2018 May-Jun:61(1):27-32. doi: 10.1016/j.pcad.2018.01.009. Epub 2018 Jan 31 [PubMed PMID: 29360523]
Reddy YNV, Melenovsky V, Redfield MM, Nishimura RA, Borlaug BA. High-Output Heart Failure: A 15-Year Experience. Journal of the American College of Cardiology. 2016 Aug 2:68(5):473-482. doi: 10.1016/j.jacc.2016.05.043. Epub [PubMed PMID: 27470455]
Chayanupatkul M, Liangpunsakul S. Cirrhotic cardiomyopathy: review of pathophysiology and treatment. Hepatology international. 2014 Jul:8(3):308-15. doi: 10.1007/s12072-014-9531-y. Epub [PubMed PMID: 25221635]
Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Shay CM, Spartano NL, Stokes A, Tirschwell DL, VanWagner LB, Tsao CW, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020 Mar 3:141(9):e139-e596. doi: 10.1161/CIR.0000000000000757. Epub 2020 Jan 29 [PubMed PMID: 31992061]
Ho KK, Pinsky JL, Kannel WB, Levy D. The epidemiology of heart failure: the Framingham Study. Journal of the American College of Cardiology. 1993 Oct:22(4 Suppl A):6A-13A [PubMed PMID: 8376698]
Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. 2017 Mar 7:135(10):e146-e603. doi: 10.1161/CIR.0000000000000485. Epub 2017 Jan 25 [PubMed PMID: 28122885]
Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, Hystad P, Brauer M, Kutty VR, Gupta R, Wielgosz A, AlHabib KF, Dans A, Lopez-Jaramillo P, Avezum A, Lanas F, Oguz A, Kruger IM, Diaz R, Yusoff K, Mony P, Chifamba J, Yeates K, Kelishadi R, Yusufali A, Khatib R, Rahman O, Zatonska K, Iqbal R, Wei L, Bo H, Rosengren A, Kaur M, Mohan V, Lear SA, Teo KK, Leong D, O'Donnell M, McKee M, Dagenais G. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet (London, England). 2020 Mar 7:395(10226):795-808. doi: 10.1016/S0140-6736(19)32008-2. Epub 2019 Sep 3 [PubMed PMID: 31492503]
Opie LH, Commerford PJ, Gersh BJ, Pfeffer MA. Controversies in ventricular remodelling. Lancet (London, England). 2006 Jan 28:367(9507):356-67 [PubMed PMID: 16443044]
Kemp CD, Conte JV. The pathophysiology of heart failure. Cardiovascular pathology : the official journal of the Society for Cardiovascular Pathology. 2012 Sep-Oct:21(5):365-71. doi: 10.1016/j.carpath.2011.11.007. Epub 2012 Jan 5 [PubMed PMID: 22227365]
Ait Mou Y, Bollensdorff C, Cazorla O, Magdi Y, de Tombe PP. Exploring cardiac biophysical properties. Global cardiology science & practice. 2015:2015():10. doi: 10.5339/gcsp.2015.10. Epub 2015 Apr 10 [PubMed PMID: 26779498]
Abassi Z, Khoury EE, Karram T, Aronson D. Edema formation in congestive heart failure and the underlying mechanisms. Frontiers in cardiovascular medicine. 2022:9():933215. doi: 10.3389/fcvm.2022.933215. Epub 2022 Sep 27 [PubMed PMID: 36237903]
Prausmüller S, Arfsten H, Spinka G, Freitag C, Bartko PE, Goliasch G, Strunk G, Pavo N, Hülsmann M. Plasma Neprilysin Displays No Relevant Association With Neurohumoral Activation in Chronic HFrEF. Journal of the American Heart Association. 2020 Jun 2:9(11):e015071. doi: 10.1161/JAHA.119.015071. Epub 2020 May 19 [PubMed PMID: 32427034]
Docherty KF, Vaduganathan M, Solomon SD, McMurray JJV. Sacubitril/Valsartan: Neprilysin Inhibition 5 Years After PARADIGM-HF. JACC. Heart failure. 2020 Oct:8(10):800-810. doi: 10.1016/j.jchf.2020.06.020. Epub [PubMed PMID: 33004114]
Obokata M, Reddy YNV, Borlaug BA. Diastolic Dysfunction and Heart Failure With Preserved Ejection Fraction: Understanding Mechanisms by Using Noninvasive Methods. JACC. Cardiovascular imaging. 2020 Jan:13(1 Pt 2):245-257. doi: 10.1016/j.jcmg.2018.12.034. Epub 2019 Jun 12 [PubMed PMID: 31202759]
Kao DP, Lewsey JD, Anand IS, Massie BM, Zile MR, Carson PE, McKelvie RS, Komajda M, McMurray JJ, Lindenfeld J. Characterization of subgroups of heart failure patients with preserved ejection fraction with possible implications for prognosis and treatment response. European journal of heart failure. 2015 Sep:17(9):925-35. doi: 10.1002/ejhf.327. Epub 2015 Aug 6 [PubMed PMID: 26250359]
Harjola VP, Mullens W, Banaszewski M, Bauersachs J, Brunner-La Rocca HP, Chioncel O, Collins SP, Doehner W, Filippatos GS, Flammer AJ, Fuhrmann V, Lainscak M, Lassus J, Legrand M, Masip J, Mueller C, Papp Z, Parissis J, Platz E, Rudiger A, Ruschitzka F, Schäfer A, Seferovic PM, Skouri H, Yilmaz MB, Mebazaa A. Organ dysfunction, injury and failure in acute heart failure: from pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). European journal of heart failure. 2017 Jul:19(7):821-836. doi: 10.1002/ejhf.872. Epub 2017 May 30 [PubMed PMID: 28560717]
King M, Kingery J, Casey B. Diagnosis and evaluation of heart failure. American family physician. 2012 Jun 15:85(12):1161-8 [PubMed PMID: 22962896]
Ali AS, Rybicki BA, Alam M, Wulbrecht N, Richer-Cornish K, Khaja F, Sabbah HN, Goldstein S. Clinical predictors of heart failure in patients with first acute myocardial infarction. American heart journal. 1999 Dec:138(6 Pt 1):1133-9 [PubMed PMID: 10577445]
Klein L, O'Connor CM, Leimberger JD, Gattis-Stough W, Piña IL, Felker GM, Adams KF Jr, Califf RM, Gheorghiade M, OPTIME-CHF Investigators. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation. 2005 May 17:111(19):2454-60 [PubMed PMID: 15867182]
Kelder JC, Cramer MJ, van Wijngaarden J, van Tooren R, Mosterd A, Moons KG, Lammers JW, Cowie MR, Grobbee DE, Hoes AW. The diagnostic value of physical examination and additional testing in primary care patients with suspected heart failure. Circulation. 2011 Dec 20:124(25):2865-73. doi: 10.1161/CIRCULATIONAHA.111.019216. Epub 2011 Nov 21 [PubMed PMID: 22104551]
Rørth R, Jhund PS, Yilmaz MB, Kristensen SL, Welsh P, Desai AS, Køber L, Prescott MF, Rouleau JL, Solomon SD, Swedberg K, Zile MR, Packer M, McMurray JJV. Comparison of BNP and NT-proBNP in Patients With Heart Failure and Reduced Ejection Fraction. Circulation. Heart failure. 2020 Feb:13(2):e006541. doi: 10.1161/CIRCHEARTFAILURE.119.006541. Epub 2020 Feb 17 [PubMed PMID: 32065760]
Hacker M, Hoyer X, Kupzyk S, La Fougere C, Kois J, Stempfle HU, Tiling R, Hahn K, Störk S. Clinical validation of the gated blood pool SPECT QBS processing software in congestive heart failure patients: correlation with MUGA, first-pass RNV and 2D-echocardiography. The international journal of cardiovascular imaging. 2006 Jun-Aug:22(3-4):407-16 [PubMed PMID: 16328851]
Jain S, Londono FJ, Segers P, Gillebert TC, De Buyzere M, Chirinos JA. MRI Assessment of Diastolic and Systolic Intraventricular Pressure Gradients in Heart Failure. Current heart failure reports. 2016 Feb:13(1):37-46. doi: 10.1007/s11897-016-0281-0. Epub [PubMed PMID: 26780916]
Cahill TJ, Ashrafian H, Watkins H. Genetic cardiomyopathies causing heart failure. Circulation research. 2013 Aug 30:113(6):660-75. doi: 10.1161/CIRCRESAHA.113.300282. Epub [PubMed PMID: 23989711]
Peterson PN, Rumsfeld JS, Liang L, Albert NM, Hernandez AF, Peterson ED, Fonarow GC, Masoudi FA, American Heart Association Get With the Guidelines-Heart Failure Program. A validated risk score for in-hospital mortality in patients with heart failure from the American Heart Association get with the guidelines program. Circulation. Cardiovascular quality and outcomes. 2010 Jan:3(1):25-32. doi: 10.1161/CIRCOUTCOMES.109.854877. Epub 2009 Dec 8 [PubMed PMID: 20123668]
Lam CSP, Mulder H, Lopatin Y, Vazquez-Tanus JB, Siu D, Ezekowitz J, Pieske B, O'Connor CM, Roessig L, Patel MJ, Anstrom KJ, Hernandez AF, Armstrong PW, VICTORIA Study Group. Blood Pressure and Safety Events With Vericiguat in the VICTORIA Trial. Journal of the American Heart Association. 2021 Nov 16:10(22):e021094. doi: 10.1161/JAHA.121.021094. Epub 2021 Nov 6 [PubMed PMID: 34743540]
Armstrong PW, Pieske B, Anstrom KJ, Ezekowitz J, Hernandez AF, Butler J, Lam CSP, Ponikowski P, Voors AA, Jia G, McNulty SE, Patel MJ, Roessig L, Koglin J, O'Connor CM, VICTORIA Study Group. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. The New England journal of medicine. 2020 May 14:382(20):1883-1893. doi: 10.1056/NEJMoa1915928. Epub 2020 Mar 28 [PubMed PMID: 32222134]
Lucas C, Johnson W, Hamilton MA, Fonarow GC, Woo MA, Flavell CM, Creaser JA, Stevenson LW. Freedom from congestion predicts good survival despite previous class IV symptoms of heart failure. American heart journal. 2000 Dec:140(6):840-7 [PubMed PMID: 11099986]
Rider I, Sorensen M, Brady WJ, Gottlieb M, Benson S, Koyfman A, Long B. Disposition of acute decompensated heart failure from the emergency department: An evidence-based review. The American journal of emergency medicine. 2021 Dec:50():459-465. doi: 10.1016/j.ajem.2021.08.070. Epub 2021 Sep 2 [PubMed PMID: 34500232]