Introduction
The hyoid bone (hyoid) is a small U-shaped (horseshoe-shaped) solitary bone situated in the midline of the neck anteriorly at the base of the mandible and posteriorly at the fourth cervical vertebra. Its anatomical position is just superior to the thyroid cartilage. It is closely linked with an extended tendon-muscular complex but not specifically interconnected to any adjacent bones and, hence, is considered by many anatomists and anthropologists to be an unconventional bone. It is anchored in the anterior triangle of the neck by muscles from the larynx, pharynx, tongue, and the floor of the mouth. The name hyoid derives from the Greek word “hyodeides,” which means “shaped like the letter Upsilon.” Although dubbed as an unconventional bone, the hyoid, being a part of the hyoid-larynx complex, is indeed a bone of clinical and forensic significance.
Structure and Function
The hyoid consists of a body, two greater horns, and two lesser horns.[1] The body forms the central quadrilateral-shaped broad segment of the hyoid. The greater horns are larger and longer than the lesser horns of the hyoid. The greater and lesser horns are also known as cornu majus and cornu minus, respectively. The body and the greater horns appear to give the hyoid its U-shape, with the greater horns forming the limbs of the "U" on either side of the body. The greater and lesser horns normally unite to the body of the hyoid via fibrous tissue or a true joint.[2] As age progresses, there is a physiological progression of ankylosis of the joints connecting the greater and lesser horns with the body of the hyoid.
The hyoid takes part in all possible functional actions of the orofacial complex. It preserves the patency of the airway between the oropharynx above and the tracheal rings below. It also connects to the larynx and hence plays a role in phonation. Other functions include tongue movement, mastication, swallowing, prevention of regurgitation, and even respiration.[1][3] Furthermore, the hyoid maintains the posture of the head due to the complex connection it presumes between the mandible and the cervical spine.[1]
Embryology
The second pharyngeal arch forms the lesser horn (cornu) and the upper body of the hyoid, while the greater horn (cornu) and the lower portion of the body derive from the third pharyngeal arch. This embryonic development of the hyoid remains controversial.[1] The ossification of the greater horns occurs toward the end of the normal gestational period of the fetus; this is followed by the ossification of the body of the hyoid soon after birth. Eventually, ossification of the lesser horns occurs during the first or second year after birth. Later in adulthood, normally, the horns fuse with the body, but this may not take place in all individuals. The hyoid is situated anterior to the second and third cervical vertebra during infancy, and ultimately, in adulthood, it descends to the level of the fourth and fifth cervical vertebra. The descent takes place simultaneously with the other functionally relevant structures, including the epiglottis and the larynx.[3]
Muscles
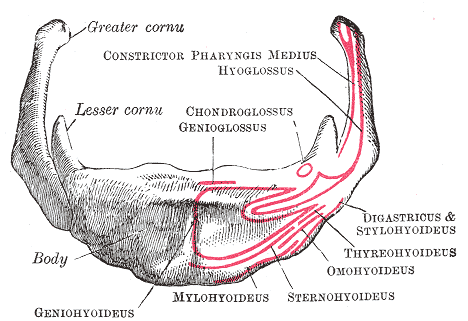
The hyoid functions as an anchor for the suprahyoid muscles (digastric, stylohyoid, mylohyoid, and geniohyoid) as well as the infrahyoid muscles (sternohyoid, sternothyroid, omohyoid, and thyrohyoid).[2] The stylohyoid ligament suspends the hyoid from the temporal styloid process on either side. It is restricted by the ligamentous attachments inferiorly to the superior aspect of the thyroid cartilage through the thyrohyoid membrane. Additionally, the hyoid is attached to the cervical spine posteriorly via the cervical fascia.[1]
Suprahyoid Muscles
The suprahyoid muscles are four in number on either side of the anterior midline above the level of the hyoid (media image, table 1). They attach the hyoid to the mandible, tongue, and skull. The digastric muscle has two bellies, posterior and anterior. The anterior belly originates from the digastric fossa of the mandible, while the posterior belly originates from the mastoid notch. Both the digastric bellies insert into the intermediate tendon of the digastric muscle, which is attached to the hyoid. The stylohyoid muscle originates from the temporal styloid process; it is a thin and long muscle that lies parallel to the posterior belly of the digastric. The mylohyoid muscle originates from the mylohyoid line of the mandible; it is a thin muscle that upholds and makes up the floor of the mouth while also creating a sling inferior to the tongue. The geniohyoid muscle is a narrow and short muscle that originates from the interior mental spine of the symphysis menti. The stylohyoid, mylohyoid, and geniohyoid insert on the body of the hyoid.[1]
Infrahyoid Muscles
The infrahyoid muscles are four pairs of muscles located in the anterior part of the neck (media image, table 2). They are found between the hyoid above and the shoulder girdle below. The sternohyoid muscle primarily originates from the back of the manubrium and inserts on the medial part of the inferior border of the hyoid body. The sternothyroid muscle originates primarily from the back of the manubrium and inserts on the oblique line of the thyroid cartilage. The omohyoid muscle has a superior belly and an inferior belly. The superior belly of the omohyoid arises from the intermediate tendon of the omohyoid and inserts on the hyoid. The inferior belly of the omohyoid originates from the scapular superior border and inserts into the intermediate tendon of the omohyoid. The thyrohyoid muscle originates from the oblique line of the thyroid cartilage and inserts at the inferior aspect of the body of the hyoid and the greater cornu.[1][4]
Other Muscles Related to the Hyoid
The hyoglossus and the middle pharyngeal constrictor originate from the hyoid. These muscles do not form the group mentioned above of muscles related to the hyoid.
Elevation of the Hyoid
The digastric, stylohyoid, mylohyoid, and geniohyoid function in elevating the hyoid.
Depression of the Hyoid
The sternohyoid, sternothyroid, omohyoid, and thyrohyoid function in depressing the hyoid.
Physiologic Variants
The hyoid shows a wide range of anatomical variations, most likely owing to the asymmetry of the greater and lesser horns. Therefore, the hyoid is considered one of the most polymorphic parts of the human body. The commonest variation of the hyoid takes place in the process of ankylosis of the joints between the horns (greater and lesser horns) and the body of the hyoid. Ethnicity, sex, age, height, and weight of the subject contribute to the morphological variations. These variations can happen unilaterally or bilaterally, and multiple variations can occur in the same individual.[2] Surprisingly, the absence of the hyoid has been reported as well in a male neonate who was also a teratoma case, had a mandibular cleft, and suffered from respiratory distress.[5] These anomalies correlate to some clinical conditions such as micrognathia, Pierre Robin sequence, and cleft lip and palate. Symptoms caused by these anomalies include dysphagia, neck movement limitations, and foreign body sensation in the throat.[2]
Surgical Considerations
The Hyoid and its Relation to Blood Vessels
The tip of the greater horn of the hyoid is a significant landmark for cervical surgery in the mid-neck region. The carotid bifurcation, the superior thyroid artery, and the lingual artery are closely related to the tip of the greater horn. The tip of the greater horn is a useful landmark in locating these arteries during cervical surgery. The carotid bifurcation is located inferior and posterior to the tip of the greater horn. Also, the origin of the superior thyroid artery, which is the first branch of the external carotid artery, lies below the level of the greater horn. The lingual artery is one of the closely related structures to the hyoid, and it branches off the external carotid artery above the level of the greater horn.[6]
The Hyoid and its Relation to Nerves
The hypoglossal and the superior laryngeal nerve are closely related to the tip of the greater horn of the hyoid. The tip of the greater horn aids the surgeon in locating these nerves during cervical surgery. The hypoglossal nerve lies superiorly to the tip of the greater horn of the hyoid. The superior laryngeal nerve divides into its external and internal branches as it passes behind the greater horn, with its external branch being deeper than the internal one.[6]
The Hyoid and Obstructive Sleep Apnea Syndrome
Obstructive sleep apnea is a chronic sleep-related breathing disorder. It is best described by repeated narrowing and obstruction of the pharyngeal airway during sleep.[7] This condition is caused by pharyngeal collapsibility, which is due to the loss of wakefulness stimulus and changes in neuromuscular control. Several factors contribute to the pharyngeal collapsibility; the hyoid position is one of these factors. An imbalance between the suprahyoid and infrahyoid muscles may lead to alteration in the position of the hyoid, thus affecting the airway patency and causing more pharyngeal collapsibility.[8] The clinical manifestations include non-refreshing sleep, daytime sleepiness, fatigue, nocturia, irritability, and morning headaches. If left unmanaged, it may lead to many complications, including cardiovascular diseases, cognitive impairment, and decreased productivity and concentration, which may lead to road traffic accidents.[7] The treatment of choice is the nasal continuous positive airway pressure; if unsuccessful, other options include oral devices, positional therapy,[9] upper airway surgery such as genioglossus advancement,[10] hyoidothyroidopexy (hyoid suspension),[11] hyoid myotomy and sliding genioplasty.[10]
Clinical Significance
Hyoid Bone Insertion Tendinitis
Hyoid bone insertion tendinitis is also known as hyoid bone syndrome. Patients describe it as neck pain that increases with swallowing and movement of the neck. The pain is characteristically either dull or sharp, radiating to the temporal area, posterior pharyngeal wall, sternocleidomastoid muscle, ear, and supraclavicular region. On examination, tenderness over the greater horn of the hyoid is noted upon palpation. The condition is diagnosed mainly by history and physical examination. Imaging may be used to exclude the other differential diagnoses. Medical therapy is the initial treatment of choice. It includes topical and systemic non-steroidal anti-inflammatory medications, local anesthetics, and steroid injections. If medical therapy fails, then surgery is the next consideration.[12]
Calcified Stylohyoid Ligament and Eagle Syndrome
- It is important to discuss Eagle syndrome here in the context of calcification of the stylohyoid ligament that connects the lesser horn of the hyoid with the tip of the styloid process, causing similar symptomatology. The literature reports cases of unilateral and bilateral calcification of the styloid ligament. There may be partial or complete calcification of the stylohyoid ligament. Incidental cases of the calcified stylohyoid ligament also present in otherwise asymptomatic subjects.[13][14]
- There are two types of Eagle syndrome. The first type is the classic Eagle syndrome or the classic styloid syndrome, usually seen after tonsillectomy as pharyngodynia found in the tonsillar fossa, occasionally associated with odynophagia, dysphagia, foreign body sensation, hypersalivation, and seldom, temporary voice changes. These symptoms appear when the tightened tonsillectomy scar tissue moves along the tip of an elongated styloid process through functional movements.
- The second type is called the stylo-carotid syndrome, and it develops following the compression of the internal and/or external carotid arteries and their perivascular sympathetic fibers, which leads to constant pain that radiates to the carotid region, such as chronic neck pain, headache, pain when moving the head and pain that radiates to the eye. Other symptoms include vertigo and ear pain. Therefore, patients with these symptoms may present to the ENT, dental, neurosurgery, or ophthalmology clinics with a variety of complaints.[15] Additionally, as described above, this syndrome may be the result of calcification of the stylohyoid ligament. However, it is mostly silent.[16]
- Differential diagnoses of this syndrome include temporomandibular joint diseases, temporal arteritis, glossopharyngeal, sphenopalatine, or trigeminal neuralgias, mastoiditis, dental pain, hyoid bursitis, cluster-type headache, and migraine.[15]
- Imaging is vital when diagnosing Eagle syndrome, as an elongated styloid process is the most common presenting sign. The styloid process is considered elongated if its length is greater than 2 inches.[1]
- Treatment options include medical and surgical. The medical treatment consists of antihistamines, neuroleptics, vasodilators, tranquilizers, antidepressants, steroid injections, and local anesthetics. Surgery is considered a secondary treatment approach, as there are recurrences reported postoperatively.[15]
Other Issues
Forensic Anatomy of the Hyoid
The forensic profile of the hyoid related to forensic anthropology primarily includes the estimation of age and determination of sex. Fusion of the hyoid is especially useful to predict age in adulthood. The bone density of the hyoid is a valuable predictor of both age and sex [3]. However, it is worth noting that the literature reports a wide range of variability in the degree and timing of fusion of the greater horns with the body of the hyoid. Using discriminant function analysis, various metric measurements of the hyoid are found to be useful in determining the sex of the bone.[17]
Forensic Significance of Hyoid Fracture
Trauma to the hyoid and laryngeal cartilages (thyroid cartilage and cricoid cartilage) is one of the significant signs of manual strangulation or throttling discovered during a forensic autopsy. Fractures of the hyoid-laryngeal complex are present in cases of death due to a constricting force around the neck. Forensic pathologists have intensively studied traumatic lesions of the hyoid-laryngeal complex in strangulation, including manual strangulation, ligature strangulation, and hanging. Other forms of blunt force impact to the neck can also cause fracture of the hyoid.
The damage commonly affects the greater horns or the region between the body of the hyoid and the horns. Injuries are mainly in the form of vertical or oblique fractures. Displacements of the fracture segments are also observed. Bilateral fractures of the hyoid and double fractures of one of the greater horns are not uncommon.[18] The frequency of a fractured hyoid is higher in cases of strangulation in comparison to cases of hanging. However, a hyoid fracture is present in only about a third of all homicides from strangulation.[19] Therefore, it merits noting that an intact hyoid does not always rule out strangulation as the underlying cause of death. The hyoid is fractured more commonly in the older victims of strangulation and is less likely to occur in younger victims of strangulation in the age group 20 to 40.[19] The differences in the age-related frequency of hyoid fracture are dependent on the degree of ankylosis of the hyoid that progresses with age. The mobility in the region of the junction between the greater horns and the body of the hyoid should not be mistaken for a fracture.