Learning Outcome
- List the causes of acute respiratory distress syndrome (ARDS)
- Describe the presentation of ARDS
- Summarize the treatment of ARDS
- Discuss the role of the nurse in the management of ARDS

Acute respiratory distress syndrome (ARDS) is a life-threatening condition of seriously ill patients, characterized by poor oxygenation, pulmonary infiltrates, and acute onset. On a microscopic level, the disorder is associated with capillary endothelial injury and diffuse alveolar damage.
ARDS is an acute disorder characterized by bilateral lung infiltrates and severe progressive hypoxemia in the absence of any evidence of cardiogenic pulmonary edema. ARDS is defined by the patient's oxygen in arterial blood (PaO2) to the fraction of the oxygen in the inspired air (FiO2). These patients usually have a PaO2/FiO2 ratio of less than 200.
Once ARDS develops, patients usually have varying degrees of pulmonary artery vasoconstriction and may subsequently develop pulmonary hypertension. ARDS carries a high mortality, and few effective therapeutic modalities exist to combat this condition.[1][2]
ARDS has many risk factors. Besides pulmonary infection or aspiration, extra-pulmonary sources include sepsis, trauma, massive transfusion, drowning, drug overdose, fat embolism, inhalation of toxic fumes, and pancreatitis. These extra-thoracic illnesses and/or injuries trigger an inflammatory cascade culminating in pulmonary injury.[3]
Estimates of ARDS incidence in the United States range from 64.2 to 78.9 cases/100,000 person-years. Twenty-five percent of ARDS cases are initially classified as mild, and 75% as moderate or severe. However, a third of the mild cases progress to moderate or severe disease.[1] A literature review revealed a mortality decrease of 1.1% per year for the period 1994 through 2006. However, the overall pooled mortality rate for all the studies evaluated was 43%.[2]
Risk factors for ARDS include:
The syndrome is characterized by the development of dyspnea and hypoxemia, which progressively worsens within hours to days, frequently requiring mechanical ventilation and intensive care unit-level care. The history is directed at identifying the underlying cause which has precipitated the disease. When interviewing patients that can communicate, they often start to complain of mild dyspnea initially, but within 12 to 24 hours, the respiratory distress escalates, becoming severe and requiring mechanical ventilation to prevent hypoxia. The etiology may be obvious in the case of pneumonia or sepsis. However, in other cases, questioning the patient or relatives on recent exposures may also be paramount in identifying the causative agent.
The physical examination will include findings associated with the respiratory system, such as tachypnea and increased breathing effort. Systemic signs may also be evident depending on the severity of the illness, such as central or peripheral cyanosis resulting from hypoxemia, tachycardia, and altered mental status. Despite 100% oxygen, patients have low oxygen saturation. Chest auscultation usually reveals rales, especially bibasilar, but they are often auscultated throughout the chest.
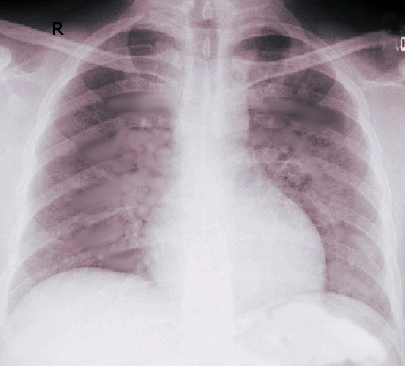
The diagnosis of ARDS is based on the following criteria: acute onset, bilateral lung infiltrates on chest radiography of a non-cardiac origin, and a PaO/FiO ratio of less than 300 mmHg. It is further sub-classified into mild (PaO2/FiO2 200 to 300 mmHg), moderate (PaO2/FiO2 100 to 200 mmHg), and severe (PaO2/FiO2 less than 100 mmHg) subtypes. Mortality and ventilator-free days increase with severity. A CT scan of the chest may be required in pneumothorax cases, pleural effusions, mediastinal lymphadenopathy, or barotrauma to properly identify infiltrates as pulmonic in location.
Assessment of left ventricular function may be required to differentiate from or quantify the contribution of congestive heart failure to the overall clinical picture. This assessment can be achieved via invasive methods, such as pulmonary artery catheter measurements, or non-invasively, such as cardiac echocardiography, thoracic bioimpedance, or pulse contour analysis. However, using pulmonary artery catheters is controversial and should be avoided if clinically possible, and noninvasive measures for assessment should be exhausted first. Bronchoscopy may be required to assess pulmonary infections and obtain material for culture.
Other laboratory and/or radiographic tests will be guided by the underlying disease process, which has triggered the inflammatory process that has led to the development of ARDS. Also, laboratory tests will be needed as patients with ARDS are highly likely to develop or be affected by associated multi-organ failure, including but not limited to renal, hepatic, and hematopoietic failures. Regularly obtaining complete blood count with differential, comprehensive metabolic panel, serum magnesium, serum ionized calcium, phosphorus levels, blood lactate level, coagulation panel, troponin, cardiac enzymes, and CKMB are recommended if clinically indicated.[3][4][5]
Unfortunately, no drug has been proven effective in preventing or managing ARDS. The chief treatment strategy is supportive care, along with adequate nutrition. Patients are mechanically ventilated, guarded against fluid overload with diuretics, and given nutritional support until evidence of improvement is observed. Interestingly, the mode in which a patient is ventilated affects lung recovery. Evidence suggests that some ventilatory strategies can exacerbate alveolar damage and perpetuate lung injury in the context of ARDS. Care focuses on preventing volutrauma (exposure to large tidal volumes), barotrauma (exposure to high plateau pressures), and atelectrauma (exposure to atelectasis).[1][6]
A lung-protective ventilatory strategy is advocated to reduce lung injury. The NIH-NHLBI ARDS Clinical Network Mechanical Ventilation Protocol (ARDSnet) sets the following goals: Tidal volume (V) from 4 to 8 mL/kg of ideal body weight (IBW), respiratory rate (RR) up to 35 bpm, SpO2 88% to 95%, plateau pressure (P) less than 30 cm H2O, pH goal 7.30 to 7.45, and inspiratory-to-expiratory time ratio less than 1. To maintain oxygenation, ARDSnet recognizes the benefit of PEEP. The protocol allows for a low or a high PEEP strategy relative to FiO2. Either strategy tolerates a PEEP of up to 24 cm HO in patients requiring 100% FiO2. The inspiratory-to-expiratory time ratio goal may need to be sacrificed and an inverse inspiratory-to-expiratory time ratio strategy instituted to improve oxygenation in a certain clinical situation.
Novel invasive ventilation strategies have been developed to improve oxygenation. These include airway pressure release ventilation and high-frequency oscillation ventilation. These open-lung ventilation strategies can be supplemented with recruitment maneuvers. Patients with mild and some with moderate ARDS may benefit from non-invasive ventilation to avoid endotracheal intubation and invasive mechanical ventilation. These modalities include continuous positive airway pressure (CPAP), bi-level airway pressure (BiPAP), proportional-assist ventilation, and high-flow nasal cannula.
A plateau pressure of less than 30 cm HO can be achieved using several strategies. Again, this is to reduce the risk of barotrauma. One strategy is to maintain as low a V and PEEP as possible. Also, increasing the rise and/or inspiration times can help maintain the P goal. Finally, the flow rate can be decreased as an adjunct to decreasing the P. High P is also a product of decreased lung compliance from non-cardiogenic pulmonary edema, a salient feature of ARDS pathophysiology.
Improving lung compliance will improve P and oxygenation goal attainment. Neuromuscular blockade has been used in this endeavor. Neuromuscular blockers instituted during the first 48 hours of ARDS improved 90-day survival and increased time off the ventilator.[12] Other causes of decreased lung compliance should be sought and addressed. These include, but are not limited to, pneumothorax, hemothorax, thoracic compartment syndrome, and intraabdominal hypertension. Prone position has shown benefits in about 50% to 70% of patients. The improvement in oxygenation is rapid and allows a reduction in FiO2 and PEEP. The prone position is safe, but there is a risk of dislodgement of lines and tubes. It is believed that in the prone position, there is the recruitment of dependent lung zones, improved diaphragmatic excursion, and increased functional residual capacity. To derive the benefits, the patient needs to be maintained in a prone position for at least 8 hours a day.
Non-ventilatory strategies have included prone positioning and conservative fluid management once resuscitation has been achieved.[14][7][8] Extracorporeal membrane oxygenation (ECMO) has recently been advocated as salvage therapy in refractory hypoxemic ARDS.[9] Nutritional support via enteral feeding is recommended. A high-fat, low-carbohydrate diet containing gamma-linolenic acid and eicosapentaenoic acid has been shown in some studies to improve oxygenation. Care is also necessary to prevent pressure sores; thus, frequent patient repositioning or turning is recommended when feasible. Skin checks per nursing routine are also advised. Physical therapy should be involved in exercising the patient when they are liberated from mechanical ventilation and stable to participate in therapy.
The outcomes for most patients with ARDS are guarded. Even those who recover have a prolonged recovery, marked by muscle wasting, polyneuropathy, and weakness.
ICU care with continuous monitoring.
ARDS is a serious disorder of the lung which has the potential to cause death. Patients with ARDS may require mechanical ventilation because of hypoxia.[10] The management is usually in the ICU with an interprofessional healthcare team. ARDS has effects beyond the lung. Prolonged mechanical ventilation often leads to bedsores, deep venous thrombosis, multi-organ failure, weight loss, and poor overall functioning. It is important to have an integrated approach to ARDS management because it usually affects many organs in the body. These patients need nutritional support, chest physiotherapy, treatment for sepsis if present, and potentially hemodialysis. Many of these patients remain in the hospital for months, and even those who survive face severe challenges due to a loss of muscle mass and cognitive changes (due to hypoxia). There is ample evidence showing that an interprofessional team approach leads to better outcomes as it facilitates communication and ensures timely intervention.[11] The team and responsibilities should consist of the following:
Outcomes
Despite advances in critical care, ARDS still has high morbidity and mortality. Even those who survive can have a poorer quality of life. While many risk factors are known for ARDS, there is no way to prevent the condition. Besides restricting fluids in high-risk patients, close monitoring for hypoxia by the team is vital. The earlier the hypoxia is identified, the better the outcome. Those who survive have a lengthy recovery period to regain functional status. Many continue to have dyspnea even with mild exertion and thus depend on care from others.
Even though many risk factors for ARDS are known, there is no way of preventing ARDS. However, careful management of fluid in high-risk patients can be helpful. Steps should be taken to prevent aspiration by keeping the head of the bed elevated before feeding.
Discharge planning should include medication reconciliation, detailed home care planning (whether by family members or in-home/visiting nursing), and plans for follow-up visits and evaluations. Patients and caregivers must be counseled on signs of when to contact the clinician in the event of exacerbation or deterioration of the patient's condition.

Gajic O, Dabbagh O, Park PK, Adesanya A, Chang SY, Hou P, Anderson H 3rd, Hoth JJ, Mikkelsen ME, Gentile NT, Gong MN, Talmor D, Bajwa E, Watkins TR, Festic E, Yilmaz M, Iscimen R, Kaufman DA, Esper AM, Sadikot R, Douglas I, Sevransky J, Malinchoc M, U.S. Critical Illness and Injury Trials Group: Lung Injury Prevention Study Investigators (USCIITG-LIPS). Early identification of patients at risk of acute lung injury: evaluation of lung injury prediction score in a multicenter cohort study. American journal of respiratory and critical care medicine. 2011 Feb 15:183(4):462-70. doi: 10.1164/rccm.201004-0549OC. Epub 2010 Aug 27 [PubMed PMID: 20802164]
Wang Y, Zhang L, Xi X, Zhou JX, China Critical Care Sepsis Trial (CCCST) Workgroup. The Association Between Etiologies and Mortality in Acute Respiratory Distress Syndrome: A Multicenter Observational Cohort Study. Frontiers in medicine. 2021:8():739596. doi: 10.3389/fmed.2021.739596. Epub 2021 Oct 18 [PubMed PMID: 34733862]
Zambon M, Vincent JL. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest. 2008 May:133(5):1120-7. doi: 10.1378/chest.07-2134. Epub 2008 Feb 8 [PubMed PMID: 18263687]
Shrestha GS, Khanal S, Sharma S, Nepal G. COVID-19: Current Understanding of Pathophysiology. Journal of Nepal Health Research Council. 2020 Nov 13:18(3):351-359. doi: 10.33314/jnhrc.v18i3.3028. Epub 2020 Nov 13 [PubMed PMID: 33210623]
Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, LUNG SAFE Investigators, ESICM Trials Group. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA. 2016 Feb 23:315(8):788-800. doi: 10.1001/jama.2016.0291. Epub [PubMed PMID: 26903337]
Sedhai YR, Yuan M, Ketcham SW, Co I, Claar DD, McSparron JI, Prescott HC, Sjoding MW. Validating Measures of Disease Severity in Acute Respiratory Distress Syndrome. Annals of the American Thoracic Society. 2021 Jul:18(7):1211-1218. doi: 10.1513/AnnalsATS.202007-772OC. Epub [PubMed PMID: 33347379]
Sharma NS, Lal CV, Li JD, Lou XY, Viera L, Abdallah T, King RW, Sethi J, Kanagarajah P, Restrepo-Jaramillo R, Sales-Conniff A, Wei S, Jackson PL, Blalock JE, Gaggar A, Xu X. The neutrophil chemoattractant peptide proline-glycine-proline is associated with acute respiratory distress syndrome. American journal of physiology. Lung cellular and molecular physiology. 2018 Nov 1:315(5):L653-L661. doi: 10.1152/ajplung.00308.2017. Epub 2018 Aug 9 [PubMed PMID: 30091378]
Huang D, Ma H, Xiao Z, Blaivas M, Chen Y, Wen J, Guo W, Liang J, Liao X, Wang Z, Li H, Li J, Chao Y, Wang XT, Wu Y, Qin T, Su K, Wang S, Tan N. Diagnostic value of cardiopulmonary ultrasound in elderly patients with acute respiratory distress syndrome. BMC pulmonary medicine. 2018 Aug 13:18(1):136. doi: 10.1186/s12890-018-0666-9. Epub 2018 Aug 13 [PubMed PMID: 30103730]
Vieillard-Baron A, Schmitt JM, Augarde R, Fellahi JL, Prin S, Page B, Beauchet A, Jardin F. Acute cor pulmonale in acute respiratory distress syndrome submitted to protective ventilation: incidence, clinical implications, and prognosis. Critical care medicine. 2001 Aug:29(8):1551-5 [PubMed PMID: 11505125]
Chen WL, Lin WT, Kung SC, Lai CC, Chao CM. The Value of Oxygenation Saturation Index in Predicting the Outcomes of Patients with Acute Respiratory Distress Syndrome. Journal of clinical medicine. 2018 Aug 8:7(8):. doi: 10.3390/jcm7080205. Epub 2018 Aug 8 [PubMed PMID: 30096809]
Rawal G, Yadav S, Kumar R. Acute Respiratory Distress Syndrome: An Update and Review. Journal of translational internal medicine. 2018 Jun:6(2):74-77. doi: 10.1515/jtim-2016-0012. Epub 2018 Jun 26 [PubMed PMID: 29984201]
Cherian SV, Kumar A, Akasapu K, Ashton RW, Aparnath M, Malhotra A. Salvage therapies for refractory hypoxemia in ARDS. Respiratory medicine. 2018 Aug:141():150-158. doi: 10.1016/j.rmed.2018.06.030. Epub 2018 Jul 3 [PubMed PMID: 30053961]
Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E, Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S, Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, Bayle F, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, PROSEVA Study Group. Prone positioning in severe acute respiratory distress syndrome. The New England journal of medicine. 2013 Jun 6:368(23):2159-68. doi: 10.1056/NEJMoa1214103. Epub 2013 May 20 [PubMed PMID: 23688302]
National Heart, Lung, and Blood Institute PETAL Clinical Trials Network, Moss M, Huang DT, Brower RG, Ferguson ND, Ginde AA, Gong MN, Grissom CK, Gundel S, Hayden D, Hite RD, Hou PC, Hough CL, Iwashyna TJ, Khan A, Liu KD, Talmor D, Thompson BT, Ulysse CA, Yealy DM, Angus DC. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. The New England journal of medicine. 2019 May 23:380(21):1997-2008. doi: 10.1056/NEJMoa1901686. Epub 2019 May 19 [PubMed PMID: 31112383]
National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF Jr, Hite RD, Harabin AL. Comparison of two fluid-management strategies in acute lung injury. The New England journal of medicine. 2006 Jun 15:354(24):2564-75 [PubMed PMID: 16714767]
Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. The New England journal of medicine. 2011 Nov 17:365(20):1905-14. doi: 10.1056/NEJMct1103720. Epub [PubMed PMID: 22087681]
Combes A, Hajage D, Capellier G, Demoule A, Lavoué S, Guervilly C, Da Silva D, Zafrani L, Tirot P, Veber B, Maury E, Levy B, Cohen Y, Richard C, Kalfon P, Bouadma L, Mehdaoui H, Beduneau G, Lebreton G, Brochard L, Ferguson ND, Fan E, Slutsky AS, Brodie D, Mercat A, EOLIA Trial Group, REVA, and ECMONet. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. The New England journal of medicine. 2018 May 24:378(21):1965-1975. doi: 10.1056/NEJMoa1800385. Epub [PubMed PMID: 29791822]
Yang P, Formanek P, Scaglione S, Afshar M. Risk factors and outcomes of acute respiratory distress syndrome in critically ill patients with cirrhosis. Hepatology research : the official journal of the Japan Society of Hepatology. 2019 Mar:49(3):335-343. doi: 10.1111/hepr.13240. Epub 2018 Aug 29 [PubMed PMID: 30084205]
Annane D, Pastores SM, Rochwerg B, Arlt W, Balk RA, Beishuizen A, Briegel J, Carcillo J, Christ-Crain M, Cooper MS, Marik PE, Umberto Meduri G, Olsen KM, Rodgers S, Russell JA, Van den Berghe G. Correction to: Guidelines for the diagnosis and management of critical illness-related corticosteroid insufficiency (CIRCI) in critically ill patients (Part I): Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017. Intensive care medicine. 2018 Mar:44(3):401-402. doi: 10.1007/s00134-018-5071-6. Epub [PubMed PMID: 29476199]
Rodrigo C, Leonardi-Bee J, Nguyen-Van-Tam J, Lim WS. Corticosteroids as adjunctive therapy in the treatment of influenza. The Cochrane database of systematic reviews. 2016 Mar 7:3():CD010406. doi: 10.1002/14651858.CD010406.pub2. Epub 2016 Mar 7 [PubMed PMID: 26950335]
Anand R, McAuley DF, Blackwood B, Yap C, ONeill B, Connolly B, Borthwick M, Shyamsundar M, Warburton J, Meenen DV, Paulus F, Schultz MJ, Dark P, Bradley JM. Mucoactive agents for acute respiratory failure in the critically ill: a systematic review and meta-analysis. Thorax. 2020 Aug:75(8):623-631. doi: 10.1136/thoraxjnl-2019-214355. Epub 2020 Jun 8 [PubMed PMID: 32513777]
Gadre SK, Duggal A, Mireles-Cabodevila E, Krishnan S, Wang XF, Zell K, Guzman J. Acute respiratory failure requiring mechanical ventilation in severe chronic obstructive pulmonary disease (COPD). Medicine. 2018 Apr:97(17):e0487. doi: 10.1097/MD.0000000000010487. Epub [PubMed PMID: 29703009]
Chiumello D, Coppola S, Froio S, Gotti M. What's Next After ARDS: Long-Term Outcomes. Respiratory care. 2016 May:61(5):689-99. doi: 10.4187/respcare.04644. Epub [PubMed PMID: 27121623]
Villar J, Schultz MJ, Kacmarek RM. The LUNG SAFE: a biased presentation of the prevalence of ARDS! Critical care (London, England). 2016 Apr 25:20(1):108. doi: 10.1186/s13054-016-1273-x. Epub 2016 Apr 25 [PubMed PMID: 27109238]
Bos LD, Cremer OL, Ong DS, Caser EB, Barbas CS, Villar J, Kacmarek RM, Schultz MJ, MARS consortium. External validation confirms the legitimacy of a new clinical classification of ARDS for predicting outcome. Intensive care medicine. 2015 Nov:41(11):2004-5. doi: 10.1007/s00134-015-3992-x. Epub 2015 Jul 23 [PubMed PMID: 26202043]