Learning Outcome
- Define what is asystole
- Describe the management of asystole
- Know the nursing protocol for asystole
Asystole, colloquially referred to as flatline, represents the cessation of electrical and mechanical activity of the heart. Asystole typically occurs as a deterioration of the initial non-perfusing ventricular rhythms: ventricular fibrillation (V-fib) or pulseless ventricular tachycardia (V-tach). Additionally, pulseless electrical activity (PEA) can cease and become asystole. Victims of sudden cardiac arrest who present with asystole as the initial rhythm have an extremely poor prognosis (10% survive to admission, 0 to 2% survival-to-hospital discharge rate).[1][2][3] Asystole represents the terminal rhythm of a cardiac arrest.
In out-of-hospital cardiac arrest, prolonged resuscitation efforts in a patient who presents in asystole are unlikely to provide a medical benefit. Termination of resuscitation efforts should be considered in these patients, in consultation with online medical direction, as allowed by local protocols. The American College of Emergency Physicians (ACEP) and National Association of Emergency Medical Services Physicians (NAEMSP) both recommend emergency medical services systems and have written protocols that allow for termination of resuscitation efforts by emergency medical services providers for a select group of patients in which further resuscitative measures and transport to the local emergency department would be considered futile.[4]
No blood pressure, no heart rate, and unresponsive
The causes of asystole in cardiac arrest are wide and varied. Asystole typically results from decompensation of prolonged ventricular fibrillation arrest. Additionally, attempted defibrillation of ventricular tachycardia or ventricular fibrillation can precipitate asystole. However, any cause of cardiac arrest can eventually result in asystole if not promptly treated. When evaluating a patient with an initial cardiac rhythm of asystole, the reversible causes must be considered. A useful mnemonic taught in Advanced Cardiac Life Support (ACLS) for the reversible causes of cardiac arrest involves the Hs and Ts. The Hs include Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/Hyperkalemia, and Hypothermia. The Ts include Tension pneumothorax, Tamponade (cardiac), Toxins, and Thrombosis (both pulmonary and coronary). When identified, these cases should be immediately treated.[5][6]
Each year, approximately 300,000 to 400,000 Americans experience a cardiac arrest outside of the hospital, with the mortality of these cases being extremely high. Data vary in different regions of the country and various studies. Differences range from 4.6% to 11% survival-to-hospital discharge rate.[2][3][7] An extensive surveillance study conducted by the Centers for Disease Control and Prevention (CDC) from 2005 through 2010 evaluated 40,274 out-of-hospital cardiac arrest cases entered into the Cardiac Arrest Registry to Enhance Survival (CARES) system. A total of 31,645 cases had a documented presenting initial rhythm. This is the largest number of cases (45.1%) presented in asystole. However, asystole had the lowest survival rate (2.3%).[8]
Fewer data are available with in-hospital cardiac arrest. This, in addition to a lack of reporting consistency, makes the true number of in-hospital cardiac arrest cases largely unknown. Extrapolation of one large data set estimates approximately 200,000 in-hospital adult cardiac arrest cases per year. This estimate was confirmed in a second study using the Get With The Guidelines-Resuscitation registry. Neither of these studies investigated cardiac rhythms associated with cardiac arrest.[1][9]
The findings of cardiac arrest are straightforward. A patient who is in cardiac arrest is unresponsive to all stimuli and is without spontaneous breathing or a palpable pulse. The American Heart Association (AHA) has simplified its basic life support (BLS) cardiac arrest algorithm to encourage minimal compression interruption. The current algorithm has eliminated the “look, listen, and feel” step to check for breathing in an unresponsive patient. Instead, the rescuer should observe to see whether the patient is breathing normally. Emphasis is placed on “gasping” or agonal breathing being abnormal. If the patient is not breathing or only has agonal respirations, the rescuer should check for a carotid pulse for the unresponsive adult or the brachial pulse in the unresponsive infant for no more than 10 seconds. If a pulse is not felt or the rescuer is unsure if a pulse was felt, CPR should be initiated immediately.
Asystole is identified on cardiac monitoring. In asystole, there is no waveform present on the cardiac monitor, only an isoelectric “flat” line. This includes a lack of P-waves, QRS complexes, and T-waves.
Asystole should be treated following current American Heart Association BLS and ACLS guidelines. High-quality CPR is the mainstay of treatment and the most important predictor of favorable outcomes. Asystole is a non-shockable rhythm. Therefore, if asystole is noted on the cardiac monitor, no attempt at defibrillation should be made. High-quality CPR should be continued with minimal (less than five seconds) interruption. CPR should not be stopped to allow for endotracheal intubation. Epinephrine (1 mg via intravenous or intraosseous line) should be delivered every three to five minutes, and treatment of reversible causes addressed. Asystole is considered a terminal rhythm of cardiac arrest. Therefore, discussion of termination of resuscitation should be considered during an in-hospital cardiac arrest in the appropriate clinical picture. Out-of-hospital cardiac arrest patients in asystole should also be considered for the cessation of efforts according to local protocol.[4]
As soon as a patient with asystole is identified, the alarm should be sounded for the cardiac arrest team.
Successful resuscitation
All healthcare workers should be familiar with asystole and its management. Asystole should be treated according to current American Heart Association BLS and ACLS guidelines. High-quality CPR is the mainstay of treatment and the most important predictor of favorable outcomes. Asystole is a non-shockable rhythm. Therefore, if asystole is noted on the cardiac monitor, no attempt at defibrillation should be made. It is mandatory for all healthcare workers who look after patients to be certified in BLS and ACLS in many hospitals.
Sound the alarm as soon as a patient with asystole is identified.
All healthcare workers, including the nurse practitioner, should be familiar with asystole and its management. In the hospital, it is usually the nurse who first identifies a patient in asystole and sounds the alarm.
Asystole should be treated according to current American Heart Association BLS and ACLS guidelines. One person should take charge and control the resuscitation. In all hospitals, there are specially assigned teams consisting of different professionals who attend cardiac arrests. The role of the nurse is to document and provide the necessary supplies. High-quality CPR is the mainstay of treatment and the most important predictor of favorable outcomes. Asystole is a non-shockable rhythm. Therefore, if asystole is noted on the cardiac monitor, no attempt at defibrillation should be made. In many hospitals, it is mandatory for all healthcare workers who look after patients to be certified in BLS and ACLS.
After every resuscitation, the ACLS cart should be refurbished with supplies. One member of the nursing staff should always make sure that the supplies and equipment to run a cardiac arrest are in working order and available.
Pitfalls
Providers should differentiate between asystole and fine ventricular fibrillation, which may respond to defibrillation.
Disclaimer: The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
I am a military service member. This work was prepared as part of my official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person’s official duties.
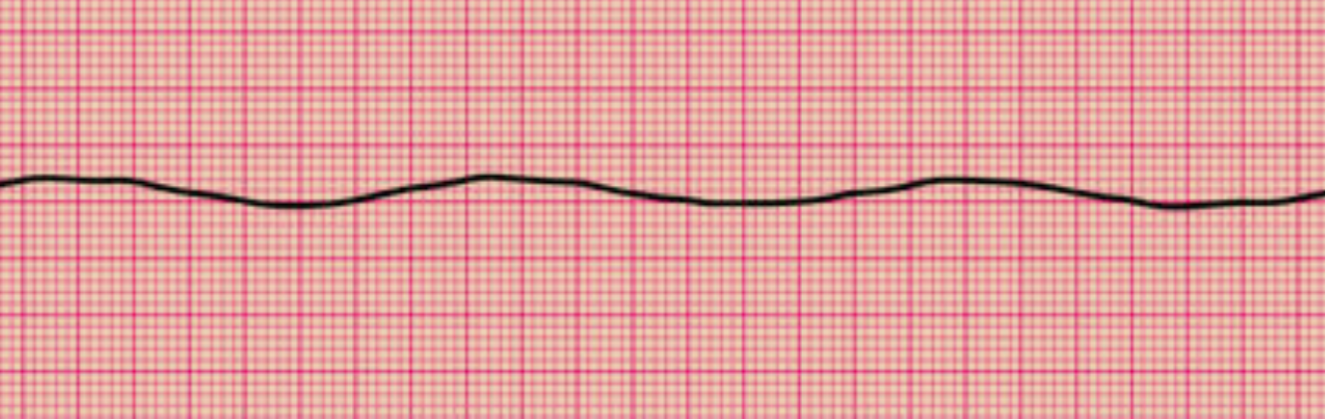
Asystole on Electrocardiography. This rhythm strip shows the total absence of an organized rhythm.
Contributed by Syed Rafay Zaidi, MD
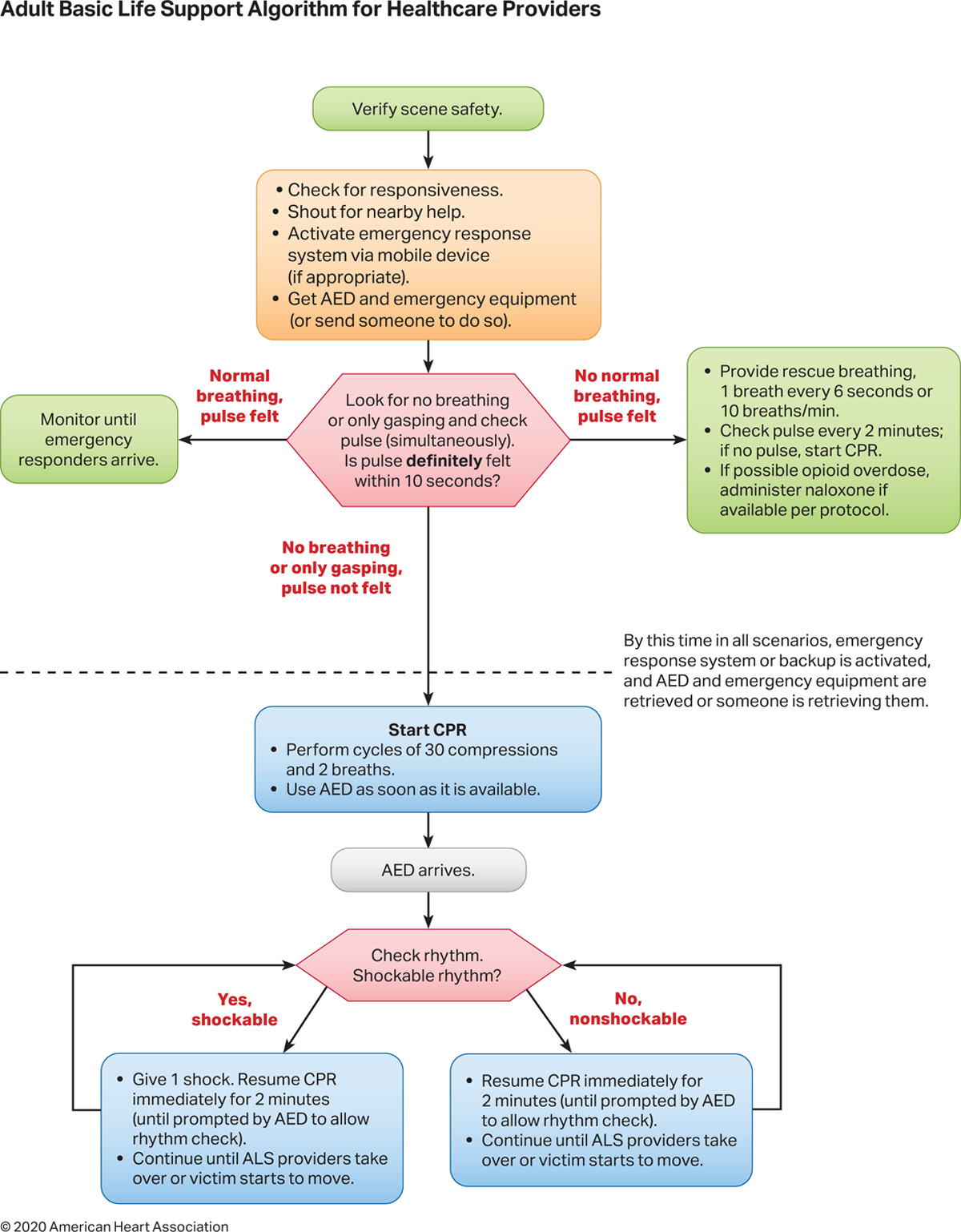
Adult Basic Life Support Algorithm for Healthcare Providers 2020. This diagram shows the initial measures to take when managing cardiac arrest.
https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000000916
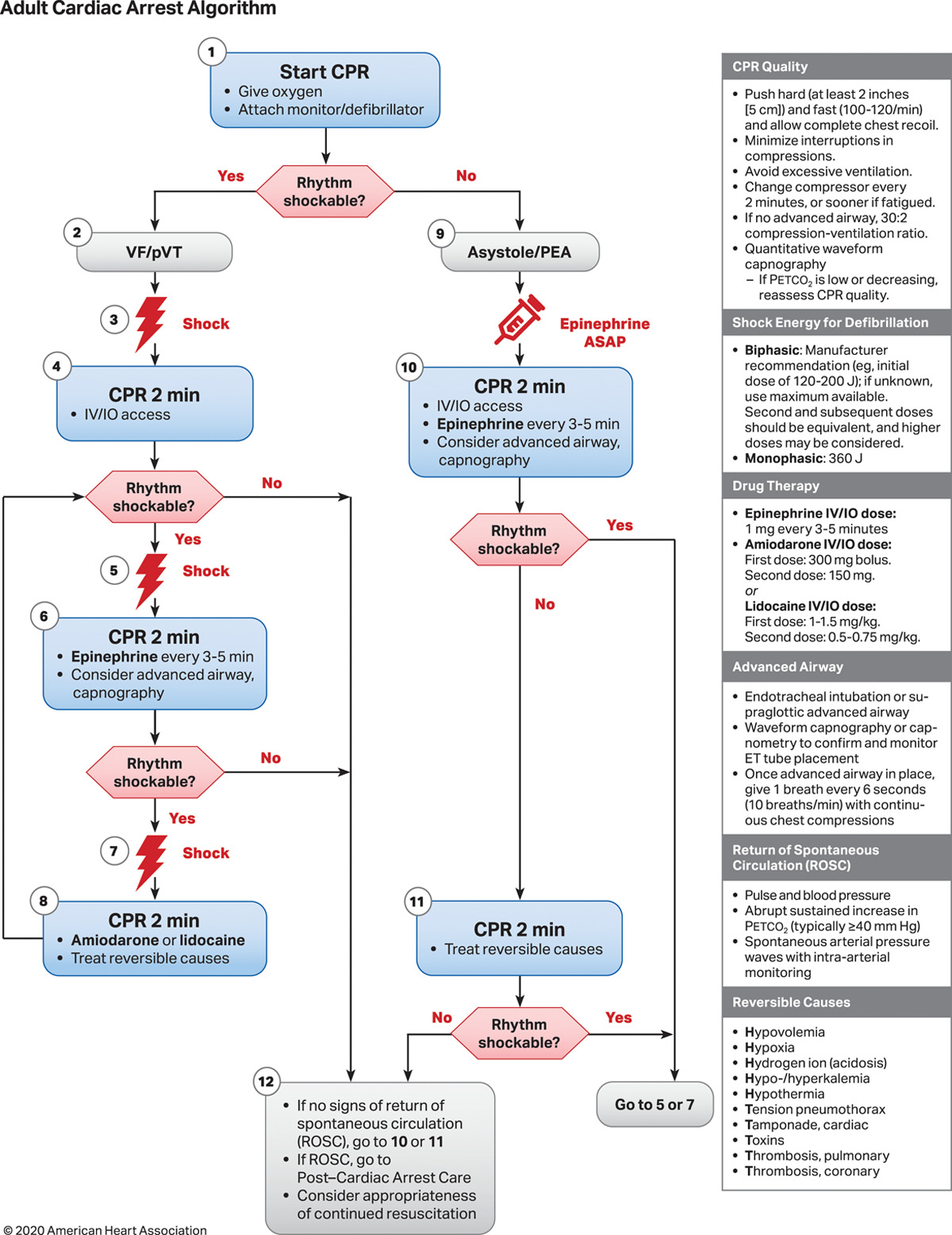
Adult Cardiac Arrest Algorithm 2020. This illustration shows the recommended measures to take when managing persistent cardiac arrest despite basic life fupport.
https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000000916

Ventricular Fibrillation on Electrocardiography. This rhythm strip shows ventricular fibrillation, lacking discernible P waves and having chaotic QRS complexes.
Contributed by Edward Burns M.D.

Monomorphic Ventricular Tachycardia on Electrocardiography. This rhythm strip shows monomorphic ventricular tachycardia, lacking P waves and with similar-looking and rapidly paced QRS complexes.
Contributed From Wikimedia User: Glen Larson (Public Domain)
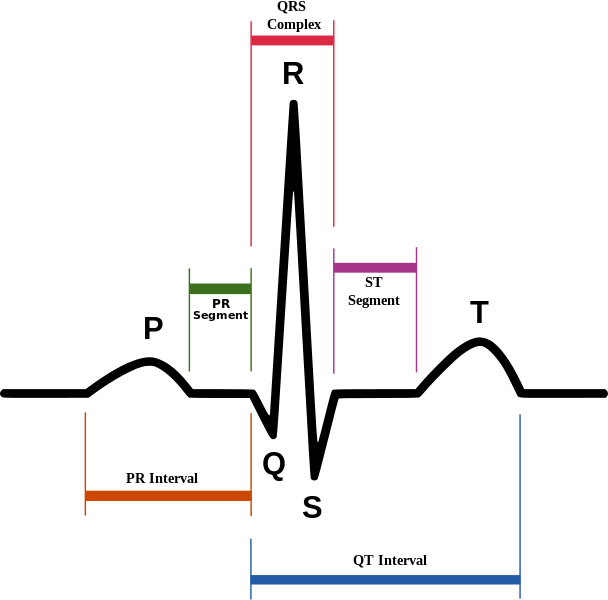
Normal Sinus Rhythm on Electrocardiography. Schematic diagram of normal sinus rhythm on electrocardiography. The P wave, QRS complex, T wave, and PR and ST segments are normal.
Contributed by Wikimedia Commons, Anthony Atkielski (Public Domain-Self)
Ching CK, Leong BS, Nair P, Chan KC, Seow E, Lee F, Heng K, Sewa DW, Lim TW, Chong DTT, Yeo KK, Fong WK, Anantharaman V, Lim SH. Singapore Advanced Cardiac Life Support Guidelines 2021. Singapore medical journal. 2021 Aug:62(8):390-403. doi: 10.11622/smedj.2021109. Epub [PubMed PMID: 35001112]
Hyman MC, Deo R. Post-cardiac arrest evaluation: understanding non-shockable rhythms. European heart journal. 2019 Dec 14:40(47):3835-3837. doi: 10.1093/eurheartj/ehz504. Epub [PubMed PMID: 31408103]
Parish DC, Goyal H, James E, Dane FC. Pulseless Electrical Activity: Echocardiographic Explanation of a Perplexing Phenomenon. Frontiers in cardiovascular medicine. 2021:8():747857. doi: 10.3389/fcvm.2021.747857. Epub 2021 Nov 5 [PubMed PMID: 37528947]
Czapla M, Zielińska M, Kubica-Cielińska A, Diakowska D, Quinn T, Karniej P. Factors associated with return of spontaneous circulation after out-of-hospital cardiac arrest in Poland: a one-year retrospective study. BMC cardiovascular disorders. 2020 Jun 12:20(1):288. doi: 10.1186/s12872-020-01571-5. Epub 2020 Jun 12 [PubMed PMID: 32532201]
de Graaf C, Beesems SG, Koster RW. Time of on-scene resuscitation in out of-hospital cardiac arrest patients transported without return of spontaneous circulation. Resuscitation. 2019 May:138():235-242. doi: 10.1016/j.resuscitation.2019.03.030. Epub 2019 Mar 27 [PubMed PMID: 30928502]
Libby C, Skinner RB, Rawal AR. EMS Termination Of Resuscitation And Pronouncement of Death. StatPearls. 2024 Jan:(): [PubMed PMID: 31082157]
Priest BT, McDermott JS. Cardiac ion channels. Channels (Austin, Tex.). 2015:9(6):352-9. doi: 10.1080/19336950.2015.1076597. Epub 2015 Aug 20 [PubMed PMID: 26556552]
Nagarajan VD, Ho SY, Ernst S. Anatomical Considerations for His Bundle Pacing. Circulation. Arrhythmia and electrophysiology. 2019 Jul:12(7):e006897. doi: 10.1161/CIRCEP.118.006897. Epub 2019 Jul 12 [PubMed PMID: 31296042]
Craig-Brangan KJ, Day MP. AHA update: BLS, ACLS, and PALS. Nursing. 2021 Jun 1:51(6):24-30. doi: 10.1097/01.NURSE.0000751340.92329.ae. Epub [PubMed PMID: 34014872]
Garcia RA, Girotra S, Jones PG, McNally B, Spertus JA, Chan PS, CARES Surveillance Group. Variation in Out-of-Hospital Cardiac Arrest Survival Across Emergency Medical Service Agencies. Circulation. Cardiovascular quality and outcomes. 2022 Jun:15(6):e008755. doi: 10.1161/CIRCOUTCOMES.121.008755. Epub 2022 Jun 14 [PubMed PMID: 35698973]
Varvarousis D, Varvarousi G, Iacovidou N, D'Aloja E, Gulati A, Xanthos T. The pathophysiologies of asphyxial vs dysrhythmic cardiac arrest: implications for resuscitation and post-event management. The American journal of emergency medicine. 2015 Sep:33(9):1297-304. doi: 10.1016/j.ajem.2015.06.066. Epub 2015 Jul 6 [PubMed PMID: 26233618]
Utsumi S, Nishikmi M, Ohshimo S, Shime N. Differences in Pathophysiology and Treatment Efficacy Based on Heterogeneous Out-of-Hospital Cardiac Arrest. Medicina (Kaunas, Lithuania). 2024 Mar 21:60(3):. doi: 10.3390/medicina60030510. Epub 2024 Mar 21 [PubMed PMID: 38541236]
Panchal AR, Bartos JA, Cabañas JG, Donnino MW, Drennan IR, Hirsch KG, Kudenchuk PJ, Kurz MC, Lavonas EJ, Morley PT, O'Neil BJ, Peberdy MA, Rittenberger JC, Rodriguez AJ, Sawyer KN, Berg KM, Adult Basic and Advanced Life Support Writing Group. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020 Oct 20:142(16_suppl_2):S366-S468. doi: 10.1161/CIR.0000000000000916. Epub 2020 Oct 21 [PubMed PMID: 33081529]
Menezes RG, Ahmed S, Pasha SB, Hussain SA, Fatima H, Kharoshah MA, Madadin M. Gastrointestinal causes of sudden unexpected death: A review. Medicine, science, and the law. 2018 Jan:58(1):5-15. doi: 10.1177/0025802417737001. Epub 2017 Nov 15 [PubMed PMID: 29141499]
Pan SY, Tian HM, Zhu Y, Gu WJ, Zou H, Wu XQ, Cheng RJ, Yang Z. Cardiac damage in autoimmune diseases: Target organ involvement that cannot be ignored. Frontiers in immunology. 2022:13():1056400. doi: 10.3389/fimmu.2022.1056400. Epub 2022 Nov 22 [PubMed PMID: 36483559]
Pfeiffer S, Lauridsen KG, Wenger J, Hunt EA, Haskell S, Atkins DL, Duval-Arnould JM, Knight LJ, Cheng A, Gilfoyle E, Su F, Balikai S, Skellett S, Hui MY, Niles DE, Roberts JS, Nadkarni VM, Tegtmeyer K, Dewan M, Pediatric Resuscitation Quality Collaborative Investigators. Code Team Structure and Training in the Pediatric Resuscitation Quality International Collaborative. Pediatric emergency care. 2021 Aug 1:37(8):e431-e435. doi: 10.1097/PEC.0000000000001748. Epub [PubMed PMID: 31045955]