Introduction
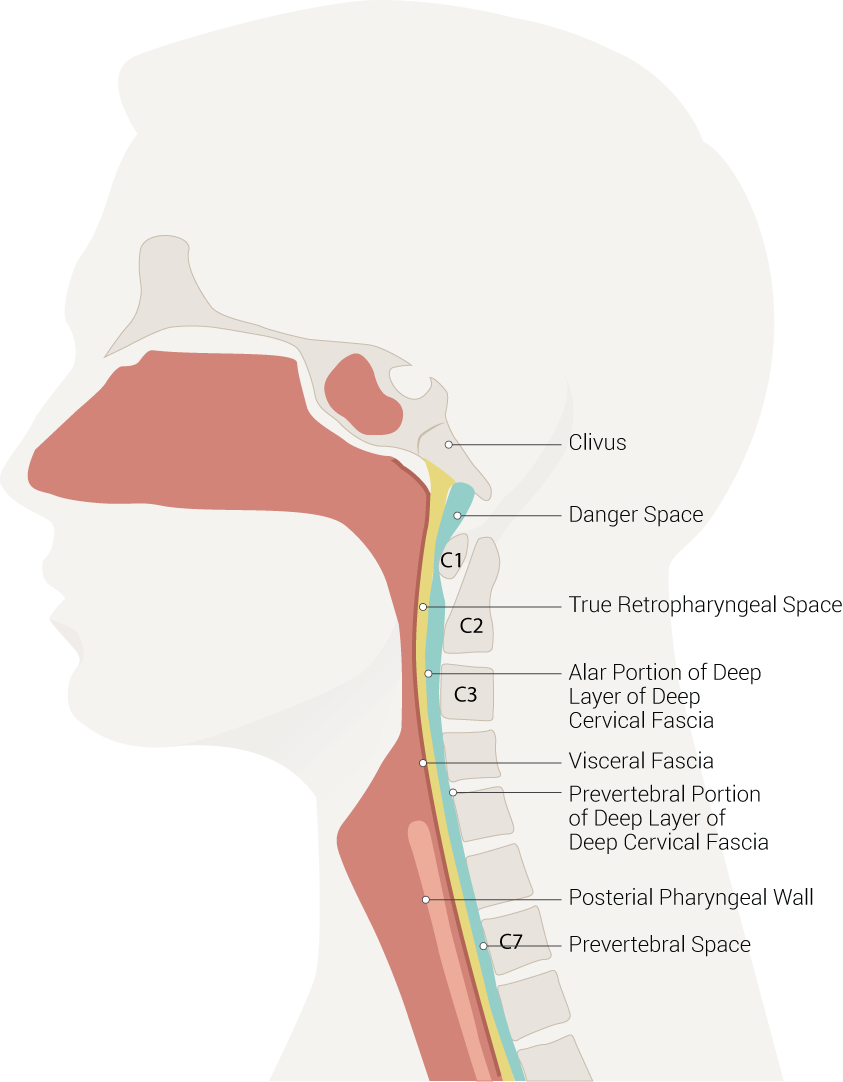
The retropharyngeal space (RPS) is the most important fascial space in the neck. The retropharyngeal space is an anatomical region that spans from the base of the skull to the mediastinum. This space is anterior to the prevertebral muscles and posterior to the pharynx and esophagus. The retropharyngeal space is bounded anteriorly by the buccopharyngeal fascia, laterally by the carotid sheath, and posteriorly by the prevertebral fascia. The RPS is divided by the alar fascia into two components–the “true” retropharyngeal space and the “danger space.” The true RPS is located anterior to the danger space and extends from the base of the skull to the alar fascia.
The retropharyngeal space functions as one of the deep compartments in the head and neck; it divides into suprahyoid and infrahyoid components. The suprahyoid RPS is composed of adipose tissue and lymph nodes.[1] The infrahyoid RPS solely contains adipose tissue.[1]
Within the true RPS, lymph nodes and fatty tissue are the predominant tissues. The suprahyoid RPS houses the retropharyngeal lymph nodes, which are responsible for most of the lymphatic drainage of the pharynx.[1] The retropharyngeal lymph nodes lie medial to the internal carotid artery and further divide into medial and lateral masses. The medial group atrophies throughout childhood, making children more likely to experience RPS infections than adults. The lateral group, named the nodes of Rouvière, persists throughout adulthood and can become a site of metastasis for head and neck cancers.[1][2]
The alar fascia is subject to considerable anatomical variation.[3] The alar fascia is generally described as a layer of dense connective tissue lying within the coronal plane. This fascial layer separates the retropharyngeal space anteriorly from the danger space posteriorly.[4] The fascia is attached to the base of the skull superiorly and laterally to the right and left carotid sheaths. It has been described as extending to the second thoracic vertebra, where it fuses with the visceral fascia, although other levels are described as well, from C6 to T2.[3][5][6]
The alar fascia separates the retropharyngeal space from the danger space located posterior to it. The danger space is so named because of the risk that an infection in this space can directly invade the mediastinum, causing serious and even fatal consequences such as mediastinitis, empyema, and necrotizing fasciitis.[4] The danger space courses more inferiorly than the true RPS, running into the posterior mediastinum until the level of the diaphragm. This anatomical connection between the pharynx and the mediastinum is where the danger space derives its name, as it serves as a potential channel for spreading infection between these two sites.[1][2]
The danger space is composed of solely adipose tissue and, therefore, can be affected by diseases that do not affect the lymph nodes, such as lipoma and liposarcoma.
An infection of the neck may spread through the prevertebral fascia and enter the retropharyngeal space.[7] An example of this is Pott disease of the spine.
A retropharyngeal abscess has been reported after the extraction of wisdom teeth.[8]
A peritonsillar abscess may also produce a retropharyngeal abscess.[9]
Structure and Function
There are two layers of cervical fascia: the superficial and deep layers. The subcutaneous superficial layer envelops the platysma muscles. With age, this layer and the platysma and overlying skin become loose, leading to the formation of a dewlap, or “turkey neck.”
The deep layer of cervical fascia has three components: the investing fascia, the pretracheal fascia, and the prevertebral fascia. The deep layer forms the carotid sheath, which contains the internal jugular vein, the common carotid artery, and the vagus nerve. The sympathetic trunk and ganglia lie posterior to the carotid sheath.
The investing layer of the deep cervical fascia divides posteriorly to invest the sternocleidomastoid and trapezius muscles. This fascia attaches to the base of the skull, the nuchal ligament, and the spinous process of the C7 vertebra.
The muscular part of the middle layer, the pretracheal fascia, envelops the infrahyoid muscles. The other part of the pretracheal fascia – the visceral part – envelops the thyroid gland, the trachea, and the esophagus. Posteriorly the visceral layer joins the carotid sheaths.
The buccopharyngeal fascia is attached to the buccinator and the superior, middle, and inferior pharyngeal constrictors.
The prevertebral fascia contains the muscles of the vertebra column, such as the longus colli and longus capitis, the deep cervical muscles, and the anterior, middle, and posterior scalene muscles.
The importance of these spaces is illustrated in the deep infections of the neck, which may be difficult to localize properly. This is important because abscesses usually require surgical drainage. By contrast, infections without abscesses can often be treated conservatively.[10]
Embryology
The structures of the head and neck, including the face, neck, and pharynx, derive from the branchial arches during weeks 4 to 7 of gestation. Six pairs of branchial arches form in cranio-caudal succession. The arches are composed of mesoderm and neural crest cells and give rise to cartilage, muscles, and nerves of the head and neck. They are surrounded externally by branchial clefts, which are ectodermal in origin and lined internally by endodermal-derived branchial pouches. This branchial apparatus is responsible for forming all structures bordering the RPS. The branchial arches give rise to the fascial components lining the RPS, and the branchial pouches form the primitive pharynx.[11]
The nerve of the first pharynx is the mandibular nerve of the trigeminal nerve. The nerve of the second arch is the facial nerve. The glossopharyngeal nerve is the nerve of the third arch. The fourth and sixth arches involve the vagus nerve.
Blood Supply and Lymphatics
The predominant tissues are within the actual retropharyngeal space, lymph nodes, and fatty tissue. The suprahyoid RPS houses the retropharyngeal lymph nodes, which are responsible for most of the lymphatic drainage of the pharynx. The retropharyngeal lymph nodes lie medial to the internal carotid artery and further divide into medial and lateral masses. The medial group atrophies throughout childhood, making children more likely to experience RPS infections than adults.
The lateral group, named the nodes of Rouvière, persists throughout adulthood and can become a site of metastasis for head and neck cancers. The danger space is composed of solely adipose tissue and, therefore, can be affected by non-nodal diseases.[1][2]
The blood supply to the pharynx varies based on anatomic location. The superior pharynx receives its blood supply from the ascending pharyngeal artery and the lesser palatine arteries. The inferior pharynx’s blood supply comes from the superior and inferior thyroid arteries. Another significant relationship is the proximity of the carotid sheath (internal carotid artery, common carotid artery, internal jugular vein, and vagus nerve) to the retropharyngeal space, composing the lateral border of the region.
Nerves
No nerves run within the retropharyngeal space, but it borders with many nerves. The pharyngeal nerve plexus and the pharyngeal venous plexus are on the buccopharyngeal fascia. This pharyngeal nerve plexus contains fibers of cranial nerves IX (glossopharyngeal), X (vagus), and XI (accessory nerve) and is considered the main sensory and motor nervous supply of the pharynx.
The vagus nerve, running within the carotid sheath, gives off the recurrent laryngeal branch, which descends inferiorly alongside the pharynx. The recurrent laryngeal nerve innervates the intrinsic muscles of the larynx, apart from the cricothyroid muscle.
Muscles
The longus colli muscles serve as an important landmark for the retropharyngeal space as they mark the location of the medial group of retropharyngeal lymph nodes from the lateral group of nodes. The medial lymph nodes are anterior to the longus colli muscle, and the lateral lymph nodes are ventral to the muscle.
The prevertebral space is located directly posterior to the danger space and houses the levator scapulae, splenius capitis, scalenes, and splenius cervicis muscles. This anatomical relationship becomes important as a mass in the prevertebral space can be suggested by anterior displacement of the RPS.[1]
Physiologic Variants
In rare cases, the internal carotid artery can take an anomalous course through the retropharyngeal space. This relationship may be congenital in nature due to an improperly descended third aortic arch and present throughout one’s life with symptoms such as dysphonia. This anomaly may be more evident in older individuals with a history of atherosclerosis and hypertension, both of which can exacerbate clinical signs and symptoms. This anomalous artery may increase a patient’s risk for vascular injury during surgery in the pharyngeal region and during intubation.[12][13]
Surgical Considerations
As described above, an anomalous internal carotid artery is an essential surgical consideration while operating in the pharyngeal area. Various disease pathologies may occur in the retropharyngeal space that could warrant surgery as one of the treatment options.[14] These include:
- Retropharyngeal abscess: The two most common causes of RPS abscess are pyogenic lymphadenitis and peritonsillar abscesses. However, any cervical infection encompassing lymphatic drainage in the pharynx, prevertebral space, middle ear, or paranasal sinuses may lead to this pathology. Symptoms that can raise concern for an RPS abscess include fever, dysphagia, and a sore throat. These symptoms are non-specific and diagnostic imaging should be done to confirm a suspected abscess. A CT scan with contrast of the neck is the diagnostic imaging of choice and will show a collection of fluid under tension in the RPS with rim enhancement. The retropharyngeal lymph nodes are also typically enlarged. An abscess in the danger space of the RPS can lead to the spreading of the infection into the mediastinum. An RPS abscess requires surgical drainage as the first line of treatment.[1][2][10]
-
Children between the ages of two and four form the most common cases of retropharyngeal abscesses, but this condition may be found at all ages.[15]
-
Primary lesions of the RPS: lipoma, liposarcoma, synovial sarcoma.[1]
- Direct spread and metastasis: nasopharyngeal carcinoma, squamous cell carcinoma (pharyngeal, laryngeal, sinonasal, oral cavity), lymphoma, melanoma, esthesioneuroblastoma, papillary thyroid carcinoma, chordoma, primary spinal tumors, and thyroid goiters.[1]
- Fluid collection: There are a variety of disease pathologies that may cause fluid accumulation in the RPS. These include foreign body ingestion, hematoma, angioedema, retropharyngeal lymphadenitis, vertebral osteomyelitis, Kawasaki disease, pyriform sinus, calcific tendinitis of the longus colli muscle, and cystic tumor caused by lymphatic malformation. Most of these conditions will be referred to a surgical specialist for management.[2]
- Surgical drainage and intravenous antibiotic therapy are the most common approaches to retropharyngeal abscesses.[8] Although the mortality rate is relatively low in uncomplicated cases, it may approach 25% in cases complicated by mediastinitis.
Clinical Significance
The retropharyngeal space is a significant region to consider when evaluating a patient with neck pain, as many pathologies can manifest and affect this area. The connection of the danger space to the mediastinum allows the spread of infections from the oral cavity to the thoracic cavity. Potential life-threatening complications related to infections in the RPS include mediastinitis and airway obstruction. These two conditions should be considered when the RPS is involved in a disease process.[14]
Other Issues
A smaller number of other etiologies may present in the retropharyngeal space, often requiring non-surgical treatment. These include:
- Thoracic duct cysts are rare entities that may cause respiratory distress in the presenting patient, most commonly linked with trauma or a neoplasm. A potential treatment option for these individuals is sclerotherapy.[16]
- Retropharyngeal emphysema: the best definition of this condition is free air in the retropharyngeal space. The causes can include trauma, surgery, obstructive respiratory disease, substance abuse, bronchial asthma, physical exertion, or spontaneous.[14][17][18][19]
- The clinical symptoms include dysphagia, neck pain, sore throat, and odynophagia. The recommended medical management includes an extensive history and physical, laryngoscopy to examine the airway, barium swallow to monitor potential esophageal perforation, and imaging studies of the neck such as CT and plain radiographs. Most patients will resolve without intensive medical therapy as the condition is typically self-limiting and treatment is supportive.[19][20]
- Other lesions: foregut duplication cysts, leiomyoma, ectopic parathyroid adenoma, and vertebral disk bulge.[1]