Learning Outcome
- Describe the triggers for asthma
- Recall the presentation of asthma
- Summarize the treatment of asthma
- List nurse management roles in asthma

Asthma is a common disease and has a range of severity, from a very mild, occasional wheeze to an acute, life-threatening airway closure. It usually presents in childhood and is associated with other features of atopy, such as eczema and hayfever.[1][2][3]
Asthma comprises a range of diseases and has a variety of heterogeneous phenotypes. The recognized factors that are associated with asthma are a genetic predisposition, specifically a personal or family history of atopy (propensity to allergy, usually seen as eczema, hay fever, and asthma).[4][5]
Asthma also is associated with exposure to tobacco smoke and other inflammatory gases or particulate matter.
The overall etiology is complex and still not fully understood, especially when it comes to being able to say which children with pediatric asthma will carry on to have asthma as adults (up to 40% of children have a wheeze, only 1% of adults have asthma), but it is agreed that it is a multifactorial pathology, influenced by both genetics and environmental exposure.
Asthma is a common pathology, affecting around 15% to 20% of people in developed countries and around 2% to 4% in less developed countries. It is significantly more common in children. Up to 40% of children will have a wheeze at some point, which, if reversible by beta-2 agonists, is termed asthma, regardless of lung function tests. Asthma is associated with exposure to tobacco smoke and inhaled particulates and is thus more common in groups with these environmental exposures.[6][7]
Patients will usually give a history of a wheeze or a cough, exacerbated by allergies, exercise, and cold. There is often diurnal variation, with symptoms being worse at night. Patients may give a history of other forms of atopy, such as eczema and hay fever. There may be some mild chest pain associated with acute exacerbations.
Physical exam findings will depend on whether the patient is currently experiencing an acute exacerbation.
During an acute exacerbation, there may be a fine tremor in the hands due to salbutamol use, and a mild tachycardia. Patients will show some respiratory distress, often sitting forwards to splint open their airways. On auscultation, a bilateral, expiratory wheeze will be heard. In life-threatening asthma, the chest may be silent, as air cannot enter or leave the lungs, and there may be signs of systemic hypoxia.
Bedside
Pulse oximetry can be useful in assessing the severity of an asthma attack or monitoring for deterioration. Note that pulse oximetry lag, and the physiological reserve of many patients means that a falling pO2 on pulse oximetry is a late finding, indicating a severely unwell or peri-arrest patient.
Peak flow measures also can be used to assess asthma and should always be checked against a nomogram as well as the individual patient's normal baseline function. The different severities of acute asthma attacks have an associated peak flow measurement, recorded as a certain percentage of expected peak flow.
Laboratory
Urea and electrolytes (kidney function) should be taken if the patient has a high dose or repeat salbutamol, as one of the side effects of salbutamol is to cause potassium to shift into the intracellular space transiently, which can induce a transient, iatrogenic hypokalaemia.
Imaging
A chest x-ray is an important test, especially if patients have a history of risk of the potential foreign body or possible infection.
Special Tests
Spirometry is the diagnostic method of choice and will show an obstructive pattern that is partially or completely resolved by salbutamol.
Conservative Measures
Measures to take include calming the patient to get them to relax, moving outside or away from the likely source of allergen, and cooling the person. Removing clothing and washing the face and mouth to remove allergens is sometimes done, but it is not evidence-based.[8][9][10]
Medical
Medical management includes bronchodilators like beta-2 agonists and muscarinic antagonists (salbutamol and ipratropium bromide respectively) and anti-inflammatories such as inhaled steroids (usually beclometasone but steroids via any route will be helpful).
Surgical
There is no surgical input into the management of typical asthma.
Other/Long Term
Weight loss, smoking cessation, occupational change, and self-monitoring are all important in preventing disease progression and reducing the number of acute attacks.
In many countries, including the US, asthma kills one out of every 100,000 persons. The worse the lung function, the higher the mortality. In addition, mortality has also been linked to poor management and lack of medication compliance, especially in young people. Other factors that increase the risk of death include smoking and use of illicit drugs.
Asthma also results in millions of school and work days lost. In the US alone, close to 2 million asthmatics seek regular care in the emergency department, which also increases the costs of healthcare.
Even though asthma is a reversible disorder, poor lifestyle and lack of management can lead to airway remodeling that leads to chronic symptoms, which are disabling.[11]
Evidence-based Medicine
Many guidelines have been published for the diagnosis and management of asthma, but the most critical feature is patient education. The nurses are the last professionals to see the patient before discharge from the emergency department or the floors. Similarly, since most asthmatics are treated as outpatients, pharmacists encounter them regularly. Evidence shows that teaching patients about this disorder and the importance of compliance are critical for good outcomes. The patient should be taught about monitoring technique, inhaler use, and modifying the environment. Many evidence-based asthma plans are available for the management of asthma and should be handed out to patients. Finally, nurses also play a vital role in school-based asthma education programs that can help improve self-esteem, knowledge and self-management behaviors.[12][13][14] (Level II)
Outcomes
Despite great awareness of the disease, asthma still results in high morbidity and even mortality. There are universal guidelines on managing the disorder, but patient compliance with medications remains a big problem. Hence, all healthcare workers have a responsibility in encouraging medication compliance and close follow up with the primary care physician.[15][16](Level V)
Patient education about the disease and modifying behavior is vital. The patient should also be encouraged to change lifestyle and control the environmental trigger factors.
Call MD if:
Take medications as prescribed
Avoid triggers like pet dander, tobacco and dust
Control the environment and avoid triggers to reduce asthma episodes.
Disposition
If the patient requires nebulized salbutamol and is not ordinarily on home nebulizers, he or she should be admitted. Anyone who has presented with severe or life-threatening asthma should usually be monitored to ensure that the disease does not return when the medication has worn off.
Pitfalls
Issues include forgetting to remove the nebulizer mask once the nebulizer is done (thus leaving the patient on only 6L of 02/min, rather than changing them to 15 L/min via a non-rebreather mask), not assessing inhaler technique, and neglecting to stress the importance of maintenance therapy with inhaled steroids even when the patient is well.
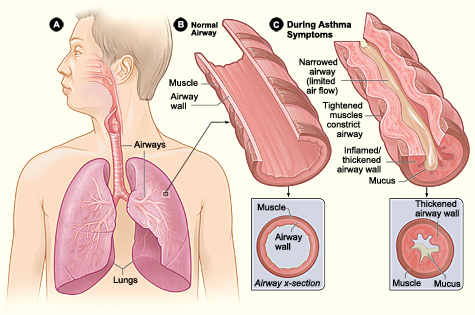
Pathophysiology of Asthma. Figure A displays the location of the lungs and airways in the body. Figure B shows a cross section of a normal airway. Figure C illustrates a cross section of an airway during asthma symptoms
National Institutes of Health
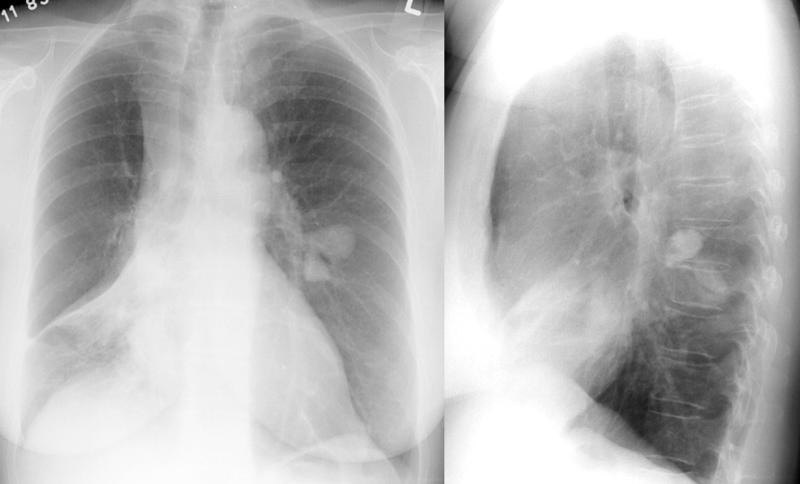
A Chest Radiograph Depicting Asthma. The image depicts both anterior and lateral radiographs of a patient with asthma. The image highlights the presence of pneumomediastinum and increased bronchovascular markings.
Contributed by H Shulman, MD
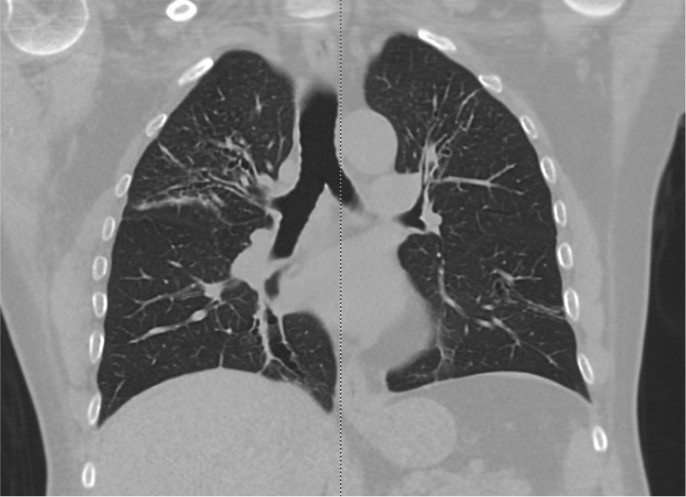
Allergic Bronchopulmonary Aspergillosis on CT Scan. Computed tomography (CT) images reveal bronchiectasis in both upper lobes of a patient with bronchial asthma, indicative of allergic bronchopulmonary aspergillosis.
Contributed by M Salahuddin, MD
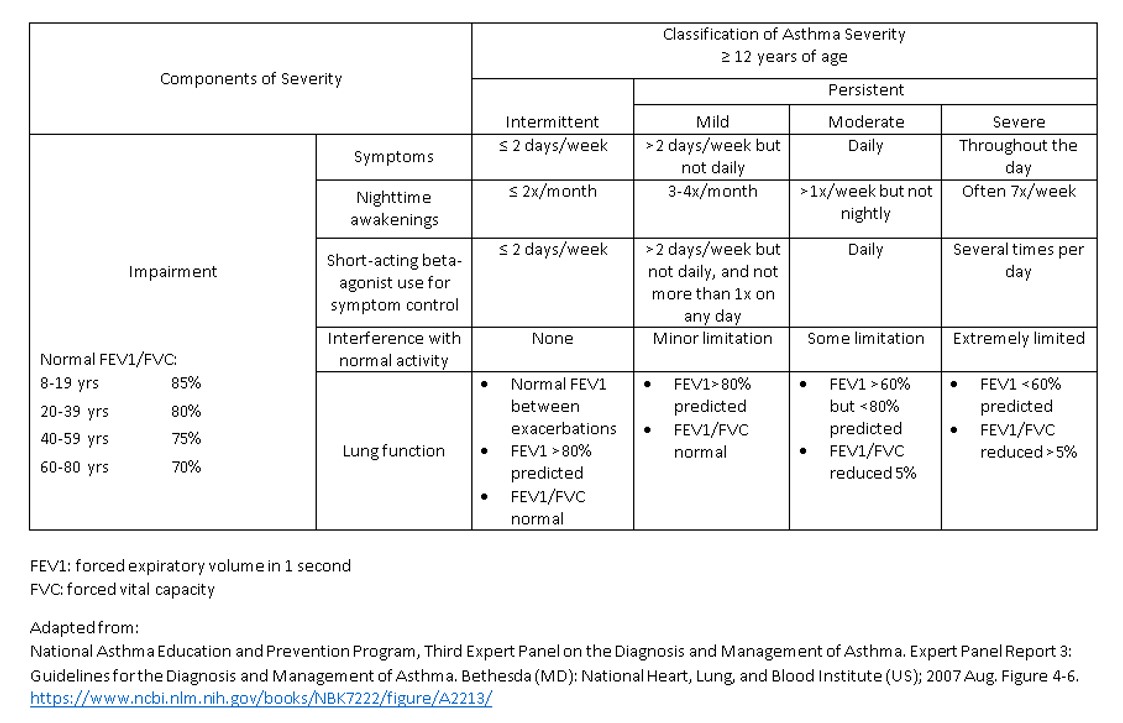
Asthma Severity Classification by The National Asthma Education and Prevention Program.
Contributed by R Chabra, DO
Lee J, McDonald C. Review: Immunotherapy improves some symptoms and reduces long-term medication use in mild to moderate asthma. Annals of internal medicine. 2018 Aug 21:169(4):JC17. doi: 10.7326/ACPJC-2018-169-4-017. Epub [PubMed PMID: 30128507]
Tesfaye ZT, Gebreselase NT, Horsa BA. Appropriateness of chronic asthma management and medication adherence in patients visiting ambulatory clinic of Gondar University Hospital: a cross-sectional study. The World Allergy Organization journal. 2018:11(1):18. doi: 10.1186/s40413-018-0196-1. Epub 2018 Aug 10 [PubMed PMID: 30128064]
Salo PM, Cohn RD, Zeldin DC. Bedroom Allergen Exposure Beyond House Dust Mites. Current allergy and asthma reports. 2018 Aug 20:18(10):52. doi: 10.1007/s11882-018-0805-7. Epub 2018 Aug 20 [PubMed PMID: 30128784]
Piloni D, Tirelli C, Domenica RD, Conio V, Grosso A, Ronzoni V, Antonacci F, Totaro P, Corsico AG. Asthma-like symptoms: is it always a pulmonary issue? Multidisciplinary respiratory medicine. 2018:13():21. doi: 10.1186/s40248-018-0136-5. Epub 2018 Aug 3 [PubMed PMID: 30123502]
Aggarwal B, Mulgirigama A, Berend N. Exercise-induced bronchoconstriction: prevalence, pathophysiology, patient impact, diagnosis and management. NPJ primary care respiratory medicine. 2018 Aug 14:28(1):31. doi: 10.1038/s41533-018-0098-2. Epub 2018 Aug 14 [PubMed PMID: 30108224]
Gui H, Levin AM, Hu D, Sleiman P, Xiao S, Mak ACY, Yang M, Barczak AJ, Huntsman S, Eng C, Hochstadt S, Zhang E, Whitehouse K, Simons S, Cabral W, Takriti S, Abecasis G, Blackwell TW, Kang HM, Nickerson DA, Germer S, Lanfear DE, Gilliland F, Gauderman WJ, Kumar R, Erle DJ, Martinez FD, Hakonarson H, Burchard EG, Williams LK. Mapping the 17q12-21.1 Locus for Variants Associated with Early-Onset Asthma in African Americans. American journal of respiratory and critical care medicine. 2021 Feb 15:203(4):424-436. doi: 10.1164/rccm.202006-2623OC. Epub [PubMed PMID: 32966749]
Torgerson DG, Ampleford EJ, Chiu GY, Gauderman WJ, Gignoux CR, Graves PE, Himes BE, Levin AM, Mathias RA, Hancock DB, Baurley JW, Eng C, Stern DA, Celedón JC, Rafaels N, Capurso D, Conti DV, Roth LA, Soto-Quiros M, Togias A, Li X, Myers RA, Romieu I, Van Den Berg DJ, Hu D, Hansel NN, Hernandez RD, Israel E, Salam MT, Galanter J, Avila PC, Avila L, Rodriquez-Santana JR, Chapela R, Rodriguez-Cintron W, Diette GB, Adkinson NF, Abel RA, Ross KD, Shi M, Faruque MU, Dunston GM, Watson HR, Mantese VJ, Ezurum SC, Liang L, Ruczinski I, Ford JG, Huntsman S, Chung KF, Vora H, Li X, Calhoun WJ, Castro M, Sienra-Monge JJ, del Rio-Navarro B, Deichmann KA, Heinzmann A, Wenzel SE, Busse WW, Gern JE, Lemanske RF Jr, Beaty TH, Bleecker ER, Raby BA, Meyers DA, London SJ, Mexico City Childhood Asthma Study (MCAAS), Gilliland FD, Children's Health Study (CHS) and HARBORS study, Burchard EG, Genetics of Asthma in Latino Americans (GALA) Study, Study of Genes-Environment and Admixture in Latino Americans (GALA2) and Study of African Americans, Asthma, Genes & Environments (SAGE), Martinez FD, Childhood Asthma Research and Education (CARE) Network, Weiss ST, Childhood Asthma Management Program (CAMP), Williams LK, Study of Asthma Phenotypes and Pharmacogenomic Interactions by Race-Ethnicity (SAPPHIRE), Barnes KC, Genetic Research on Asthma in African Diaspora (GRAAD) Study, Ober C, Nicolae DL. Meta-analysis of genome-wide association studies of asthma in ethnically diverse North American populations. Nature genetics. 2011 Jul 31:43(9):887-92. doi: 10.1038/ng.888. Epub 2011 Jul 31 [PubMed PMID: 21804549]
Parnes JR, Molfino NA, Colice G, Martin U, Corren J, Menzies-Gow A. Targeting TSLP in Asthma. Journal of asthma and allergy. 2022:15():749-765. doi: 10.2147/JAA.S275039. Epub 2022 Jun 3 [PubMed PMID: 35685846]
Fishe JN, Labilloy G, Higley R, Casey D, Ginn A, Baskovich B, Blake KV. Single Nucleotide Polymorphisms (SNPs) in PRKG1 & SPATA13-AS1 are associated with bronchodilator response: a pilot study during acute asthma exacerbations in African American children. Pharmacogenetics and genomics. 2021 Sep 1:31(7):146-154. doi: 10.1097/FPC.0000000000000434. Epub [PubMed PMID: 33851947]
Loss GJ, Depner M, Hose AJ, Genuneit J, Karvonen AM, Hyvärinen A, Roduit C, Kabesch M, Lauener R, Pfefferle PI, Pekkanen J, Dalphin JC, Riedler J, Braun-Fahrländer C, von Mutius E, Ege MJ, PASTURE (Protection against Allergy Study in Rural Environments) Study Group. The Early Development of Wheeze. Environmental Determinants and Genetic Susceptibility at 17q21. American journal of respiratory and critical care medicine. 2016 Apr 15:193(8):889-97. doi: 10.1164/rccm.201507-1493OC. Epub [PubMed PMID: 26575599]
Jaakkola JJ, Ahmed P, Ieromnimon A, Goepfert P, Laiou E, Quansah R, Jaakkola MS. Preterm delivery and asthma: a systematic review and meta-analysis. The Journal of allergy and clinical immunology. 2006 Oct:118(4):823-30 [PubMed PMID: 17030233]
Been JV, Lugtenberg MJ, Smets E, van Schayck CP, Kramer BW, Mommers M, Sheikh A. Preterm birth and childhood wheezing disorders: a systematic review and meta-analysis. PLoS medicine. 2014 Jan:11(1):e1001596. doi: 10.1371/journal.pmed.1001596. Epub 2014 Jan 28 [PubMed PMID: 24492409]
Leps C, Carson C, Quigley MA. Gestational age at birth and wheezing trajectories at 3-11 years. Archives of disease in childhood. 2018 Dec:103(12):1138-1144. doi: 10.1136/archdischild-2017-314541. Epub 2018 Jun 2 [PubMed PMID: 29860226]
Crump C, Sundquist J, Sundquist K. Preterm or early term birth and long-term risk of asthma into midadulthood: a national cohort and cosibling study. Thorax. 2023 Jul:78(7):653-660. doi: 10.1136/thorax-2022-218931. Epub 2022 Jul 30 [PubMed PMID: 35907641]
Castro-Rodriguez JA, Forno E, Rodriguez-Martinez CE, Celedón JC. Risk and Protective Factors for Childhood Asthma: What Is the Evidence? The journal of allergy and clinical immunology. In practice. 2016 Nov-Dec:4(6):1111-1122. doi: 10.1016/j.jaip.2016.05.003. Epub 2016 Jun 8 [PubMed PMID: 27286779]
Wolsk HM, Chawes BL, Litonjua AA, Hollis BW, Waage J, Stokholm J, Bønnelykke K, Bisgaard H, Weiss ST. Prenatal vitamin D supplementation reduces risk of asthma/recurrent wheeze in early childhood: A combined analysis of two randomized controlled trials. PloS one. 2017:12(10):e0186657. doi: 10.1371/journal.pone.0186657. Epub 2017 Oct 27 [PubMed PMID: 29077711]
Litonjua AA, Weiss ST. Is vitamin D deficiency to blame for the asthma epidemic? The Journal of allergy and clinical immunology. 2007 Nov:120(5):1031-5 [PubMed PMID: 17919705]
McEvoy CT, Schilling D, Clay N, Jackson K, Go MD, Spitale P, Bunten C, Leiva M, Gonzales D, Hollister-Smith J, Durand M, Frei B, Buist AS, Peters D, Morris CD, Spindel ER. Vitamin C supplementation for pregnant smoking women and pulmonary function in their newborn infants: a randomized clinical trial. JAMA. 2014 May:311(20):2074-82. doi: 10.1001/jama.2014.5217. Epub [PubMed PMID: 24838476]
McEvoy CT, Shorey-Kendrick LE, Milner K, Schilling D, Tiller C, Vuylsteke B, Scherman A, Jackson K, Haas DM, Harris J, Schuff R, Park BS, Vu A, Kraemer DF, Mitchell J, Metz J, Gonzales D, Bunten C, Spindel ER, Tepper RS, Morris CD. Oral Vitamin C (500 mg/d) to Pregnant Smokers Improves Infant Airway Function at 3 Months (VCSIP). A Randomized Trial. American journal of respiratory and critical care medicine. 2019 May 1:199(9):1139-1147. doi: 10.1164/rccm.201805-1011OC. Epub [PubMed PMID: 30522343]
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England). 2020 Oct 17:396(10258):1204-1222. doi: 10.1016/S0140-6736(20)30925-9. Epub [PubMed PMID: 33069326]
Mortimer K, Lesosky M, García-Marcos L, Asher MI, Pearce N, Ellwood E, Bissell K, El Sony A, Ellwood P, Marks GB, Martínez-Torres A, Morales E, Perez-Fernandez V, Robertson S, Rutter CE, Silverwood RJ, Strachan DP, Chiang CY, Global Asthma Network Phase I Study Group. The burden of asthma, hay fever and eczema in adults in 17 countries: GAN Phase I study. The European respiratory journal. 2022 Sep:60(3):. doi: 10.1183/13993003.02865-2021. Epub 2022 Sep 15 [PubMed PMID: 35210319]
Pate CA, Zahran HS, Qin X, Johnson C, Hummelman E, Malilay J. Asthma Surveillance - United States, 2006-2018. Morbidity and mortality weekly report. Surveillance summaries (Washington, D.C. : 2002). 2021 Sep 17:70(5):1-32. doi: 10.15585/mmwr.ss7005a1. Epub 2021 Sep 17 [PubMed PMID: 34529643]
Liu MC, Hubbard WC, Proud D, Stealey BA, Galli SJ, Kagey-Sobotka A, Bleecker ER, Lichtenstein LM. Immediate and late inflammatory responses to ragweed antigen challenge of the peripheral airways in allergic asthmatics. Cellular, mediator, and permeability changes. The American review of respiratory disease. 1991 Jul:144(1):51-8 [PubMed PMID: 2064141]
Riccio MM, Proud D. Evidence that enhanced nasal reactivity to bradykinin in patients with symptomatic allergy is mediated by neural reflexes. The Journal of allergy and clinical immunology. 1996 Jun:97(6):1252-63 [PubMed PMID: 8648021]
Limb SL, Brown KC, Wood RA, Wise RA, Eggleston PA, Tonascia J, Adkinson NF Jr. Irreversible lung function deficits in young adults with a history of childhood asthma. The Journal of allergy and clinical immunology. 2005 Dec:116(6):1213-9 [PubMed PMID: 16337448]
Förster-Ruhrmann U, Olze H. [Importance of aspirin challenges in patients with NSAID-exacerbated respiratory disease]. HNO. 2024 Apr 10:():. doi: 10.1007/s00106-024-01460-9. Epub 2024 Apr 10 [PubMed PMID: 38597968]
Lee DL, Baptist AP. Understanding the Updates in the Asthma Guidelines. Seminars in respiratory and critical care medicine. 2022 Oct:43(5):595-612. doi: 10.1055/s-0042-1745747. Epub 2022 Jun 21 [PubMed PMID: 35728605]
Stanojevic S, Kaminsky DA, Miller MR, Thompson B, Aliverti A, Barjaktarevic I, Cooper BG, Culver B, Derom E, Hall GL, Hallstrand TS, Leuppi JD, MacIntyre N, McCormack M, Rosenfeld M, Swenson ER. ERS/ATS technical standard on interpretive strategies for routine lung function tests. The European respiratory journal. 2022 Jul:60(1):. pii: 2101499. doi: 10.1183/13993003.01499-2021. Epub 2022 Jul 13 [PubMed PMID: 34949706]
Tsuyuki RT, Midodzi W, Villa-Roel C, Marciniuk D, Mayers I, Vethanayagam D, Chan M, Rowe BH. Diagnostic practices for patients with shortness of breath and presumed obstructive airway disorders: a cross-sectional analysis. CMAJ open. 2020 Jul-Sep:8(3):E605-E612. doi: 10.9778/cmajo.20190168. Epub 2020 Sep 25 [PubMed PMID: 32978240]
Aaron SD, Vandemheen KL, FitzGerald JM, Ainslie M, Gupta S, Lemière C, Field SK, McIvor RA, Hernandez P, Mayers I, Mulpuru S, Alvarez GG, Pakhale S, Mallick R, Boulet LP, Canadian Respiratory Research Network. Reevaluation of Diagnosis in Adults With Physician-Diagnosed Asthma. JAMA. 2017 Jan 17:317(3):269-279. doi: 10.1001/jama.2016.19627. Epub [PubMed PMID: 28114551]
Coates AL, Wanger J, Cockcroft DW, Culver BH, Bronchoprovocation Testing Task Force: Kai-Håkon Carlsen, Diamant Z, Gauvreau G, Hall GL, Hallstrand TS, Horvath I, de Jongh FHC, Joos G, Kaminsky DA, Laube BL, Leuppi JD, Sterk PJ. ERS technical standard on bronchial challenge testing: general considerations and performance of methacholine challenge tests. The European respiratory journal. 2017 May:49(5):. pii: 1601526. doi: 10.1183/13993003.01526-2016. Epub 2017 May 1 [PubMed PMID: 28461290]
Gauvreau GM, O'Byrne PM, Boulet LP, Wang Y, Cockcroft D, Bigler J, FitzGerald JM, Boedigheimer M, Davis BE, Dias C, Gorski KS, Smith L, Bautista E, Comeau MR, Leigh R, Parnes JR. Effects of an anti-TSLP antibody on allergen-induced asthmatic responses. The New England journal of medicine. 2014 May 29:370(22):2102-10. doi: 10.1056/NEJMoa1402895. Epub 2014 May 20 [PubMed PMID: 24846652]
Dhuper S, Chandra A, Ahmed A, Bista S, Moghekar A, Verma R, Chong C, Shim C, Cohen H, Choksi S. Efficacy and cost comparisons of bronchodilatator administration between metered dose inhalers with disposable spacers and nebulizers for acute asthma treatment. The Journal of emergency medicine. 2011 Mar:40(3):247-55. doi: 10.1016/j.jemermed.2008.06.029. Epub 2008 Dec 11 [PubMed PMID: 19081697]
Cates CJ, Welsh EJ, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. The Cochrane database of systematic reviews. 2013 Sep 13:2013(9):CD000052. doi: 10.1002/14651858.CD000052.pub3. Epub 2013 Sep 13 [PubMed PMID: 24037768]
Newman KB, Milne S, Hamilton C, Hall K. A comparison of albuterol administered by metered-dose inhaler and spacer with albuterol by nebulizer in adults presenting to an urban emergency department with acute asthma. Chest. 2002 Apr:121(4):1036-41 [PubMed PMID: 11948030]
Normansell R, Kew KM, Mansour G. Different oral corticosteroid regimens for acute asthma. The Cochrane database of systematic reviews. 2016 May 13:2016(5):CD011801. doi: 10.1002/14651858.CD011801.pub2. Epub 2016 May 13 [PubMed PMID: 27176676]
Kew KM, Kirtchuk L, Michell CI. Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department. The Cochrane database of systematic reviews. 2014 May 28:2014(5):CD010909. doi: 10.1002/14651858.CD010909.pub2. Epub 2014 May 28 [PubMed PMID: 24865567]
Rovsing AH, Savran O, Ulrik CS. Magnesium sulfate treatment for acute severe asthma in adults-a systematic review and meta-analysis. Frontiers in allergy. 2023:4():1211949. doi: 10.3389/falgy.2023.1211949. Epub 2023 Jul 28 [PubMed PMID: 37577333]
Knightly R, Milan SJ, Hughes R, Knopp-Sihota JA, Rowe BH, Normansell R, Powell C. Inhaled magnesium sulfate in the treatment of acute asthma. The Cochrane database of systematic reviews. 2017 Nov 28:11(11):CD003898. doi: 10.1002/14651858.CD003898.pub6. Epub 2017 Nov 28 [PubMed PMID: 29182799]
Stefan MS, Nathanson BH, Lagu T, Priya A, Pekow PS, Steingrub JS, Hill NS, Goldberg RJ, Kent DM, Lindenauer PK. Outcomes of Noninvasive and Invasive Ventilation in Patients Hospitalized with Asthma Exacerbation. Annals of the American Thoracic Society. 2016 Jul:13(7):1096-104. doi: 10.1513/AnnalsATS.201510-701OC. Epub [PubMed PMID: 27070493]
Soroksky A, Stav D, Shpirer I. A pilot prospective, randomized, placebo-controlled trial of bilevel positive airway pressure in acute asthmatic attack. Chest. 2003 Apr:123(4):1018-25 [PubMed PMID: 12684289]
Nair P, Milan SJ, Rowe BH. Addition of intravenous aminophylline to inhaled beta(2)-agonists in adults with acute asthma. The Cochrane database of systematic reviews. 2012 Dec 12:12(12):CD002742. doi: 10.1002/14651858.CD002742.pub2. Epub 2012 Dec 12 [PubMed PMID: 23235591]
Cremer NM, Baptist AP. Race and Asthma Outcomes in Older Adults: Results from the National Asthma Survey. The journal of allergy and clinical immunology. In practice. 2020 Apr:8(4):1294-1301.e7. doi: 10.1016/j.jaip.2019.12.014. Epub 2020 Feb 5 [PubMed PMID: 32035849]
Nardone A, Casey JA, Morello-Frosch R, Mujahid M, Balmes JR, Thakur N. Associations between historical residential redlining and current age-adjusted rates of emergency department visits due to asthma across eight cities in California: an ecological study. The Lancet. Planetary health. 2020 Jan:4(1):e24-e31. doi: 10.1016/S2542-5196(19)30241-4. Epub [PubMed PMID: 31999951]
Song WJ, Lee JH, Kang Y, Joung WJ, Chung KF. Future Risks in Patients With Severe Asthma. Allergy, asthma & immunology research. 2019 Nov:11(6):763-778. doi: 10.4168/aair.2019.11.6.763. Epub [PubMed PMID: 31552713]